The Effectiveness and Cost-Effectiveness of Screening for HIV in Migrants in the EU/EEA: A Systematic Review


 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Methods
- Should newly arrived migrants be screened for HIV? Who should be targeted and how?
- What implementation considerations should be considered when screening for HIV in newly arrived migrants to the EU/EEA?
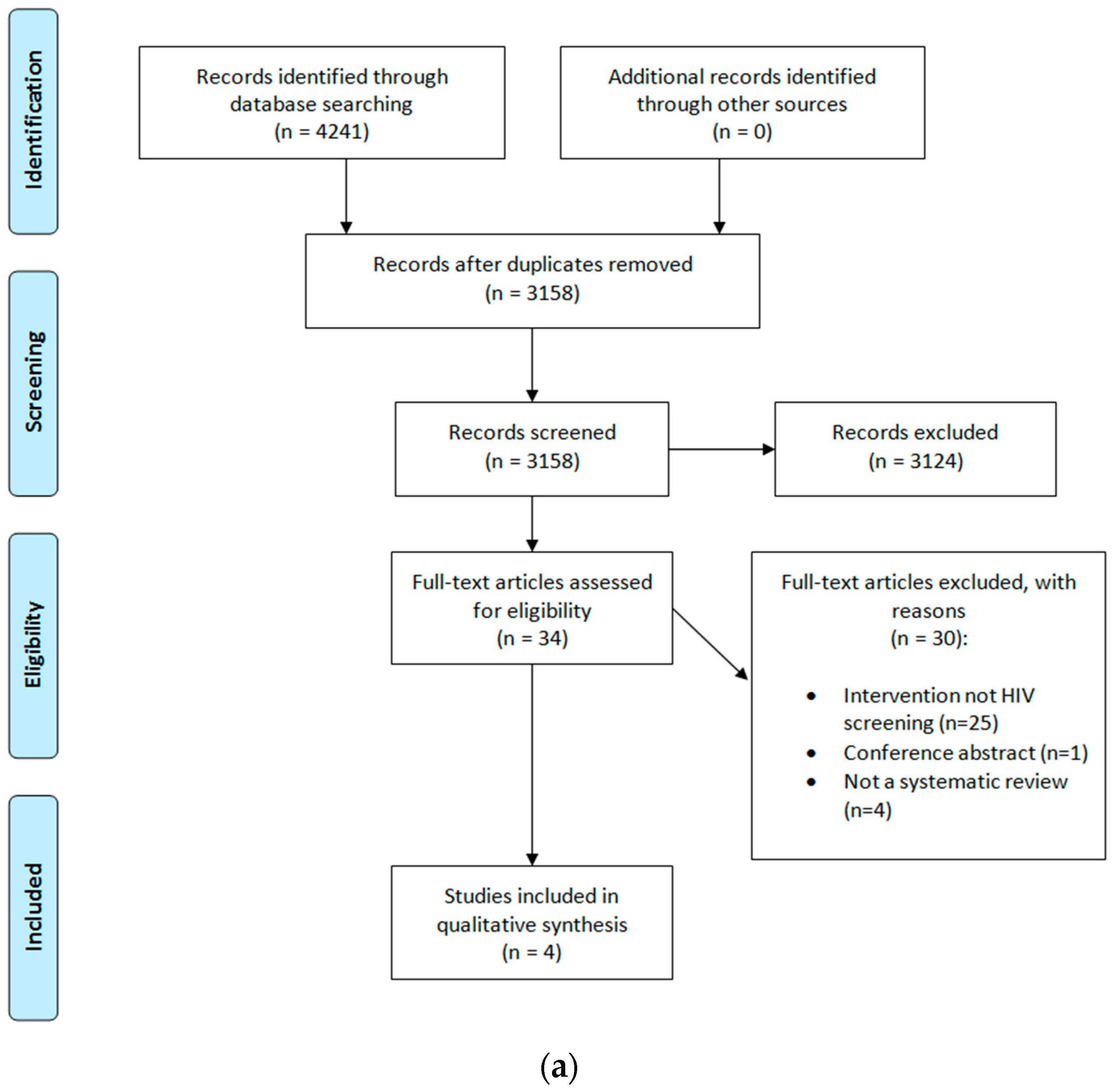
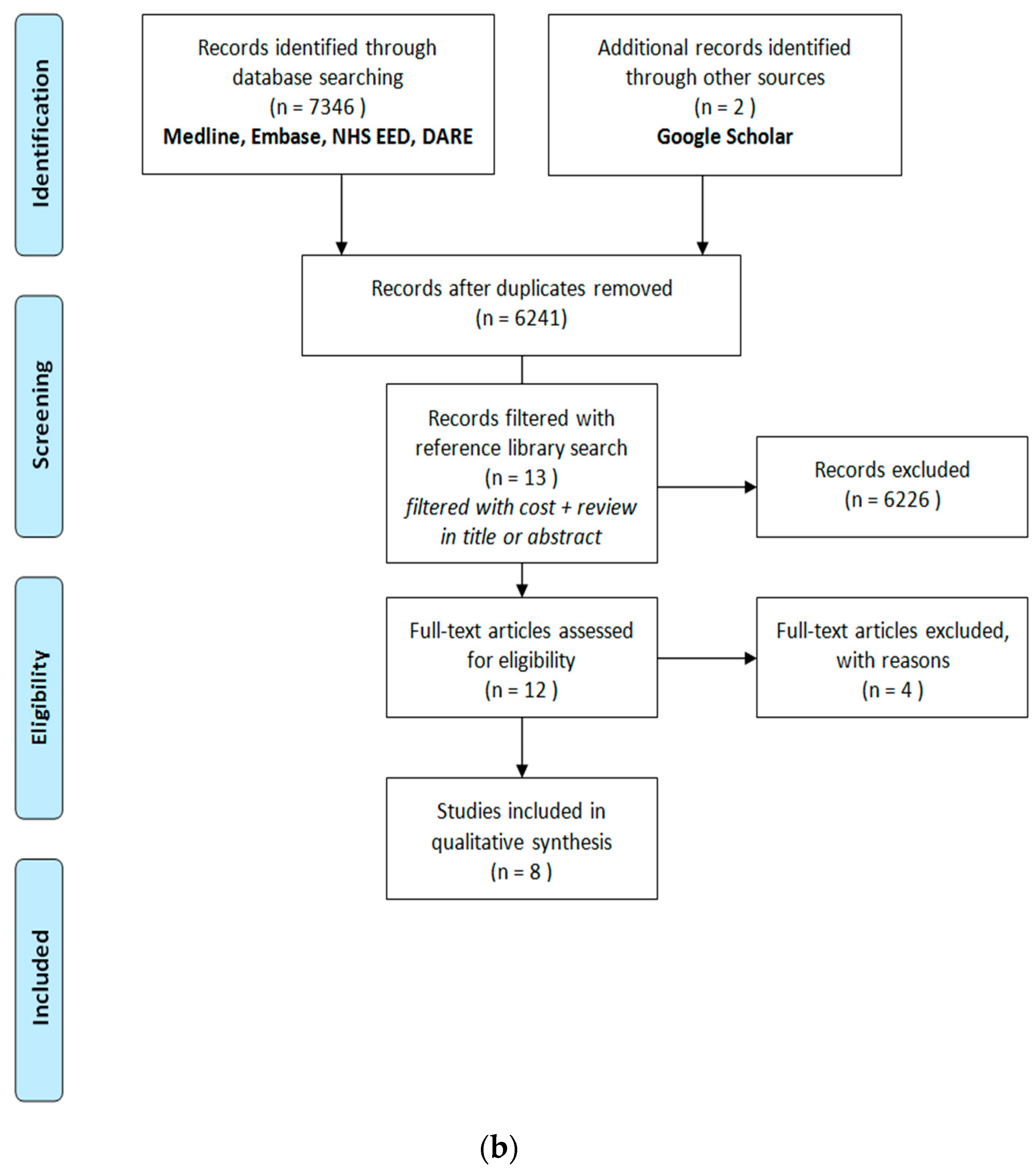
3. Results
Cost-Effectiveness
4. Discussion
4.1. Implementation Issues
4.2. Public Health Considerations
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

Appendix B. Search Strategy
- (hiv or hiv1$ or hiv2$).mp. (277,362)
- (human adj (immunedeficienc$ or immune deficienc$ or immunodeficienc$ or immuno deficienc$)).tw. (72,052)
- Acquired Immunodeficiency Syndrome/(74,163)
- (acquired adj (immunedeficienc$ or immune deficienc$ or immunodeficienc$ or immuno deficienc$)).tw. (20,316)
- aids.hw. (59,809)
- (aids adj2 (infect$ or virus$)).tw. (5953)
- or/1–6 (346,871)
- exp Mass Screening/(107,701)
- (screened or screening?).tw. (417,187)
- Early Diagnosis/(18,989)
- [or/8–15] (0)
- [or/17–19] (0)
- [remove duplicates from 24] (0)
- (hiv or hiv1$ or hiv2$).mp. (277,362)
- (human adj (immunedeficienc$ or immune deficienc$ or immunodeficienc$ or immuno deficienc$)).tw. (72,052)
- Acquired Immunodeficiency Syndrome/(74,163)
- (acquired adj (immunedeficienc$ or immune deficienc$ or immunodeficienc$ or immuno deficienc$)).tw. (20,316)
- aids.hw. (59,809)
- (aids adj2 (infect$ or virus$)).tw. (5953)
- or/14–19 (346,871)
- exp Mass Screening/(107,701)
- (screened or screening?).tw. (417,187)
- Early Diagnosis/(18,989)
- ((case? or early) adj2 (detected or detection? or diagnos$ or discover$)).tw. (149,145)
- exp Population Surveillance/(55,996)
- (disease? adj2 surveillance).tw. (4047)
- Contact Tracing/(3517)
- contact tracing.tw. (1151)
- or/21–28 (646,541)
- meta analysis.mp,pt. (90,987)
- review.pt. (2,033,544)
- search$.tw. (253,118)
- or/30–32 (2,219,856)
- animals/not (humans/and animals/) (4,191,261)
- 33 not 34 (2,063,224)
- 20 and 29 and 35 (3419)
- 36 and (2010$ or 2011$ or 2012$ or 2013$ or 2014$ or 2015$ or 2016$).ed. (1178)
- remove duplicates from 37 (1137)
- (hiv or hiv1$ or hiv2$).mp. (313,646)
- exp Human immunodeficiency virus infection/(322,600)
- exp Human immunodeficiency virus/(156,358)
- (human adj (immunedeficienc$ or immune deficienc$ or immunodeficienc$ or immuno deficienc$)).tw. (81,168)
- (acquired adj (immunedeficienc$ or immune deficienc$ or immunodeficienc$ or immuno deficienc$)).tw. (22,202)
- aids.hw. (11,098)
- (aids adj2 (infect$ or virus$)).tw. (6778)
- or/1–7 (447,157)
- exp mass screening/(178,092)
- (screened or screening?).tw. (612,553)
- anonymous testing/(221)
- early diagnosis/(82,014)
- ((case? or early) adj2 (detected or detection? or diagnos$ or discover$)).tw. (223,587)
- exp health survey/(182,039)
- (disease? adj2 surveillance).tw. (5133)
- contact examination/(2820)
- contact tracing.tw. (1443)
- or/9–17 (1,076,977)
- meta analys$.mp. (166,352)
- search$.tw. (360,207)
- review.pt. (2,126,810)
- or/19–21 (2,466,318)
- animals/not (humans/and animals/) (1,150,973)
- 22 not 23 (2,401,775)
- 8 and 18 and 24 (5168)
- 25 and (2010$ or 2011$ or 2012$ or 2013$ or 2014$ or 2015$ or 2016$).dd. (2136)
- remove duplicates from 26 (2080)
- ID
- Search
- #1
- (hiv or hiv1* or hiv2*) (15,056)
- #2
- human next (immunedeficienc* or immune deficienc* or immunodeficienc* or immuno deficienc*):ti,ab (2799)
- #3
- MeSH descriptor: [Acquired Immunodeficiency Syndrome] this term only (1248)
- #4
- acquired next (immunedeficienc* or immune deficienc* or immunodeficienc* or immuno deficienc*):ti,ab (646)
- #5
- aids:kw (2253)
- #6
- aids near/2 (infect* or virus*):ti,ab (457)
- #7
- #1 or #2 or #3 or #4 or #5 or #6 (16,330)
- #8
- MeSH descriptor: [Mass Screening] explode all trees (5443)
- #9
- (screened or screening*):ti,ab (22,416)
- #10
- MeSH descriptor: [Early Diagnosis] this term only (538)
- #11
- (case* or early) near/2 (detected or detection* or diagnos* or discover*):ti,ab (3639)
- #12
- MeSH descriptor: [Population Surveillance] explode all trees (709)
- #13
- disease* near/2 surveillance:ti,ab (30)
- #14
- MeSH descriptor: [Contact Tracing] this term only (96)
- #15
- contact tracing:ti,ab (30)
- #16
- #8 or #9 or #10 or #11 or #12 or #13 or #14 or #15 (27,248)
