Community Resilience Learning Collaborative and Research Network (C-LEARN): Study Protocol with Participatory Planning for a Randomized, Comparative Effectiveness Trial

 , , ,
, , , {kind=link}
{kind=link}
Abstract
:1. Introduction
2. Study Design
2.1. Aims
- To engage communities in South Louisiana in a community learning initiative on how to best build capacity to enhance resilience to depression, adverse social determinants of health, and disaster exposure. This aim includes a qualitative assessment of local community resilience priorities and assets to inform study implementation.
- To compare the effectiveness for improving mental health quality of life (MHRQL) (primary) and coping with stressors and other resilience outcomes (secondary), of two program-level interventions to build capacity for resilience programs: (1) Technical Assistance (TA) to individual programs vs. (2) Community Engagement and Planning (CEP) to support multi-sector coalitions. Hypothesis: CEP will be more effective at enhancing individual client (primary and secondary) outcomes. In addition, CEP will be more effective than TA in engaging programs and providers in trainings to improve services for depression, social risks and disaster concerns (primary), and in increasing the use of such services by programs and providers (secondary).
- To compare the effectiveness for improving MHRQL and other resilience outcomes of two mobile apps: CR and CR+eCBT: (1) CR—An app providing only information on community resources, or (2) CR+eCBT—An app providing information on community resources and education on a cognitive behavioral therapy (eCBT) based approach to enhance individual resilience (i.e., coping with mood and stressors). Hypothesis: CR + eCBT mobile app will be more effective CR in improving the same primary and secondary client outcomes as for Aim 2. To describe strategies from CEP coalitions used to address depression, social determinants and disaster resilience, to inform interpretation and dissemination of findings.
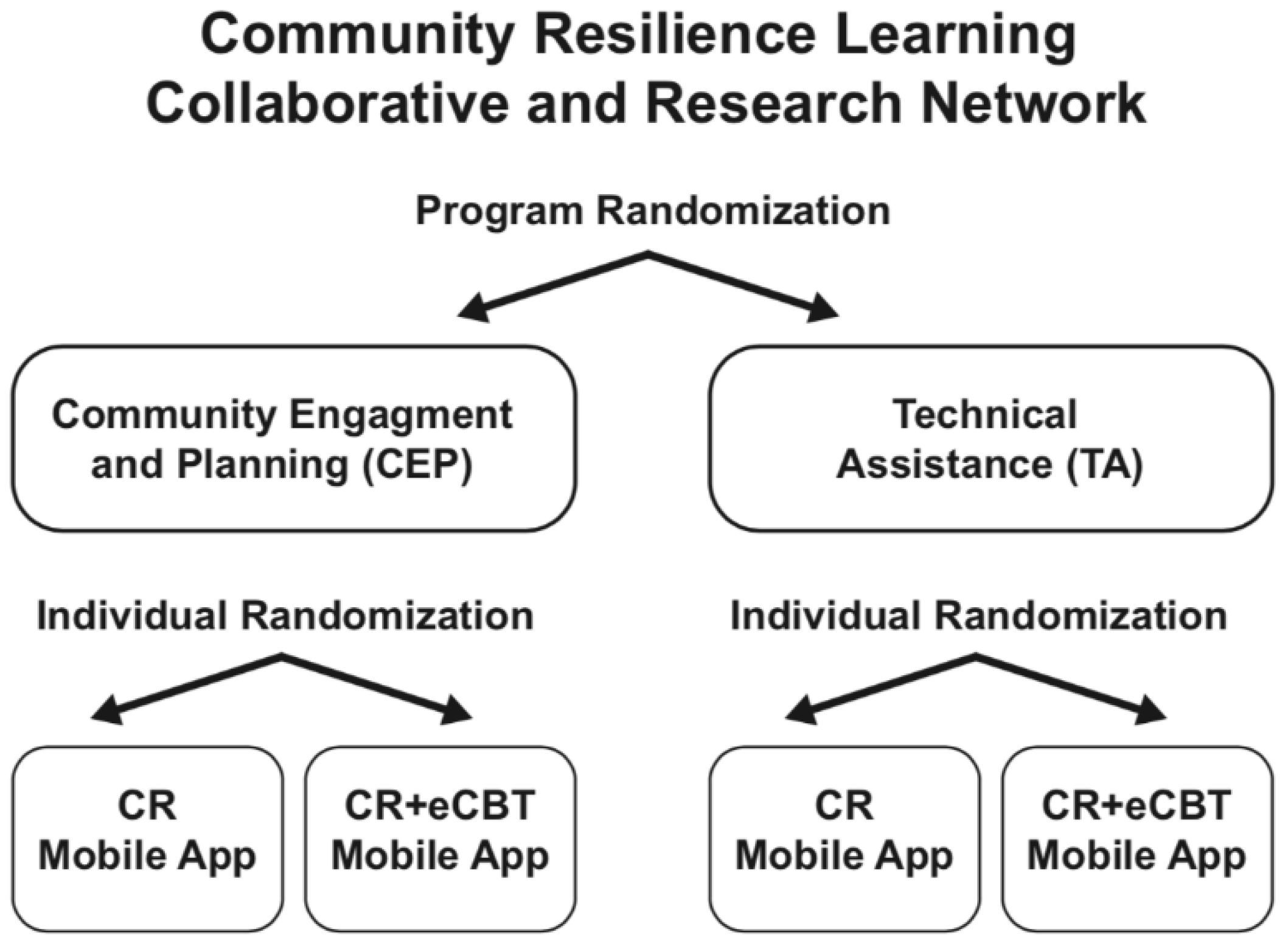
2.2. Design
2.3. Interventions
2.3.1. CEP for Coalitions
2.3.2. TA for Individual Programs
2.3.3. Individual-Level Mobile Apps
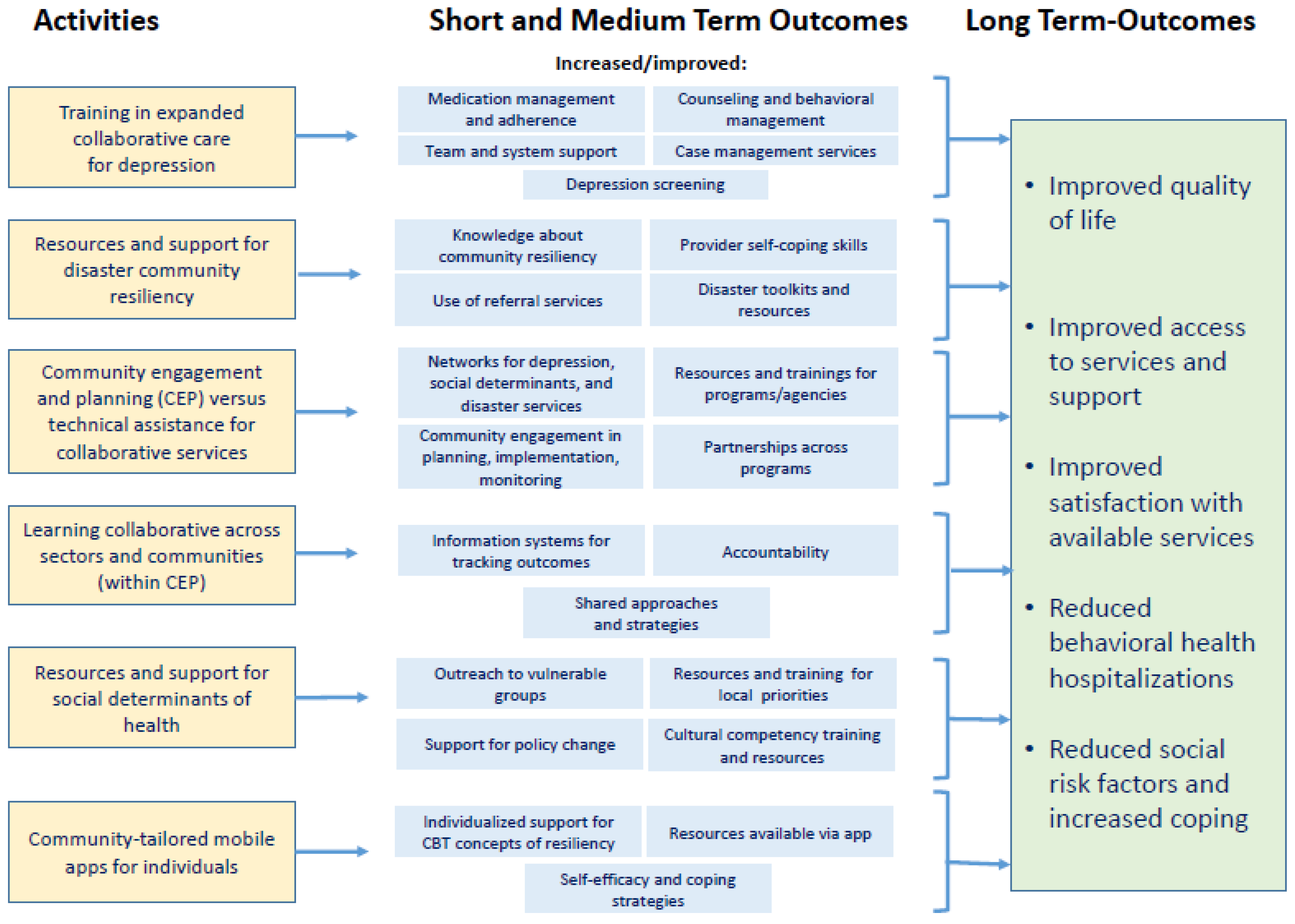
2.3.4. Driver Diagram
2.4. Measures
2.4.1. Measures for Client/Community Participants
2.4.2. Administrator/Provider Measures
