Prevalence of All-Cause Mortality and Suicide among Bariatric Surgery Cohorts: A Meta-Analysis




Abstract
:1. Introduction
2. Methodology
2.1. Comprehensive Search Strategy
2.2. Inclusion and Exclusion Criteria
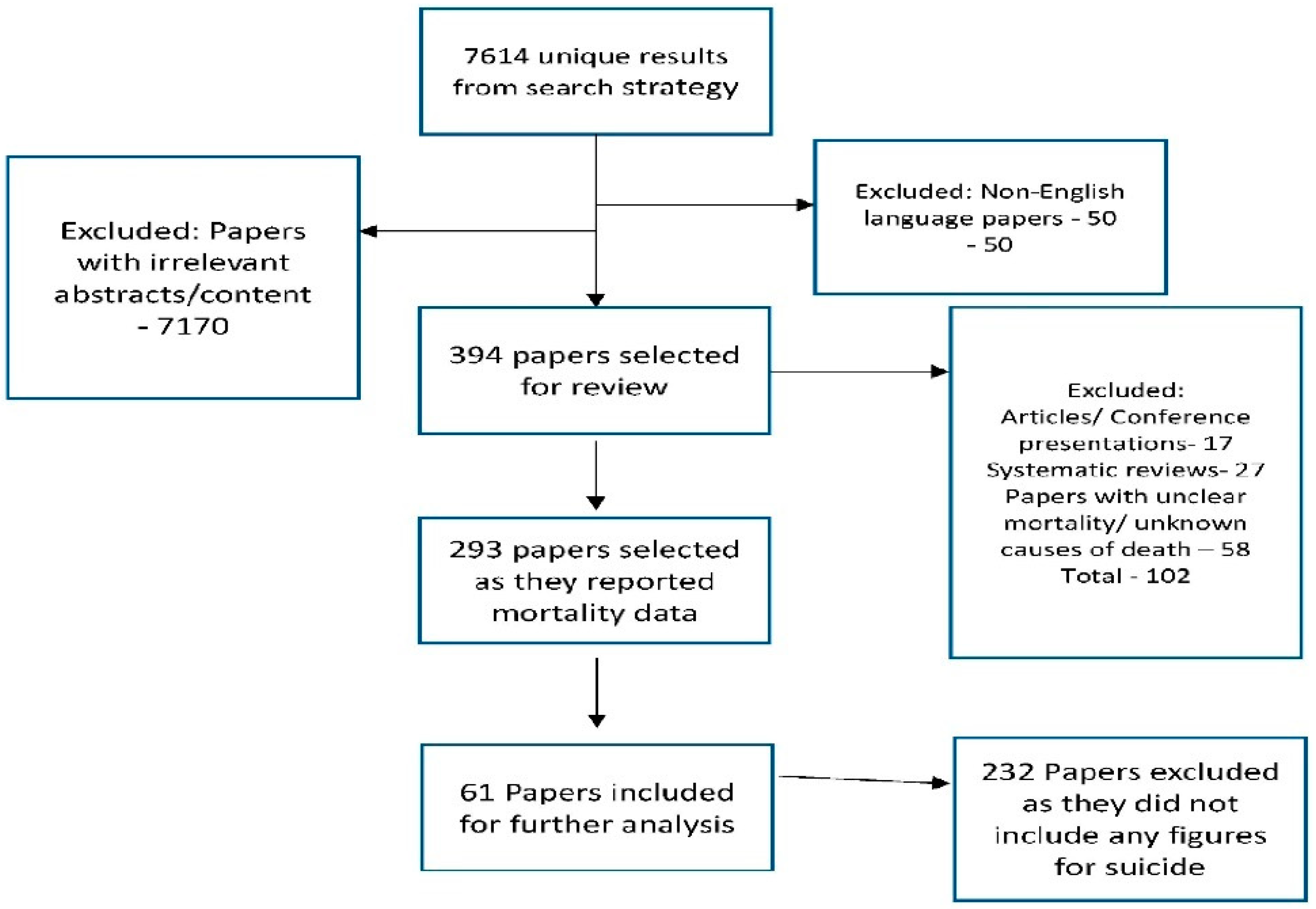
2.3. Selection of Articles
2.4. Statistical Methods
2.4.1. Data Extraction
2.4.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. Obesity. 2017. Available online: http://www.who.int/topics/obesity/en/ (assessed on 27 April 2017).
- Sanjeev, S.; Raed, H. Psychiatric Care in Severe Obesity: An Interdisciplinary Guide to Integrated Care, 1st ed.; Springer: Berlin, Germany, 2017. [Google Scholar]
- Rajan, T.M.; Menon, V. Psychiatric disorders and obesity: A review of association studies. J. Postgrad. Med. 2017, 63, 182–190. [Google Scholar] [PubMed]
- Global Strategy on Diet, Physical Activity and Health. World Health Organization. 2017. Available online: http://www.who.int/dietphysicalactivity/en/ (assessed on 27 April 2017).