- #17
- #7 and #16 (1173)
- #18
- #17 in Other Reviews (27)
- #19
- #17 in Cochrane Reviews (Reviews and Protocols) (195)
- S27
- S23 AND S26 297
- S26
- S24 OR S25 2,588,490
- S25
- EM 2010 or EM 2011 or EM 2012 or EM 2013 or EM 2014 or EM 2015 or EM 2016 2,411,599
- S24
- PY 2010 or PY 2011 or PY 2012 or PY 2013 or PY 2014 or PY 2015 or PY 2016 2,338,383
- S23
- S8 AND S16 AND S22 527
- S22
- S17 OR S18 OR S19 OR S20 OR S21 220,800
- S21
- (TI meta analy* or AB meta analy*) 29,599
- S20
- (MH “Meta Analysis”) 24,899
- S19
- PT review 141,121
- S18
- PT systematic review 53,358
- S17
- (MH “Systematic Review”) 37,370
- S16
- S9 OR S10 OR S11 OR S12 OR S13 OR S14 OR S15 154,560
- S15
- contact tracing 1457
- S14
- (disease* or population) N2 surveillance 18,647
- S13
- (MH “Population Surveillance+”) 5939
- S12
- (case* or early) N2 (detected or detection* or diagnos* or discover*) 29,738
- S11
- (MH “Early Diagnosis”) 4469
- S10
- TI ((screened or screening*)) OR AB ((screened or screening*)) 78,064
- S9
- (MH “Health Screening+”) 62,689
- S8
- S1 OR S2 OR S3 OR S4 OR S5 S6 OR S7 108,656
- S7
- TX aids N2 (infect* or virus*) 10,961
- S6
- MW aids 22,515
- S5
- TX acquired N1 (immunedeficienc* or immune deficienc* or immunodeficienc* or immuno deficienc*) 21,283
- S4
- (MH “Acquired Immunodeficiency Syndrome”) 13,583
- S3
- TX human N1 (immunedeficienc* or immune deficienc* or immunodeficienc* or immuno deficienc*) 23,570
- S2
- (hiv or hiv1* or hiv2*) 79,932
- S1
- (MH “Human Immunodeficiency Virus+”) 6511
Appendix C

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Population: | Migrants and refugees to EU/EEA countries (primary population of interest); will consider indirect evidence of marginalized groups in settings of high HIV prevalence |
| Intervention: | Voluntary testing for HIV |
| Outcome: | Testing outcomes: testing uptake, HIV incidence Treatment outcomes: Efficacy, withdrawals |
References
- Salama, P.; Dondero, T.J. HIV surveillance in complex emergencies. AIDS 2001, 15, S4–S12. [Google Scholar] [CrossRef] [PubMed]
- Europe ECfDPaCWROf. HIV/AIDS Surveillance in Europe 2017–2016 Data; ECDC: Stockholm, Sweden, 2017. [Google Scholar]
- Fakoya, I.; Reynolds, R.; Caswell, G.; Shiripinda, I. Barriers to HIV testing for migrant black Africans in Western Europe. HIV Med. 2008, 9, 23–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rice, B.D.; Elford, J.; Delpech, V.C. A new method to assign country of HIV infection among heterosexuals born abroad and diagnosed with HIV. AIDS 2012, 26, 1961–1966. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Desgrées-du-Loû, A.P.J.; Ravalihasy, A.; Gosselin, A.; Supervie, V.; Panjo, H.; Bajos, N.; Lert, F.; Lydié, N.; Dray-Spira, R. Sub-Saharan African migrants living with HIV acquired after migration, France, ANRS PARCOURS study, 2012 to 2013. Eurosurveillance 2015, 20, 30065. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-del Arco, D.; Fakoya, I.; Thomadakis, C.; Pantazis, N.; Touloumi, G.; Gennotte, A.-F.; Zuure, F.; Barros, H.; Staehelin, C.; GÃpel, S.; et al. High levels of postmigration HIV acquisition within nine European countries. AIDS 2017, 31, 1979–1988. [Google Scholar] [CrossRef] [PubMed]
- Pharris, A.; Quinten, C.; Noori, T.; Amato-Gauci, A.J.; van Sighem, A. Estimating HIV incidence and number of undiagnosed individuals living with HIV in the European Union/European Economic Area, 2015. Eurosurveillance 2016, 21, 30417. [Google Scholar] [CrossRef] [PubMed]
- Hernando, V.; Alvárez-del Arco, D.; Alejos, B.; Monge, S.; Amato-Gauci, A.J.; Noori, T.; Pharris, A.; del Amo, J. HIV Infection in Migrant Populations in the European Union and European Economic Area in 2007–2012: An Epidemic on the Move. JAIDS J. Acquir. Immune Defic. Syndr. 2015, 70, 204–211. [Google Scholar] [CrossRef] [PubMed]
- Joint United Nations Programme on HA. 90-90-90 An Ambitious Treatment Target to Help End the AIDS Epidemic; UNAIDS: Geneva, Switzerland, 2014. [Google Scholar]
- European Centre for Disease Prevention and Control. HIV Testing: Increasing Uptake and Effectiveness in the European Union; European Centre for Disease Prevention and Control: Stockholm, Sweden, 2010. [Google Scholar]
