Implementing Supported Employment. Lessons from the Making IPS Work Project

Abstract
:1. Introduction
2. Materials and Methods
2.1. Making IPS Work Project
2.2. Recording of Quantitative Data
2.3. Sources of Qualitative Evidence
3. Results
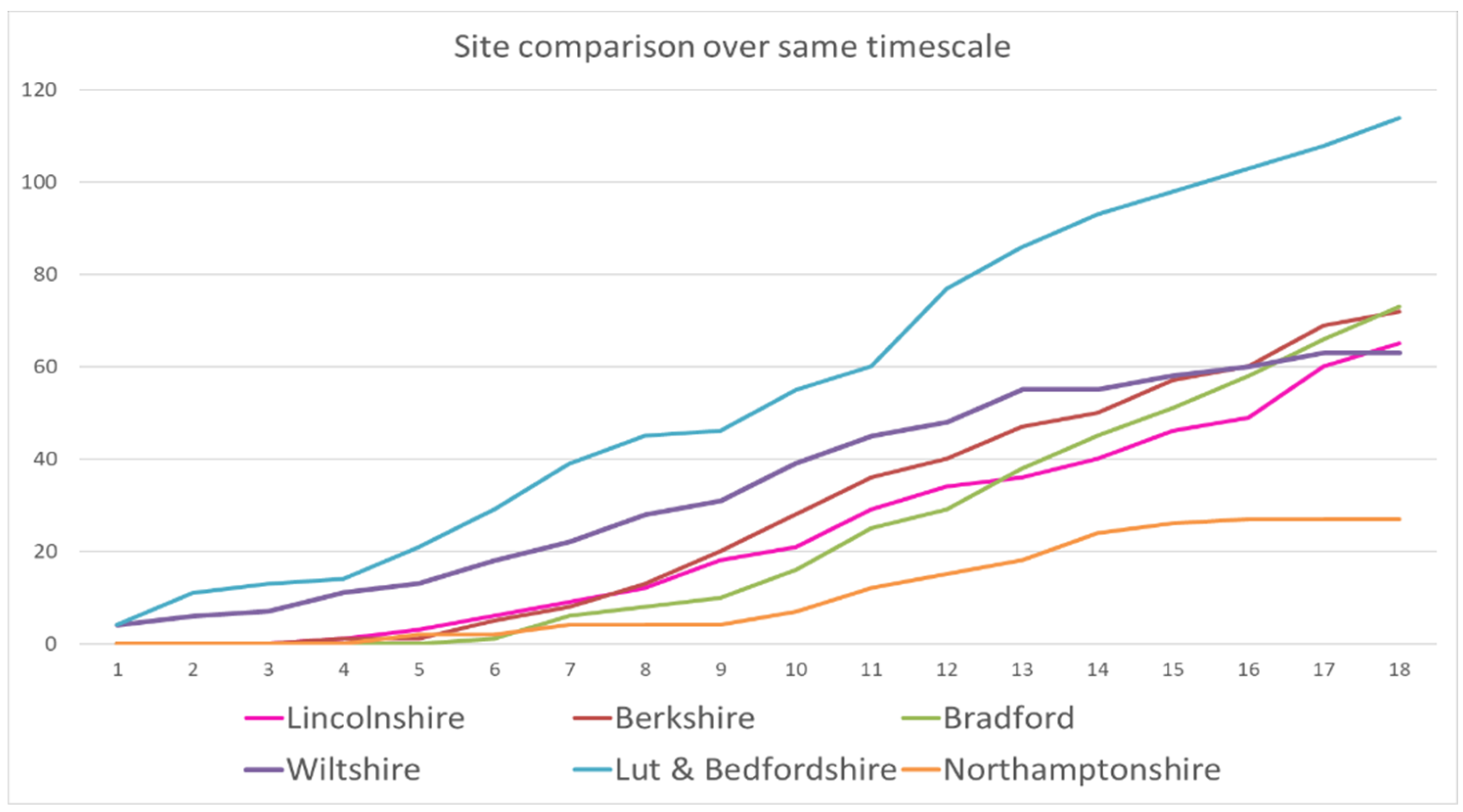
3.1. Employment Outcomes
3.2. Fidelity Measures
3.3. Qualitative Outcomes
3.3.1. The Distinctiveness of IPS
“Having [an Employment Specialist] in place has helped; we knew it was going to make a massive difference… helps ease burden, freed a lot of time. Eight out of ten clients who try the traditional job centre approach fail. The difference is in the practical help in IPS; clients would struggle to go to find jobs on their own; the help they get is great, practical, CVs etc had one client who calmed down a lot under [Employment Specialists] support; he established good relationships, he has credibility with them and with us as staff.”(Care-coordinator)
“Having a job gives me a reason to live. When working, I can show ‘I am like you, I am like others’. Especially because of the stigma in our community. Work is a lifesaver. It’s not the money, it’s therapeutic. You need a structure, rather than days in front of the X-box, you need to get out. I’m in control, but [Employment Specialist] is there to support me if I need him.”(Client referred to Employment Specialist)
“Dealing with your own ill-health is hard enough. Getting into work is another big battle. I went for jobs but got nowhere on my own through the universal job centre. On your own, you don’t know if you are coming or going. My condition means I can only take in so much, it’s the stress that gets you, lack of sleep. I need structure.”(Client referred to Employment Specialist)
“I’ve got a job as a kitchen assistant. I didn’t want to be out in public. I would never have considered something like that—me in a kitchen? Never worked in one before, thought I might spill everything. XXX said try it, that working with food can be therapeutic. I’d never thought of that. He gave me the confidence to apply. It’s perfect hours and fits with the kids and it’s working out really well.”(Client referred to Employment Specialist)
“They gave me a leaflet, and I read it. You need to realise that I need written information in order to absorb facts. The leaflet was the most important thing that sold it. There were bullet points, it was practical, it said the service can help with this and this. It was in black and white in simple English. And it was in my pocket and gave me a boost. It led me to say to myself: ‘OK, now I can do things’.”(Client referred to Employment Specialist)
“This service? It’s got to carry on!”(Client referred to Employment Specialist)
3.3.2. Strengths of IPS Workers
“The Employment Specialist was great. Inspiring, passionate but reacts to emotions, flexible… To be good, he has to be up on mental health issues and I know he is—some people are really conservative… Has to have the right personality, because even if you don’t get a job, you can benefit from the process of having someone like [the employment specialist]”(Client referring to the employment specialist).
“…trust is a big issue. A few months ago, my CPN thought I was ready to work, and I was told there was a person who could help. I didn’t believe it.”(Client referring to the employment specialist).
“[Employment specialist] came to meet me five months ago, along with my care-coordinator, and I thought ‘I’m not sure about this’. I thought it would be the same experience… fruitless. But there was no pressure on me and nothing to lose.”(Client referring to the employment specialist)