2.5. Randomization
2.5.1. Program-Level (CEP vs. TA)
2.5.2. Individual-Level
2.6. Sampling
2.6.1. Communities
2.6.2. Programs
2.6.3. Administrators and Providers/Staff
2.6.4. Clients/Community Members
2.6.5. Data Collection
2.6.6. Human Subjects Protection
2.6.7. Power Calculations
2.7. Proposed Analysis
2.7.1. General Issues
2.7.2. Aim 2 Analysis (CEP vs. TA)
2.7.3. Aim 3 Analysis: (CR App vs. CR + eCBT App)
2.7.4. Qualitative Analysis
2.7.5. Linguistic Predictors
2.7.6. Mixed-Methods Analyses
2.7.7. Partnered Synthesis
3. Discussion
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Portier, C.; Thigpen, T.K.; Carter, S.; Dilworth, C. A Human Health Perspective on Climate Change: A Report Outlining the Research Needs on the Human Health Effects of Climate Change; Environmental Health Perspectives/National Institute of Environmental Health Sciences: Research Triangle Park, NC, USA, 2010.
- Greenough, G.; McGeehin, M.; Bernard, S.M.; Trtanj, J.; Riad, J.; Engelberg, D. The potential impacts of climate variability and change on health impacts of extreme weather events in the United States. Environ. Health Perspect. 2001, 109, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, S.M.; Peters, E.S.; Trapido, E.J.; Oral, E.; Scribner, R.A.; Rung, A.L. Assessing mediation of behavioral and stress pathways in the association between neighborhood environments and obesity outcomes. Prev. Med. Rep. 2016, 4, 248–255. [Google Scholar] [CrossRef] [PubMed]
- Woodward, A.J.; Samet, J.M. Climate Change, Hurricanes, and Health. Am. J. Public Health 2018, 108, 33–35. [Google Scholar] [CrossRef] [PubMed]
- Lane, K.; Kizzy, C.-G.; Wheeler, K.; Abid, Z.; Graber, N.; Matte, T. Health Effects of Coastal Storms and Flooding in Urban Areas: A Review and Vulnerability Assessment. J. Environ. Public Health 2013, 2013, 913064. [Google Scholar] [CrossRef] [PubMed]
- Ryan, B.; Franklin, R.C.; Burkle, F.M., Jr.; Aitken, P.; Smith, E.; Watt, K.; Leggat, P. Identifying and Describing the Impact of Cyclone, Storm and Flood Related Disasters on Treatment Management, Care and Exacerbations of Non-communicable Diseases and the Implications for Public Health. PLOS Curr. Disasters 2015, 7. [Google Scholar] [CrossRef] [PubMed]