- Mounier-Jack, S.; Nielsen, S.; Coker, R.J. HIV testing strategies across European countries. HIV Med. 2008, 9, 13–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Centre for Disease Prevention and Control. HIV and migrants. In Monitoring Implementation of the Dublin Declaration on Partnership to Fight HIV/AIDS in Europe and Central Asia; European Centre for Disease Prevention and Control: Stockholm, Sweden, 2017. [Google Scholar]
- Alvarez-Del Arco, D.; Monge, S.; Caro-Murillo, A.M.; Ramirez-Rubio, O.; Azcoaga-Lorenzo, A.; Belza, M.J.; Rivero-Montesdeoca, Y.; Noori, T.; Del Amo, J. HIV testing policies for migrants and ethnic minorities in EU/EFTA Member States. Eur. J. Public Health 2014, 24, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Broeckaert, L.; Challacombe, L. Rapid Point-of-Care HIV Testing: A Review of the Evidence; Canadian AIDS Treatment Information Exchange (CATIE): Toronto, ON, Canada, 2015. [Google Scholar]
- World Health Organization. Consolidated Guidelines on the Use of Antiretroviral Drugs for Treating and Preventing HIV Infection; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Mascolini, M. Late HIV diagnosis: Predictors, costs, consequences, and solutions. Res. Initiat. 2011, 16, 5. [Google Scholar]
- Ager, A.; Strang, A. Understanding Integration: A Conceptual Framework. J. Refug. Stud. 2008, 21, 166–191. [Google Scholar] [CrossRef] [Green Version]
- Pottie, K.; Mayhew, A.; Morton, R.; Greenaway, C.; Akl, E.; Rahman, P. Prevention and assessment of infectious diseases among children and adult migrants arriving to the European Union/European Economic Association: A protocol for a suite of systematic reviews for public health and health systems. BMJ Open 2017. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alahdab, F.; Alsawas, M.; Murad, M.H. Where should preappraised evidence summaries and guidelines place in a pyramid? Evid. Based Med. 2016. [Google Scholar] [CrossRef] [PubMed]
- Murad, M.H.; Asi, N.; Alsawas, M.; Alahdab, F. New evidence pyramid. Evid. Based Med. 2016, 21, 125–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shea, B.J.; Grimshaw, J.M.; Wells, G.A.; Boers, M.; Andersson, N.; Hamel, C.; Porter, A.C.; Tugwell, P.; Moher, D.; Bouter, L.M. Development of AMSTAR: A measurement tool to assess the methodological quality of systematic reviews. BMC Med. Res. Methodol. 2007, 7, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wells, G.; Shea, B.; O’Connell, B. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 10 July 2017).
- Alonso-Coello, P.; Schünemann, H.J.; Moberg, J.; Brignardello-Petersen, R.; Akl, E.A.; Davoli, M.; Treweek, S.; Mustafa, R.; Rada, G.; Rosenbaum, S.; et al. GRADE Evidence to Decision (EtD) frameworks: A systematic and transparent approach to making well informed healthcare choices. 1: Introduction. Br. Med. J. 2016, 353, i2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Information Center on Health Services Research and Health Care Technology. Health Economics Information Resources: A Self-Study Course; National Information Center on Health Services Research and Health Care Technology: Bethesda, MD, USA, 2016.
- Pottie, K.; Medu, O.; Welch, V.; Dahal, G.P.; Tyndall, M.; Rader, T.; Wells, G. Effect of rapid HIV testing on HIV incidence and services in populations at high risk for HIV exposure: An equity-focused systematic review. BMJ Open 2014, 4. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, C.E.; Fonner, V.A.; Sweat, M.D.; Okero, F.A.; Baggaley, R.; O’Reilly, K.R. Provider-Initiated HIV Testing and Counseling in Low- and Middle-Income Countries: A Systematic Review. AIDS Behav. 2013, 17, 1571–1590. [Google Scholar] [CrossRef] [PubMed]
- Chou, R.; Selph, S.; Dana, T.; Bougatsos, C.; Zakher, B.; Blazina, I.; Korthuis, P.T. Screening for HIV: Systematic Review to Update the U.S. Preventive Services Task Force Recommendation; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2012.
- Desai, M.; Woodhall, S.C.; Nardone, A.; Burns, F.; Mercey, D.; Gilson, R. Active recall to increase HIV and STI testing: A systematic review. Sex. Transm. Infect. 2015, 91, 314–323. [Google Scholar] [CrossRef] [PubMed]
- Farnham, P.G.; Gorsky, R.D.; Holtgrave, D.R.; Jones, W.K.; Guinan, M.E. Counseling and testing for HIV prevention: Costs, effects, and cost-effectiveness of more rapid screening tests. Public Health Rep. 1996, 111, 44–54. [Google Scholar] [PubMed]
