Assessing the Impact of a Risk-Based Intervention on Piped Water Quality in Rural Communities: The Case of Mid-Western Nepal


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Site
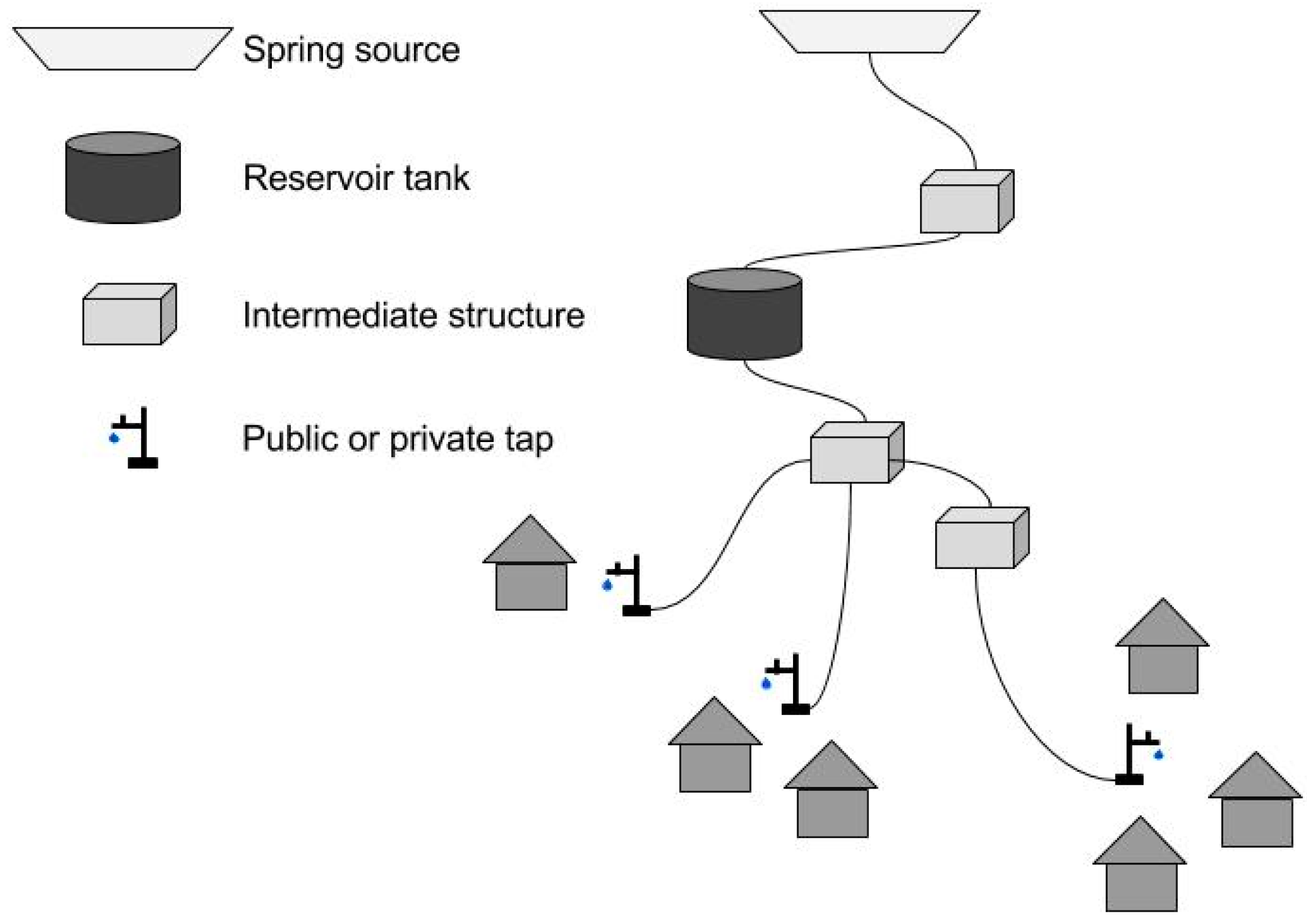
2.2. Description of Drinking Water Schemes
2.3. Study Design and Sample Strategy
2.3.1. Baseline and Endline Surveys
2.3.2. Regular Monitoring
2.4. Water Safety Plan, Interventions, and Laboratories
2.5. Data Collection Tools and Water Quality Analysis
2.5.1. Mobile Data Collection
2.5.2. Water Sampling and Microbial Water Quality Testing Protocol
2.5.3. Bacteria Enumeration and Quality Control
2.6. Data Analysis
2.7. Ethics Statement
3. Results
3.1. Household and Drinking Water Scheme Characteristics
3.1.1. Generalities
3.1.2. Hygiene Practices and Reported Illness
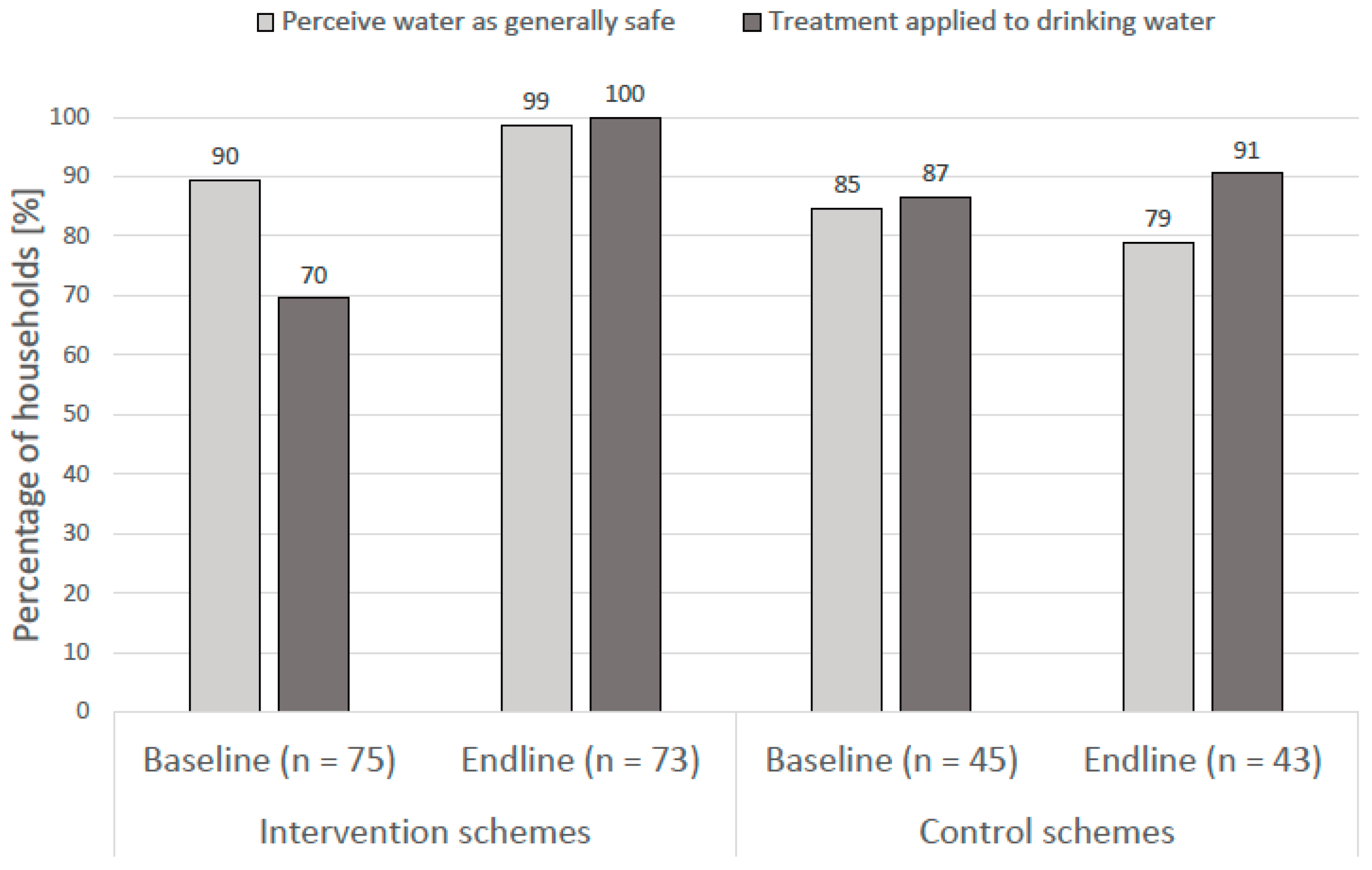
3.1.3. Perception of Drinking Water Quality and Water Treatment Practices
3.1.4. Water Supply Characteristics
3.1.5. Water Supply Management
3.1.6. Activities within Intervention Schemes
3.2. Water Quality Analysis
3.2.1. Household Stored Water Sample Characteristics
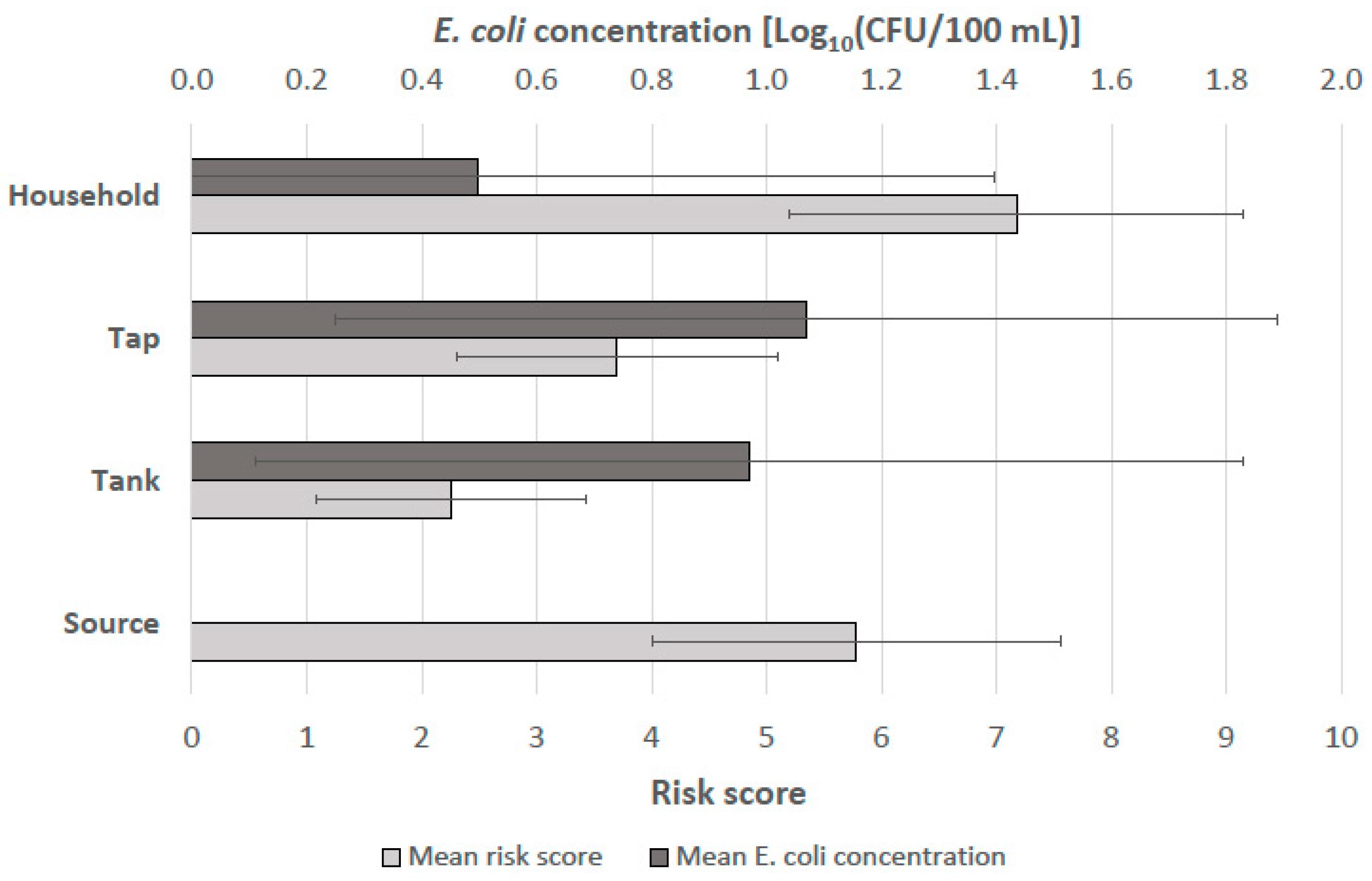
3.2.2. Baseline Water Quality and Qualitative Sanitary Observations
3.2.3. Monthly Monitoring of Intervention Schemes
3.2.4. Endline Water Quality and Qualitative Sanitary Observations
3.3. Comparisons of Fecal Contamination at the Baseline and Endline Measurement
3.3.1. Average Contamination by Scheme and Sampling Point
3.3.2. Statistical Comparisons of Fecal Contamination at the Baseline and Endline Measurements for Intervention and Control Schemes
3.3.3. Difference-in-Differences Analysis
4. Discussion
4.1. Study Novelty and Insights
4.2. Study Limitations
4.3. Recommendations for Water Sector Policy and Practice
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| CFU | colony forming units |
| HWTS | household water treatment and safe storage |