“When I met [Employment Specialist], it was chilled out, in a coffee shop. We slowly talked about the situation and met a week later. I could tell that he saw me as a person and would ask ‘are you ready?’.”(Client referring to the employment specialist)
“He gave me some options. I needed digest it all. XXX helped me with filling out applications. A burden was lifted off my shoulders, I didn’t know even how to say ‘dear sir or madam’, it would have been Mission Impossible.”(Client referring to the employment specialist)
“He said it was up to me whether to post it, as he knew I might change my mind, and didn’t want to pressure me. He even phoned me on the Monday morning before the interview and guided me, got me to keep it simple, got me to practice over and over again. This was important, it got me the job. He gave me bullet points, kept it simple, he understands how I take things in. If it wasn’t for [Employment Specialist] I would not have got it, I would have given up. He said be yourself.”(Client referring to the employment specialist)
“[Employment specialist] knows if you’ve had a bad day. He is more of a friend than a professional. The service is better than the job centre, there’s more of a connection. [Employment specialist] understands me. He has a rapport, he creates trust and has empathy. He asks me how I feel and didn’t just urge me to apply for hundreds of jobs”.(Client referring to the employment specialist)
“…like a great taxi driver. You don’t want to sit with a smelly taxi driver. I look forward to seeing him. He has helped me get up in the morning. He speaks the lingo and has cred, knows the jargon…”(Client referring to the employment specialist)
3.3.3. The Value of Employment Specialists for Community Mental Health Teams
“We try to explain things really well in initial meetings—dispel myths to the service users and seek to reassure them and provide a sense of hope. It’s all about building and maintaining relationships.”(Employment specialist)
“…less anxiety about the model (after time), become a bit more flexible concerning attitudes to paperwork—the [IPS] ‘review’ helped us to see flexibility inherent in model…Still need to educate care co-ordinations…get them into the discipline of seeing the benefits…”(Employment specialist)
“The team have done an incredible job in a short time. They’ve taken on board the model, which is the most important aspect…The targets seemed hard. I almost had a heart attack when I saw it. If we get over 40 I’d be pleased, I thought. 72 now! And this is incredible thinking of this area as a place of high unemployment and low growth. We’ve exceeded expectations—this has smashed where we were…”(Regional coordinator)
“In a client I am looking for an explicit reference to wanting to work, or I know the signs intuitively, if there’s discussion on where they go from here and what helps, if I see they want to be self-sustaining, or want to be busy… also have conversations sometimes with the Employment Specialist before mentioning it to client… I can rely on those conversations about how client is doing, for example a health visitor reported something to me and I can ask [Employment Specialist] to keep an eye on them. [The Employment Specialist] is there for the long haul. The service is a really effective antidepressant…but this is more than about just minimising challenges—it transforms lives”(Health professional)
3.3.4. Challenges to Implementation Fidelity
- Finding office space for the implementation manager and team supervisor
- Identifying resources to create IPS employment specialist posts
- Setting up internal referral systems from clinicians to employment specialists
- Dealing with separate health and social care systems