- Kassler, W.J.; Dillon, B.A.; Haley, C.; Jones, W.K.; Goldman, A. On-site, rapid HIV testing with same-day results and counseling. AIDS 1997, 11, 1045–1051. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilkinson, D.; Wilkinson, N.; Lombard, C.; Martin, D.; Smith, A.; Floyd, K.; Ballard, R. On-site HIV testing in resource-poor settings: Is one rapid test enough? AIDS 1997, 11, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Kallenborn, J.C.; Price, T.G.; Carrico, R.; Davidson, A.B. Emergency Department Management of Occupational Exposures: Cost Analysis of Rapid HIV Test. Infect. Control Hosp. Epidemiol. 2001, 22, 289–293. [Google Scholar] [CrossRef] [PubMed]
- Ekwueme, D.U.; Pinkerton, S.D.; Holtgrave, D.R.; Branson, B.M. Cost comparison of three HIV counseling and testing technologies. Am. J. Prev. Med. 2003, 25, 112–121. [Google Scholar] [CrossRef]
- Doyle, N.M.; Levison, J.E.; Gardner, M.O. Rapid HIV versus enzyme-linked immunosorbent assay screening in a low-risk Mexican American population presenting in labor: A cost-effectiveness analysis. Am. J. Obstet. Gynecol. 2005, 193, 1280–1285. [Google Scholar] [CrossRef] [PubMed]
- Paltiel, A.D.; Weinstein, M.C.; Kimmel, A.D.; Seage, G.R.; Losina, E.; Zhang, H.; Freedberg, K.A.; Walensky, R.P. Expanded Screening for HIV in the United States—An Analysis of Cost-Effectiveness. N. Engl. J. Med. 2005, 352, 586–595. [Google Scholar] [CrossRef] [PubMed]
- Vickerman, P.; Terris-Prestholt, F.; Delany, S.; Kumaranayake, L.; Rees, H.; Watts, C. Are targeted HIV prevention activities cost-effective in high prevalence settings? Results from a sexually transmitted infection treatment project for sex workers in Johannesburg, South Africa. Sex. Transm. Dis. 2006, 33, S122–S132. [Google Scholar] [CrossRef] [PubMed]
- Walensky, R.P.; Reichmann, W.M.; Arbelaez, C.; Wright, E.; Katz, J.N.; Seage, G.R., 3rd; Safren, S.A.; Hare, A.Q.; Novais, A.; Losina, E. Counselor-Versus Provider-Based HIV Screening in the Emergency Department: Results From the Universal Screening for HIV Infection in the Emergency Room (USHER) Randomized Controlled Trial. Ann. Emerg. Med. 2011, 58, S126–S132. [Google Scholar] [CrossRef] [PubMed]
- Schünemann, H.J.; Tugwell, P.; Reeves, B.C.; Akl, E.A.; Santesso, N.; Spencer, F.A.; Shea, B.; Wells, G.; Helfand, M. Non-randomized studies as a source of complementary, sequential or replacement evidence for randomized controlled trials in systematic reviews on the effects of interventions. Res. Synth. Methods 2013, 4, 49–62. [Google Scholar] [CrossRef] [PubMed]
- Haukoos, J.S.; Hopkins, E.; Conroy, A.A.; Silverman, M.; Byyny, R.L.; Eisert, S.; Thrun, M.W.; Wilson, M.L.; Hutchinson, A.B.; Forsyth, J.; et al. Routine opt-out rapid hiv screening and detection of hiv infection in emergency department patients. JAMA 2010, 304, 284–292. [Google Scholar] [CrossRef] [PubMed]
- Lundgren, J.D.; Babiker, A.G.; Gordin, F.; Emery, S.; Grund, B.; Sharma, S.; An-chalee, A. Initiation of Antiretroviral Therapy in Early Asymptomatic HIV Infection. N. Engl. J. Med. 2015, 373, 795–807. [Google Scholar] [PubMed] [Green Version]
- Alvarez-del Arco, D.; Monge, S.; Azcoaga, A.; Rio, I.; Hernando, V.; Gonzalez, C.; Alejos, B.; Caro, A.M.; Perez-Cachafeiro, S.; Ramirez-Rubio, O.; et al. HIV testing and counselling for migrant populations living in high-income countries: A systematic review. Eur. J. Public Health 2013, 23, 1039–1045. [Google Scholar] [CrossRef] [PubMed]
- Deblonde, J.; De Koker, P.; Hamers, F.F.; Fontaine, J.; Luchters, S.; Temmerman, M. Barriers to HIV testing in Europe: A systematic review. Eur. J. Public Health 2010, 20, 422–432. [Google Scholar] [CrossRef] [PubMed]
- Blondell, S.J.; Kitter, B.; Griffin, M.P.; Durham, J. Barriers and Facilitators to HIV Testing in Migrants in High-Income Countries: A Systematic Review. AIDS Behav. 2015, 19, 2012–2024. [Google Scholar] [CrossRef] [PubMed]
- Dias, S.; Gama, A.; Pingarilho, M.; Simões, D.; Mendão, L. Health Services Use and HIV Prevalence Among Migrant and National Female Sex Workers in Portugal: Are We Providing the Services Needed? AIDS Behav. 2017, 21, 2316–2321. [Google Scholar] [CrossRef] [PubMed]
- Aids & Mobility Europe. Sweden: Mikael’s Testimony about His Friend Sebastian: Denied the Medication He Needed to Live; Aids and Mobility Europe: Hanover, Germany, 2006; pp. 27–29. [Google Scholar]
- Manirankunda, L.; Loos, J.; Alou, T.A.; Colebunders, R.; Nöstlinger, C. “It’s Better Not To Know”: Perceived Barriers to HIV Voluntary Counseling and Testing among Sub-Saharan African Migrants in Belgium. AIDS Educ. Prev. 2009, 21, 582–593. [Google Scholar] [CrossRef] [PubMed]