| IWRM | integrated water resources management |
| MDGs | Millennium Development Goals |
| NGO | non-governmental organization |
| NPR | Nepalese Rupee |
| 3R | recharge, retention, and reuse |
| SDGs | Sustainable Development Goals |
| Eawag | Swiss Federal Institute of Aquatic Science and Technology |
| WASH | water, sanitation and hygiene |
| WSP | water safety plan |
| WHO | World Health Organization |
| USD | United States Dollar |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Question | Score (yes = 1, no = 0) | |
|---|---|---|
| HOUSEHOLD STORED WATER CONTAINER | ||
| 1 | Are the drinking water storage containers used only for storing drinking and cooking water? | |
| 2 | Are the drinking water storage containers kept above ground level? | |
| 3 | Are the drinking water storage containers’ lids or covers present and in place? | |
| 4 | Are the drinking water storage containers sanitary and free from cracks? | |
| 5 | Is the area around the drinking water storage containers sanitary? | |
| 6 | Are animals prevented from accessing the area around the drinking water storage containers? | |
| 7 | Are the taps or utensils used to draw water from the drinking water storage containers sanitary? | |
| 8 | Is the water treated in any way before drinking? | |
| 9 | Has the water supply been continuous over the past 10 days? | |
| 10 | Is the water obtained from only one source? | |
| RISK SCORE = (10 – total # yes answers) = | ||
| PIPED WATER TAP | ||
| 1 | Does the tap stand leak? | |
| 2 | Is any part of the tap stand cracked or broken? | |
| 3 | Is there standing water around the tap stand? | |
| 4 | Are there any visible pipe leaks between the tank and the tap stand? | |
| 5 | Is the area uphill from the tap stand visibly eroded? (roughly 30m) | |
| 6 | Are pipes visibly exposed nearby the tap stand? (roughly 10m) | |
