The Role of Emotional Intelligence in Engagement in Nurses

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Instruments
2.3. Procedure
2.4. Data Analysis
3. Results
3.1. Emotional Intelligence, Engagement, and Sociodemographic Variables
3.2. Components of Emotional Intelligence as Predictors of Engagement in Nurses
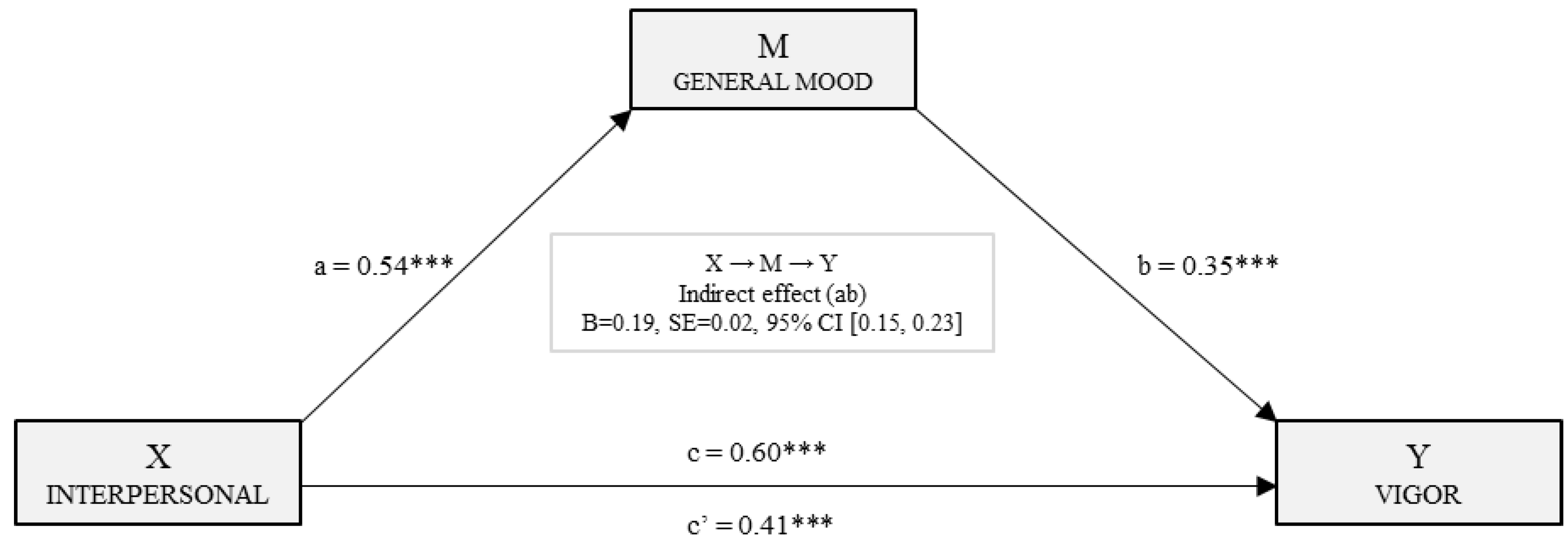
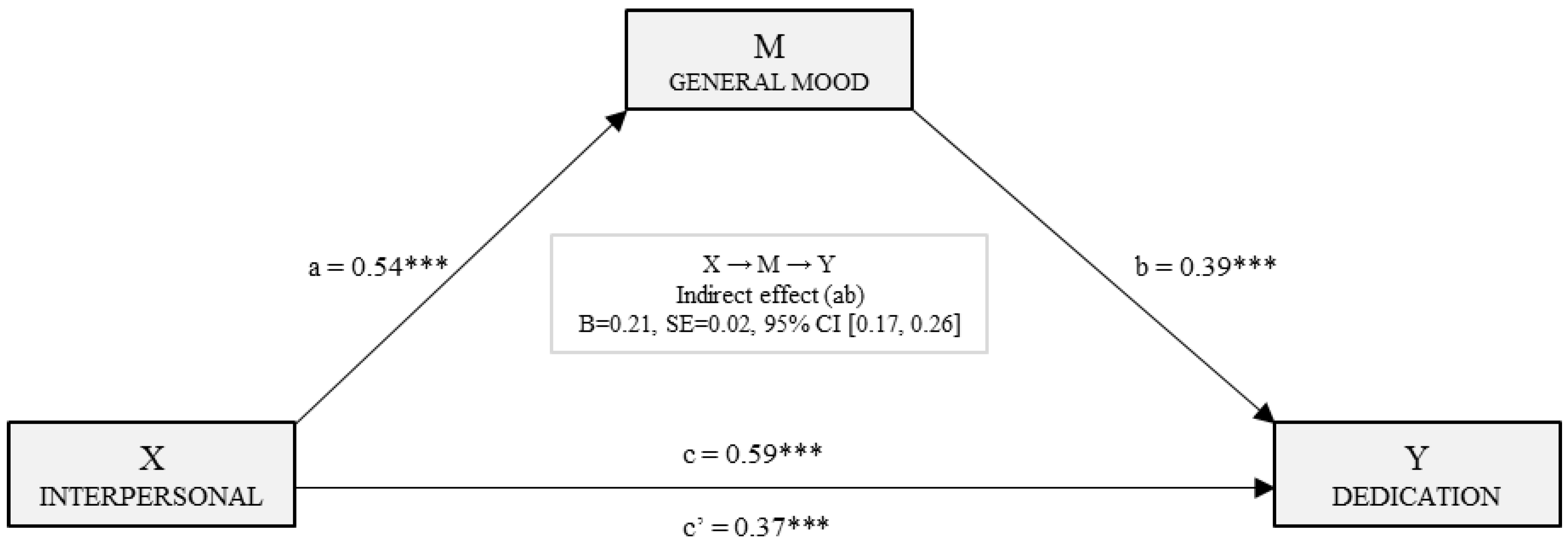
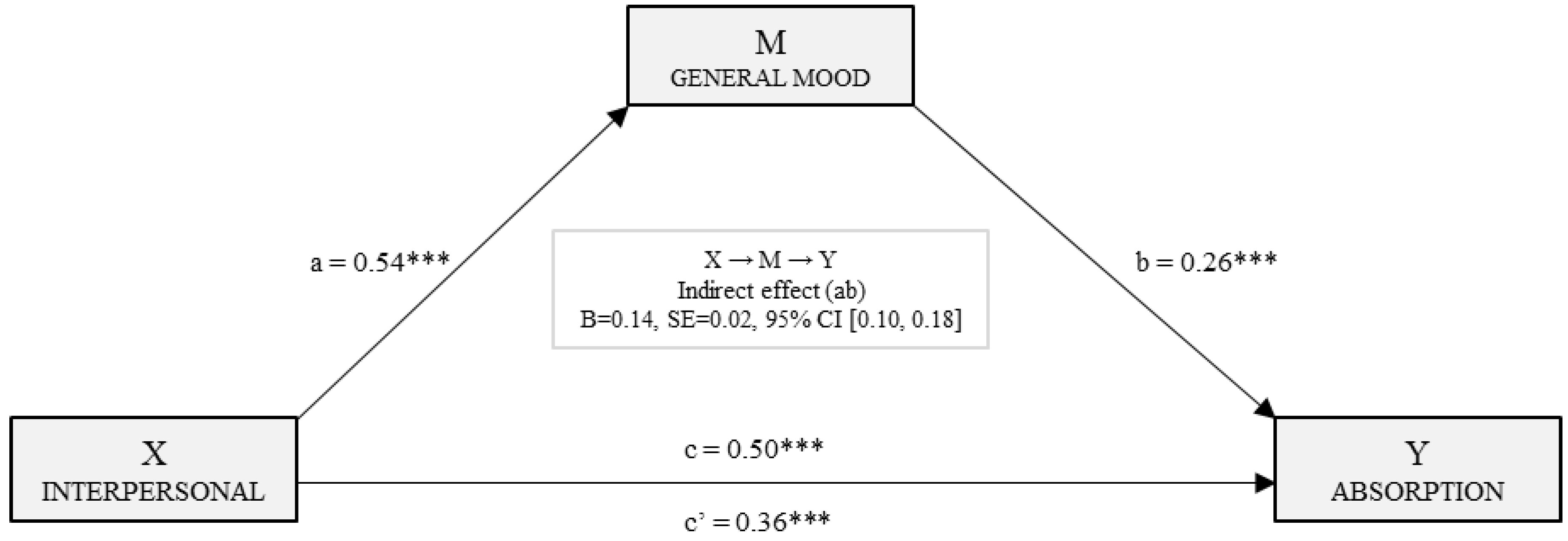
3.3. Mediation Models for Estimating the Effects on Engagement Dimensions
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Constitution of the World Health Organization. Available online: http://www.who (accessed on 22 April 2018).