- Senger, E. Bariatric surgery guidelines in need of revision, experts argue. CMAJ 2011, 183, E234. [Google Scholar] [CrossRef] [PubMed]
- Maggard, M.A.; Shugarman, L.R.; Suttorp, M.; Maglione, M.; Sugerman, H.J.; Livingston, E.H.; Nguyen, N.T.; Li, Z.; Mojica, W.A.; Hilton, L. Meta-analysis: Surgical treatment of obesity. Ann. Intern. Med. 2005, 142, 547–559. [Google Scholar] [CrossRef] [PubMed]
- Angrisani, L.; Santonicola, A.; Iovino, P.; Formisano, G.; Buchwald, H.; Scopinaro, N. Bariatric Surgery Worldwide 2013. Obes. Surg. 2015, 25, 1822–1832. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slomski, A. Bariatric Surgery Has Durable Effects in Controlling Diabetes. JAMA 2017, 317, 1615. [Google Scholar] [CrossRef] [PubMed]
- Tirado, R.; Masdeu, M.J.; Vigil, L.; Rigla, M.; Luna, A.; Rebasa, P.; Pareja, R.; Hurtado, M.; Caixàs, A. Impact of Bariatric Surgery on Heme Oxygenase-1, Inflammation, and Insulin Resistance in Morbid Obesity with Obstructive Sleep Apnea. Obes. Surg. 2017, 27, 2338–2346. [Google Scholar] [CrossRef] [PubMed]
- Neff, K.J.; Baud, G.; Raverdy, V.; Caiazzo, R.; Verkindt, H.; Noel, C.; le Roux, C.W.; Pattou, F. Renal Function and Remission of Hypertension After Bariatric Surgery: A 5-Year Prospective Cohort Study. Obes. Surg. 2017, 27, 613–619. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, L.; Rodrigues, D.; Gomes, L.; Carrilho, F. Short- and long-term mortality after bariatric surgery: A systematic review and meta-analysis. Diabetes Obes. Metab. 2017. [Google Scholar] [CrossRef] [PubMed]
- Peterhänsel, C.; Petroff, D.; Klinitzke, G.; Kersting, A.; Wagner, B. Risk of completed suicide after bariatric surgery: A systematic review. Obes. Rev. 2013, 14, 369–382. [Google Scholar] [CrossRef] [PubMed]
- Tindle, H.A.; Omalu, B.; Courcoulas, A.; Marcus, M.; Hammers, J.; Kuller, L.H. Risk of suicide after long-term follow-up from bariatric surgery. Am. J. Med. 2010, 123, 1036–1042. [Google Scholar] [CrossRef] [PubMed]
- Hensel, J.; Selvadurai, M.; Anvari, M.; Taylor, V. Mental Illness and psychotropic medication use among people assessed for bariatric surgery in Ontario, Canada. Obes. Surg. 2016, 26, 1531–1536. [Google Scholar] [CrossRef] [PubMed]
- Yen, Y.C.; Huang, C.K.; Tai, C.M. Psychiatric aspects of bariatric surgery. Curr. Opin. Psychiatry 2014, 27, 374–379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yusufov, M.; Dalrymple, K.; Bernstein, M.H.; Walsh, E.; Rosenstein, L.; Chelminski, I.; Zimmerman, M. Body mass index, depression, and suicidality: The role of self-esteem in bariatric surgery candidates. J. Affect. Disord. 2017, 208, 238–247. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, J.E.; Crosby, R.; de Zwaan, M.; Engel, S.; Roerig, J.; Steffen, K.; Gordon, K.H.; Karr, T.; Lavender, J.; Wonderlich, S. Possible risk factors for increased suicide following bariatric surgery. Obesity 2013, 21, 665–672. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ho, R.C.; Ong, H.S.; Kudva, K.G.; Cheung, M.W.; Mak, A. How to critically appraise and apply meta-analyses in clinical practice. Int. J. Rheum. Dis. 2010, 13, 294–299. [Google Scholar] [CrossRef] [PubMed]
- Cheung, M.W.; Ho, R.C.; Lim, Y.; Mak, A. Conducting a meta-analysis: Basics and good practices. Int. J. Rheum. Dis. 2012, 15, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Loh, A.Z.; Tan, J.S.; Zhang, M.W.; Ho, R.C. The Global Prevalence of Anxiety and Depressive Symptoms among Caregivers of Stroke Survivors. J. Am. Med. Dir. Assoc. 2017, 18, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Ho, R.C.; Ong, H.; Thiaghu, C.; Lu, Y.; Ho, C.S.; Zhang, M.W. Genetic Variants That Are Associated with Neuropsychiatric Systemic Lupus Erythematosus. J. Rheumatol. 2016, 43, 541–551. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Andiappan, A.K.; Lee, B.; Ho, R.; Lim, T.K.; Kuan, W.S.; Goh, D.Y.T.; Mahadevan, M.; Sim, T.B.; Wang, D.Y.; et al. Neuropeptide Y associated with asthma in young adults. Neuropeptides 2016, 59, 117–121. [Google Scholar] [CrossRef] [PubMed]
- Puthran, R.; Zhang, M.W.; Tam, W.W.; Ho, R.C. Prevalence of depression amongst medical students: A meta-analysis. Med. Educ. 2016, 50, 456–468. [Google Scholar] [CrossRef] [PubMed]
- Aarts, E.O.; Dogan, K.; Koehestanie, P.; Aufenacker, T.J.; Janssen, I.M.; Berends, F.J. Long-term results after laparoscopic adjustable gastric banding: A mean fourteen year follow-up study. Surg. Obes. Relat. Dis. 2014, 10, 633–640. [Google Scholar] [CrossRef] [PubMed]
- Adams, T.D.; Gress, R.E.; Smith, S.C.; Halverson, R.C.; Simper, S.C.; Rosamond, W.D.; LaMonte, M.J.; Stroup, A.M.; Hunt, S.C. Long-term mortality after gastric bypass surgery. N. Engl. J. Med. 2007, 357, 753–761. [Google Scholar] [CrossRef] [PubMed]
- Adams, T.D.; Davidson, L.E.; Litwin, S.E.; Kolotkin, R.L.; LaMonte, M.J.; Pendleton, R.C.; Strong, M.B.; Vinik, R.; Wanner, N.A.; Hopkins, P.N.; et al. Health benefits of gastric bypass surgery after 6 years. JAMA 2012, 308, 1122–1131. [Google Scholar] [CrossRef] [PubMed]