- Attempting to integrate or work in complementary ways with third sector employment support organisations.
“The team have done an incredible job in a short time. They’ve taken on board the model, which is the most important aspect…The targets seemed hard. I almost had a heart attack when I saw it. If we get over 40 I’d be pleased, I thought. 72 now! And this is incredible thinking of this area as a place of high unemployment, with low growth; We’ve exceeded expectations—this has smashed where we were…”(IPS coordinator)
3.3.5. Working across and Outside of the Mental Health Organisation
3.3.6. Sustaining the IPS Services
“Even if the project demonstrates great outcomes, there’s no guarantee the trust will be able to prioritise it”(Board Member)
4. Discussion
4.1. Context
4.2. Process
4.3. Outcomes
4.4. Limitations of the Evaluation
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| IPS | Individual Placement and Support |
| NHS | National Health Service |
| CCG | Clinical Commissioning Group |
| OT | Occupational Therapist |
| CMHT | Community Mental Health Team |
| CV | Curriculum Vitae |
| DWP | Department for Work and Pensions |
| NICE | The National Institute for Health and Care Excellence |
References
- Drake, R.; Bond, G.; Becker, D.R. Individual Placement and Support: An Evidence-Based Approach to Supported Employment. Evidence Based Practice Series; Oxford University Press: Oxford, UK, 2012. [Google Scholar]
- Modini, M.; Tan, L.; Brinchmann, B.; Wang, M.-J.; Killackey, E.; Glozier, N.; Mykletun, A.; Harvey, S.B. Supported employment for people with severe mental illness: Systematic review and meta-analysis of the international evidence. Br. J. Psychiatry 2016, 209, 14–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bond, G.R.; Drake, R.E.; Becker, D.R. Generalizability of the Individual Placement and Support (IPS) model of supported employment outside the US. World Psychiatry 2012, 11, 32–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carroll, C.; Patterson, M.; Wood, S.; Booth, A.; Rick, J.; Balain, S. A conceptual framework for implementation fidelity. Implement. Sci. 2007, 2, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lockett, H.; Waghorn, G.; Kydd, R.; Chant, D. Predictive validity of evidence-based practices in supported employment: A systematic review and meta-analysis. Ment. Health Rev. J. 2016, 21, 261–281. [Google Scholar] [CrossRef]
- Rinaldi, M.; Miller, L.; Perkins, R. Implementing the individual placement and support (IPS) approach for people with mental health conditions in England. Int. Rev. Psychiatry 2010, 22, 163–172. [Google Scholar] [CrossRef] [PubMed]
- Burns, T.; Catty, J.; Becker, T.; Drake, R.E.; Fioritti, A.; Knapp, M.; Lauber, C.; Rössler, W.; Tomov, T.; van Busschbach, J.; et al. The effectiveness of supported employment for people with severe mental illness: A randomized controlled trial in six European countries. Lancet 2007, 370, 1146–1152. [Google Scholar] [CrossRef]
- Menear, M.; Reinharz, D.; Corbière, M.; Houle, N.; Lanctôt, N.; Goering, P.; Goldner, E.M.; Kirsh, B.; Lecomte, T. Organizational analysis of Canadian supported employment programs for people with psychiatric disabilities. Soc. Sci. Med. 2011, 72, 1028–1035. [Google Scholar] [CrossRef] [PubMed]
- Fioritti, A.; Burns, T.; Hilarion, P.; van Weeghel, J.; Cappa, C.; Suñol, R. Individual Placement and Support in Europe. Psychiatr. Rehabil. J. 2014, 37, 123–128. [Google Scholar] [CrossRef] [PubMed]
- NHS England. Implementing the Five Year Forward View for Mental Health; NHS England: London, UK, 2015. [Google Scholar]
- NHS Benchmarking Network (2018). Available online: https://www.nhsbenchmarking.nhs.uk/community-mental-health-stocktake (accessed on 20 July 2018).