- Musheke, M.; Ntalasha, H.; Gari, S.; McKenzie, O.; Bond, V.; Martin-Hilber, A.; Merten, S. A systematic review of qualitative findings on factors enabling and deterring uptake of HIV testing in Sub-Saharan Africa. BMC Public Health 2013, 13, 220. [Google Scholar] [CrossRef] [PubMed]
- Control ECfDPa. Antenatal Screening for HIV, Hepatitis B, Syphilis and Rubella Susceptability in the EU/EEA; Report No.: 9789291938445; ECDC: Stockholm, Sweden, 2017. [Google Scholar]
- Australasian Society for Infectious Diseases. Recommendations for Comprehensive Post-Arrival Health Assessment for People from Refugee-Like Backgrounds; Australasian Society for Infectious Diseases: Surry Hills, Australia, 2016. [Google Scholar]
- Centre HPS. Infectious Disease Assessment for Migrants; Health Protection Surveillance Centre, Committee MHASoHSA: Dublin, Ireland, 2015. [Google Scholar]
- Pottie, K.; Greenaway, C.; Feightner, J. Evidence-based clinical guidelines for immigrants and refugees. CMAJ 2011, 183, E824–E925. [Google Scholar] [CrossRef] [PubMed]
- Health USDo, Human Services/Centers for Disease Control and Prevention. Screening for HIV Infection during the Refugee Domestic Medical Examination; CDC: Atlanta, GA, USA, 2013. [Google Scholar]
- Navaza, B.; Abarca, B.; Bisoffi, F.; Pool, R.; Roura, M. Provider-Initiated HIV Testing for Migrants in Spain: A Qualitative Study with Health Care Workers and Foreign-Born Sexual Minorities. PLoS ONE 2016, 11, e0150223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dias, S.; Gama, A.; Severo, M.; Barros, H. Factors associated with HIV testing among immigrants in Portugal. Int. J. Public Health 2011, 56, 559–566. [Google Scholar] [CrossRef] [PubMed]
- Cohen, M.S.; Chen, Y.Q.; McCauley, M.; Gamble, T.; Hosseinipour, M.C. Prevention of HIV-1 infection with early antiretroviral therapy. N. Engl. J. Med. 2011, 365, 493–505. [Google Scholar] [CrossRef] [PubMed]
- Marks, G.; Crepaz, N.; Janssen, R.S. Estimating sexual transmission of HIV from persons aware and unaware that they are infected with the virus in the USA. AIDS 2006, 20, 1447–1450. [Google Scholar] [CrossRef] [PubMed] [Green Version]



| Study | Design and Quality | Included Studies | Population | Intervention | Results/Outcomes |
|---|---|---|---|---|---|
| Should Voluntary Testing for HIV Infection be Offered to all Recently Arrived Migrants to the EU/EEA? | |||||
| Pottie et al., 2014 [26] | Systematic review AMSTAR 9/11 | n = 13
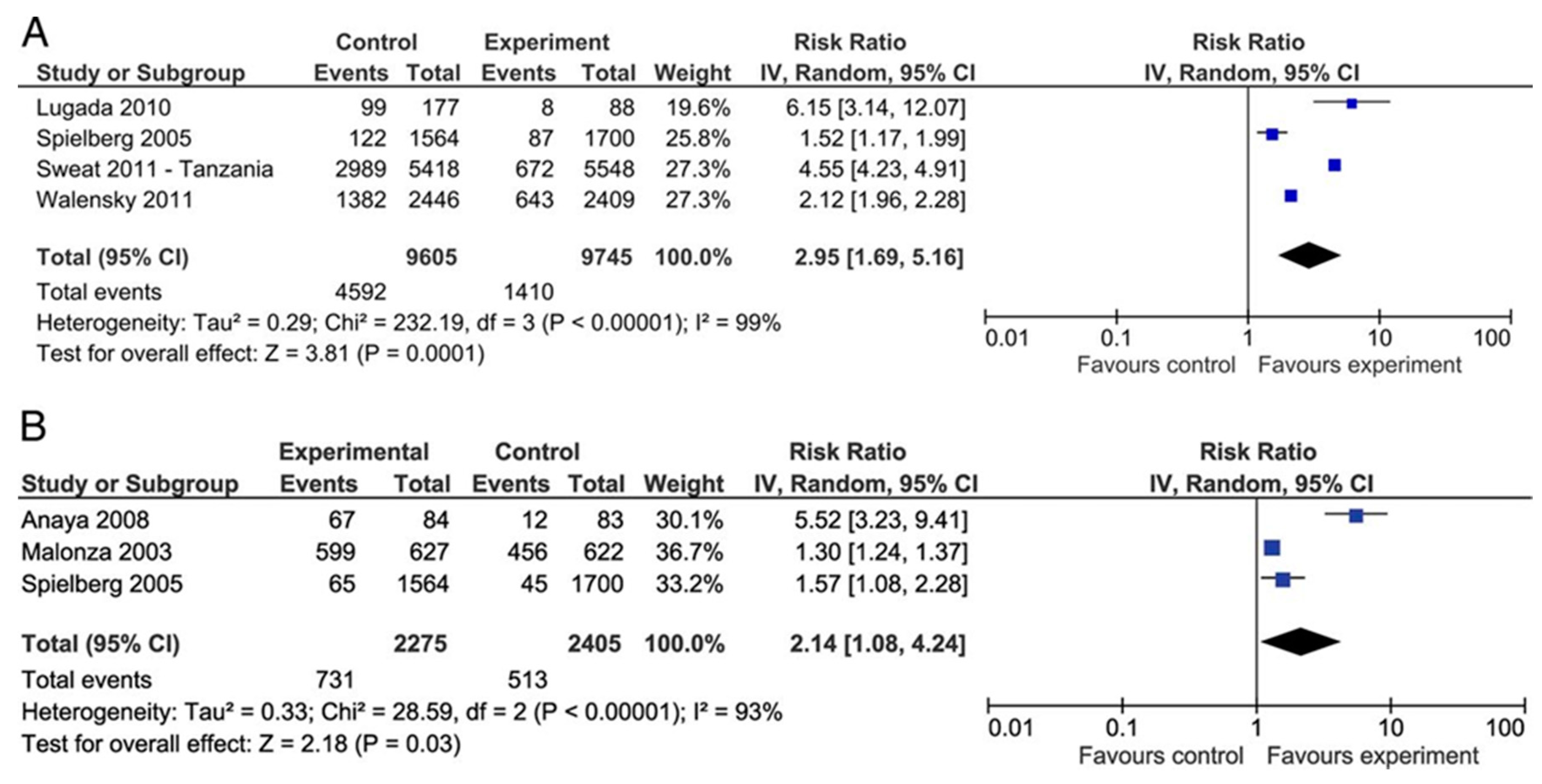
| Individuals at high risk of exposure | Facilitated voluntary enrolment; use of a rapid-testing approach (providing results within 24 h); outreach counseling, delivery of results and treatment options. | Receipt of HIV test results: Increased likelihood among participants randomized to the rapid approach study arms to receive test results (RR = 2.14, 95% CI 1.08 to 4.24) (n = 3; RCTs). Repeat HIV testing and test incidence rate: increased HIV repeat testing among those in the intervention arm (RR = 2.28, 95% CI 0.35 to 15.07) (n = 1; cluster RCT). HIV incidence 36-month period in five countries showed an 11% reduction in estimated incidence in intervention RR = 0.89, 95% CI = 0.63 to 1.24). Treatment program uptake: OR = 1.7, 95% CI 0.8 to 3.7 for the uptake of perinatal HIV-1 interventions between rapid VCT versus conventional VCT (n = 1) |
| Kennedy et al., 2013 [27] | Systematic Review AMSTAR 5/11 | n = 19
| Low- and middle-income countries; health care setting where individuals were seeking health care services other than HIV testing. Individuals, couples, or groups had to receive pre- and post-test counseling about HIV and an HIV test | Provider-initiated testing and counseling (PITC) (aligned with the 2007 WHO). | The majority of studies were conducted before WHO PITC guidelines were developed, indicating that provider-initiated testing was occurring in many locations prior to global guidance. All studies included in this review that reported rates of HIV testing uptake showed increases associated with a PITC approach. Comparing behavior in the three months preceding PITC to behavior in the three months after PITC, the percentage of participants who reported engaging in risky sex decreased and knowing their partner’s HIV status increased for both HIV-positive and HIV-negative participants. |