| 7 | Is excreta or garbage found within 10 m of the tap stand? | |
| 8 | Are there any animals within 10 m of the tap stand? | |
| 9 | Is there a sewer or latrine within 10 m of the tap stand? | |
| 10 | Has there been discontinuity within the past 10 days at the sample site? | |
| RISK SCORE = (total # yes answers) = | ||
| RESERVOIR TANK | ||
| 1 | Are there any visible pipe leaks between the source and the tank? | |
| 2 | Is there standing water around the tank? | |
| 3 | Is the area uphill from the tank visibly eroded? (roughly 30m) | |
| 4 | Are pipes visibly exposed close to the tank? (roughly 10m) | |
| 5 | Are excreta, garbage, or animals found within 10 m of the tank? | |
| 6 | Is there a sewer or latrine within 10m of the tank? | |
| 7 | Has there been discontinuity within last 10 days at the sample site? | |
| 8 | Are there signs of leaks around the tank? | |
| 9 | Is the tank cracked or damaged? | |
| 10 | Are the air vents or inspection covers unsanitary, damaged, or open? | |
| RISK SCORE = (total # yes answers) = | ||
| SOURCE | ||
| 1 | Is the water protected from surface contamination (masonry, concrete wall, or spring box)? | |
| 2 | Is the structure protecting the source in good condition? | |
| 3 | Is there a locked sanitary inspection cover? | |
| 4 | Is there a sanitary air vent in the structure? | |
| 5 | Is there a sanitary overflow pipe in the structure? | |
| 6 | Is there a functional surface water diversion ditch above the source? | |
| 7 | Is the source free from contaminating silt or animal excreta? | |
| 8 | Is the area around the source properly fenced? | |
| 9 | Are animals prevented from entering within 10 m of the source? | |
| 10 | Is the area within 10 m of the source free from the presence of latrines? | |
| RISK SCORE = (total # yes answers) = |
| Description | Baseline | Endline | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Households | Tanks | Taps | Households | Tanks | Taps | |||||||