- Barbeau, D.N.; Grimsley, L.F.; White, L.E.; El-Dahr, J.M.; Lichtveld, M. Mold Exposure and Health Effects Following Hurricanes Katrina and Rita. Annu. Rev. Public Health 2010, 31, 165–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stanke, C.; Murray, V.; Amlôt, R.; Nurse, J.; Williams, R. The effects of flooding on mental health: Outcomes and recommendations from a review of the literature. PLoS Curr. 2012, 4, e4f9f1fa9c3cae. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berry, H.L.; Bowen, K.; Kjellstrom, T. Climate change and mental health: A causal pathways framework. Int. J. Public Health 2010, 55, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Fritze, J.C.; Blashki, G.A.; Burke, S.; Wiseman, J. Hope, despair and transformation: Climate change and the promotion of mental health and wellbeing. Int. J. Ment. Health Syst. 2008, 2, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaston, S.; Nugent, N.; Peters, E.S.; Ferguson, T.F.; Trapido, E.J.; Robinson, W.T.; Rung, A.L. Exploring heterogeneity and correlates of depressive symptoms in the Women and Their Children’s Health (WaTCH) Study. J. Affect. Disord. 2016, 205, 190–199. [Google Scholar] [CrossRef] [PubMed]
- Rung, A.L.; Gaston, S.; Oral, E.; Robinson, W.T.; Fontham, E.; Harrington, D.J.; Trapido, E.; Peters, E.S. Depression, mental distress, and domestic conflict among Louisiana women exposed to the Deepwater Horizon oil spill in the WatCH study. Environ. Health Perspect. 2016, 124, 1429–1435. [Google Scholar] [CrossRef] [PubMed]
- Rung, A.L.; Oral, E.; Fontham, E.; Harrington, D.J.; Trapido, E.J.; Peters, E.S. Mental Health Impact of the Deepwater Horizon Oil Spill among Wives of Clean-up Workers. Epidemiology 2015, 26, e44–e46. [Google Scholar] [CrossRef] [PubMed]
- Palinkas, L.A.; Petterson, J.S.; Russell, J.; Downs, M.A. Community patterns of psychiatric disorders after the Exxon Valdez oil spill. Am. J. Psychiatry 1993, 150, 1517–1523. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.; Galea, S.; Gruber, M.; Sampson, N.; Ursano, R.; Wessel, S. Trends in mental illness and suicidality after Hurricane. Mol. Psychol. 2008, 13, 374–384. [Google Scholar] [CrossRef] [PubMed]
