Mind–Body (Baduanjin) Exercise Prescription for Chronic Obstructive Pulmonary Disease: A Systematic Review with Meta-Analysis


Abstract
:1. Introduction
2. Methods
2.1. Data Sources
2.2. Inclusion Criteria and Study Selection
2.3. Study Quality Assessment for Eligible Studies Selected
2.4. Data Extraction and Synthesis
3. Results
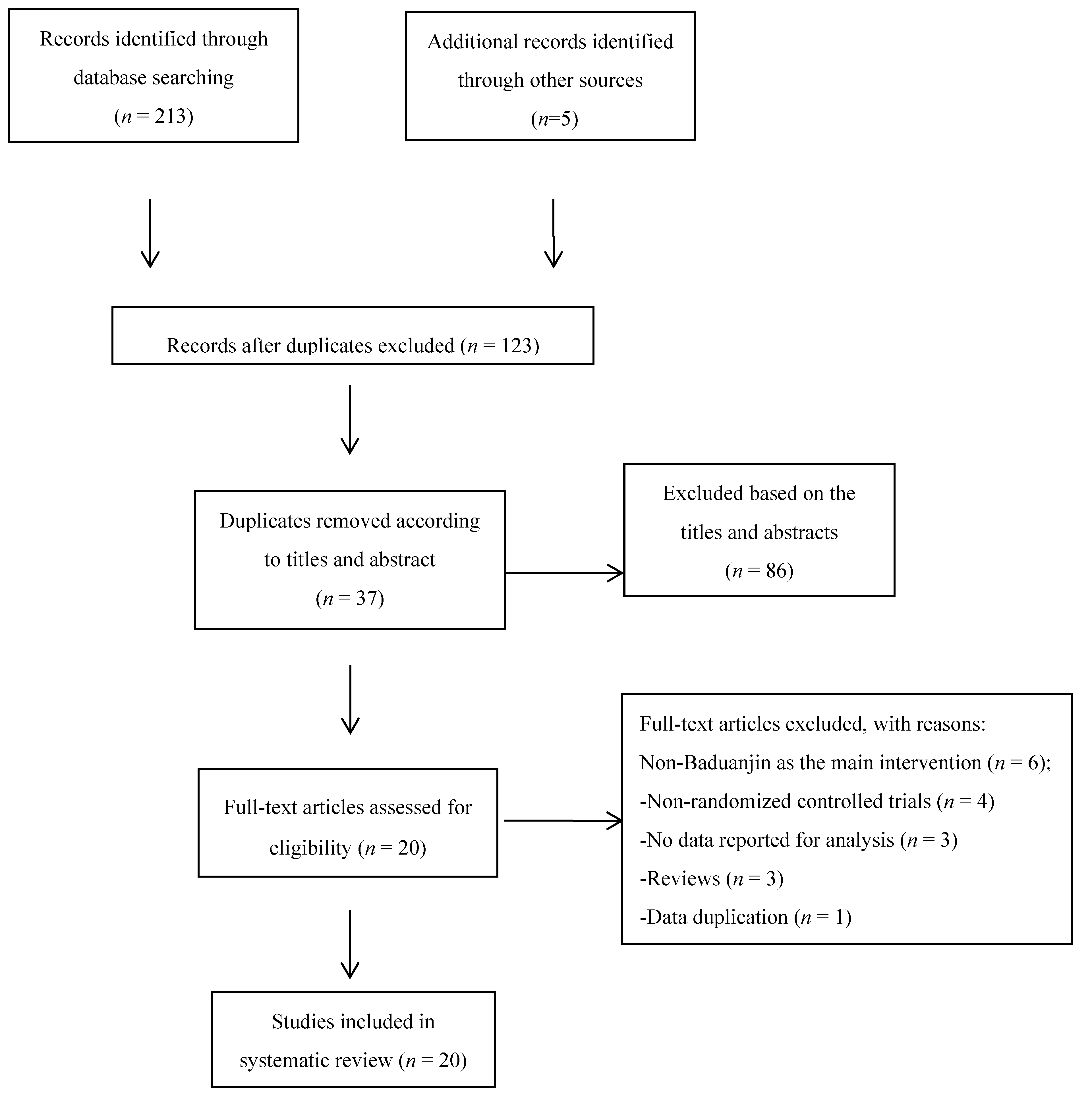
3.1. Study Selection
3.2. Study Characteristics
3.3. Methodological Quality
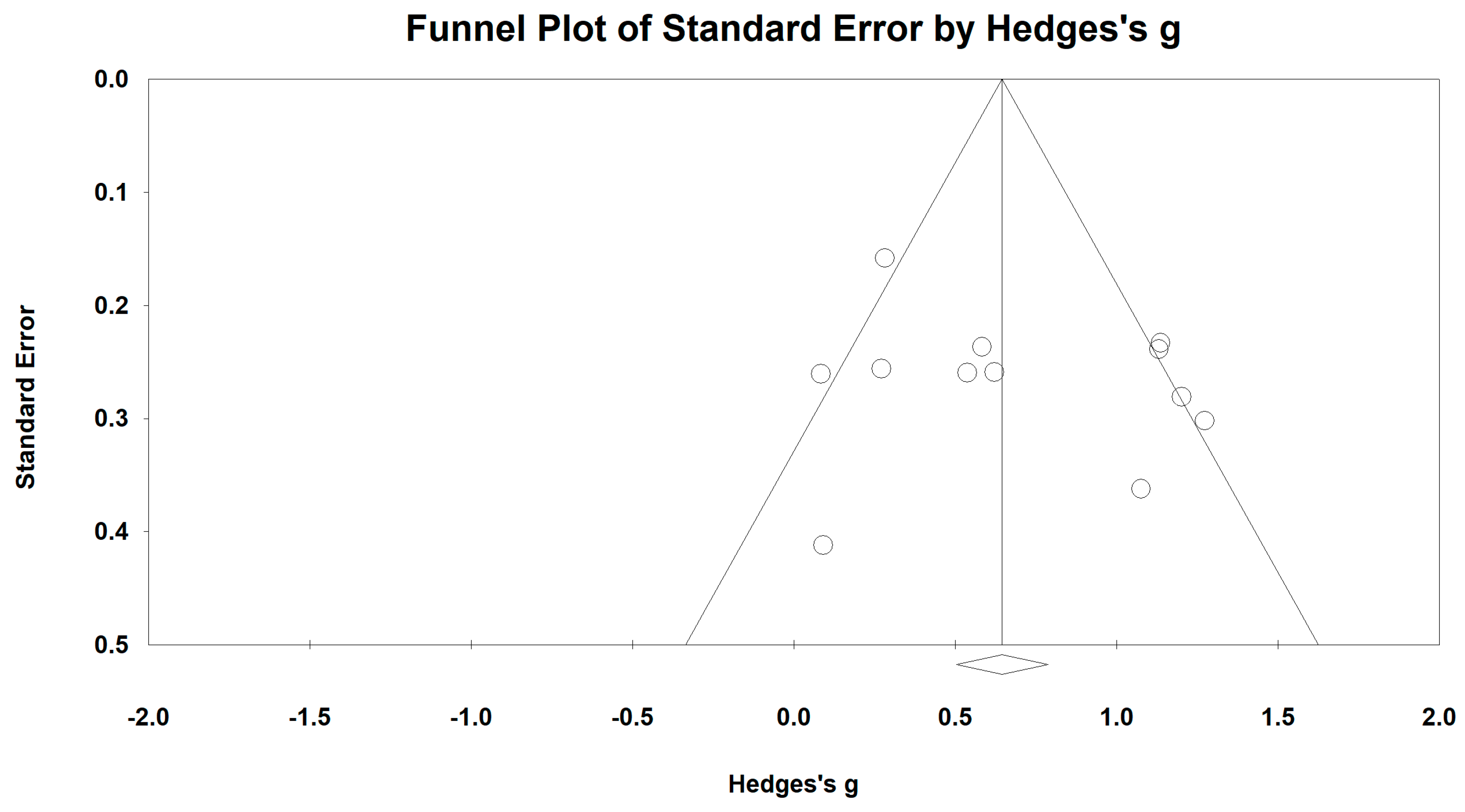
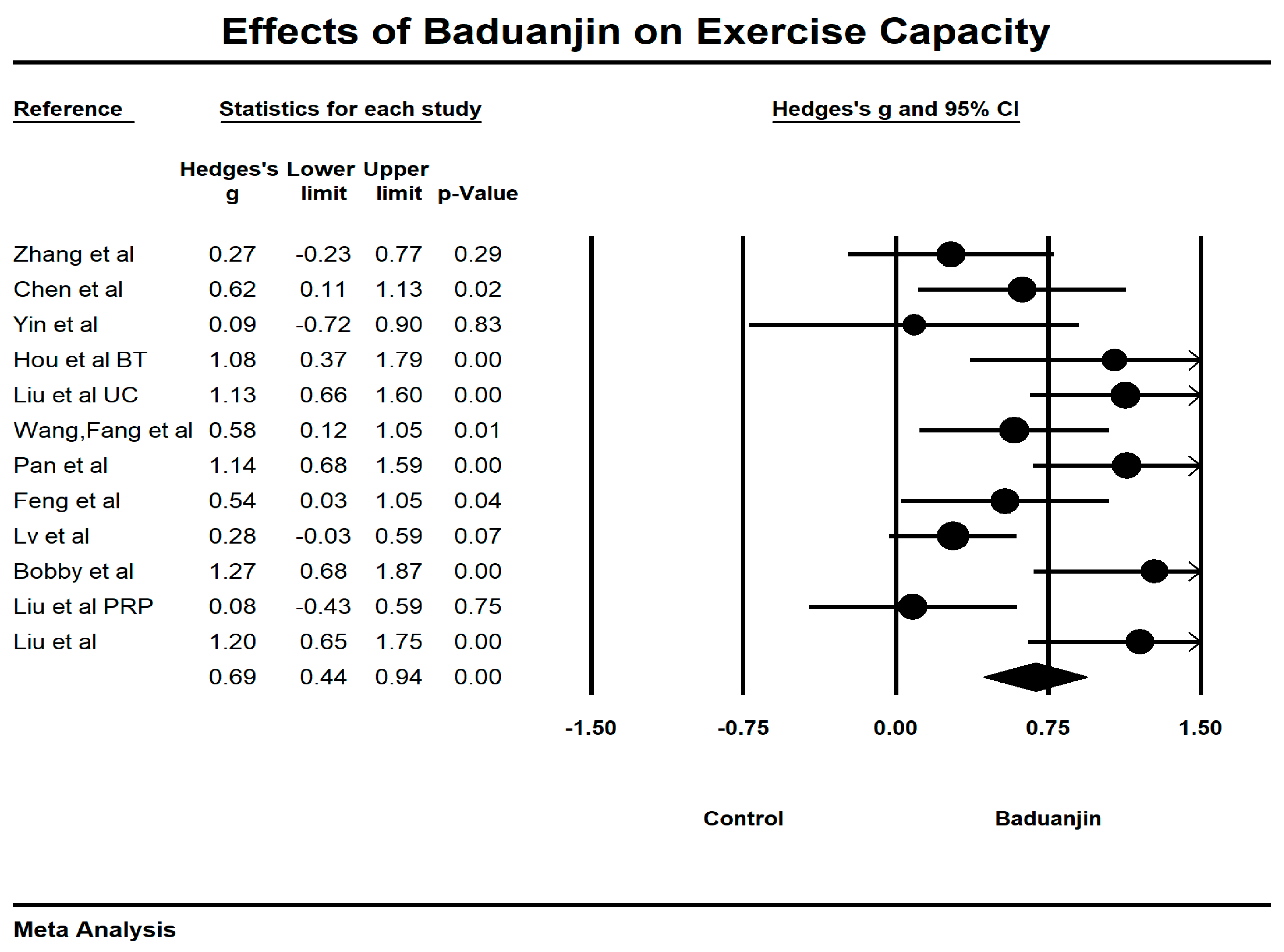