- Arapis, K.; Chosidow, D.; Lehmann, M.; Bado, A.; Polanco, M.; Kamoun-Zana, S.; Pelletier, A.L.; Kousouri, M.; Marmuse, J.-P. Long-term results of adjustable gastric banding in a cohort of 186 super-obese patients with a BMI ≥ 50 kg/m2. J. Visc. Surg. 2012, 149, e143–e152. [Google Scholar] [CrossRef] [PubMed]
- Arman, G.A.; Himpens, J.; Dhaenens, J.; Ballet, T.; Vilallonga, R.; Leman, G. Long-term (11+years) outcomes in weight, patient satisfaction, comorbidities, and gastroesophageal reflux treatment after laparoscopic sleeve gastrectomy. Surg. Obes. Relat. Dis. 2016, 12, 1778–1786. [Google Scholar] [CrossRef] [PubMed]
- Biertho, L.; Biron, S.; Hould, F.S.; Lebel, S.; Marceau, S.; Marceau, P. Is biliopancreatic diversion with duodenal switch indicated for patients with body mass index <50 kg/m2? Surg. Obes. Relat. Dis. 2010, 6, 508–514. [Google Scholar] [CrossRef] [PubMed]
- Bolckmans, R.; Himpens, J. Long-term (>10 years) Outcome of the Laparoscopic Biliopancreatic Diversion with Duodenal Switch. Ann. Surg. 2016, 264, 1029–1037. [Google Scholar] [CrossRef] [PubMed]
- Busetto, L.; Mirabelli, D.; Petroni, M.L.; Mazza, M.; Favretti, F.; Segato, G.; Chiusolo, M.; Merletti, F.; Balzola, F.; Enzi, G. Comparative long-term mortality after laparoscopic adjustable gastric banding versus nonsurgical controls. Surg. Obes. Relat. Dis. 2007, 3, 496–502. [Google Scholar] [CrossRef] [PubMed]
- Busetto, L.; De Stefano, F.; Pigozzo, S.; Segato, G.; De Luca, F.; Favretti, F. Long-term cardiovascular risk and coronary events in morbidly obese patients treated with laparoscopic gastric banding. Surg. Obes. Relat. Dis. 2014, 10, 112–120. [Google Scholar] [CrossRef] [PubMed]
- Cadière, G.-B.; Himpens, J.; Bazi, M.; Cadière, B.; Vouche, M.; Capelluto, E.; Dapri, G. Are laparoscopic gastric bypass after gastroplasty and primary laparoscopic gastric bypass similar in terms of results? Obes. Surg. 2011, 21, 692–698. [Google Scholar] [CrossRef] [PubMed]
- Capella, J.F.; Capella, R.F. The weight reduction operation of choice: Vertical banded gastroplasty or gastric bypass? Am. J. Surg. 1996, 171, 74–79. [Google Scholar] [CrossRef]
- Carelli, A.M.; Youn, H.A.; Kurian, M.S.; Ren, C.J.; Fielding, G.A. Safety of the laparoscopic adjustable gastric band: 7-year data from a U.S. center of excellence. Surg. Endosc. 2010, 24, 1819–1823. [Google Scholar] [CrossRef] [PubMed]
- Christou, N.V.; Look, D.; Maclean, L.D. Weight gain after short- and long-limb gastric bypass in patients followed for longer than 10 years. Ann. Surg. 2006, 244, 734–740. [Google Scholar] [CrossRef] [PubMed]
- Cobourn, C.; Chapman, M.A.; Ali, A.; Amrhein, J. Five-year weight loss experience of outpatients receiving laparoscopic adjustable gastric band surgery. Obes. Surg. 2013, 23, 903–910. [Google Scholar] [CrossRef] [PubMed]
- Diniz Mde, F.; Moura, L.D.; Kelles, S.M.; Diniz, M.T. Long-term mortality of patients submitted to Roux-en-Y gastric bypass in Public Health System: High prevalence of alcoholic cirrhosis and suicides. Arq. Bras. Cir. Dig. 2013, 26 (Suppl. 1), 53–56. [Google Scholar] [PubMed]
- Goldfeder, L.B.; Ren, C.J.; Gill, J.R. Fatal complications of bariatric surgery. Obes. Surg. 2006, 16, 1050–1056. [Google Scholar] [CrossRef] [PubMed]
- Gribsholt, S.B.; Thomsen, R.W.; Svensson, E.; Richelsen, B. Overall and cause-specific mortality after Roux-en-Y gastric bypass surgery: A nationwide cohort study. Surg. Obes. Relat. Dis. 2017, 13, 581–587. [Google Scholar] [CrossRef] [PubMed]
- Higa, K.D.; Boone, K.B.; Ho, T. Complications of the laparoscopic Roux-en-Y gastric bypass: 1040 patients—What have we learned? Obes. Surg. 2000, 10, 509–513. [Google Scholar] [CrossRef] [PubMed]
- Himpens, J.; Cadière, G.B.; Bazi, M.; Vouche, M.; Cadière, B.; Dapri, G. Long-term outcomes of laparoscopic adjustable gastric banding. Arch. Surg. 2011, 146, 802–807. [Google Scholar] [CrossRef] [PubMed]
- Himpens, J.; Verbrugghe, A.; Cadière, G.B.; Everaerts, W.; Greve, J.W. Long-term results of laparoscopic Roux-en-Y Gastric bypass: Evaluation after 9 years. Obes. Surg. 2012, 22, 1586–1593. [Google Scholar] [CrossRef] [PubMed]
- Bruschi Kelles, S.M.; Diniz, M.F.; Machado, C.J.; Barreto, S.M. Mortality rate after open Roux-in-Y gastric bypass: A 10-year follow-up. Braz. J. Med. Biol. Res. 2014, 47, 617–625. [Google Scholar] [CrossRef]
- Kral, J.G.; Görtz, L.; Hermansson, G.; Wallin, G.S. Gastroplasty for obesity: Long-term weight loss improved by vagotomy. World J. Surg. 1993, 17, 75–78. [Google Scholar] [CrossRef] [PubMed]
- Lagerros, Y.T.; Brandt, L.; Hedberg, J.; Sundbom, M.; Bodén, R. Suicide, Self-harm, and Depression after Gastric Bypass Surgery: A Nationwide Cohort Study. Ann. Surg. 2017, 265, 235–243. [Google Scholar] [CrossRef] [PubMed]