- Hirth, J.M.; Leyser-Whalen, O.; Berenson, A.B. Effects of a Major U.S. Hurricane on Mental Health Disorder Symptoms Among Adolescent and Young Adult Females. J. Adolesc. Health 2013, 52, 765–772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cherry, K.E.; Galea, S.; Su, L.J.; Welsh, D.A.; Jazwinski, S.M.; Silva, J.L.; Erwin, M.J. Cognitive and Psychosocial Consequences of Hurricanes Katrina and Rita Among Middle-Aged, Older, and Oldest-Old Adults in the Louisiana Healthy Aging Study (LHAS). J. Appl. Soc. Psychol. 2010, 40, 2463–2487. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, R.M.; Gillezeau, C.N.; Liu, B.; Lieberman-Cribbin, W.; Taioli, E. Longitudinal Impact of Hurricane Sandy Exposure on Mental Health Symptoms. Int. J. Environ. Res. Public Health 2017, 14, 957. [Google Scholar] [CrossRef] [PubMed]
- Mearns, R.; Norton, A. The Social Dimensions of Climate Change, Equity and Vulnerability in a Warming World; The World Bank: Washington, DC, USA, 2010; Volume 81. [Google Scholar]
- Gitay, H.; Bettencourt, S.; Kull, D. Building Resilience: Integrating Climate and Disaster Risk into Development; The World Bank Group experience: Washington, DC, USA, 2013. [Google Scholar]
- Peres, L.C.; Trapido, E.; Rung, A.L.; Harrington, D.J.; Oral, E.; Fang, Z.; Fontham, E.; Peters, E.S. The Deepwater Horizon Oil Spill and physical health among adult women in southern Louisiana: The Women and Their Children’s Health (WaTCH) study. Environ. Health Perspect. 2016, 124, 1208–1213. [Google Scholar] [CrossRef] [PubMed]
- Morton, M.J.; Lurie, N. Community resilience and public health practice. Am. J. Public Health 2013, 103, 1158–1160. [Google Scholar] [CrossRef] [PubMed]
- Chandra, A.; Williams, M.; Plough, A.; Stayton, A.; Wells, K.B.; Horta, M.; Tang, J. Getting actionable about community resilience: The Los Angeles county community disaster resilience project. Am. J. Public Health 2013, 103, 1181–1189. [Google Scholar] [CrossRef] [PubMed]
- United Nations Office for Disaster Risk Reduction. Terminology. Available online: https://www.unisdr.org/we/inform/terminology#letter-r (accessed on 15 May 2018).
- Norris, F.H.; Stevens, S.P.; Pfefferbaum, B.; Wyche, K.F.; Pfefferbaum, R.L. Community resilience as a metaphor, theory, set of capacities, and strategy for disaster readiness. Am. J. Community Psychol. 2008, 41, 127–150. [Google Scholar] [CrossRef] [PubMed]
- Aldrich, D.P.; Meyer, M.A. Social capital and community resilience. Am. Behav. Sci. 2014, 59, 254–269. [Google Scholar] [CrossRef]
- FEMA. A Whole Community Approach to Emergency Management: Principles, Themes, and Pathways for Action; Fdoc 104-008-1; FEMA: Washington, DC, USA, 2011; 24p.