| I (n = 75) | C (n = 45) | I (n = 11) | C (n = 10) | I (n = 14) | C (n = 9) | I (n = 72) | C (n = 43) | I (n = 15) | C (n = 10) | I (n = 14) | C (n = 9) | |
| Median [CFU/100 mL] | 24 | 8 | 12 | 49.5 | 10.5 | 38 | 0 | 4 | 4 | 8.5 | 0.5 | 3 |
| % of samples at the WHO guidelines [0 CFU/100 mL] | 17.3 | 20.0 | 18.2 | 0 | 7.2 | 0 | 52.8 | 23.3 | 26.7 | 10.0 | 50.0 | 11.1 |
| % of samples at low risk [1–10 CFU/100 mL] | 25.3 | 31.1 | 27.3 | 30.0 | 42.8 | 33.3 | 22.2 | 32.6 | 40.0 | 40.0 | 50.0 | 66.7 |
| % of samples at higher risk [11-TNTC CFU/100 mL] | 57.3 | 48.9 | 54.5 | 70.0 | 50.0 | 66.7 | 25.1 | 44.2 | 33.3 | 50.0 | 0 | 22.2 |
References
- WHO/UNICEF Joint Monitoring Programme. Progress on Drinking Water, Sanitation and Hygiene: Update and MDG Assessment; WHO Press: Geneva, Switzerland; New York, NY, USA, 2015; ISBN 9789241509145. [Google Scholar]
- Onda, K.; Lobuglio, J.; Bartram, J. Global access to safe water: Accounting for water quality and the resulting impact on MDG progress. Int. J. Environ. Res. Public Health 2012, 9, 880–894. [Google Scholar] [CrossRef] [PubMed]
- Bain, R.; Cronk, R.; Wright, J.; Yang, H.; Slaymaker, T.; Bartram, J. Fecal contamination of drinking-water in low- and middle-income countries: A systematic review and meta-analysis. PLoS Med. 2014, 11, e1001644. [Google Scholar] [CrossRef] [PubMed]
- Prüss-Ustün, A.; Bartram, J.; Clasen, T.; Colford, J.M.; Cumming, O.; Curtis, V.; Bonjour, S.; Dangour, A.D.; De France, J.; Fewtrell, L.; et al. Burden of disease from inadequate water, sanitation and hygiene in low- and middle-income settings: A retrospective analysis of data from 145 countries. Trop. Med. Int. Health 2014, 19, 894–905. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). Guidelines for Drinking Water Quality, 4th ed.; WHO Press: Geneva, Switzerland, 2011; ISBN 9789241548151. [Google Scholar]