- Lemanu, D.P.; Singh, P.P.; Rahman, H.; Hill, A.G.; Babor, R.; MacCormick, A.D. Five-year results after laparoscopic sleeve gastrectomy: A prospective study. Surg. Obes. Relat. Dis. 2015, 11, 518–524. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, K.G., Jr.; Long, S.D.; Swanson, M.S.; Brown, B.M.; Morris, P.; Dohm, G.L.; Pories, W.J. The gastric bypass operation reduces the progression and mortality of non-insulin-dependent diabetes mellitus. J. Gastrointest. Surg. 1997, 1, 213–220. [Google Scholar] [CrossRef]
- MacLean, L.D.; Rhode, B.M.; Nohr, C.W. Late outcome of isolated gastric bypass. Ann. Surg. 2000, 231, 524–528. [Google Scholar] [CrossRef] [PubMed]
- Marceau, P.; Biron, S.; Hould, F.-S.; Lebel, S.; Marceau, S.; Lescelleur, O.; Biertho, L.; Simard, S. Duodenal switch: Long-term results. Obes. Surg. 2007, 17, 1421–1430. [Google Scholar] [CrossRef] [PubMed]
- Marceau, P.; Biron, S.; Hould, F.-S.; Lebel, S.; Marceau, S.; Lescelleur, O.; Biertho, L.; Simard, S. Duodenal switch improved standard biliopancreatic diversion: A retrospective study. Surg. Obes. Relat. Dis. 2009, 5, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Marceau, P.; Biron, S.; Marceau, S.; Hould, F.S.; Lebel, S.; Lescelleur, O.; Biertho, L.; Simard, S.; Kral, J.G. Long-Term Metabolic Outcomes 5 to 20 Years After Biliopancreatic Diversion. Obes. Surg. 2015, 25, 1584–1593. [Google Scholar] [CrossRef] [PubMed]
- Marsk, R.; Näslund, E.; Freedman, J.; Tynelius, P.; Rasmussen, F. Bariatric surgery reduces mortality in Swedish men. Br. J. Surg. 2010, 97, 877–883. [Google Scholar] [CrossRef] [PubMed]
- McPhee, J.; Khlyavich Freidl, E.; Eicher, J.; Zitsman, J.L.; Devlin, M.J.; Hildebrandt, T.; Sysko, R. Suicidal Ideation and Behaviours Among Adolescents Receiving Bariatric Surgery: A Case-Control Study. Eur. Eat. Disord. Rev. 2015, 23, 517–523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitchell, J.E.; Lancaster, K.L.; Burgard, M.A.; Howell, L.M.; Krahn, D.D.; Crosby, R.D.; Wonderlich, S.A.; Gosnell, B.A. Long-term follow-up of patients’ status after gastric bypass. Obes. Surg. 2001, 11, 464–468. [Google Scholar] [CrossRef] [PubMed]
- Näslund, E.; Granström, L.; Stockeld, D.; Backman, L. Marlex Mesh Gastric Banding: A 7–12 Year Follow-up. Obes. Surg. 1994, 4, 269–273. [Google Scholar] [CrossRef] [PubMed]
- Näslund, E.; Backman, L.; Granström, L.; Stockeld, D. Does the Size of the Upper Pouch Affect Weight Loss after Vertical Banded Gastroplasty. Obes. Surg. 1995, 5, 378–381. [Google Scholar] [CrossRef] [PubMed]
- Nocca, D.; Krawczykowsky, D.; Bomans, B.; Noël, P.; Picot, M.C.; Blanc, P.M.; de Seguin de Hons, C.; Millat, B.; Gagner, M.; Monnier, L.; et al. A prospective multicenter study of 163 sleeve gastrectomies: Results at 1 and 2 years. Obes. Surg. 2008, 18, 560–565. [Google Scholar] [CrossRef] [PubMed]
- Obeid, N.R.; Malick, W.; Concors, S.J.; Fielding, G.A.; Kurian, M.S.; Ren-Fielding, C.J. Long-term outcomes after Roux-en-Y gastric bypass: 10- to 13-year data. Surg. Obes. Relat. Dis. 2016, 12, 11–20. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, P.E.; MacDonald, L.; Anderson, M.; Brennan, L.; Brown, W.A. Long-term outcomes after bariatric surgery: Fifteen-year follow-up of adjustable gastric banding and a systematic review of the bariatric surgical literature. Ann. Surg. 2013, 257, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Omalu, B.I.; Ives, D.G.; Buhari, A.M.; Lindner, J.L.; Schauer, P.R.; Wecht, C.H.; Kuller, L.H. Death rates and causes of death after bariatric surgery for Pennsylvania residents, 1995 to 2004. Arch. Surg. 2007, 142, 923–928. [Google Scholar] [CrossRef] [PubMed]
- Peeters, A.; O’Brien, P.E.; Laurie, C.; Anderson, M.; Wolfe, R.; Flum, D.; MacInnis, R.J.; English, D.R.; Dixon, J. Substantial intentional weight loss and mortality in the severely obese. Ann. Surg. 2007, 246, 1028–1033. [Google Scholar] [CrossRef] [PubMed]
- Pekkarinen, T.; Koskela, K.; Huikuri, K.; Mustajoki, P. Long-term Results of Gastroplasty for Morbid Obesity: Binge-Eating as a Predictor of Poor Outcome. Obes. Surg. 1994, 4, 248–255. [Google Scholar] [CrossRef] [PubMed]
- Pories, W.J.; MacDonald, K.G., Jr.; Flickinger, E.G.; Dohm, G.L.; Sinha, M.K.; Barakat, H.A.; May, H.J.; Khazanie, P.; Swanson, M.S.; Morgan, E.; et al. Is type II diabetes mellitus (NIDDM) a surgical disease? Ann. Surg. 1992, 215, 633–642; discussion 643. [Google Scholar] [CrossRef] [PubMed]
- Pories, W.J.; Swanson, M.S.; MacDonald, K.G.; Long, S.B.; Morris, P.G.; Brown, B.M.; Barakat, H.A.; de Ramon, R.A.; Israel, G.; Dolezal, J.M.; et al. Who would have thought it? An operation proves to be the most effective therapy for adult-onset diabetes mellitus. Ann. Surg. 1995, 222, 339–350; discussion 350–352. [Google Scholar] [CrossRef] [PubMed]
- Powers, P.S.; Boyd, F.; Blair, C.R.; Stevens, B.; Rosemurgy, A. Psychiatric Issues in Bariatric Surgery. Obes. Surg. 1992, 2, 315–325. [Google Scholar] [CrossRef] [PubMed]
- Powers, P.S.; Rosemurgy, A.; Boyd, F.; Perez, A. Outcome of gastric restriction procedures: Weight, psychiatric diagnoses, and satisfaction. Obes. Surg. 1997, 7, 471–477. [Google Scholar] [CrossRef] [PubMed]