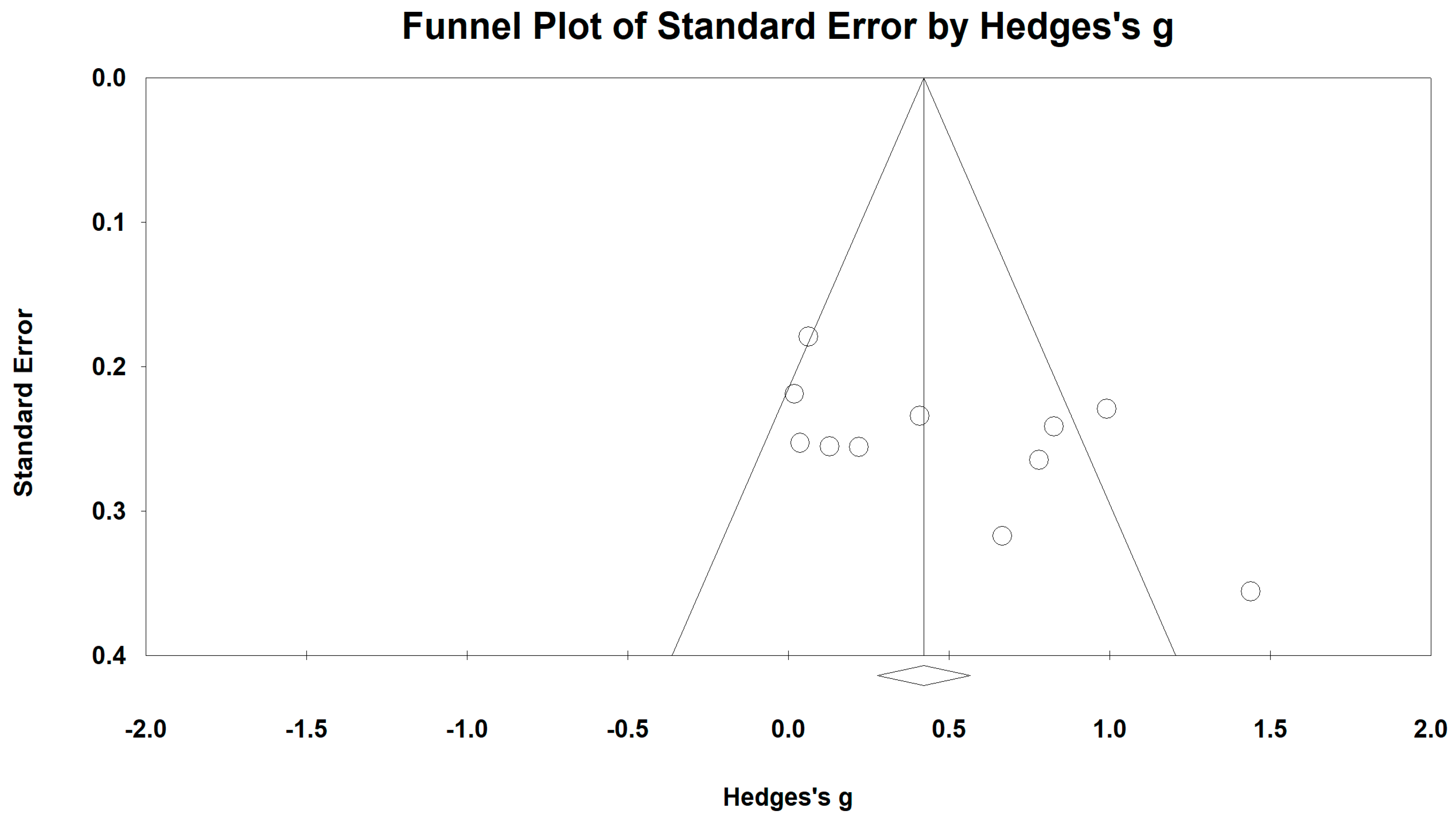
3.4. Effects of Baduanjin on 6-Minute Walking Test
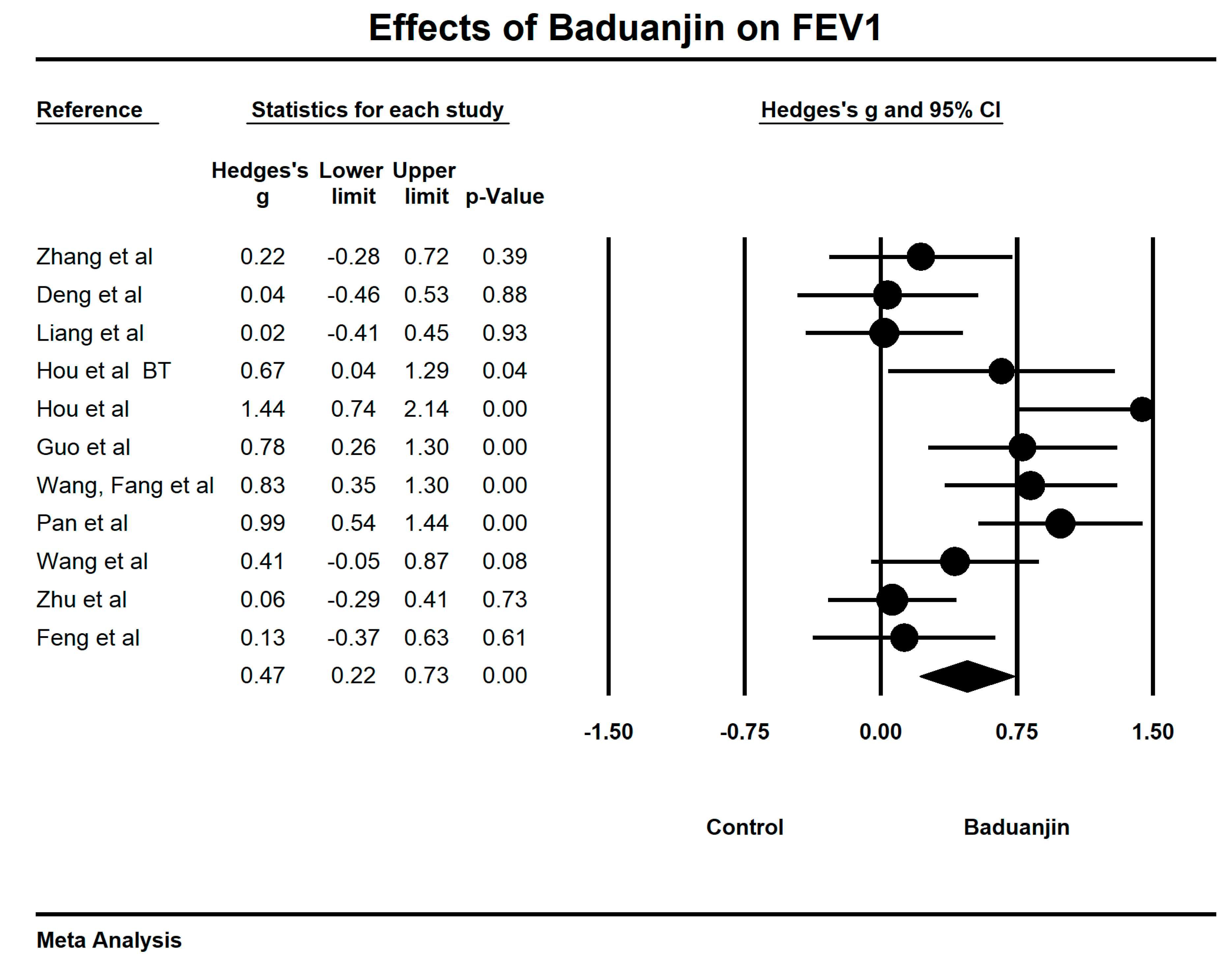
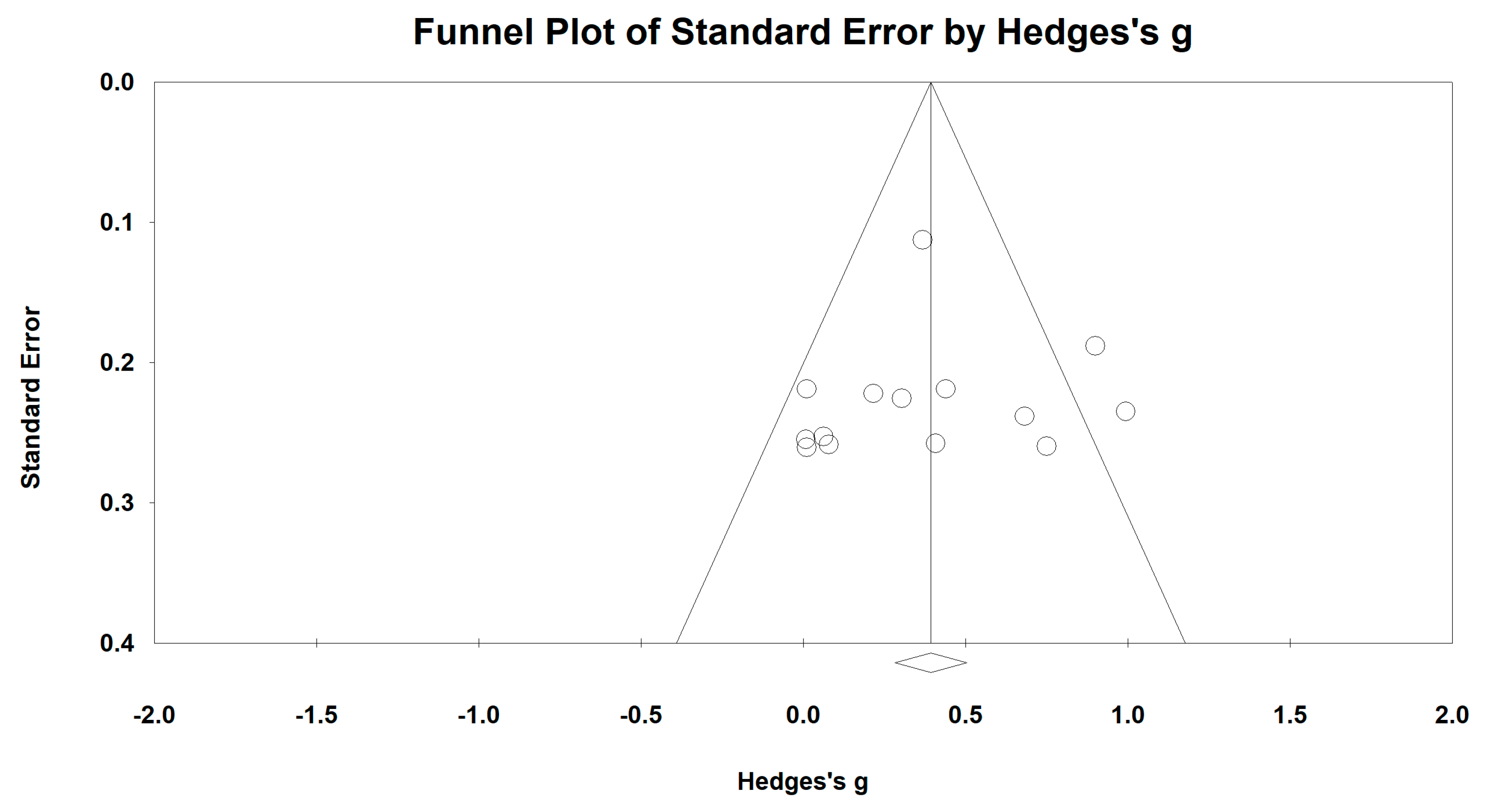
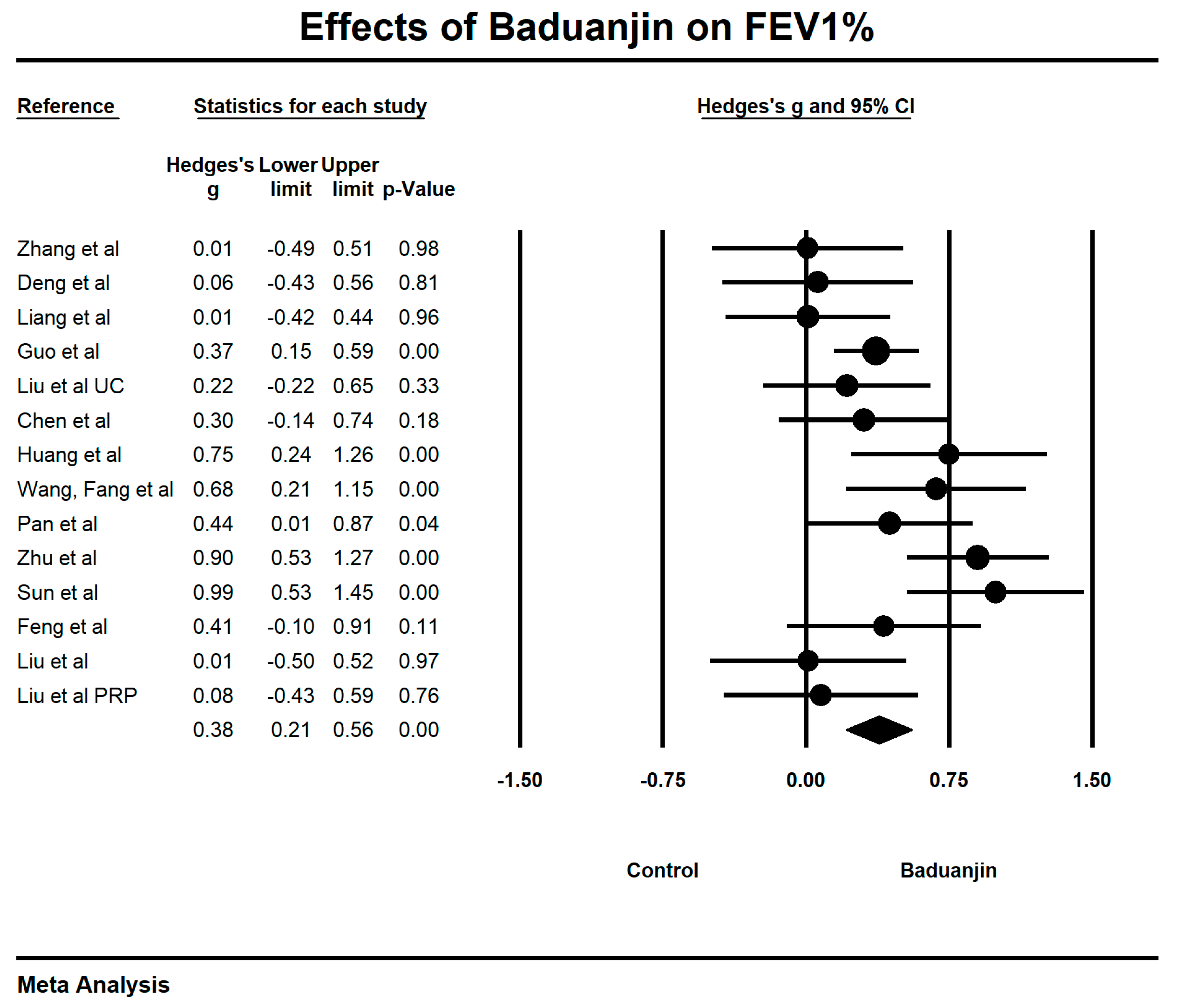
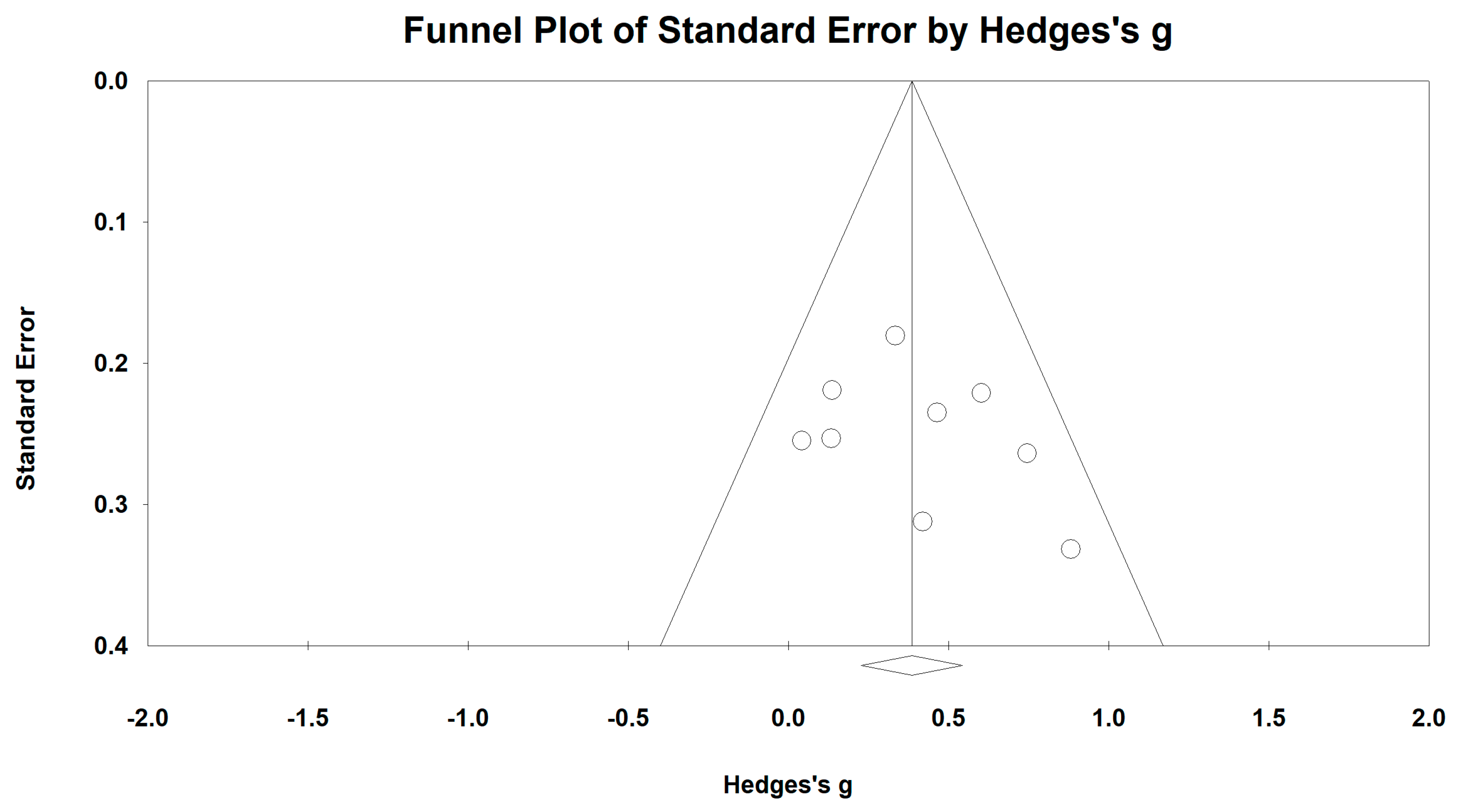
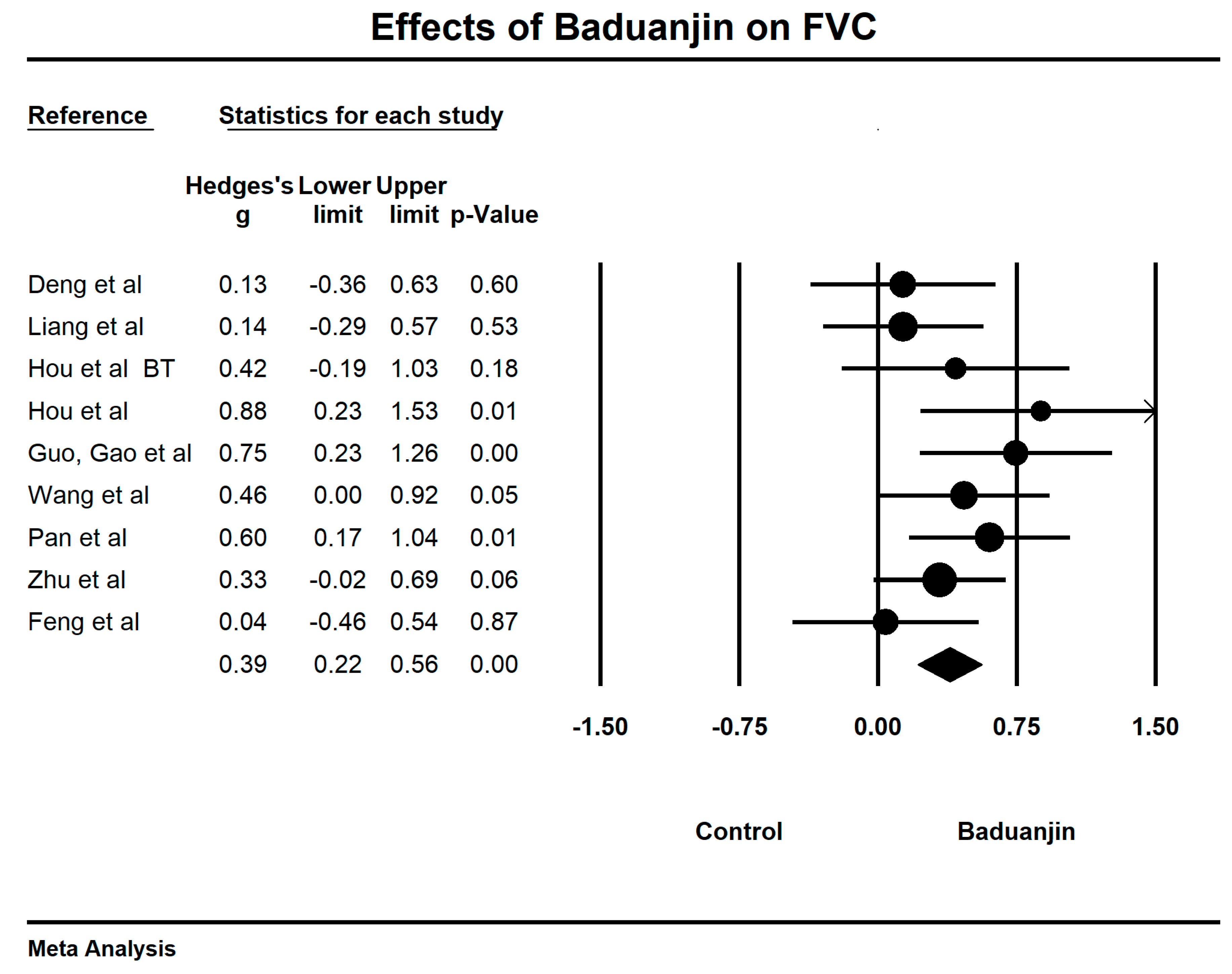
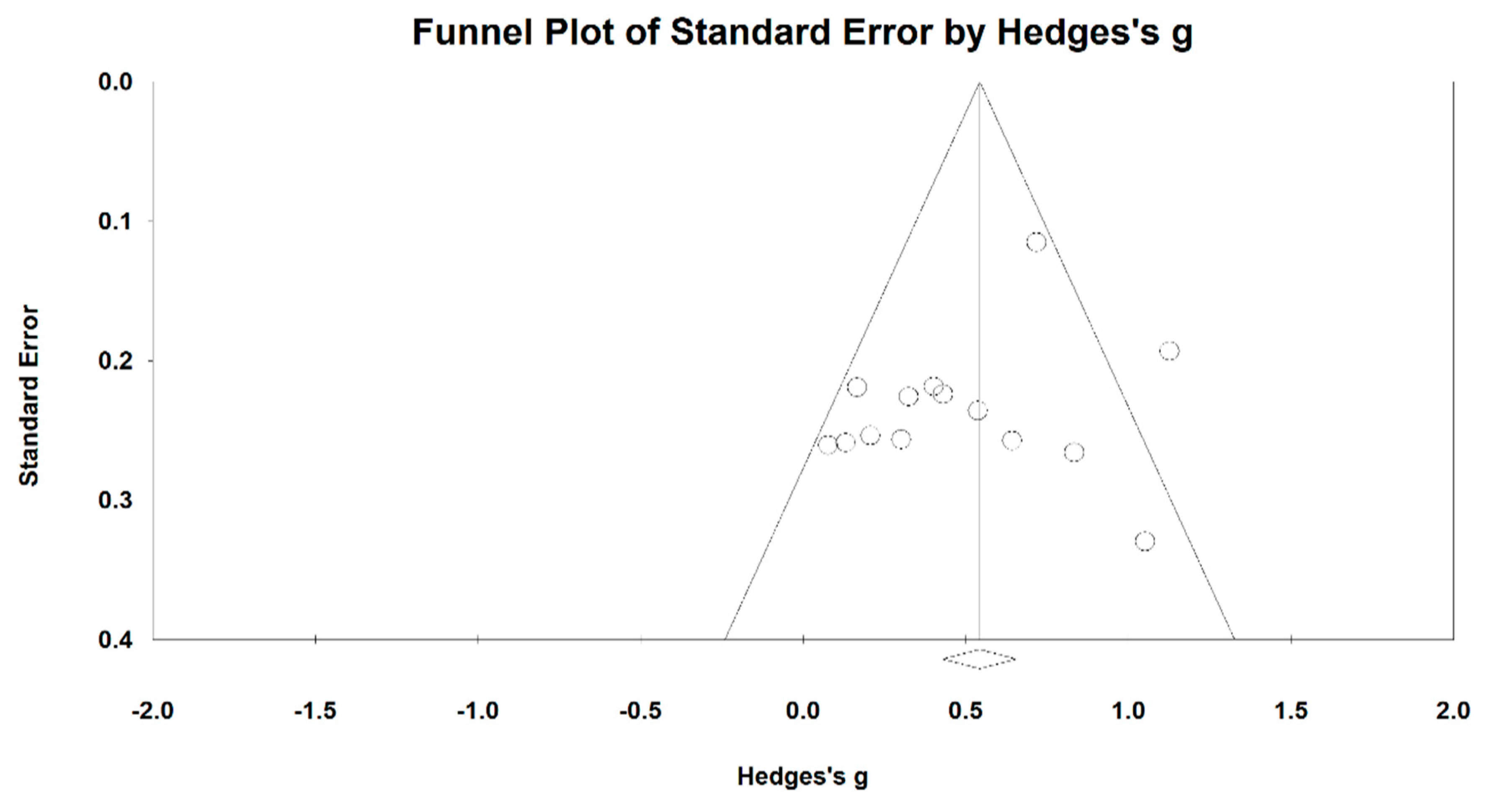
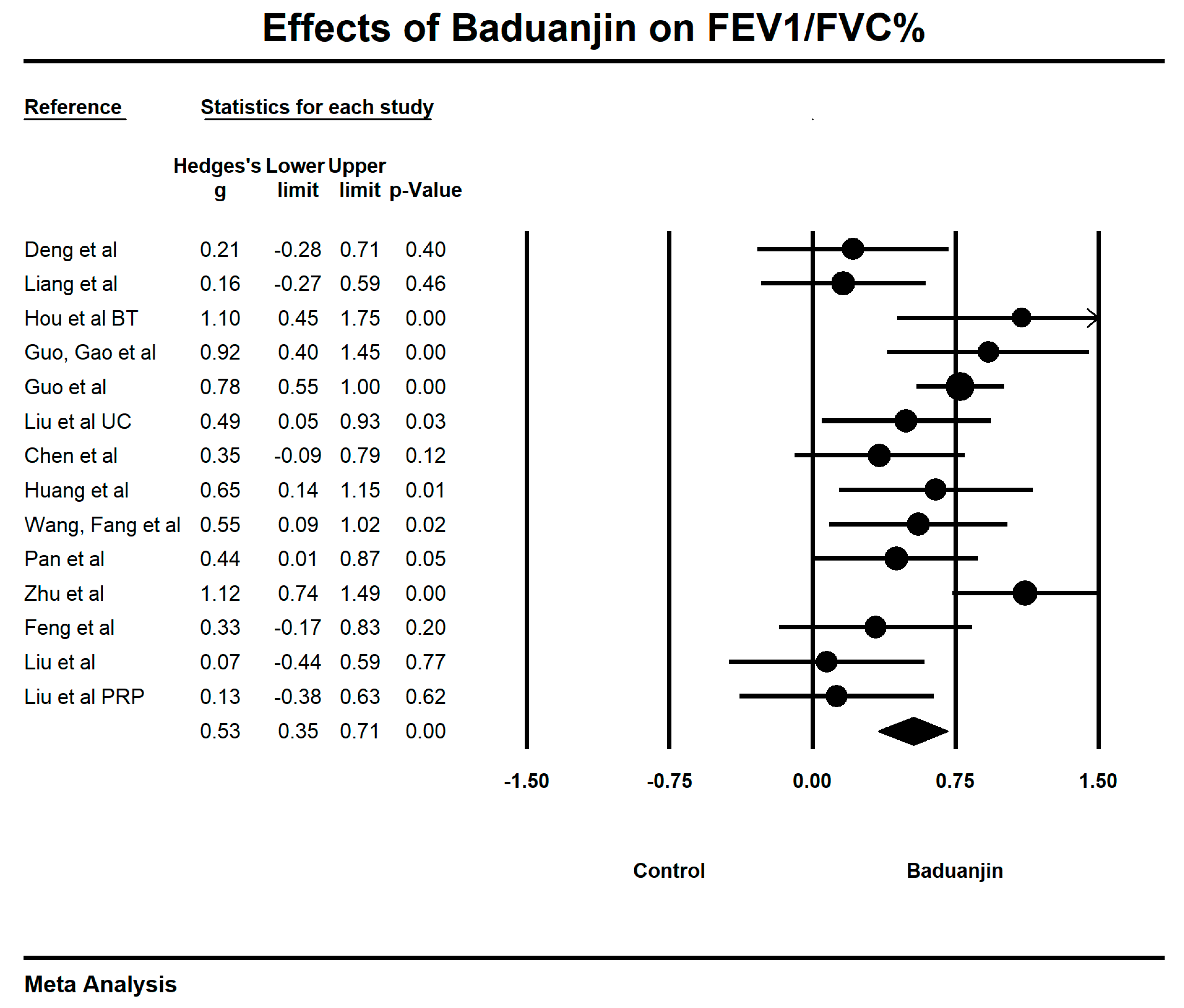
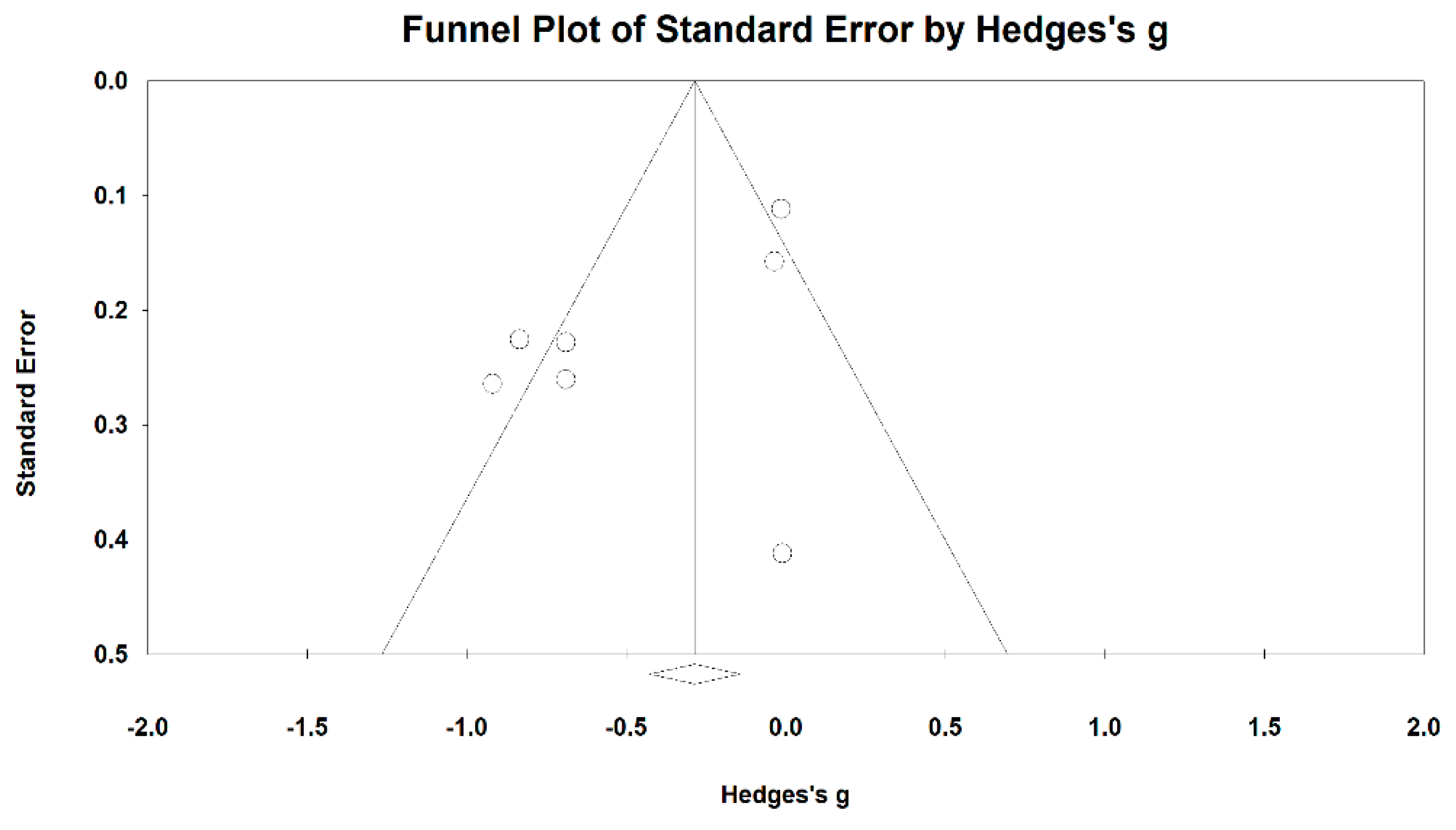
3.5. Effects of Baduanjin on Lung Functions
3.6. Effects of Baduanjin on Quality of Life