- Adams, K.L.; Iseler, J.L. The relationship of bedside nurses’ emotional intelligence with quality of care. J. Nurs. Care Qual. 2014, 29, 174–181. [Google Scholar] [CrossRef] [PubMed]
- Freeney, Y.; Fellenz, M.R. Work engagement as a key driver of quality of care: A study with midwives. J. Health Organ. Manag. 2013, 27, 330–349. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Liu, Y. Impact of professional nursing practice environment and psychological empowerment on nurses’ work engagement: Test of structural equation modelling. J. Nurs. Manag. 2015, 23, 287–296. [Google Scholar] [CrossRef] [PubMed]
- García-Sierra, R.; Fernández-Castro, J.; Martínez-Zaragoza, F. Work engagement in nursing: An integrative review of the literatura. J. Nurs. Manag. 2016, 24, 101–111. [Google Scholar] [CrossRef] [PubMed]
- Seligman, M.E. Flourish: A Visionary New Understanding of Happiness and Well-Being; Simon and Schuster: New York, NY, USA, 2012. [Google Scholar]
- Seligman, M.; Csikszentmihalyi, M. Positive Psychology: An introduction. Am. Psychol. 2000, 55, 5–14. [Google Scholar] [CrossRef] [PubMed]
- Deci, E.L.; Ryan, R.M. Intrinsic Motivation and Self-Determination in Human Behavior; Plenum: New York, NY, USA, 1985. [Google Scholar]
- Ryan, R.M.; Deci, E.L. Self-Determination Theory and the Facilitation of Intrinsic Motivation, Social Development, and Well-Being. Am. Psychol. 2000, 55, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Salanova, M.; Lorente, M.L.; Chambel, M.J.; Martínez, I.M. Linking transformational leadership to nurses’ extra role performance: The mediating role of self-efficacy and work engagement. J. Adv. Nurs. 2011, 67, 2256–2266. [Google Scholar] [CrossRef] [PubMed]
- Walker, A.; Campbell, K. Work readiness of graduate nurses and the impact on job satisfaction, work engagement and intention to remain. Nurse Educ. Today 2013, 33, 1490–1495. [Google Scholar] [CrossRef] [PubMed]
- Fiabane, E.; Giorgi, I.; Sguazzin, C.; Argentero, P. Work engagement and occupational stress in nurses and other healthcare workers: The role of organizational and personal factors. J. Clin. Nurs. 2013, 22, 2614–2624. [Google Scholar] [CrossRef] [PubMed]
- Kunie, K.; Kawakami, N.; Shimazu, A.; Yonekura, Y.; Miyamoto, Y. The relationship between work engagement and psychological distress of hospital nurses and the perceived communication behaviors of their nurse managers: A cross-sectional survey. Int. J. Nurs. Stud. 2017, 71, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Schaufeli, W.; Salanova, M.; González-Roma, V.; Bakker, A. The measurement of engagement and burnout: A two sample confirmatory factor analytic approach. J. Happiness Stud. 2002, 3, 71–92. [Google Scholar] [CrossRef]
- Maslach, C.; Schaufeli, W.B.; Leiter, M.P. Job burnout. Annu. Rev. Psychol. 2001, 52, 397–422. [Google Scholar] [CrossRef] [PubMed]
- Schaufeli, W.B.; Bakker, A.B.; Salanova, M. The measurement of work engagement with a short questionnaire: A Cross-national study. Educ. Psychol. Meas. 2006, 66, 701–716. [Google Scholar] [CrossRef]
- Fong, T.C.; Ng, S. Measuring Engagement at Work: Validation of the Chinese Version of the Utrecht Work Engagement Scale. Int. J. Behav. Med. 2012, 19, 391–397. [Google Scholar] [CrossRef] [PubMed]