- World Health Organization (WHO). Safely Managed Drinking Water—Thematic Report on Drinking Water; WHO Press: Geneva, Switzerland, 2017; ISBN 9789241565424. [Google Scholar]
- WHO/UNICEF Joint Monitoring Programme. Progress on Drinking Water, Sanitation and Hygiene: 2017 Update and SDG Baselines; WHO Press: Geneva, Switzerland; New York, NY, USA, 2017; ISBN 9789241512893. [Google Scholar]
- Shrestha, A.; Sharma, S.; Gerold, J.; Erismann, S.; Sagar, S.; Koju, R.; Schindler, C.; Odermatt, P.; Utzinger, J.; Cissé, G. Water quality, sanitation, and hygiene conditions in schools and households in Dolakha and Ramechhap Districts, Nepal: Results from a cross-sectional survey. Int. J. Environ. Res. Public Health 2017, 14, 89. [Google Scholar] [CrossRef] [PubMed]
- Marks, S.J.; Diener, A.; Bhatta, M.; Sihombing, D.; Meierhofer, R. Researching Water Quality, Consumer Preferences and Treatment Behaviour. Available online: https://www.eawag.ch/fileadmin/Domain1/Abteilungen/sandec/schwerpunkte/WST/researching_water_quality.pdf (accessed on 27 July 2018).
- Diener, A.; Kenea, M.A.; Pratama, I.Y.; Bhatta, M.; Bhatta, M.; Marks, S.J. Safer Water for Remote Nepal—Novel Pathways Towards SDG 6.1. Available online: https://www.eawag.ch/fileadmin/Domain1/Abteilungen/sandec/schwerpunkte/WST/safer_water_remote_nepal.pdf (accessed on 27 July 2018).
- World Health Organization (WHO). Water Safety Planning for Small Community Water Supplies: Step-By-Step Risk Management Guidance for Drinking-Water Supplies in Small Communites; WHO Press: Geneva, Switzerland, 2012; ISBN 9789241548427. [Google Scholar]
- Rickert, B.; Schmoll, O.; Rinehold, A.; Barrenberg, E. Water Safety Plan: A Field Guide to Improving Drinking-Water Safety in Small Communities; WHO Regional Office for Europe: Copenhagen, Denmark, 2014; ISBN 9789289050074. [Google Scholar]