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Barberã, J.A.; Peces-Barba, G.; Agustã, A.G.; Izquierdo, J.L.; Monsó, E.; Montemayor, T.; Viejo, J.L.; Sociedad Española de Neumología y Cirugía Torácica (SEPAR). Clinical guidelines for the diagnosis and treatment of chronic obstructive pulmonary disease. Arch. Bronconeumol. 2001, 37, 297–316. [Google Scholar] [CrossRef] [PubMed]
- Miravitlles, M.; Anzueto, A. Chronic Respiratory Infection in Patients with Chronic Obstructive Pulmonary Disease: What Is the Role of Antibiotics? Int. J. Mol. Sci. 2017, 18, 1344. [Google Scholar] [CrossRef] [PubMed]
- Falk, J.A.; Kadiev, S.; Criner, G.J.; Scharf, S.M.; Minai, O.A.; Diaz, P. Cardiac Disease in Chronic Obstructive Pulmonary Disease. Proc. Am. Thorac. Soc. 2008, 5, 543–548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Durham, A.L.; Adcock, I.M. The relationship between COPD and lung cancer. Lung Cancer 2015, 90, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Barberà, J.A.; Peinado, V.I.; Santos, S. Pulmonary hypertension in chronic obstructive pulmonary disease. Eur. Respir. J. 2003, 21, 892–905. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hynninen, K.M.; Breitve, M.H.; Wiborg, A.B.; Pallesen, S.; Nordhus, I.H. Psychological characteristics of patients with chronic obstructive pulmonary disease: A review. J. Psychosom. Res. 2005, 59, 429–431. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Burden of Disease (GBD) 2002 estimates. In World Health Report 2004; WHO: Geneva, Switzerland, 2004; Available online: http://www.who.int/healthinfo/global_burden_disease/estimates_regional_2002/en/ (accessed on 18 June 2018).