- Lovakov, A.V.; Agadullina, E.R.; Schaufeli, W.B. Psychometric properties of the Russian version of the Utrecht Work Engagement Scale (UWES-9). Psychol. Russ. State Art 2017, 10, 145–162. [Google Scholar] [CrossRef]
- Mukkavilli, M.; Kulkarni, S.; Doshi, D.; Reddy, S.; Reddy, P.; Reddy, S. Assessment of work engagement among dentists in Hyderabad. Work 2017, 58, 333–340. [Google Scholar] [CrossRef] [PubMed]
- Schaufeli, W.B.; Bakker, A.B. Test Manual for the Utrecht Work Engagement Scale; Utrecht University: Utrecht, The Netherlands, 2004. [Google Scholar]
- Martos, A.; Pérez-Fuentes, M.C.; Molero, M.M.; Gázquez, J.J.; Simón, M.M.; Barragán, A.B. Burnout y engagement en estudiantes de Ciencias de la Salud. Eur. J. Investig. 2018, 8, 23–36. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.; Yansane, A.I.; Zhang, Y.; Fu, H.; Hong, N.; Kalenderian, E. Burnout and study engagement among medical students at Sun Yat-sen University, China: A cross-sectional study. Medicine 2018, 97, e0326. [Google Scholar] [CrossRef] [PubMed]
- Liébana, C.; Fernández, M.; Bermejo, J.C.; Carabias, M.; Rodríguez, M.; Villacieros, M. Inteligencia emocional & vínculo laboral en trabajadores del Centro San Camilo. Gerokomos 2012, 23, 63–68. [Google Scholar]
- Bar-On, R. The Emotional Quotient Inventory (EQ-i): Technical Manual; Multi-Health Systems: Toronto, ON Canada, 1997. [Google Scholar]
- Brunetto, Y.; Teo, S.T.T.; Shacklock, K.; Farr-Wharton, R. Emotional intelligence, job satisfaction, well-being and engagement: Explaining organizational commitment and turnover intentions in policing. Hum. Resour. Manag. 2012, 22, 428–441. [Google Scholar] [CrossRef]
- Carvalho, V.S.; Guerrero, E.; Chambel, M.J. Emotional intelligence and health students’ well-being: A two-wave study with students of medicine, physiotherapy and nursing. Nurse Educ. Today 2018, 63, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Görgens-Ekermans, G.; Brand, T. Emotional intelligence as a moderator in the stress-burnout relationship: A questionnaire study on nurses. J. Clin. Nurs. 2012, 21, 2275–2285. [Google Scholar] [CrossRef] [PubMed]
- Karimi, L.; Leggat, S.G.; Donohue, L.; Farrell, G.; Couper, G.E. Emotional rescue: The role of emotional intelligence and emotional labour on well-being and job-stress among community nurses. J. Adv. Nurs. 2014, 70, 176–186. [Google Scholar] [CrossRef] [PubMed]
- Gerits, L.; Derksen, J.J.; Verbruggen, A.B. Emotional intelligence and adaptative success of nurses caring people with mental retardation and severe behavior problems. Ment. Retard. 2004, 42, 106–121. [Google Scholar] [CrossRef]
- Azimi, S.; AsgharNejad Farid, A.A.; Kharazi Fard, M.J.; Khoei, N. Emotional intelligence of dental students and patient satisfaction. Eur. J. Dent. Educ. 2010, 14, 129–132. [Google Scholar] [CrossRef] [PubMed]
- Van Dusseldorp, L.R.; van Meijel, B.K.; Derksen, J.J. Emotional intelligence of mental health nurses. J. Clin. Nurs. 2011, 20, 555–562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arteche, A.; Chamorro-Premuzic, T.; Furnham, A.; Crump, J. The Relationship of Trait EI with Personality, IQ and sex in a UK sample of employees. Int. J. Sel. Assess. 2008, 16, 421–426. [Google Scholar] [CrossRef]