- Boardman, J.; Rinaldi, M. Difficulties in implementing supported employment for people with severe mental health problems. Br. J. Psychiatry 2013, 203, 247–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mueser, K.T.; Torrey, W.C.; Lynde, D.; Singer, P.; Drake, R.E. Implementing Evidence-Based Practices for People with Severe Mental Illness. Behav. Modif. 2003, 27, 387–411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Becker, D.R.; Drake, R.E.; Bond, G.R.; Nawaz, S.; Haslett, W.R.; Martinez, R.A. Best practices: A national mental health learning collaborative on supported employment. Psychiatr. Serv. 2011, 62, 704–706. [Google Scholar] [CrossRef] [PubMed]
- Centre for Mental Health. Implementing What Works: The Impact of the Individual Placement and Support Regional Trainer; Centre for Mental Health: London, UK, 2012. [Google Scholar]
- Bond, G.R.; McHugo, G.J.; Becker, D.R.; Rapp, C.A.; Whitely, R. Fidelity of Supported Employment: Lessons learned from the National Evidence-Based Practices Project. Psychiatr. Rehabil. J. 2008, 31, 300–305. [Google Scholar] [CrossRef] [PubMed]
- Frey, W.D.; Drake, R.E.; Bond, G.R.; Miller, A.L.; Goldman, H.H.; Salkever, D.S.; Holsenbeck, S. Mental Health Treatment Study: Final Report; Westat: Rockville, MD, USA, 2011. Available online: www.socialsecurity.gov/disability research/mentalhealth.htm (accessed on 20 July 2018).
- Becker, D.R.; Drake, R.E.; Bond, G.R. The IPS supported employment learning collaborative. Psychiatr. Rehabil. J. 2014, 37, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Bond, G.R.; Drake, R.E.; Becker, D.R.; Noel, V.A. The IPS Learning Community: A Longitudinal Study of Sustainment, Quality, and Outcome. Psychiatr. Serv. 2016, 67, 864–869. [Google Scholar] [CrossRef] [PubMed]
- NICE. Psychosis and Schizophrenia in Adults: Treatment and Management; NICE Clinical Guideline 178. guidance.nice.org.uk/cg178; National Institute for Health and Care Excellence: London, UK, 2014. [Google Scholar]
- NICE. Bipolar Disorder, Psychosis and Schizophrenia in Children and Young People; Quality Standard. nice.org.uk/guidance/qs102; National Institute for Health and Care Excellence: London, UK, 2015. [Google Scholar]
- NICE. Psychosis and Schizophrenia in Adults; Quality Standard. nice.org.uk/guidance/qs80; National Institute for Health and Care Excellence: London, UK, 2015. [Google Scholar]
- Brooks, H.; Pilgrim, D.; Rogers, A. Innovation in mental health services: What are the key components of success? Implement. Sci. 2011, 6, 120. [Google Scholar] [CrossRef] [PubMed]
- Department for Work and Pensions, Department of Health. Improving Lives. In The Future of Work, Health and Disability; Cm 9526; Her Majesty’s Stationery Office: London, UK, 2017. [Google Scholar]
- Social Exclusion Unit. Mental Health and Social Exclusion; Office of the Deputy Prime Minister: London, UK, 2004.