- Lozano, R.; Naghavi, M.; Foreman, K.; Lim, S.; Shibuya, K.; Aboyans, V.; Abraham, J.; Adair, T. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2095–2128. [Google Scholar] [CrossRef]
- Lopez, A.D.; Shibuya, K.; Rao, C.; Mathers, C.D.; Hansell, A.L.; Held, L.S.; Schmid, V.; Buist, S. Chronic obstructive pulmonary disease: Current burden and future projections. Eur. Respir. J. 2006, 27, 397–412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathers, C.D. Uncertainty and data availability for the global burden of disease estimates 2000–2002. In Evidence and Information for Policy Working Paper; WHO: Geneva, Switzerland, 2005; Available online: http://www.who.int/healthinfo/global_Burden_disease/en/index.html (accessed on 18 June 2018).
- Fabbri, L.M.; Hurd, S.S. For the GOLD Scientific Committee. Global strategy for the diagnosis, management and prevention of COPD: 2003 update. Eur. Respir. J. 2003, 22, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Nici, L.; Donner, C.; Wouters, E. ATS/ERS Pulmonary Rehabilitation Writing Committee. American Thoracic Society/European Respiratory Society statement on pulmonary rehabilitation. Am. J. Respir. Crit. Care Med. 2006, 173, 1390–1413. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Harrison, S.; Houchen, L.; Wagg, K. Exercise assessment and training in pulmonary rehabilitation for patients with copd. Eur. J. Phys. Rehabil. Med. 2011, 47, 483–497. [Google Scholar] [PubMed]
- Zou, L.; Wang, H.; Xiao, Z.; Fang, Q.; Zhang, M.; Li, T.; Du, G.; Liu, Y. Taichi for health benefits in patients with multiple sclerosis: A systematic review. PLoS ONE 2017, 12, 17–21. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Wang, C.; Chen, K.; Shu, Y.; Chen, X.; Luo, L.; Zhao, X. The Effect of Taichi Practice on Attenuating Bone Mineral Density Loss: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2017, 14, 1000. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Wang, H.; Li, T. Effects of Traditional Chinese Mind-Body Exercise on Disease Activity, Spinal Mobility, and Quality of Life in Patients with Ankylosing Spondyliti. Trav. Hum. 2017, 80, 1585–1597. [Google Scholar]
- Zou, L.; Sasaki, J.; Zeng, N.; Wang, C.; Sun, L. A Systematic Review with Meta-Analysis of Mindful Exercises on Rehabilitative Outcomes among post-stroke patients. Arch. Phys. Med. Rehabil. 2018, 4, 25–31. [Google Scholar] [CrossRef]
- Zou, L.; Yeung, A.; Zeng, N.; Wang, C.; Sun, L.; Thomas, G.; Wang, H. Effects of Mind-Body Exercises for Mood and Functional Capabilities in Post-Stroke Patients: An Analytical Review of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2018, 15, 721. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; SasaKi, J.; Wang, H.; Xiao, Z.; Fang, Q.; Zhang, M. A Systematic Review and Meta-Analysis Baduanjin Qigong for Health Benefits: Randomized Controlled Trials. Evid.-Based Complement. Altern. Med. 2017, 4548706. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Wang, C.; Yeung, A.; Liu, Y.; Pan, Z. A Review Study on the beneficial effects of Baduanjin. J. Altern. Complement. Med. 2018, 24, 324–335. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Wang, C.; Chen, X.; Wang, H. Baduanjin Exercise for Stroke Rehabilitation: A Systematic Review with Meta-Analysis of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2018, 15, 600. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Albert, Y.; Quan, X.; Wang, H. A Systematic review and Meta-Analysis of Mindfulness-based (Baduanjin) exercise for alleviating musculoskeletal pain and improving sleep quality in people with chronic diseases. Int. J. Environ. Res. Public Health 2018, 15, 206. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.; Tan, C.; Yuan, S. Baduanjin exercise for insomnia: A systematic review and meta-analysis. Behav. Sleep Med. 2017, 4, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Yeung, A.; Quan, X.; Hui, S.S.-C.; Hu, X.; Chan, J.S.M.; Wang, C.; Boyden, S.D.; Sun, L.; Wang, H. Mindfulness-based Baduanjin exercise for depression and anxiety in people with physical or mental illnesses: A Systematic Review and Meta-analysis of randomized controlled trials. Int. J. Environ. Res. Public Health 2018, 15, 321. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Yeung, A.; Li, C.; Wei, G.-X.; Chen, K.W.; Kinser, P.A.; Chan, J.S.M.; Ren, Z. Effects of Meditative Movements on Major Depressive Disorder: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2018, 7, 195. [Google Scholar] [CrossRef] [PubMed]
- Xue, G.W.; Feng, Q.Y.; Yao, X.Q.; Qi, Y.; Wang, Y.N. Efficacy evaluation of Health Qigong Baduanjin in stable pulmonary rehabilitation of chronic obstructive pulmonary disease. J. Beijing Univ. Tradit. Chin. Med. 2015, 38, 139–144. [Google Scholar] [CrossRef]
- Chen, Y. Effect of Baduanjin Exercise Rehabilitation on Rehabilitation of Patients with Chronic Obstructive Pulmonary Disease. J. Liaoning Univ. Tradit. Chin. Med. 2017, 6, 213–215. [Google Scholar] [CrossRef]
- Liu, S.R.; Chen, Y.F. Clinical Study on the Effect of Health Qigong Baduanjin on Patients with Chronic Obstructive Pulmonary Disease in Stable Phase. J. Sichuan Med. 2014, 11, 1481–1482. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 18, 123. [Google Scholar] [CrossRef]
- Zou, L.; Han, J.; Li, X.C.; Yeung, A.; Hui, S.C.; Tsang, W.N.; Ren, Z.B.; Wang, L. The Effects of Tai Chi on Lower Limb Proprioception in Adults Aged Over 55: A Systematic Review and Meta-Analysis. Arch. Phys. Med. Rehabil. 2018, 8, 18. [Google Scholar] [CrossRef] [PubMed]
- Foley, N.C.; Teasell, R.W.; Bhogal, S.K.; Speechley, M.R. Stroke Rehabilitation Evidence-Based Review: Methodology. Top. Stroke Rehabil. 2003, 10, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Yeung, A.; Li, C.; Chiou, S.Y.; Zeng, N.; Tzeng, H.M.; Wang, L. Effects of Mind⁻Body Movements on Balance Function in Stroke Survivors: A Meta-Analysis of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2018, 15, 6. [Google Scholar] [CrossRef] [PubMed]
- Hou, D.; Huang, F.; Yu, S.; Tan, Y.; Luo, J. Study on the efficacy of Baduanjin combined with respiratory training in patients with chronic obstructive pulmonary disease in the community. Guangzhou Pharm. 2017, 29–32. [Google Scholar] [CrossRef]
- Liu, S.; Chen, Y. Clinical studies on Qigong Baduanjin 6min walking in patients with chronic obstructive pulmonary disease improved from stable. Sichuan Med. 2013, 34, 1090–1092. [Google Scholar] [CrossRef]
- Chen, Y.; Liu, S. Effect of Health Qigong Baduanjin on Pulmonary Function in Patients with Chronic Obstructive Pulmonary Disease in Stable Phase. Chin. Med. Mod. Distance Educ. 2015, 13, 16–18. [Google Scholar] [CrossRef]
- Pan, M.; Luo, J. Observation on the Curative Effect of Stationary Baduanjin Rehabilitation Exercise on Patients with Chronic Obstructive Pulmonary Disease in Stable Phase. J. Chengdu Univ. Tradit. Chin. Med. 2016, 39, 49–52. [Google Scholar] [CrossRef]
- Yin, G. Clinical Study on the Effect of Baduanjin and Respiratory Exercises on Quality of Life in Patients with Moderate to Severe COPD. Master’s Thesis, Guangzhou University, Guangzhou, China, 2013. Available online: http://kns.cnki.net/KCMS/detail/detail.aspx?dbcode=CMFD&d (accessed on 18 June 2018).