- String, G.; Lantagne, D. A systematic review of outcomes and lessons learned from general, rural, and country-specific Water Safety Plan implementations. Water Sci. Technol. Water Supply 2016, 16, ws2016073. [Google Scholar] [CrossRef]
- Ercumen, A.; Naser, A.M.; Arnold, B.F.; Unicomb, L.; Colford, J.M.; Luby, S.P. Can sanitary inspection surveys predict risk of microbiological contamination of groundwater sources? Evidence from shallow tubewells in rural Bangladesh. Am. J. Trop. Med. Hyg. 2017, 96, 561–568. [Google Scholar] [CrossRef] [PubMed]
- Mushi, D.; Byamukama, D.; Kirschner, A.K.T.; Mach, R.L.; Brunner, K.; Farnleitner, A.H. Sanitary inspection of wells using risk-of-contamination scoring indicates a high predictive ability for bacterial faecal pollution in the peri-urban tropical lowlands of Dar es Salaam, Tanzania. J. Water Health 2012, 10, 236–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Misati, A.G.; Ogendi, G.; Peletz, R.; Khush, R.; Kumpel, E. Can sanitary surveys replace water quality testing? Evidence from Kisii, Kenya. Int. J. Environ. Res. Public Health 2017, 14, 152. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Sanitary Inspection Package Update. In WHO Meeting on the Guidelines for Drinking-Water Quality: Small Water Supplies and Small Drinking-Water Supplies: A Guide to Field Work; WHO Regional Office for Europe: Chisinau, Moldova, 2017. [Google Scholar]
- Shrestha, N.R. In the Name of Development: A Reflection on Nepal; University Press of America: Lanham, MD, USA; Oxford, UK, 1997; ISBN 0761807594. [Google Scholar]
- United Nations Department of Economic and Social Affairs/Population Division. Volume I: Comprehensive Tables (ST/ESA/SER.A/399); United Nations: New York, NY, USA, 2017. [Google Scholar]
- World Bank. The World Bank Open Data Portal. Available online: http://data.worldbank.org/ (accessed on 1 April 2018).