| AHRQ 2012 [28] | Systematic Review AMSTAR 9/11 | n= 42
| Testing for asymptomatic HIV infection in Non-pregnant adults and adolescents. | Screening Strategies | No randomized trial or observational study compared clinical outcomes between adults and adolescents screened and not screened for HIV infection. Some modeling studies have estimated the cost-effectiveness of strategies involving repeat screening. No study directly evaluated the acceptability of universal versus targeted HIV screening. One study found universal, opt-out rapid screening associated with higher likelihood of testing compared with physician-directed, targeted rapid screening (25% vs. 0.8%; relative risk [RR], 30 [95% CI, 26 to 34]). One study found universal testing associated with a higher median CD4 count and lower likelihood of CD4 count <0.200 × 109 cells/L at the time of diagnosis compared with targeted HIV screening, but these differences were not statistically significant. |
| Desai et al., 2015 [29] | Systematic Review AMSTAR 6/11 | n = 17
| HIV-negative or unknown status in all countries; Hospitals, sexual health clinics, general practice, community venues, and home sampling/testing | Active recall | SMS: OR for retesting as compared to the control group ranged between 0.93 (95% CI 0.65 to 1.33) and 5.87 (95% CI 1.16 to 29.83). The pooled OR among the observational studies was 2.19 (95% CI 1.47 to 3.23). A pooled OR for retesting among SMS group is 5.66 (95% CI 1.78 to 17.99) among 126. Phone calls: phone calls and verbal advice and counseling had higher rates of retesting OR = 2.50 (95% CI 1.3 to 4.8) compared to phone calls only. Groups receiving phone calls and verbal advice had higher rates if retesting OR = 14.0 (95% CI 1.63 to 120.09) compared to phone calls only. |
| Study | Quality/Drummond Score | Design | Population | Intervention | Cost Effectiveness | Resource Requirements |
|---|---|---|---|---|---|---|
| What are the Cost-Effectiveness and Resource Requirements of HIV Testing? | ||||||
| Farnham et al., 1996 [30] | Allowance was made for uncertainty, sensitivity analysis performed around a variety of model inputs. One-way sensitivity analysis in a decision analytic framework. Sensitivity analysis compares basic value with the breakeven value that makes the two strategies equally cost-effective. No range of values tested and no a priori justification for values tested in sensitivity analysis. There was no assumed range, as noted above, but results seem to be sensitive to plausible changes in some model inputs, especially waiting and counselling times. | Decision analytic model, societal perspective. Costs measured in 1992 U.S. dollars. | United States of America | ELISA test, and counselling and testing (C/T) vs. rapid C/T vs. no intervention | ELISA C/T: Average not incremental cost-effectiveness ratios: $1165 per correctly identified case vs. no intervention; rapid C/T $940 per correctly identified case Rapid vs. ELISA: $596 per correctly identified case | ELISA C/T: positive individual $103 per person, negative individual $33. Rapid C/T: positive individual $135 per person, negative individual $33 per person. Low to moderate costs of both strategies. |
| Kassler et al., 1997 [31] | No allowance was made of uncertainty. No sensitivity analyses. | Cost comparison, societal perspective. Comparison of testing strategies in an HIV clinic. Costs measured in 1993 U.S. dollars. | Individuals attending an anonymous testing clinic and a sexually transmitted disease (STD) clinic in Dallas, Texas | Standard C/T vs. rapid C/T | No incremental cost-effectiveness ratio calculated, not a full economic evaluation. | Cost per person receiving results and counselling: standard $151, rapid $131. Low to moderate cost savings of rapid C/T over standard C/T. |
| Wilkinson et al., 1997 [32] | No allowance was made for uncertainty. No sensitivity analyses. | Cost comparison, prospective comparison of testing strategies in a South African hospital. Costs measured in 1996 South African rand. | Resource-poor setting: adult inpatients of a rural South African district hospital | ELISA C/T vs. single rapid C/T vs. double rapid C/T. The double rapid strategy consists of two different rapid tests: a Capillus test and an Abbott test. | N/A | Cost per person counselled post-test: single rapid R 14–31.2, double rapid R 45.2, ELISA R 83.8. Cost savings of single rapid test. |
