Work Related Stress, Well-Being and Cardiovascular Risk among Flight Logistic Workers: An Observational Study

 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
- -
- smoking habit: current smokers vs. former smoker or never smokers;
- -
- recreational physical activity: regular, if the subject exercised at least twice per week vs. sporadic (<2 times per week) or none;
- -
- alcohol intake: abstinent or sporadic (<1 alcohol unit per day, such as social drinking) vs. only on the weekend vs. at least 1 alcohol unit daily;
- -
- coffee intake: low (<2 per day), medium (2–4 per day), and high (>4 per day);
- -
- type of shiftwork schedule: fixed daytime workers vs. h12 vs. h24 shift workers;
- -
- education: low (≤8 years of education), medium (8–13 years), and high (>13 years with a degree); and
- -
- job tasks: operative jobs, security personnel, administrative jobs/ flight control personnel.
2.2. Work Related Stress and Well-Being Assessment
2.3. Cardiovascular Risk Assessment
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Lopez, A.D.; Mathers, C.D.; Ezzati, M.; Jamison, D.T.; Murray, C.J.L. Global and Regional Burden of Disease and Risk Factors, 2001: Systematic Analysis of Population Health Data. Lancet 2006, 367, 1747–1757. [Google Scholar] [CrossRef]
- Kreatsoulas, C.; Anand, S.S. The Impact of Social Determinants on Cardiovascular Disease. Can. J. Cardiol. 2010, 26 (Suppl. C), 8C–13C. [Google Scholar] [CrossRef]
- Portoghese, I.; Galletta, M.; Burdorf, A.; Cocco, P.; D’Aloja, E.; Campagna, M. Role Stress and Emotional Exhaustion Among Health Care Workers: The Buffering Effect of Supportive Coworker Climate in a Multilevel Perspective. J. Occup. Environ. Med. 2017, 59, e187–e193. [Google Scholar] [CrossRef] [PubMed]
- Kivimaki, M.; Virtanen, M.; Elovainio, M.; Kouvonen, A.; Vaananen, A.; Vahtera, J. Work stress in the etiology of coronary heart disease—A meta-analysis. Scand. J. Work Environ. Health 2006, 32, 431–442. [Google Scholar] [CrossRef] [PubMed]
- Belkic, K.L.; Landsbergis, P.A.; Schnall, P.L.; Baker, D. Is job strain a major source of cardiovascular disease risk? Scand. J. Work Environ. Health 2004, 30, 85–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- United Nations. World Population Prospects the 2012 Revision Highlights and Advance Tables. New York, NY, USA, 2012. Available online: https://esa.un.org/unpd/wpp/ publications/Files/WPP2012_HIGHLIGHTS.pdf (accessed on 27 July 2018).
- CIIP–Consulta Interassociativa Italiana per la Prevenzione. Libro D’argento. Campagna 2016–2017: Ambienti di Lavoro Sani e Sicuri Ad Ogni età. E-book “Invecchiamento e Lavoro”. 2017. Available online: https://www.ciip-consulta.it/images/AgingEbook/Aging EBook.1.pdf (accessed on 27 July 2018).
- European Agency for Safety and Health at Work. Healthy Workplaces for All Ages. 2016. Available online: https:// www.healthy-workplaces.eu (accessed on 27 July 2018).
- WHO. Workplace Health Protection and Promotion in the Policy and Practice of Social and Health Insurance Institutions Report on a WHO Meeting. 1999. Available online: http://www.who.int/occupational_health/regions/en/ oeheurworkplaceprotect.pdf?ua=1 (accessed on 27 July 2018).
- The European Network for Workplace Health Promotion (ENWHP). Luxembourg Declaration on Workplace Health Promotion in the European Union 2 Luxembourg Declaration on Workplace Health Promotion. 2007. Available online: http://www.enwhp.org/fileadmin/rs-dokumente/dateien/Luxembourg_Declaration.pdf (accessed on 27 July 2018).