- NHS Confederation Mental Health Network, Centre for Mental Health. Supporting Recovery in Mental Health; NHS Confederation: London, UK, 2012. [Google Scholar]
- Department of Health. No Health without Mental Health: A Cross-Government Mental Health Outcomes Strategy for People of All Ages; Department of Health: London, UK, 2011.




{kind=link}
{kind=link}
{kind=link}
| Site | Start Date | Internal Resources | External Resources | Sustainability |
|---|---|---|---|---|
| Berkshire | 28 January 2015 | 2 IPS posts in Reading and Slough CMHTs. | None achieved | The 2 new posts continued after the grant period. |
| Lincolnshire | 28 January 2015 | Conversion of 2 existing supported employment posts to IPS. Team Leader post fulfilled by part-time senior occupational therapist. | None achieved | The 2 posts continued after the grant period, but the senior OT post disappeared when the postholder left. |
| Bradford | 28 January 2015 | Four posts created with internal investment of surplus and one post funded by salary released from seconded staff to grant-funded team leader post. | None achieved | The five posts and team leader continued after the grant period, but recurrent revenue funding was under threat and required matched disinvestment to become fully sustainable. |
| Wiltshire | 1 October 2015 | None required | The IPS team was fully funded by Wiltshire Council and Wiltshire Clinical Commissioning Group (CCG) | Wiltshire joint commissioning provided funding for a team leader and 5.5 employment specialists with a 3–5-year contract. |
| Bedfordshire and Luton | 28 September 2015 | Four posts in Luton created with internal resources (primarily the salaries released from the secondment of two members of staff to grant funded posts). Three posts in Bedfordshire already in existence. | None achieved | The Bedfordshire posts continued but as commissioners were unable to pick up funding for the Luton posts these were made redundant 6 months after the grant period ended. |
| Northamptonshire | 1 December 2015 | Salary of seconded staff member funded a post in the forensic service. An existing employment post within the Early Intervention Service provided a second IPS post. | The secondment of a post funded by an outside agency was added to the IPS team during the grant period | Although the seconded post ended, the trust continued to fund the team leader in addition to the forensic service post and early intervention post. |
| Trust | Visit 1 | Visit 2 | Visit 3 | Number of Interviews Undertaken | |||
|---|---|---|---|---|---|---|---|
| Staff | Service Users | Staff | Service Users | Staff | Service Users | ||
| Berkshire | 15 | 0 | 18 | 7 | 16 | 4 | 49 staff 11 service users |
| Lincolnshire | 9 | 5 | 9 | 4 | 11 | 7 | 22 staff 16 service users |
| Bradford | 12 | 0 | 17 | 3 | 13 | 3 | 42 staff 6 service users |
| Northamptonshire | 9 | 2 | 13 | 6 | 11 | 6 | 33 staff 14 service users |
| Wiltshire | 17 | 6 | 15 | 2 | 12 | 6 | 44 staff 14 service users |
| Luton and Bedfordshire | 16 | 0 | 14 | 4 | 15 | 0 | 45 staff 4 service users |
| Site | Referrals and Jobs Achieved |
|---|---|
| Berkshire | 240 referrals and 74 jobs achieved—31% success |
| Bradford | 193 referrals and 78 jobs achieved—40% |
| Lincolnshire | 170 referrals and 65 jobs achieved—38% |
| Luton & Bedfordshire | 264 referrals and 114 jobs achieved—43% |
| Northamptonshire | 139 referrals and 27 jobs achieved—19% |
| Wiltshire | 155 referrals and 63 jobs achieved—41% |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hutchinson, J.; Gilbert, D.; Papworth, R.; Boardman, J. Implementing Supported Employment. Lessons from the Making IPS Work Project. Int. J. Environ. Res. Public Health 2018, 15, 1545. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15071545
Hutchinson J, Gilbert D, Papworth R, Boardman J. Implementing Supported Employment. Lessons from the Making IPS Work Project. International Journal of Environmental Research and Public Health. 2018; 15(7):1545. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15071545
Chicago/Turabian StyleHutchinson, Jan, David Gilbert, Rachel Papworth, and Jed Boardman. 2018. "Implementing Supported Employment. Lessons from the Making IPS Work Project" International Journal of Environmental Research and Public Health 15, no. 7: 1545. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15071545