- Sun, Y. Therapeutic Effect of Health Qigong “Baduanjin” on Patients with Stable Stage II Chronic Obstructive Pulmonary Disease. Master’s Thesis, Changchun University, Changchun, China, 2014. Available online: http://kreader.cnki.net/Kreader/CatalogViewPage.aspx?dbCode=cdmd&filename (accessed on 18 June 2018).
- Zhang, L.; Wang, T.; Shi, L.; Zou, Q.; Zhu, T.G.; Sun, Y.L.; Zhang, L.L. Effects of Ba Duanjin’s “Zong Zongqi” on nutritional status and cardiopulmonary rehabilitation in patients with chronic obstructive pulmonary disease. Changchun Univ. Tradit. Chin. Med. 2017, 33, 954–956. [Google Scholar] [CrossRef]
- Guo, J.; Gao, Y.; Xie, X.H. Effects of Baduanjin exercise on rehabilitation of patients with chronic obstructive pulmonary disease in stable phase. Qi Lu Nurs. J. 2016, 22, 97–98. [Google Scholar] [CrossRef]
- Guo, J. Analysis of the efficacy of traditional fitness exercise Baduanjin in promoting pulmonary rehabilitation in patients with stable COPD. J. Shandong Med. Coll. 2016, 38, 171–174. [Google Scholar] [CrossRef]
- Huang, B.; Yao, Q. Therapeutic effect of Health Qigong Baduanjin on the treatment of chronic obstructive pulmonary disease with stable lung and spleen deficiency. Hubei J. Tradit. Chin. Med. 2017, 39, 4–6. [Google Scholar]
- Wang, L.; Fang, L. Effects of practiced Baduanjin on stable lung function in patients with chronic obstructive pulmonary disease. TCM Her. 2018, 3. [Google Scholar] [CrossRef]
- Wang, J.Y. Clinical observation of herbal administration and eight-section brocade in treating chronic obstructive pulmonary disease of stable stage. Shanghai J. Tradit. Chin. Med. 2015, 7, 41–42. [Google Scholar] [CrossRef]
- Zhu, Z.G.; Chen, Y. Impacts of Baduanjin Qigong of Sitting Style on Lung Function in COPD Patients. World J. Integr. Tradit. West. Med. 2014, 8, 846–848. [Google Scholar] [CrossRef]
- Deng, Y.; Chen, J. Effect of Baduanjin single-lift on rehabilitation of patients with chronic obstructive pulmonary disease. Chin. J. Nurs. 2015, 50, 1458–1463. [Google Scholar]
- Liang, X. Effect of Baduanjin Single-lifting Exercise on Rehabilitation of Patients with Chronic Obstructive Pulmonary Disease. J. Nurs. Pract. Res. 2016, 13, 156–157. [Google Scholar] [CrossRef]
- Chen, J.; Deng, Y.; Chen, Q.; Zhang, W.X.; Deng, L.J. Effects of Baduanjin on the quality of life and exercise tolerance of patients with chronic obstructive pulmonary disease with pulmonary spleen qi deficiency syndrome. J. Rehabil. 2015, 25, 13–17. [Google Scholar] [CrossRef]
- Ng, B.H.; Tsang, H.W.; Jones, A.Y.; So, C.T.; Mok, T.Y.W. Functional and psychosocial effects of health qigong in patients with COPD: A randomized controlled trial. J. Altern. Complement. Med. 2011, 17, 243–251. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.D.; Jin, H.Z.; Ng, H.P.; Gu, Y.-H.; Wu, Y.-C.; Lu, G. Therapeutic Effects of Qigong in Patients with COPD: A Randomized Controlled Trial. Hong Kong J. Occup. Ther. 2012, 22, 38–46. [Google Scholar] [CrossRef]
- Feng, Y.; Pan, H. Observation of the efficacy of Baduanjin exercise on elderly patients with chronic obstructive pulmonary disease at stable stage. New J. Tradit. Chin. Med. 2009, 8, 36–37. [Google Scholar] [CrossRef]
- Yan, L.U.; Jiazhen, L.I.; Zhang, L.; Guo, J.; Liu, S. Effect of gymnastic qigong Baduanjin on the quality of life and satisfac-tion of patients with chronic obstructive pulmonary diseases. China Med. Her. 2015, 30, 161–164. [Google Scholar]
- Peng, W.P. Evaluation of the effects of aerobic exercise therapy on lung rehabilitation in patients with chronic obstructive pulmonary disease. J. Mudanjiang Med. 2014, 6, 39–41. [Google Scholar] [CrossRef]
- Ding, M.; Zhang, W.; Li, K.; Chen, X. Effectiveness of T’ai Chi and Qigong on Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis. J. Altern. Complement. Med. 2014, 20, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.L.; Lin, Z.K.; Weng, H.D.; Qi, Q.F.; Lu, J.; Liu, K.X. Effectiveness of meditative movement on COPD: A systematic review and meta-analysis. Int. J. Chron. Obstr. Pulm. Dis. 2018, 13, 1239–1250. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.C.; Pan, L.; Hu, Q.; Dong, W.P.; Yan, J.H.; Dong, L. Effects of yoga training in patients with chronic obstructive pulmonary disease: A systematic review and meta-analysis. J. Thorac. Dis. 2016, 6, 795–802. [Google Scholar] [CrossRef]
- Puhan, M.A.; Guyatt, G.H.; Goldstein, R.; Mador, J.; McKim, D.; Stahl, E.; Griffith, L.; Schünemann, H.J. Relative responsiveness of the Chronic Respiratory Questionnaire, St. Georges Respiratory Questionnaire and four other health-related quality of life instruments for patients with chronic lung disease. Respir. Med. 2007, 101, 308. [Google Scholar] [CrossRef] [PubMed]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Location (Language) | Participant Characteristics | Intervention Program | Baduanjin Training | Outcome Measured | Adverse Event; Follow-Up | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Sample Size (Attrition Rate) | Mean Age or Age Range | Course of Disease | Frequency (weekly) | Time (min) | Duration (week) | |||||
| Zhang et al. [39] | Changchun, China (Chinese) | 60 (0%) | BJ: 68.50 (9.18) CG: 68.03 (7.18) | NR | BJ: Baduanjin + Drug Therapy CG: Drug Therapy | 7 | / | 8 | Lung function (FEV1, FEV1%, FVC), Exercise Capacity (6-MWT) | No; No |
| Deng et al. [46] | Fujian, China (Chinese) | 60 (1.6%) | BJ: 66.26 (5.13) CG: 66.90 (4.63) | BJ: 4.68 (2.54) CG: 4.77 (2.52) | BJ: Baduanjin + Usual Care CG: Usual Care | 7 | 30 | 12 | Lung function (FEV1, FEV1%, FVC, FEV1/FVC) | No; No |
| Liang et al. [47] | Guangdong, China (Chinese) | 82 (0%) | BJ: 60.23 (9.32) CG: 60.23 (9.32) | BJ: 4.25 (2.05) CG: 4.25 (2.05) | BJ: Baduanjin + Usual Care CG: Usual Care | 7 | 30 | 12 | Lung function (FEV1, FEV1%, FVC, FEV1/FVC) | No; No |
| Chen et al. [48] | Fujian, China (Chinese) | 60 (3.4%) | BJ: 66.26 (5.13) CG: 66.90 (4.63) | BJ: 4.68 (2.54) CG: 4.77 (2.52) | BJ: Baduanjin + Usual Care CG: Usual Care | 7 | 30 | 12 | Exercise Capacity (6-MWT), Quality of life (CAT) | No; No |
| Yin et al. [37] | Guangzhou, China (Chinese) | 24 (0%) | BJ: 70.40 (7.56) CG: 69.17 (7.66) | NR | BJ: Baduanjin + Drug Therapy CG: Breathing training + Drug Therapy | 7 | 30 | 24 | Quality of life (SGRQ), Exercise Capacity (6-MWT) | No; No |
| Hou et al. [33] | Dongwan, China (Chinese) | 60 (0%) | BJ: 63.34 (5.95) CG1: 62.87 (6.01) CG2: 63.77 (6.14) | NR | BJ: Baduanjin + Breathing Training CG1: Breathing Training CG2: Unaltered Lifestyle | 2 | 30 | 12 | Lung function (FEV1, FVC, FEV1/FVC), Exercise Capacity (6-MWT), Quality of life (SGRQ) | No; No |