- Italian Ministry of Health. Protocollo di Intesa tra Ministero della salute e Società Italiana di Medicina del Lavoro. Rome, Italy, 2018. Available online: http://www.salute.gov.it/imgs/C_17_notizie_3292_listaFile_itemName_0_file.pdf (accessed on 27 July 2018).
- Wulsin, L.; Herman, J.; Thayer, J.F. Stress, autonomic imbalance, and the prediction of metabolic risk: A model and a proposal for research. Neurosci. Biobehav. Rev. 2018, 86, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Gilbert-Ouimet, M.; Trudel, X.; Brisson, C.; Milot, A.; Vézina, M. Adverse effects of psychosocial work factors on blood pressure: Systematic review of studies on demand–control–support and effort–reward imbalance models. Scand. J. Work Environ. Health 2014, 40, 109–132. [Google Scholar] [CrossRef] [PubMed]
- Magnavita, N.; Fileni, A. Work stress and metabolic syndrome in radiologists: First evidence. Radiol. Med. 2014, 119, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Enoki, M.; Maeda, E.; Iwata, T.; Murata, K. The Association between Work-Related Stress and Autonomic Imbalance among Call Center Employees in Japan. Tohoku J. Exp. Med. 2017, 243, 321–328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stansfeld, S.; Candy, B. Psychosocial work environment and mental health—A meta-analytic review. Scand. J. Work Environ. Health 2006, 32, 443–462. [Google Scholar] [CrossRef] [PubMed]
- Siegrist, J. Adverse health effects of high-effort/low-reward conditions. J. Occup. Health Psychol. 1996, 1, 27–41. [Google Scholar] [CrossRef] [PubMed]
- Karasek, R.; Brisson, C.; Kawakami, N.; Houtman, I.; Bongers, P.; Amick, B. The Job Content Questionnaire (JCQ): An instrument for internationally comparative assessments of psychosocial job characteristics. J. Occup. Health Psychol. 1998, 3, 322–355. [Google Scholar] [CrossRef] [PubMed]
- Karasek, R.A. Job Demands, Job Decision Latitude, and Mental Strain: Implications for Job Redesign. Adm. Sci. Q. 1979, 24, 285–308. [Google Scholar] [CrossRef]
- Karasek, R.; Theorell, T. Healthy Work: Stress, Productivity and the Reconstruction of Working Life; Basic Books: New York, NY, USA, 1990. [Google Scholar]
- Häusser, J.A.; Mojzisch, A.; Niesel, M.; Schulz-Hardt, S. Ten years on: A review of recent research on the Job Demand–Control (-Support) model and psychological well-being. Work Stress 2010, 24, 1–35. [Google Scholar] [CrossRef]
- Mancia, G.; Fagard, R.; Narkiewicz, K.; Redon, J.; Zanchetti, A.; Böhm, M.; Christiaens, T.; Cifkova, R.; De Backer, G.; Dominiczak, A.; et al. 2013 ESH/ESC guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur. Heart J. 2013, 34, 2159–2219. [Google Scholar] [PubMed]
- Yumuk, V.; Tsigos, C.; Fried, M.; Schindler, K.; Busetto, L.; Micic, D.; Toplak, H. Obesity Management Task Force of the European Association for the Study of Obesity. European Guidelines for Obesity Management in Adults. Obes. Facts 2015, 8, 402–424. [Google Scholar] [CrossRef] [PubMed]
- INAIL. La Metodologia per la Valutazione e Gestione del Rischio Stress Lavoro-Correlato. 2017. Available online: https://www.inail.it (accessed on 23 August 2018).