- Plough, A.; Fielding, J.E.; Chandra, A.; Williams, M.; Eisenman, D.; Wells, K.B.; Law, G.Y.; Fogleman, S.; Magaña, A. Building community disaster resilience: Perspectives from a large urban county department of public health. Am. J. Public Health 2013, 103, 1190–1197. [Google Scholar] [CrossRef] [PubMed]
- Delgado, M.; Humm-Delgado, D. Asset Assessments and Community Social Work Practice; Oxford University Press: Oxford, UK, 2013. [Google Scholar]
- Ryan, B.; Franklin, R.C.; Burkle, F.M. Jr.; Aitken, P.; Smith, E.; Watt, K.; Leggat, P.; Luthar, S.; Cicchetti, D.; Becker, B.; et al. Identifying and Describing the Impact of Cyclone, Storm and Flood Related Disasters on Treatment Management, Care and Exacerbations of Non-communicable Diseases and the Implications for Public Health. PLOS Curr. Disasters 2015. [Google Scholar] [CrossRef] [PubMed]
- Norris, F.H.; Baker, C.K.; Murphy, A.D.; Kaniasty, K. Social support mobilization and deterioration after Mexico’s 1999 flood: Effects of context, gender, and time. Am. J. Community Psychol. 2005, 36, 15–28. [Google Scholar] [CrossRef] [PubMed]
- Sherbourne, C.D.; Edelen, M.O.; Zhou, A.; Bird, C.; Duan, N.; Wells, K.B. How a Therapy-Based Quality Improvement Intervention for Depression Affected Life Events and Psychological Well-Being over Time. Med. Care 2008, 46, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Neria, Y.; Nandi, A.; Galea, S. Post-traumatic stress disorder following disasters: A systematic review. Psychol. Med. 2008, 38, 467–480. [Google Scholar] [CrossRef] [PubMed]
- Norris, F.H. Epidemiology of trauma: Frequency and impact of different potentially traumatic events on different demographic groups. J. Consult. Clin. Psychol. 1992, 60, 409–418. [Google Scholar] [CrossRef] [PubMed]
- North, C.S.; Pfefferbaum, B. Mental health response to community disasters: A systematic review. JAMA J. Am. Med. Assoc. 2013, 310, 507–518. [Google Scholar] [CrossRef] [PubMed]
- Palinkas, L.; Russell, J.; Downs, M.; Petterson, J. Ethnic differences in stress, coping, and depressive symptoms after the Exxon Valdez oil spill. J. Nerv. Ment. Dis. 1992, 180, 287–295. [Google Scholar] [CrossRef] [PubMed]
- Palinkas, L.A.; Petterson, J.S.; Russell, J.C.; Downs, M.A. Ethnic differences in symptoms of post-traumatic stress after the Exxon Valdez oil spill. Prehosp. Disaster Med. 2004, 19, 102–111. [Google Scholar] [CrossRef] [PubMed]
- Marmot, M.; Wilkinson, R. Social Determinants of Health; Oxford University Press: Evans Road Cary, NC, USA, 2006. [Google Scholar]
- Galea, S.; Vlahov, D. Social determinants and the health of drug users: Socioeconomic status, homelessness, and incarceration. Public Health Rep. 2002, 117 (Suppl. 1), S135–S145. [Google Scholar] [CrossRef]
- Wilkinson, R.G.; Pickett, K.E. Income inequality and population health: A review and explanation of the evidence. Soc. Sci. Med. 2006, 62, 1768–1784. [Google Scholar] [CrossRef] [PubMed]
- Jane-Llopis, E.; Anderson, P. A policy framework for the promotion of mental health and the prevention of mental disorders. In Mental Health Policy and Practice across Europe; McGraw-Hill Education: London, UK, 2006; p. 188. [Google Scholar]
- Galea, S.; Ahern, J.; Nandi, A.; Tracy, M.; Beard, J.; Vlahov, D. Urban Neighborhood Poverty and the Incidence of Depression in a Population-Based Cohort Study. Ann. Epidemiol. 2007, 17, 171–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lustman, P.J.; Anderson, R.J.; Freedland, K.E.; De Groot, M.; Carney, R.M.; Clouse, R.E. Depression and poor glycemic control: A meta-analytic review of the literature. Diabetes Care 2000, 23, 934–942. [Google Scholar] [CrossRef] [PubMed]
- Wadsworth, M.E.; Achenbach, T.M. Explaining the link between low socioeconomic status and psychopathology: Testing two mechanisms of the social causation hypothesis. J. Consult. Clin. Psychol. 2005, 73, 1146–1153. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Closing the Gap in a Generation: Health Equity through Action on the Social Determinants of Health; World Health Organization: Geneva, Switzerland, 2008; p. 40. [Google Scholar]
- Adger, W.N.; Hughes, T.P.; Folke, C.; Carpenter, S.R.; Rockstrom, J. Social-ecological resilience to coastal disasters. Science 2005, 309, 1036–1039. [Google Scholar] [CrossRef] [PubMed]
- Aitsi-Selmi, A.; Egawa, S.; Sasaki, H.; Wannous, C.; Murray, V. The Sendai Framework for Disaster Risk Reduction: Renewing the Global Commitment to People’s Resilience, Health, and Well-being. Int. J. Disaster Risk Sci. 2015, 6, 164–176. [Google Scholar] [CrossRef] [Green Version]
- Sciences, N. A. of Gulf Research Program. Available online: http://www.nationalacademies.org/gulf/about/index.html (accessed on 15 May 2018).