- Rawlins, L.; Rawlins, M.P.; Brown, C.C.; Schumacher, D.L. Sleeve gastrectomy: 5-year outcomes of a single institution. Surg. Obes. Relat. Dis. 2013, 9, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Van Rutte, P.W.; Smulders, J.F.; de Zoete, J.P.; Nienhuijs, S.W. Outcome of sleeve gastrectomy as a primary bariatric procedure. Br. J. Surg. 2014, 101, 661–668. [Google Scholar] [CrossRef] [PubMed]
- Shah, K.; Johnny Nergard, B.; Stray Frazier, K.; Geir Leifsson, B.; Aghajani, E.; Gislason, H. Long-term effects of laparoscopic Roux-en-Y gastric bypass on metabolic syndrome in patients with morbid obesity. Surg. Obes. Relat. Dis. 2016, 12, 1449–1456. [Google Scholar] [CrossRef] [PubMed]
- Sieber, P.; Gass, M.; Kern, B.; Peters, T.; Slawik, M.; Peterli, R. Five-year results of laparoscopic sleeve gastrectomy. Surg. Obes. Relat. Dis. 2014, 10, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Skroubis, G.; Karamanakos, S.; Sakellaropoulos, G.; Panagopoulos, K.; Kalfarentzos, F. Comparison of early and late complications after various bariatric procedures: Incidence and treatment during 15 years at a single institution. World J. Surg. 2011, 35, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.C.; Goodman, G.N.; Edwards, C.B. Roux-en-Y Gastric Bypass: A 7-year Retrospective Review of 3,855 Patients. Obes. Surg. 1995, 5, 314–318. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.C.; Edwards, C.B.; Goodman, G.N.; Halversen, R.C.; Simper, S.C. Open vs laparoscopic Roux-en-Y gastric bypass: Comparison of operative morbidity and mortality. Obes. Surg. 2004, 14, 73–76. [Google Scholar] [CrossRef] [PubMed]
- Suter, M.; Calmes, J.M.; Paroz, A.; Giusti, V. A 10-year experience with laparoscopic gastric banding for morbid obesity: High long-term complication and failure rates. Obes. Surg. 2006, 16, 829–835. [Google Scholar] [CrossRef] [PubMed]
- Suter, M.; Donadini, A.; Romy, S.; Demartines, N.; Giusti, V. Laparoscopic Roux-en-Y gastric bypass: Significant long-term weight loss, improvement of obesity-related comorbidities and quality of life. Ann. Surg. 2011, 254, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Svenheden, K.E.; Akesson, L.A.; Holmdahl, C.; Näslund, I. Staple disruption in vertical banded gastroplasty. Obes. Surg. 1997, 7, 136–138. [Google Scholar] [CrossRef] [PubMed]
- Tao, W.; Plecka-Östlund, M.; Lu, Y.; Mattsson, F.; Lagergren, J. Causes and risk factors for mortality within 1 year after obesity surgery in a population-based cohort study. Surg. Obes. Relat. Dis. 2015, 11, 399–405. [Google Scholar] [CrossRef] [PubMed]
- Thereaux, J.; Corigliano, N.; Poitou, C.; Oppert, J.M.; Czernichow, S.; Bouillot, J.L. Five-year weight loss in primary gastric bypass and revisional gastric bypass for failed adjustable gastric banding: Results of a case-matched study. Surg. Obes. Relat. Dis. 2015, 11, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Van de Weijgert, E.J.; Ruseler, C.H.; Elte, J.W. Long-term follow-up after gastric surgery for morbid obesity: Preoperative weight loss improves the long-term control of morbid obesity after vertical banded gastroplasty. Obes. Surg. 1999, 9, 426–432. [Google Scholar] [CrossRef] [PubMed]
- Werling, M.; Fändriks, L.; Björklund, P.; Maleckas, A.; Brandberg, J.; Lönroth, H.; Le Roux, C.W.; Olbers, T. Long-term results of a randomized clinical trial comparing Roux-en-Y gastric bypass with vertical banded gastroplasty. Br. J. Surg. 2013, 100, 222–230. [Google Scholar] [CrossRef] [PubMed]
- Yale, C.E. Gastric surgery for morbid obesity. Complications and long-term weight control. Arch. Surg. 1989, 124, 941–946. [Google Scholar] [CrossRef] [PubMed]
- Zitsman, J.L.; DiGiorgi, M.F.; Fennoy, I.; Kopchinski, J.S.; Sysko, R.; Devlin, M.J. Adolescent laparoscopic adjustable gastric banding (LAGB): Prospective results in 137 patients followed for 3 years. Surg. Obes. Relat. Dis. 2015, 11, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.H.; Stoll, C.R.; Song, J.; Varela, J.E.; Eagon, C.J.; Colditz, G.A. The effectiveness and risks of bariatric surgery: An updated systematic review and meta-analysis, 2003–2012. JAMA Surg. 2013, 149, 275–287. [Google Scholar] [CrossRef] [PubMed]
- Rottenstreich, A.; Keidar, A.; Yuval, J.B.; Abu-Gazala, M.; Khalaileh, A.; Elazary, R. Outcome of bariatric surgery in patients with type 1 diabetes mellitus: Our experience and reviewof the literature. Surg. Endosc. 2016, 30, 5428–5433. [Google Scholar] [CrossRef] [PubMed]
- Balla, A.; Batista Rodríguez, G.; Corradetti, S.; Balagué, C.; Fernández-Ananín, S.; Targarona, E.M. Outcomes after bariatric surgery according to large databases: A systematic review. Langenbecks Arch. Surg. 2017. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Available online: http://www.who.int/mental_health/prevention/suicide/suicideprevent/en/ (assessed on 6 September 2017).