- United Nations Development Programme (UNDP). Human Development Report; United Nations: New York, NY, USA, 2016; ISBN 9789211264135. [Google Scholar]
- Udmale, P.; Ishidaira, H.; Thapa, B.; Shakya, N. The status of domestic water demand: Supply deficit in the Kathmandu Valley, Nepal. Water 2016, 8, 196. [Google Scholar] [CrossRef]
- Merz, J.; Nakarmi, G.; Shrestha, S.K.; Dahal, B.M.; Dangol, P.M.; Dhakal, M.P.; Dongol, B.S.; Sharma, S.; Shah, P.B.; Weingartner, R. Water: A scarce resource in rural watersheds of Nepal’s middle mountains. Mt. Res. Dev. 2003, 23, 41–49. [Google Scholar] [CrossRef]
- Xu, J.; Grumbine, R.E.; Shrestha, A.; Eriksson, M.; Yang, X.; Wang, Y.; Wilkes, A. The melting Himalayas: Cascading effects of climate change on water, biodiversity, and livelihoods. Conserv. Biol. 2009, 23, 520–530. [Google Scholar] [CrossRef] [PubMed]
- Government of Nepal. Nepal Drinking Water Quality Surveillance Guideline; Ministry of Health and Population: Kathmandu, Nepal, 2010.
- Government of Nepal. Nepal Water Supply, Sanitation and Hygiene Sector Development Plan (2016–2030) 2016; Ministry of Water Supply and Sanitation: Kathmandu, Nepal, 2016.
- Government of Nepal. National Drinking Water Quality Standards; Ministry of Water Supply and Sanitation: Kathmandu, Nepal, 2005.
- Marks, S.J.; Davis, J. Does user participation lead to sense of ownership for rural water systems? Evidence from Kenya. World Dev. 2012, 40, 1569–1576. [Google Scholar] [CrossRef]







| Activity | Intervention Communities | Control Communities |
|---|---|---|
| Helvetas-Nepal program activities established before the study | Constructed piped water scheme | Same as intervention schemes |
| Established water users’ committee | ||
| Conducted household hygiene campaign | ||
| Installed ceramic water filters | ||
| Trained community health volunteer and village maintenance worker | ||
| Data collection at study baseline and endline | Household survey | Same as intervention schemes |
| Water quality sampling | ||
| System sanitary inspection | ||
| Physical upgrades to water schemes | Source protection | None |
| Intake improvement | ||
| Scheme level chlorination 1 | ||
| Small repairs | ||
| 3R measures (Recharge, Retention, Reuse) | ||
| Management interventions | Creation of the Water Safety Plan task force | None |
| Regular monitoring of sanitary state and water quality | ||
| Laboratory coverage | ||
| Improved maintenance | ||
| Behavior change interventions | Promotion of good handling practices for ceramic candle filter | None |
| Household sanitary inspections |
| Sampling Phase | Household | Tank | Tap |
|---|---|---|---|
| Baseline | 120 | 21 | 23 |
| Regular monitoring | 23 | 23 | 23 |
| Endline | 115 | 25 | 23 |
| Characteristics | Intervention Schemes | Control Schemes |
|---|---|---|
| Households served | 66.8 (32.2), [29 to 108] | 84.3 (30.4), [50 to 108] |
| Population served | 411.8 (209.5), [177 to 683] | 511.7 (194.9), [292 to 664] |