- Cousins, R.; MacKay, C.J.; Clarke, S.D.; Kelly, C.; Kelly, P.J.; McCaig, R.H. ‘Management Standards’ work-related stress in the UK: Practical development. Work Stress 2004, 18, 113–136. [Google Scholar] [CrossRef]
- Topp, C.W.; Østergaard, S.D.; Søndergaard, S.; Bech, P. The WHO-5 well-being index: A systematic review of the literature. Psychother. Psychosom. 2015, 84, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Framingham Heart Study. Available online: http://www.framinghamheartstudy.org/risk-functions/cardiovascular-disease/10-year-risk.php# (accessed on 12 June 2018).
- D’Agostino, R.B.; Vasan, R.S.; Pencina, M.J.; Wolf, P.A.; Cobain, M.; Massaro, J.M.; Kannel, W.B. General cardiovascular risk profile for use in primary care: The Framingham heart study. Circulation 2008, 117, 743–753. [Google Scholar] [CrossRef] [PubMed]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.T.; Corrà, U.; Cosyns, B.; Deaton, C.; et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts) Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar] [PubMed]
- Cesana, G.; Sega, R.; Ferrario, M.; Chiodini, P.; Corrao, G.; Mancia, G. Job Strain and Blood Pressure in Employed Men and Women. Psychosom. Med. 2003, 65, 558–563. [Google Scholar] [CrossRef] [PubMed]
- Saijo, Y.; Chiba, S.; Yoshioka, E.; Nakagi, Y.; Ito, T.; Kitaoka-Higashiguchi, K.; Yoshida, T. Synergistic interaction between job control and social support at work on depression, burnout, and insomnia among Japanese civil servants. Int. Arch. Occup. Environ. Health 2014, 88, 143–152. [Google Scholar] [CrossRef] [PubMed]
- Birket-Smith, M.; Hansen, B.H.; Hanash, J.A.; Hansen, J.F.; Rasmussen, A. Mental disorders and general well-being in cardiology outpatients-6-year survival. J. Psychosom. Res. 2009, 67, 5–10. [Google Scholar] [CrossRef] [PubMed]
- Borchini, R.; Ferrario, M.M.; Bertù, L.; Veronesi, G.; Bonzini, M.; Dorso, M.; Cesana, G. Prolonged job strain reduces time-domain heart rate variability on both working and resting days among cardiovascular-susceptible nurses. Int. J. Occup. Med. Environ. Health 2015, 28, 42–51. [Google Scholar] [CrossRef] [PubMed]
- Collins, S.; Karasek, R. Reduced vagal cardiac control variancein exhausted and high strain job subjects. Int. J. Occup. Med. Environ. Health. 2010, 23, 267–278. [Google Scholar] [CrossRef] [PubMed]
- Edwards, E.M.; Stuver, S.O.; Heeren, T.C.; Fredman, L. Job Strain and Incident Metabolic Syndrome Over 5 Years of Follow-up: The Coronary Artery Risk Development in Young Adults Study. J. Occup. Environ. Med. Am. Coll. Occup. Environ. Med. 2012, 54, 1447–1452. [Google Scholar] [CrossRef] [PubMed]
- Babu, G.R.; Jotheeswaran, A.; Mahapatra, T.; Mahapatra, S.; Kumar, A.; Detels, R.; Pearce, N. Is hypertension associated with job strain? A meta-analysis of observational studies. Occup. Environ. Med. 2014, 71, 220–227. [Google Scholar] [CrossRef] [PubMed]
- Mutambudzi, M.; Javed, Z. Job Strain as a Risk Factor for Incident Diabetes Mellitus in Middle and Older Age, U.S. Workers. J. Gerontol. B Psychol. Sci. Soc. Sci. 2016, 71, 1089–1096. [Google Scholar] [CrossRef] [PubMed]
- Tang, K.L.; Rashid, R.; Godley, J.; Ghali, W.A. Association between subjective social status and cardiovascular disease and cardiovascular risk factors: A systematic review and meta-analysis. BMJ Open 2016, 6, e010137. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, G.A.; Keil, J.E. Socioeconomic factors and cardiovascular disease: A review of the literature. Circulation 1993, 88, 1973–1998. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Ruan, W.; Chen, Z.; Peng, Y.; Li, W. Shift work and risk of cardiovascular disease morbidity and mortality: A dose–response meta-analysis of cohort studies. Eur. J. Prev. Cardiol. 2018, 25, 1293–1302. [Google Scholar] [CrossRef] [PubMed]
- Aiyar, S.; Ebeke, C.; Shao, X. The Impact of Workforce Aging on European Productivity. IMF Work Paper. 2016. Available online: https://www.imf.org/external/pubs/ft/wp/2016/wp16238.pdf (accessed on 29 July 2018).