- Adams, T.D.; Mehta, T.S.; Davidson, L.E.; Hunt, S.C. All-Cause and Cause-Specific Mortality Associated with Bariatric Surgery: A Review. Curr. Atheroscler. Rep. 2015, 17, 74. [Google Scholar] [CrossRef] [PubMed]
- Roizblatt, A.; Roizblatt, D.; Soto-Aguilar, B.F. Suicide risk after bariatric surgery. Rev. Med. Chile 2016, 144, 1171–1176. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, I.; Sogg, S.; Perna, F.M. Behavioral and psychological care in weight loss surgery: Best practice update. Obesity 2009, 17, 880–884. [Google Scholar] [CrossRef] [PubMed]
- Padwal, R.S.; Klarenbach, S.W.; Wang, X.; Sharma, A.M.; Karmali, S.; Birch, D.W.; Majumdar, S.R. A simple prediction rule for all-cause mortality in a cohort eligible for bariatric surgery. JAMA Surg. 2013, 148, 1109–1115. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author and Year | Study Type | Sample Size (n) | Mortality (n) | Suicide (n) | Mean Age | % Male | % Female | Mean BMI | Procedure | Country | Longest Follow-Up (Month) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Aarts et al. 2014 [24] | Prospective Cohort Study | 201 | 6 | 1 | 37 | 0.23 | 0.77 | 45.6 | Laparoscopic adjustable gastric banding | The Netherlands | 216 |
| 2 | Adams et al. 2007 [25] | Retrospective Cohort Study | 9949 | 288 | 21 | 39.3 | 0.14 | 0.86 | 44.9 | Roux- En-Y Gastric Bypass | USA | 216 |
| 3 | Adams et al. 2012 [26] | Prospective Cohort Study | 1156 | 12 | 4 | 42.5 | 0.18 | 0.82 | 45.9 | Roux- En-Y Gastric Bypass | USA | 72 |
| 4 | Arapis et al. 2017 [27] | Prospective Cohort Study | 897 | 6 | 1 | 39.5 | 0.13 | 0.87 | 39.5 | Laproscopic adjustable gastric banding | France | 228 |
| 5 | Arman et al. 2016 [28] | Prospective Cohort Study | 106 | 2 | 1 | 38.5 | 0.26 | 0.74 | 38.5 | Laproscopic Sleeve Gastrectomy | Belgium | 140 |
| 6 | Biertho et al. 2010 [29] | Retrospective Cohort Study | 810 | 25 | 5 | 41.1 | 0.21 | 0.79 | 44.2 | Biliopancreatic diversion with duodenal switch | Canada | 201 |
| 7 | Bolckmans et al. 2016 [30] | Retrospective Cohort Study | 153 | 9 | 1 | 40.6 | 0.16 | 0.84 | 46.4 | Biliopancreatic diversion with duodenal switch | Belgium | 135 |
| 8 | Busetto et al. 2007 [31] | Case control study | 821 | 8 | 1 | 38.2 | 0.24 | 0.76 | 48.6 | Laproscopic adjustable gastric banding | Italy | 120 |
| 9 | Busetto et al. 2014 [32] | Prospective Cohort Study | 318 | 15 | 1 | 38.6 | 0.18 | 0.82 | 46.7 | Laproscopic adjustable gastric banding | Italy | 120 |
| 10 | Cadiere et al. 2011 [33] | Retrospective Cohort Study | 470 | 1 | 1 | 40 | 0.166 | 0.834 | NA | Laproscopic gastric bypass | Belgium | 66 |
| 11 | Capella et al. 1996 [34] | Prospective Cohort Study | 888 | 8 | 3 | 37 | 0.178 | 0.822 | 52 | Vertical banded gastroplasty/Vertical banded gastroplasty-Roux-en-y gastric bypass | USA | 60 |
| 12 | Carelli et al. 2010 [35] | Retrospective Cohort Study | 2909 | 10 | 1 | NA | 0.32 | 0.68 | 45.27 | Laproscopic adjustable gastric banding | USA | 60 |
| 13 | Christou et al. 2006 [36] | Retrospective Cohort Study | 272 | 8 | 2 | 42 | 0.18 | 0.82 | 48.1 | Roux- En-Y Gastric Bypass | Canada | NA |
| 14 | Cobourn et al. 2013 [37] | Retrospective Cohort Study | 2815 | 9 | 1 | 43 | 0.18 | 0.82 | 44.6 | Laproscopic Adjustable Gastric Banding | Canada | 60 |
| 15 | Diniz et al. 2013 [38] | Prospective Cohort Study | 248 | 9 | 2 | 39.7 | 0.25 | 0.75 | 53 | Roux- En-Y Gastric Bypass | Brazil | NA |
| 16 | Goldfeder et al. 2006 [39] | Retrospective Cohort Study | 107 | 107 | 1 | NA | NA | NA | NA | NA | USA | NA |
| 17 | Girbsholt et al. 2016 [40] | Retrospective Cohort Study | 9895 | 91 | 10 | 40.2 | 0.217 | 0.783 | 46 | Roux- En-Y Gastric Bypass | Denmark | 50 |
| 18 | Higa et al. 2000 [41] | Prospective Cohort Study | 1040 | 5 | 1 | NA | 0.174 | 0.826 | 47.8 | Roux- En-Y Gastric Bypass | USA | 12 |
| 19 | Himpens et al. 2011 [42] | Prospective Cohort Study | 82 | 3 | 1 | 50 | 0.1 | 0.9 | 41.57 | Laproscopic Adjustable Gastric Banding | Belgium | NA |
| 20 | Himpens et al. 2012 [43] | Prospective Cohort Study | 77 | 2 | 1 | 38.9 | 0.2 | 0.8 | 40.3 | Laproscopic Roux-En-Y Gastric bypass | Belgium | 112 |
| 21 | Kelles et al. 2014 [44] | Prospective Cohort Study | 4344 | 82 | 8 | 34.9 | 0.21 | 0.79 | 42 | Roux- En-Y Gastric Bypass | Brazil | 120 |