- Harper, M.G.; Jones-Schenk, J. The emotional intelligence profile of successful staff nurses. J. Contin. Educ. Nurs. 2012, 43, 354–362. [Google Scholar] [CrossRef] [PubMed]
- Kahraman, N.; Hiçdurmaz, D. Identifying emotional intelligence skills of Turkish clinical nurses according to sociodemographic and professional variables. J. Clin. Nurs. 2016, 25, 1006–1015. [Google Scholar] [CrossRef] [PubMed]
- Mérida-López, S.; Extremera, N.; Rey, L. Contributions of Work-Related Stress and Emotional Intelligence to Teacher Engagement: Additive and Interactive Effects. Int. J. Environ. Res. Public Health 2017, 14, 1156. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Liu, C.; Guo, B.; Zhao, L.; Lou, F. The impact of emotional intelligence on work engagement of registered nurses: The mediating role of organizational justice. J. Clin. Nurs. 2015, 24, 2115–2124. [Google Scholar] [CrossRef] [PubMed]
- Garrosa, E.; Moreno-Jiménez, B.; Rodríguez-Muñoz, A.; Rodríguez-Carvajal, R. Role stress and personal resources in nursing: A cross-sectional study of burnout and engagement. Int. J. Nurs. Stud. 2011, 48, 479–489. [Google Scholar] [CrossRef] [PubMed]
- Nel, J.A.; Jonker, C.S.; Rabie, T. Emotional intelligence and wellness among employees working in the nursing environment. J. Psychol. Afr. 2013, 23, 195–203. [Google Scholar] [CrossRef]
- Pérez-Fuentes, M.C.; Gázquez, J.J.; Mercader, I.; Molero, M.M. Brief Emotional Intelligence Inventory for Senior Citizens (EQ-i-M20). Psicothema 2014, 26, 524–530. [Google Scholar] [CrossRef]
- Bar-On, R.; Parker, J.D.A. Emotional Quotient Inventory: Youth Version (EQ-i:YV): Technical Manual; Multi-Health Systems: Toronto, ON, Canada, 2000. [Google Scholar]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; The Guilford Press: New York, NY, USA, 2013. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total n = 2126 | Men n = 321 | Women n = 1805 | t | Sig. | |||||
|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | ||||
| Emotional Intelligence | Intrapersonal | 2.62 | 0.698 | 2.46 | 0.690 | 2.65 | 0.696 | −4.315 *** | 0.000 |
| Interpersonal | 3.06 | 0.501 | 2.94 | 0.530 | 3.08 | 0.493 | −4.609 *** | 0.000 | |
| Stress Management | 3.25 | 0.567 | 3.26 | 0.569 | 3.24 | 0.567 | 0.380 | 0.704 | |
| Adaptability | 2.91 | 0.526 | 2.96 | 0.527 | 2.90 | 0.526 | 2.040 * | 0.042 | |
| General Mood | 3.08 | 0.599 | 3.11 | 0.607 | 3.08 | 0.598 | 0.871 | 0.384 | |
| Engagement | Vigor | 3.85 | 0.771 | 3.72 | 0.808 | 3.87 | 0.762 | −3.131 ** | 0.002 |
| Dedication | 4.07 | 0.794 | 3.94 | 0.884 | 4.09 | 0.775 | −2.843 ** | 0.005 | |
| Absorption | 3.52 | 0.800 | 3.38 | 0.849 | 3.55 | 0.788 | −3.532 *** | 0.000 | |
| Vigor | Model | R | R2 | Adjusted R2 | Change Statistics | Durbin Watson | ||||
| Standard Error of Estimation | Change in R2 | Change in F | Sig. of Change in F | |||||||
| 1 | 0.397 | 0.158 | 0.158 | 0.708 | 0.158 | 398.401 | 0.000 | 1.964 | ||
| 2 | 0.465 | 0.216 | 0.216 | 0.683 | 0.058 | 158.160 | 0.000 | |||
| 3 | 0.473 | 0.224 | 0.223 | 0.680 | 0.008 | 20.508 | 0.000 | |||
| 4 | 0.477 | 0.228 | 0.226 | 0.678 | 0.004 | 10.834 | 0.001 | |||
| Model 4 | Non-standardized Coefficients | Standardized Coefficients | t | Sig. | Collinearity | |||||
| B | std. error | Beta | Tol. | VIF | ||||||