| Guo, Gao et al. [40] | Qingdao, China (Chinese) | 60 (0%) | BJ: 63.4 (NR) CG: 62.8 (NR) | BJ: 4.67 (1.54) CG: 4.75 (1.52) | BJ: Baduanjin + Drug Therapy CG: Drug Therapy | >4 | 30 | 24 | Lung function (FEV1, FEV1%, FVC, FEV1/FVC) | No; No |
| Guo et al. [41] | Qingdao, China (Chinese) | 320 (0%) | BJ: 64.87 (8.86) CG: 64.15 (8.97) | BJ: 16.19 (5.48) CG: 16.21 (5.53) | BJ: Baduanjin + Drug Therapy CG: Drug Therapy | >4 | 30 | 24 | Lung function (FEV1%, FEV1/FVC), Quality of life (CAT) | No; No |
| Liu et al. [34] | Chengdu, China (Chinese) | 80 (0%) | BJ: 59.77 (7.08) CG: 60.67 (6.95) | NR | BJ: Baduanjin + Usual Care CG: Usual Care | 7 | 30 | 12 | Lung function (FEV1%, FEV1/FVC), Exercise Capacity (6-MWT) | No; No |
| Chen, Liu et al. [35] | Chengdu, China (Chinese) | 78 (0%) | BJ: 60.52 (7.24) CG: 59.67 (6.91) | NR | BJ: Baduanjin + Usual Care CG: Usual Care | 7 | 30 | 12 | Lung function (FEV1%, FEV1/FVC) | No; No |
| Huang et al. [42] | Nanjing, China (Chinese) | 62 (0%) | BJ: 68.24 (3.28) CG: 69.77 (4.42) | BJ: 24.60 (10.6) CG: 17.32 (14.44) | BJ: Baduanjin + Drug Therapy CG: Drug Therapy | 7 | 30 | 24 | Lung function (FEV1, FEV1%, FEV1/FVC) Quality of life (CAT) | No; No |
| Wang, Fang et al. [43] | Dalian, China (Chinese) | 73 (3.9%) | BJ: 63.17 (9.95) CG: 63.67 (9.75) | BJ: 15.17 (6.73) CG: 14.83 (7.89) | BJ: Baduanjin + Drug Therapy CG: Drug Therapy | 7 | 30 | 12 | Lung function (FEV1, FEV1%, FVC, FEV1/FVC), Exercise Capacity (6-MWT), Quality of life (SGRQ) | No; No |
| Pan et al. [36] | SiChuan, China (Chinese) | 82 (0%) | BJ: 60.7 (5.6) CG: 61.8 (7.2) | BJ: 6.7 (6.2) CG: 8.8 (5.3) | BJ: Baduanjin + Usual Care CG: Usual Care | 7 | 30 | 24 | Lung function (FEV1, FEV1%, FVC, FEV1/FVC), Exercise Capacity (6-MWT), Quality of life (SGRQ) | No; No |
| Wang [44] | Beijing, China (Chinese) | 73 (0%) | BJ: 66.76 (5.80) CG: 66.69 (4.60) | BJ: 11.02 (3.38) CG: 10.85 (3.53) | BJ: Baduanjin + Drug Therapy CG: Drug Therapy | 7 | 30 | 48 | Lung function (FEV1%, FEV1), Exercise Capacity (6-MWT) | No; No |
| Zhu et a. [45] | ChangSha, China (Chinese) | 125 (0%) | BJ: 69.00 (8.70) CG: 68.00 (9.20) | BJ: 12.50 (10.70) CG: 10.80 (8.90) | BJ: Baduanjin + Drug Therapy CG: Drug Therapy | 14 | 30 | 24 | Lung function (FEV1, FEV1%, FVC, FEV1/FVC), Exercise Capacity (6-MWT) | No; No |
| Sun et al. [38] | ChangChun, China (Chinese) | 60 (5.4%) | BJ: 62.97 (6.87) CG: 63.21 (7.02) | BJ: 11.02 (3.38) CG: 10.85 (3.53) | BJ: Baduanjin + Drug Therapy CG: Drug Therapy | 7 | 30 | 48 | Lung function (FEV1%) , Exercise Capacity (6-MWT) and Quality of life (CAT) | No; No |
| Feng et al. [51] | GuangZhou, China (Chinese) | 60 (0%) | BJ: 63 (4.00) CG: 62 (5.00) | BJ: 5.2 (2.2) CG: 5.4 (1.9) | BJ: Baduanjin + Conventional Therapy CG: Conventional Therapy | 10 | 45 | 24 | Lung function (FEV1, FEV1%, FVC, FEV1/FVC), Exercise Capacity (6-MWT) | No; No |
| Lv et al. [52] | Beijing, China (Chinese) | 160 (0%) | BJ: 64.88 (8.87) CG: 63.14 (9.12) | BJ: 16.21 (5.49) CG: 16.57 (5.17) | BJ: Baduanjin + Conventional Therapy CG: Conventional Therapy | 7 | 20 | 2 | Exercise Capacity (6-MWT), Quality of life (CAT) | No; No |
| Bobby et al. [49] | Hong kong, China (English) | 51 (36.25%) | BJ: 71.75 (1.05) CG: 73.12 (1.33) | NR | BJ: Baduanjin CG: walking training | >4 | 30 | 24 | Exercise Capacity (6-MWT) | No; No |
| Liu et al. [50] | ShangHai, China (English) | 132 (10.60%) | BJ: 61.82 (7.69) CG1: 62.2 (6.34) CG2: 61.34 (8.34) | BJ: 7.54 (2.73) CG1: 7.75 (2.20) CG2: 6.34 (2.34) | BJ: Baduanjin CG1: Health Education CG2: Conventional Pulmonary Rehabilitation (walking + ball training) | 3 | 60 | 24 | Lung function (FEV1%, FEV1/FVC), Exercise Capacity (6-MWT) | No; No |
| Author [Reference] | Item 1 | Item 2 | Item 3 | Item 4 | Item 5 | Item 6 | Item 7 | Item 8 | Item 9 | Score |
|---|---|---|---|---|---|---|---|---|---|---|
| Zhang et al. [39] | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 7 |
| Deng et al. [46] | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 7 |
| Liang et al. [47] | 1 | 0 | 1 | 0 | 1 | 0 | 1 | 1 | 0 | 5 |
| Chen et al. [48] | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 6 |
| Yin et al. [37] | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 0 | 6 |
| Hou et al. [33] | 1 | 0 | 1 | 0 | 1 | 0 | 1 | 1 | 0 | 5 |
| Guo, Gao et al. [40] | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 6 |
| Guo et al. [41] | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 6 |
| Liu et al. [34] | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 6 |
| Chen, Liu et al. [35] | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 7 |
| Huang et al. [42] | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 6 |
| Wang, Fang et al. [43] | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 6 |
| Pan et al. [36] | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 6 |
| Wang [44] | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 6 |
| Zhu et al. [45] | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 7 |
| Sun et al. [38] | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 7 |
| Feng et al. [51] | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 7 |
| Lv et al. [52] | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 6 |
| Bobby et al. [49] | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 7 |
| Liu et al. [50] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 9 |
| Outcomes | Studies | Sample Size | Hedge’s g | 95% CI | Heterogeneity | ||
|---|---|---|---|---|---|---|---|
| Baduanjin Group | Control Group | I2 (%) | p Value | ||||
| FEV1 value | 10 | 398 | 411 | 0.47 | 0.22–0.73 | 68.01% | p < 0.001 |
| FEV1% value | 13 | 711 | 706 | 0.38 | 0.21–0.56 | 54.74% | p < 0.001 |
| FVC | 8 | 330 | 344 | 0.39 | 0.22–0.56 | 14.57% | p < 0.001 |
| FEV1/FVC value | 13 | 629 | 655 | 0.5 | 0.33–0.68 | 53.49% | p < 0.001 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, S.-J.; Ren, Z.; Wang, L.; Wei, G.-X.; Zou, L. Mind–Body (Baduanjin) Exercise Prescription for Chronic Obstructive Pulmonary Disease: A Systematic Review with Meta-Analysis. Int. J. Environ. Res. Public Health 2018, 15, 1830. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15091830
Liu S-J, Ren Z, Wang L, Wei G-X, Zou L. Mind–Body (Baduanjin) Exercise Prescription for Chronic Obstructive Pulmonary Disease: A Systematic Review with Meta-Analysis. International Journal of Environmental Research and Public Health. 2018; 15(9):1830. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15091830
Chicago/Turabian StyleLiu, Shi-Jie, Zhanbing Ren, Lin Wang, Gao-Xia Wei, and Liye Zou. 2018. "Mind–Body (Baduanjin) Exercise Prescription for Chronic Obstructive Pulmonary Disease: A Systematic Review with Meta-Analysis" International Journal of Environmental Research and Public Health 15, no. 9: 1830. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15091830