| 22 | Kral et al. 1993 [45] | Prospective Cohort Study | 69 | 3 | 1 | 38 | 0.18 | 0.82 | 47 | Vertical Banded Gastroplasty | Sweden | 60 |
| 23 | Laggeros et al. 2017 [46] | Retrospective Cohort Study | 22,539 | NA | 17 | 41.3 | 0.753 | 0.247 | NA | NA | Sweden | 26 |
| 24 | Lemanu et al. 2015 [47] | Prospective Cohort Study | 96 | 3 | 1 | 46.9 | 0.182 | 0.818 | 50.7 | Laproscopic Sleeve Gastrectomy | New Zealand | 60 |
| 25 | Macdonald et al. 1997 [48] | Prospective Cohort Study | 154 | 14 | 1 | 41.9 | 0.234 | 0.766 | 50.6 | Roux- En-Y Gastric Bypass | USA | 132 |
| 26 | Maclean et al. 2000 [49] | Prospective Cohort Study | 274 | 3 | 1 | NA | NA | NA | 43.2 | Isolated Gastric Bypass | Canada | NA |
| 27 | Marceau et al. 2007 [50] | Prospective Cohort Study | 1423 | 67 | 6 | 40.1 | NA | NA | 51.5 | Duodenal Switch | Canada | 180 |
| 28 | Marceau et al. 2009 [51] | Prospective Cohort Study | 686 | 49 | 3 | NA | NA | NA | 48.3 | Biliopancreatic diversion with distal gastrectomy/Biliopancreatic diversion with duodenal switch | Canada | 120 |
| 29 | Marceau et al. 2015 [52] | Prospective Cohort Study | 2615 | 123 | 9 | 42 | 0.307 | 0.693 | 52 | Biliopancreatic diversion | Canada | NA |
| 30 | Marsk et al. 2010 [53] | Case control study | 1216 | 43 | 4 | NA | 1 | 0 | NA | NA | Sweden | NA |
| 31 | Mcphee et al. 2015 [54] | Case control study | 206 | 2 | 2 | NA | NA | NA | NA | Laproscopic sleeve gastrectomy/Laproscopic adjustable gastric banding | USA | NA |
| 32 | Mitchell et al. 2001 [55] | Prospective Cohort Study | 78 | 8 | 1 | 56.8 | 0.17 | 0.83 | 43.8 | Gastric bypass | USA | 180 |
| 33 | Naslund et al. 1994 [56] | Prospective Cohort Study | 37 | 5 | 2 | 37 | 0.18 | 0.82 | 45.5 | Gastric banding | Sweden | 120 |
| 34 | Naslund et al. 1995 [57] | Prospective Cohort Study | 158 | 3 | 1 | 39.3 | 0.16 | 0.84 | 44.7 | Vertical Banded Gastroplasty | Sweden | NA |
| 35 | Nocca et al. 2007 [58] | Prospective Cohort Study | 163 | 1 | 1 | 41 | 0.32 | 0.68 | 45.9 | Laproscopic Sleeve Gastrectomy | France | 24 |
| 36 | N Obeid et al. 2015 [59] | Prospective Cohort Study | 328 | 9 | 2 | 41.4 | 0.17 | 0.83 | 47.5 | Roux- En-Y Gastric Bypass | USA | 120 |
| 37 | O’Brien et al. 2013 [60] | Prospective Cohort Study | 3227 | 4 | 1 | 47.1 | 0.22 | 0.78 | 43.8 | Laproscopic Adjustable Gastric Banding | Australia | 120 |
| 38 | Omalu et al. 2007 [61] | Retrospective Cohort Study | 16,683 | 440 | 16 | 48 | 0.177 | 0.823 | NA | NA | USA | NA |
| 39 | Peeters et al. 2007 [62] | Cohort study | 966 | 4 | 1 | 47 | 0.23 | 0.77 | 44.9 | Laproscopic Adjustable Gastric Banding | Australia | NA |
| 40 | Pekkarinen et al. 1994 [63] | Prospective Cohort Study | 33 | 3 | 1 | 36 | 0.33 | 0.67 | 50 | Vertical Banded Gastroplasty | Finland | NA |
| 41 | Pories et al. 1992 [64] | Prospective Cohort Study | 515 | 23 | 3 | NA | 0.15 | 0.85 | NA | Greenville Gastric Bypass | USA | 132 |
| 42 | Pories et al. 1995 [65] | Prospective Cohort Study | 608 | 34 | 3 | 37.3 | 0.168 | 0.832 | NA | Greenville Gastric Bypass | USA | 168 |
| 43 | Powers et al. 1992 [66] | Prospective Cohort Study | 100 | 2 | 1 | 38.8 | 0.15 | 0.85 | 47 | Vertical Banded Gastroplasty | USA | NA |
| 44 | Powers et al. 1007 [67] | Prospective Cohort Study | 131 | 5 | 1 | 39.4 | 0.15 | 0.85 | NA | NA | USA | NA |
| 45 | Rawlins et al. 2012 [68] | Prospective Cohort Study | 55 | 2 | 1 | 44 | 0.3 | 0.7 | 65 | Laproscopic Sleeve Gastrectomy | USA | 60 |
| 46 | Rutte et al. 2014 [69] | Prospective Cohort Study | 1041 | 6 | 1 | 42.5 | 0.29 | 0.71 | 44.3 | Sleeve gastrectomy | The Netherlands | 60 |
| 47 | Shah et al. 2016 [70] | Prospective Cohort Study | 3795 | 14 | 1 | 42.4 | 0.21 | 0.79 | 40.9 | Roux- En-Y Gastric Bypass | Norway | 60 |
| 48 | Sieber et al. 2013 [71] | Prospective Cohort Study | 68 | 1 | 1 | 43.1 | 0.22 | 0.78 | 43 | Laproscopic Sleeve Gastrectomy | Switzerland | NA |
| 49 | Skroubis et al. 2010 [72] | Prospective Cohort Study | 1162 | 21 | 2 | 36.3 | 0.26 | 0.74 | 53 | Vertical Banded Gastroplasty/Laproscopic sleeve gastrectomy/Roux-en-y gastric bypass/Biliopancreatic diversion | Greece | NA |
| 50 | Smith et al. 1995 [73] | Retrospective Cohort Study | 3855 | 24 | 2 | NA | 0.11 | 0.89 | NA | Roux- En-Y Gastric Bypass | USA | 84 |
| 51 | Smith et al. 2004 [74] | Retrospective Cohort Study | 779 | 2 | 1 | 39.3 | NA | NA | 40.32 | Roux- En-Y Gastric Bypass | USA | 29 |