| Kallenborn et al., 2001 [33] | Some allowance made for uncertainty. Sensitivity analysis limited and discursive. Not statistically rigorous. No range of values for sensitivity analysis provided. Results overall not sensitive to whether basic or expanded regimen used, but as noted sensitivity analysis was incomplete. | Cost comparison study, retrospective chart review of Health Care Workers in an emergency department. Costs measured in 1999 U.S. dollars. | Healthcare workers | Rapid testing vs. ELISA testing | N/A. This is just a cost comparison | Total costs for 17 patients: ELISA $5966, Rapid test $466. Cost savings of switching from ELISA testing to rapid testing in health care workers. |
| Ekwueme et al., 2003 [34] | Allowance made for uncertainty. One-way sensitivity analysis performed in a cost analysis model. Range of sensitivity analysis is +/− 50% of the base value, or as wide as possible in the absence of hard data. Rank order of two-step rapid relative to standard C/T sensitive to the return rate for standard C/T, but one-step rapid consistently least expensive. | Cost analysis study using a decision analysis model, costs estimated from both societal and provider perspective, in 2000 U.S. dollars | United States of America | Standard ELISA C/T vs. both one-step (multiple rapid assays) and two-step rapid C/T (i.e., with a confirmatory Western blot test) | N/A | From both a provider and societal perspective, costs vary based on sero-status. However, one-step rapid testing is consistently the lowest cost option, and two-step rapid testing tends to be the highest cost. There appear to be cost savings of using a one-step rapid C/T protocol vs. standard ELISA testing or two-step rapid C/T. |
| Doyle et al., 2005 [35] | Allowance made for uncertainty. One-way sensitivity analysis on “sensitivity, specificity, and positive predictive values of each screening test and confirmatory Western blot test, the costs of each test, and the costs of treatments” in a decision analytic model. Range of values tested in sensitivity analysis appears to be based on published estimates but this is not explicitly stated. The Oraquick rapid test is the dominant strategy over a wide range of assumptions. Results not sensitive to plausible changes. | Decision analysis techniques: decision tree | Low risk Mexican American population, incidence 0.05% | (1) testing with enzyme linked immunosorbent assay that was confirmed by Western blot (2) testing with Oraquick rapid testing that was confirmed by Western blot | Oraquick as the primary screening test for the unknown HIV status of women who were in labor was the most cost-effective at $217,718 per HIV case that was prevented. Assuming a 70-year lifespan, this equals $3111 per life-year gained. | Oraquick cost $98 spent for each child who was HIV negative, ELISA screening cost $491. High cost of ELISA screening in a low-prevalence Mexican American population were from unnecessary treatment of women and infants with false-positive test results. Oraquick has a relatively modest costs. |
| Paltiel et al., 2005 [36] | Allowance made for uncertainty One-way sensitivity analysis performed. Range of estimates seems to be derived from published estimates/a plausible a priori estimate. Not explicitly stated. Some sensitivity to assumptions regarding background therapy, adherence to ARV therapy, and rates of linkage to care. This does not significantly change the results, may simply change whether screening every three or five years is preferable. Results regarding rapid vs. conventional testing are unclear and sensitive to plausible changes in background testing rates, acceptance and linkage to care, and rate of secondary transmission. | A stochastic model (individual model) of HIV screening and treatment: The cost-effectiveness of preventing AIDS, and a complications model (CEPAC model) | United States of America | (i) routine, voluntary HIV, CTR (counselling, testing and referral); (ii) current practice: background testing OR presentation with opportunistic infections in three target populations: | Compared to current practice, current practice plus one time ELISA costs $36,000 per Quality-Adjusted Life Year (QALY) gained; current practice plus ELISA every 5 years costs $50,000 per QALY gained; current practice plus ELISA every 3 years costs $63,000; current practics plus ELISA every year costs $100,000 per QALY gained | For