- Jones, L.; Wells, K. Strategies for Academic and Clinician Engagement in Community-Participatory Partnered Research. JAMA 2007, 297, 407. [Google Scholar] [CrossRef] [PubMed]
- Wells, K.; Jones, L. “Research” in community-partnered, participatory research. JAMA - J. Am. Med. Assoc. 2009, 302, 320–321. [Google Scholar] [CrossRef] [PubMed]
- Unützer, J.; Katon, W.; Callahan, C.M.; Williams, J.W., Jr.; Hunkeler, E.; Harpole, L.; Hoffing, M.; Della Penna, R.D.; Noël, P.H.; Lin, E.H.; et al. Collaborative care management of late-life depression in the primary care setting: A randomized controlled trial. JAMA 2002, 288, 2836–2845. [Google Scholar] [CrossRef] [PubMed]
- Wells, K.B.; Sherbourne, C.; Schoenbaum, M.; Duan, N.; Meredith, L.; Unützer, J.; Miranda, J.; Carney, M.F.; Rubenstein, L.V. Impact of Disseminating Quality Improvement Programs for Depression in Managed Primary Care. JAMA 2000, 283, 212–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miranda, J.; Chung, J.Y.; Green, B.L.; Krupnick, J.; Siddique, J.; Revicki, D.A.; Belin, T. Treating Depression in Predominantly Low-Income Young Minority Women: A Randomized Controlled Trial. JAMA J. Am. Med. Assoc. 2003, 290, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Springgate, B.F.; Wennerstrom, A.; Meyers, D.; Allen, I.I.I.C.E.; Vannoy, S.D.; Bentham, W.; Wells, K.B. Building community resilience through mental health infrastructure and training in post-Katrina New Orleans. Ethn. Dis. 2011, 21 (Suppl. 1), S1-20-9. [Google Scholar] [PubMed]
- Wennerstrom, A.; Vannoy, S.D.; Allen, C.E.; Meyers, D.; O’Toole, E.; Wells, K.B.; Springgate, B.F. Community-based participatory development of a community health worker mental health outreach role to extend collaborative care in post-Katrina New Orleans. Ethn. Dis. 2011, 21 (Suppl. 1), S1-45-21. [Google Scholar]
- Meyers, D.; Allien, C.E., 3rd; Dunn, D.; Wennerstrom, A.; Springgate, B.F. Community perspectives on post-Katrina mental health recovery in New Orleans. Ethn. Dis. 2011, 21 (Suppl. 1), S1-52-7. [Google Scholar]
- Ngo, V.K.; Centanni, A.; Wong, E.; Wennerstrom, A.; Miranda, J. Building capacity for cognitive behavioral therapy delivery for depression in disaster-impacted contexts. Ethn. Dis. 2011, 21 (Suppl. 1), S1-38-44. [Google Scholar]
- Bentham, W.; Vannoy, S.D.; Badger, K.; Wennerstrom, A.; Springgate, B.F. Opportunities and challenges of implementing collaborative mental health care in post-Katrina New Orleans. Ethn. Dis. 2011, 21 (Suppl. 1), S1-30-7. [Google Scholar]
- Wells, K.B.; Springgate, B.F.; Lizaola, E.; Jones, F.; Plough, A. Community Engagement in Disaster Preparedness and Recovery: A Tale of Two Cities—Los Angeles and New Orleans. Psychiatr. Clin. N. Am. 2013, 36, 451–466. [Google Scholar] [CrossRef] [PubMed]
- Eisenman, D.; Chandra, A.; Fogleman, S.; Magana, A.; Hendricks, A.; Wells, K.; Williams, M.; Tang, J.; Plough, A. The Los Angeles county community disaster resilience project—A Community-Level, public health initiative to build community disaster resilience. Int. J. Environ. Res. Public Health 2014, 11, 8475–8490. [Google Scholar] [CrossRef] [PubMed]
- Arevian, A.; O’hora, J.; Jones, F.; Mango, J.; Jones, L.; P, W.; Booker-Vaughns, J.; Pulido, E.; Banner, D.; Wells, K. Participatory Technology Development to Enhance Community Resilience. Ethn. Dis. In press.