| Spring sources | 2.6 (1.1), [1 to 4] | 3.3 (1.2), [2 to 4] |
| Reservoir tanks | 3.2 (1.5), [1 to 5] | 3.7 (0.6), [3 to 4] |
| Taps | 19.4 (3.6), [15 to 24] | 26.7 (14.2), [18 to 43] |
| Sample Characteristic | Intervention Schemes | Control Schemes | ||
|---|---|---|---|---|
| BL (%) | EL (%) | BL (%) | EL (%) | |
| Sample collected from: | ||||
| Ceramic candle filter outlet | 57 | 99 | 78 | 81 |
| Gagri/jerrycan/bucket | 43 | 1 | 22 | 19 |
| Visual quality: | ||||
| Clear | 100 | 97 | 96 | 81 |
| Somewhat turbid | 0 | 3% | 4 | 19 |
| Very turbid | 0 | 0 | 0 | 0 |
| Received treatment at: | ||||
| Household level only | 59 | 25 | 76 | 86 |
| Scheme level only | 0 | 0 | 0 | 0 |
| Both household and scheme level | 3 | 75 | 6 | 0 |
| No treatment | 37 | 0 | 18 | 14 |
| Location | Sampling Phase | Intervention Schemes | Control Schemes | ||||||
|---|---|---|---|---|---|---|---|---|---|
| n | Median [CFU/100 mL] | Mean (SD), [Range] [Log10(CFU/100 mL)] | Student’s t-test | n | Median [CFU/100 mL] | Mean (SD), [Range] [Log10(CFU/100 mL)] | Student’s t-Test | ||
| Household | Baseline | 75 | 24 | 1.25 (1.00), [−0.30 to 2.48] | t = −5.645, df = 145, p < 0.001 | 45 | 8 | 1.01 (0.97), [−0.30 to 2.48] | t = −1.026, df = 86, p = 0.308 |
| Endline | 72 | 0 | 0.36 (0.92), [−0.30 to 2.48] | 43 | 4 | 0.80 (0.98), [−0.30 to 2.48] | |||
| Tank | Baseline | 11 | 12 | 1.00 (0.80), [−0.30 to 2.04] | t = −1.120, df = 24, p = 0.274 | 10 | 50 | 1.52 (0.86), [0.00 to 2.48] | t = −1.381, df = 18, p = 0.184 |
| Endline | 15 | 4 | 0.63 (0.87), [−0.30 to 2.08] | 10 | 9 | 0.98 (0.89), [−0.30 to 2.48] | |||
| Tap | Baseline | 14 | 11 | 1.14 (0.79), [−0.30 to 2.18] | t = −4.086, df = 26, p < 0.000 | 9 | 38 | 1.54 (1.01), [0.00 to 2.48] | t = −2.040, df = 16, p = 0.058 |
| Endline | 14 | 1 | 0.13 (0.49), [−0.30 to 0.85] | 9 | 3 | 0.65 (0.82), [−0.30 to 2.48] | |||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tosi Robinson, D.; Schertenleib, A.; Kunwar, B.M.; Shrestha, R.; Bhatta, M.; Marks, S.J. Assessing the Impact of a Risk-Based Intervention on Piped Water Quality in Rural Communities: The Case of Mid-Western Nepal. Int. J. Environ. Res. Public Health 2018, 15, 1616. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15081616
Tosi Robinson D, Schertenleib A, Kunwar BM, Shrestha R, Bhatta M, Marks SJ. Assessing the Impact of a Risk-Based Intervention on Piped Water Quality in Rural Communities: The Case of Mid-Western Nepal. International Journal of Environmental Research and Public Health. 2018; 15(8):1616. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15081616
Chicago/Turabian StyleTosi Robinson, Dorian, Ariane Schertenleib, Bal Mukunda Kunwar, Rubika Shrestha, Madan Bhatta, and Sara J. Marks. 2018. "Assessing the Impact of a Risk-Based Intervention on Piped Water Quality in Rural Communities: The Case of Mid-Western Nepal" International Journal of Environmental Research and Public Health 15, no. 8: 1616. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15081616