HIV infected persons only: current practice costs: $78,100 lifetime cost per person; current practice plus one time ELISA costs $80,700; current practice plus ELISA every five years costs $89,000; current practice plus ELISA every 3 years costs $92,500; current practices plus ELISA every year costs $98,600 For general population: current practice costs $32,700 lifetime cost per person, current practice plus one-time ELISA costs $33,800; current practice plus ELISA every five years costs $37,300 current practice plus ELISA every three years costs $38,900; current practices plus ELISA every year costs $41,700. More frequent screening produced large costs, due to screening test cost plus the cost of managing false positives. |
| Vickerman et al., 2006 [37] | Allowance made for uncertainty. Univariate sensitivity analysis for a number of dimensions. Model input ranges derived from published estimates. The cost-effectiveness of the POC rapid test is sensitive to test cost. | Dynamic compartmental model | Female sex workers | A range of sensitivities of point of care (POC) tests. | If the POC test cost $2 per test (2004 $US), and was 70% sensitive, then POC test would cost $152 per additional HIV infection averted, which is cost-effective. If the cost of the POC test was $1 and the sensitivity was 80%, the cost per HIV infection averted would have been $58, which is cost-effective. When the POC test has a low sensitivity, of 50%, POC is not cost-effective. | Possible cost savings from using POC tests include the reduction in the number of STI clinic attenders receiving treatment. Assuming each test takes an extra 0.3 h to undertake, POC testing costs for 4 years is $13,399 if the test cost $1 and $34 621 if the test cost $3 (in 2004 U.S.$). Moderate costs. |
| Certainty Assessment | Effect | Certainty | Importance | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No. of Studies | Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | Relative (95% CI) | Absolute (95% CI) | ||||
| Outcome: Testing Uptake (follow up: 7 to 24 months) | ||||||||||||
| 3 (9745 participants) | Randomised trials | Serious concerns, allocation concealment was unclear, blinding of intervention not possible, and inability to determine blinding of researchers | No serious inconsistency | No serious indirectness | No serious imprecision | No other concerns | RR 2.95 (1.69 to 5.16) | Without rapid testing for HIV | With rapid testing for HIV | Difference | Moderate | Critical |
| General population | ||||||||||||
| 0.1% | 0.3% (0.2 to 0.5) | 0.2% more (0.1 more to 0.4 more) | ||||||||||
| High risk population | ||||||||||||
| 2.0% | 5.9% (3.4 to 10.3) | 3.9% more (1.4 more to 8.3 more) | ||||||||||
| Outcome: HIV incidence (follow up: 36 months) | ||||||||||||
| 1 (8324 participants) | Randomised trial | Serious concerns Allocation concealment was unclear, blinding of intervention not possible and inability to determine blinding of researchers | No serious inconsistency | No serious indirectness | Serious imprecision | No other concerns | RR 0.89 (0.63 to 1.24) | Low risk population | Low | Critical | ||
| 7.2% | 6.4% (4.5 to 8.9) | 0.8% fewer (2.7 fewer to 1.7 more) | ||||||||||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pottie, K.; Lotfi, T.; Kilzar, L.; Howeiss, P.; Rizk, N.; Akl, E.A.; Dias, S.; Biggs, B.-A.; Christensen, R.; Rahman, P.; et al. The Effectiveness and Cost-Effectiveness of Screening for HIV in Migrants in the EU/EEA: A Systematic Review. Int. J. Environ. Res. Public Health 2018, 15, 1700. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15081700
Pottie K, Lotfi T, Kilzar L, Howeiss P, Rizk N, Akl EA, Dias S, Biggs B-A, Christensen R, Rahman P, et al. The Effectiveness and Cost-Effectiveness of Screening for HIV in Migrants in the EU/EEA: A Systematic Review. International Journal of Environmental Research and Public Health. 2018; 15(8):1700. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15081700
Chicago/Turabian StylePottie, Kevin, Tamara Lotfi, Lama Kilzar, Pamela Howeiss, Nesrine Rizk, Elie A. Akl, Sonia Dias, Beverly-Ann Biggs, Robin Christensen, Prinon Rahman, and et al. 2018. "The Effectiveness and Cost-Effectiveness of Screening for HIV in Migrants in the EU/EEA: A Systematic Review" International Journal of Environmental Research and Public Health 15, no. 8: 1700. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15081700