- Wells, K.B.; Jones, L.; Chung, B.; Dixon, E.L.; Tang, L.; Gilmore, J.; Sherbourne, C.; Ngo, V.K.; Ong, M.K.; Stockdale, S.; et al. Community-partnered cluster-randomized comparative effectiveness trial of community engagement and planning or resources for services to address depression disparities. J. Gen. Intern. Med. 2013, 28, 1268–1278. [Google Scholar] [CrossRef] [PubMed]
- Chung, B.; Ngo, V.K.; Ong, M.K.; Pulido, E.; Jones, F.; Gilmore, J.; Stoker-Mtume, N.; Johnson, M.; Tang, L.; Wells, K.B.; et al. Participation in Training for Depression Care Quality Improvement: A Randomized Trial of Community Engagement or Technical Support. Psychiatr. Serv. 2015, 66, 831–839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nembhard, I.M. All teach, all learn, all improve? Health Care Manag. Rev. 2012, 37, 154–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sherbourne, C.D.; Stewart, A.L. The MOS social support survey. Soc. Sci. Med. 1991, 32, 705–714. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Weathers, F.; Litz, B.; Herman, D.; Huska, J.; Keane, T. The PTSD Checklist (PCL): Reliability, Validity, and Diagnostic Utility. In Proceedings of the Annual Convention of the International Society for Traumatic Stress Studies, San Antonio, TX, USA, 25 October 1993. [Google Scholar]
- Chan, C.S.; Rhodes, J.E. Measuring exposure in hurricane Katrina: A meta-analysis and an integrative data analysis. PLoS ONE 2014, 9, e92899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohn, M.A.; Mehl, M.R.; Pennebaker, J.W. Linguistic markers of psychological change surrounding September 11, 2001. Psychol. Sci. 2004, 15, 687–693. [Google Scholar] [CrossRef] [PubMed]
- Wells, K.B.; Tang, J.; Lizaola, E.; Jones, F.; Brown, A.; Stayton, A.; Williams, M.; Chandra, A.; Eisenman, D.; Fogleman, S.; et al. Applying community engagement to disaster planning: Developing the vision and design for the Los Angeles county community disaster resilience initiative. Am. J. Public Health 2013, 103, 1172–1180. [Google Scholar] [CrossRef] [PubMed]
- Landry, C.M.; Jackson, A.P.; Tang, L.; Miranda, J.; Chung, B.; Jones, F.; Ong, M.K.; Wells, K. The effects of collaborative care training on case managers’ perceived depression-related services delivery. Psychiatr. Serv. 2017, 68, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Murray, D.M. Design and Analysis of Group-Randomized Trials; Oxford University Press: Oxford, UK, 1998. [Google Scholar]
- Chung, B.; Jones, L.; Dixon, E.L.; Miranda, J.; Wells, K. Community Partners in Care Steering. Using a Community Partnered Participatory Research Approach to Implement a Randomized Controlled Trial: Planning Community Partners in Care. J. Health Care Poor Underserved 2010, 21, 780–795. [Google Scholar] [CrossRef] [PubMed]
- Little, R.J.A. Missing-data adjustments in large surveys. J. Bus. Econ. Stat. 1988, 6, 287–296. [Google Scholar] [CrossRef]
- Tang, L.; Song, J.; Belin, T.R.; Unützer, J. A comparison of imputation methods in a longitudinal randomized clinical trial. Stat. Med. 2005, 24, 2111–2128. [Google Scholar] [CrossRef] [PubMed]
- Groves, R.M.; Dillman, D.A.; Eltinge, J.L.; Little, R.J.A. Survey Nonresponse; Wiley-Interscience: Hoboken, NJ, USA, 2002. [Google Scholar]
- Korn, E.; Graubard, B. Analysis of Health Surveys; Wiley-Interscience: Hoboken, NJ, USA, 1999. [Google Scholar]
- Benjamini, Y.; Hochberg, Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J. R. Stat. Soc. Ser. B 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Afifi, A.A.; Kotlerman, J.B.; Ettner, S.L.; Cowan, M. Methods for Improving Regression Analysis for Skewed Continuous or Counted Responses. Annu. Rev. Public Health 2007, 28, 95–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bernard, H. Research Methods in Anthropology-Qualitative and Quantitative Approaches; Sage Publications: Thousand Oaks, CA, USA, 2002. [Google Scholar]