| 52 | Suter et al. 2006 [75] | Prospective Cohort Study | 317 | 5 | 1 | 38 | 0.136 | 0.864 | 43.5 | Laproscopic Adjustable Gastric Banding | Switzerland | 84 |
| 53 | Suter et al. 2011 [76] | Prospective Cohort Study | 379 | 9 | 2 | 39.4 | 0.26 | 0.74 | 46.3 | Roux- En-Y Gastric Bypass | Switzerland | 84 |
| 54 | Svenheden et al. 1997 [77] | Prospective Cohort Study | 95 | 2 | 1 | NA | 0.21 | 0.79 | 42.5 | Vertical Banded Gastroplasty | Sweden | 24 |
| 55 | Tao et al. 2014 [78] | Retrospective Cohort Study | 22,487 | 85 | 1 | NA | NA | NA | NA | Gastric bypass/Gastric Banding/Vertical Banded Gastroplasty/Laproscopic Sleeve Gastrectomy/Billiopancreatic Diversion with duodenal Switch/Jejunoileal bypass | Sweden | 12 |
| 56 | Thereaux et al. 2014 [79] | Prospective Cohort Study | 330 | 7 | 1 | 43.4 | 0.089 | 0.911 | 46.9 | Laproscopic Roux-En-Y Gastric bypass | France | 60 |
| 57 | Tindle et al. 2010 [13] | Prospective Cohort Study | 16,683 | NA | 31 | 48 | 0.177 | 0.823 | NA | Various | USA | NA |
| 58 | Van de Weijgert et al. 1999 [80] | Prospective Cohort Study | 153 | 10 | 1 | 34 | 0.131 | 0.869 | 46 | Roux-en-Y Gastric Bypass/Vertical Banded Gastroplasty | The Netherlands | 168 |
| 59 | Werling et al. 2012 [81] | Randomized Controlled Study | 82 | 2 | 1 | 44.9 | 0.28 | 0.72 | 42.1 | Roux-en-Y Gastric Bypass/Vertical Banded Gastroplasty | Sweden | 120 |
| 60 | Yale 1989 [82] | Prospective Cohort Study | 537 | 9 | 5 | 36 | 0.162 | 0.838 | 46.8 | Roux-en-Y GastroJejunostomy/Vertical Banded Gastroplasty/Gastrogastrotomy | USA | 60 |
| 61 | Zitsman et al. 2014 [83] | Prospective Cohort Study | 137 | 2 | 1 | 17 | 0.31 | 0.69 | 48.3 | Laproscopic Adjustable Gastric Banding | USA | 60 |
| Moderators | No. of Studies Used | Slope | Standard Error | Lower Limit (95% CI) | Upper Limit (95% CI) | Z Value | p Value |
|---|---|---|---|---|---|---|---|
| Mean Age | 50 | −0.02370 | 0.03244 | −0.08729 | 0.03988 | −0.73065 | 0.46499 |
| Proportion of males | 54 | −0.01258 | 0.01069 | −0.03353 | 0.00838 | −1.17621 | 0.23951 |
| Mean BMI | 49 | 0.008284 | 0.03481 | 0.01461 | 0.15107 | 2.37980 | 0.01732 * |
| Longest follow-up interval | 44 | 0.01177 | 0.00271 | 0.00646 | 0.01708 | 4.34545 | 0.00001 * |
| Predictor | No. of Studies | Pooled Prevalence (%) | 95% CI | p-Value in between Group Comparison |
|---|---|---|---|---|
| Restrictive procedures | 25 | 1.4 | 0.9–2.3 | 0.309 |
| Malabsorptive procedures | 24 | 2.4 | 1.8–3.3 | |
| Restrictive and/or Malabsorptive procedures | 6 | 1.6 | 0.6–4.1 | |
| Unspecified procedures | 6 | 2.5 | 0.6–9.2 | |
| Overall: | 61 | 2.1 | 1.6–2.7 | |
| Continent—North America | 28 | 2.1 | 1.5–2.9 | 0.380 |
| Continent—Europe | 28 | 1.7 | 1.1–2.7 | |
| Continent—South America | 2 | 2.4 | 1.3–4.5 | |
| Continent—Oceania | 3 | 0.5 | 0.1–3.1 | |
| Overall: | 61 | 2.0 | 1.6–2.5 |
| Predictor | No. of Studies | Pooled Prevalence (%) | 95% CI | p-Value in between Group Comparison |
|---|---|---|---|---|
| Restrictive procedures | 25 | 0.5 | 0.3–0.8 | 0.131 |
| Malabsorptive procedures | 24 | 0.3 | 0.2–0.4 | |
| Restrictive and/or Malabsorptive procedures | 6 | 0.3 | 0.1–1.0 | |
| Unspecified procedures | 6 | 0.2 | 0.1–0.3 | |
| Overall: | 61 | 0.3 | 0.2–0.4 | |
| Continent—North America | 28 | 0.3 | 0.2–0.5 | 0.878 |
| Continent—Europe | 28 | 0.4 | 0.2–0.6 | |
| Continent—South America | 2 | 0.3 | 0.1–1.4 | |
| Continent—Oceania | 3 | 0.1 | 0–1.1 | |
| Overall: | 61 | 0.3 | 0.3–0.5 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, R.B.C.; Zhang, M.W.B.; Ho, R.C.M. Prevalence of All-Cause Mortality and Suicide among Bariatric Surgery Cohorts: A Meta-Analysis. Int. J. Environ. Res. Public Health 2018, 15, 1519. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15071519
Lim RBC, Zhang MWB, Ho RCM. Prevalence of All-Cause Mortality and Suicide among Bariatric Surgery Cohorts: A Meta-Analysis. International Journal of Environmental Research and Public Health. 2018; 15(7):1519. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15071519
Chicago/Turabian StyleLim, Russell B.C., Melvyn W.B. Zhang, and Roger C.M. Ho. 2018. "Prevalence of All-Cause Mortality and Suicide among Bariatric Surgery Cohorts: A Meta-Analysis" International Journal of Environmental Research and Public Health 15, no. 7: 1519. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15071519