| (Constant) | 1.134 | 0.118 | 9.593 | 0.000 | ||||||
| General Mood | 0.264 | 0.033 | 0.205 | 8.104 | 0.000 | 0.570 | 1.756 | |||
| Interpersonal | 0.364 | 0.037 | 0.236 | 9.953 | 0.000 | 0.647 | 1.547 | |||
| Stress Management | 0.128 | 0.028 | 0.094 | 4.629 | 0.000 | 0.879 | 1.138 | |||
| Adaptability | 0.128 | 0.039 | 0.087 | 3.292 | 0.001 | 0.519 | 1.928 | |||
| Dedication | Model | R | R2 | Adjusted R2 | Change Statistics | Durbin Watson | ||||
| Standard Error of Estimation | Change in R2 | Change in F | Sig. of Change in F | |||||||
| 1 | 0.407 | 0.165 | 0.165 | 0.726 | 0.165 | 420.764 | 0.000 | 1.941 | ||
| 2 | 0.458 | 0.210 | 0.209 | 0.706 | 0.044 | 119.178 | 0.000 | |||
| 3 | 0.466 | 0.217 | 0.216 | 0.703 | 0.007 | 19.051 | 0.000 | |||
| 4 | 0.467 | 0.219 | 0.217 | 0.703 | 0.002 | 4.800 | 0.029 | |||
| Model 4 | Non-Standardized Coefficients | Standardized Coefficients | t | Sig. | Collinearity | |||||
| B | std. error | Beta | Tol. | VIF | ||||||
| (Constant) | 1.391 | 0.122 | 11.449 | 0.000 | ||||||
| General Mood | 0.336 | 0.031 | 0.253 | 10.688 | 0.000 | 0.655 | 1.526 | |||
| Interpersonal | 0.354 | 0.035 | 0.223 | 10.026 | 0.000 | 0.745 | 1.343 | |||
| Stress Management | 0.130 | 0.029 | 0.093 | 4.510 | 0.000 | 0.875 | 1.142 | |||
| Intrapersonal | 0.054 | 0.025 | 0.048 | 2.191 | 0.029 | 0.774 | 1.292 | |||
| Absorption | Model | R | R2 | Adjusted R2 | Change statistics | Durbin Watson | ||||
| Standard Error of Estimation | Change in R2 | Change in F | Sig. of Change in F | |||||||
| 1 | 0.316 | 0.100 | 0.100 | 0.759 | 0.100 | 236.011 | 0.000 | 1.961 | ||
| 2 | 0.362 | 0.131 | 0.130 | 0.746 | 0.031 | 76.359 | 0.000 | |||
| 3 | 0.369 | 0.136 | 0.135 | 0.744 | 0.005 | 12.570 | 0.000 | |||
| 4 | 0.374 | 0.140 | 0.138 | 0.743 | 0.003 | 8.322 | 0.004 | |||
| Model 4 | Non-Standardized Coefficients | Standardized Coefficients | t | Sig. | Collinearity | |||||
| B | std. error | Beta | Tol. | VIF | ||||||
| (Constant) | 1.361 | 0.128 | 10.598 | 0.000 | ||||||
| Interpersonal | 0.325 | 0.037 | 0.204 | 8.725 | 0.000 | 0.745 | 1.343 | |||
| General Mood | 0.202 | 0.033 | 0.152 | 6.093 | 0.000 | 0.655 | 1.526 | |||
| Intrapersonal | 0.098 | 0.026 | 0.086 | 3.743 | 0.000 | 0.774 | 1.292 | |||
| Stress Management | 0.088 | 0.030 | 0.062 | 2.885 | 0.004 | 0.875 | 1.142 | |||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Fuentes, M.D.C.; Molero Jurado, M.D.M.; Gázquez Linares, J.J.; Oropesa Ruiz, N.F. The Role of Emotional Intelligence in Engagement in Nurses. Int. J. Environ. Res. Public Health 2018, 15, 1915. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15091915
Pérez-Fuentes MDC, Molero Jurado MDM, Gázquez Linares JJ, Oropesa Ruiz NF. The Role of Emotional Intelligence in Engagement in Nurses. International Journal of Environmental Research and Public Health. 2018; 15(9):1915. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15091915
Chicago/Turabian StylePérez-Fuentes, María Del Carmen, María Del Mar Molero Jurado, José Jesús Gázquez Linares, and Nieves Fátima Oropesa Ruiz. 2018. "The Role of Emotional Intelligence in Engagement in Nurses" International Journal of Environmental Research and Public Health 15, no. 9: 1915. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15091915