- Emerson, R.; Fretz, R.; Shaw, L. Writing Ethnographic Fieldnotes; University of Chicago Press: Chicago, IL, USA, 2011. [Google Scholar]
- Mundt, J.C.; Vogel, A.P.; Feltner, D.E.; Lenderking, W.R. Vocal acoustic biomarkers of depression severity and treatment response. Biol. Psychiatry 2012, 72, 580–587. [Google Scholar] [CrossRef] [PubMed]
- Hashim, N.W.; Wilkes, M.; Salomon, R.; Meggs, J.; France, D.J. Evaluation of Voice Acoustics as Predictors of Clinical Depression Scores. J. Voice 2017, 31, 256.e1–256.e6. [Google Scholar] [CrossRef] [PubMed]
- Faurholt-Jepsen, M.; Busk, J.; Frost, M.; Vinberg, M.; Christensen, E.M.; Winther, O.; Bardram, J.E.; Kessing, L.V. Voice analysis as an objective state marker in bipolar disorder. Transl. Psychiatry 2016, 6, e856. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nicodemus, K.K.; Elvevåg, B.; Foltz, P.W.; Rosenstein, M.; Diaz-Asper, C.; Weinberger, D.R. Category fluency, latent semantic analysis and schizophrenia: A candidate gene approach. Cortex 2014, 55, 182–191. [Google Scholar] [CrossRef] [PubMed]
- Miller, W.L.; Crabtree, B.F. Primary care research: A multimethod typology and qualitative road map. In Doing Qualitative Research; Sage Publications: Newbury Park, CA, USA, 1992; Volume 3, pp. 3–28. ISBN 0761914978. [Google Scholar]
- Ryan, G.W.; Bernard, H.R. Techniques to identify themes in qualitative data. Field Methods 2003, 15, 85–109. [Google Scholar] [CrossRef]
- Saint, S.; Kowalski, C.P.; Forman, J.; Damschroder, L.; Hofer, T.P.; Kaufman, S.R.; Creswell, J.W.; Krein, S.L. A Multicenter Qualitative Study on Preventing Hospital-Acquired Urinary Tract Infection in US Hospitals. Infect. Control Hosp. Epidemiol. 2008, 29, 333–341. [Google Scholar] [CrossRef] [PubMed]
- MacQueen, K.M.; McLellan, E.; Kay, K.; Milstein, B. Codebook development for team-based qualitative analysis. Field methods 1998, 10, 31–36. [Google Scholar] [CrossRef]
- Maxwell, J.A. Qualitative Research Design: An Interactive Approach (2nd Edition); Sage Publications: Thousand Oaks, CA, 2005; ISBN 9781412981194. [Google Scholar]
- Creswell, J. Qualitative Inquiry and Research Design: Choosing Among Five Approaches; Sage Publications: Thousand Oaks, CA, 2012; ISBN 9781412916066. [Google Scholar]
- Springgate, B.F.; Allen, C.; Jones, C.; Lovera, S.; Meyers, D.; Campbell, L.; Palinkas, L.A.; Wells, K.B. Rapid community participatory assessment of health care in post-storm New Orleans. Am. J. Prev. Med. 2009, 37, S237–S243. [Google Scholar] [CrossRef] [PubMed]


© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Springgate, B.F.; Arevian, A.C.; Wennerstrom, A.; Johnson, A.J.; Eisenman, D.P.; Sugarman, O.K.; Haywood, C.G.; Trapido, E.J.; Sherbourne, C.D.; Everett, A.; et al. Community Resilience Learning Collaborative and Research Network (C-LEARN): Study Protocol with Participatory Planning for a Randomized, Comparative Effectiveness Trial. Int. J. Environ. Res. Public Health 2018, 15, 1683. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15081683
Springgate BF, Arevian AC, Wennerstrom A, Johnson AJ, Eisenman DP, Sugarman OK, Haywood CG, Trapido EJ, Sherbourne CD, Everett A, et al. Community Resilience Learning Collaborative and Research Network (C-LEARN): Study Protocol with Participatory Planning for a Randomized, Comparative Effectiveness Trial. International Journal of Environmental Research and Public Health. 2018; 15(8):1683. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15081683
Chicago/Turabian StyleSpringgate, Benjamin F., Armen C. Arevian, Ashley Wennerstrom, Arthur J. Johnson, David P. Eisenman, Olivia K. Sugarman, Catherine G. Haywood, Edward J. Trapido, Cathy D. Sherbourne, Ashley Everett, and et al. 2018. "Community Resilience Learning Collaborative and Research Network (C-LEARN): Study Protocol with Participatory Planning for a Randomized, Comparative Effectiveness Trial" International Journal of Environmental Research and Public Health 15, no. 8: 1683. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15081683