- Seitsamo, J.; Ilmarinen, J. Life-style, aging and work ability among active Finnish workers in 1981–1992. Scand. J. Work Environ. Health 1997, 23, 20–26. [Google Scholar] [PubMed]
- European Social Partners. European Social Partners’ Autonomous Framework Agreement on Active Ageing and an Inter-generational Approach. 2017. Available online: http://www.ceep.eu/wp-content/uploads/2017/03/Without-signatures_Framework-agreement-on-active-ageing.pdf (accessed on 29 July 2018).
- ISTAT. Italia in Cifre. 2016. Available online: http://www.istat.it (accessed on 29 July 2018).
- Corbett, D.B.; Fennell, C.; Peroutky, K.; Kingsley, J.D.; Glickman, E.L. The effects of a 12-week worksite physical activity intervention on anthropometric indices, blood pressure indices, and plasma biomarkers of cardiovascular disease risk among university employees NCT03385447 NCT. BMC Res. Notes 2018, 11, 80. [Google Scholar] [CrossRef] [PubMed]
- Cahill, K.; Lancaster, T. Workplace interventions for smoking cessation. Cochrane Database Syst. Rev. 2014, 26, CD003440. [Google Scholar] [CrossRef] [PubMed]
- Sultan-Taïeb, H.; Chastang, J.F.; Mansouri, M.; Niedhammer, I. The annual costs of cardiovascular diseases and mental disorders attributable to job strain in France. BMC Public Health 2013, 13, 748. [Google Scholar] [CrossRef] [PubMed]
- Maeda, E.; Iwata, T.; Murata, K. Effects of work stress and home stress on autonomic nervous function in Japanese male workers. Ind. Health 2015, 53, 132–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dupre, M.E.; Nelson, A.; Lynch, S.M.; Granger, B.B.; Xu, H.; Churchill, E.; Willis, J.M.; Curtis, L.H.; Peterson, E.D. Socioeconomic, Psychosocial and Behavioral Characteristics of Patients Hospitalized with Cardiovascular Disease. Am. J. Med. Sci. 2017, 354, 565–572. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| n. | % | Denominator | |
|---|---|---|---|
| Total workforce | 1572 | 100 | 1572 |
| Potentially eligible for study | 617 | 39.2 | 1572 |
| Confirmed eligible | 568 | 92 | 617 |
| Included in the study | 568 | 92 | 617 |
| Causes for exclusion | |||
| - Female gender | 2 | 0.3 | 617 |
| - <30 years of age | 39 | 6 | 617 |
| - Previous diagnosis of CVD | 4 | 0.6 | 617 |
| myocardial infarction | 2 | 0.3 | 617 |
| ischemic heart disease | 1 | 0.1 | 617 |
| dilated cardiomyopathy | 1 | 0.1 | 617 |
| - Questionnaire incomplete | 3 | 0.5 | 617 |
| - Did not match the criteria for CVD risk calculation (SBP < 90 mmHg). | 1 | 0.1 | 617 |
| Parametric Variables | Min. | Max | Mean | sd |
|---|---|---|---|---|
| Age (years) | 30 | 63 | 44.9 | 6.69 |
| Duration of employment (years) | 1 | 39 | 7.00 | 7.37 |
| Weight (kg) | 57 | 118 | 78.9 | 9.90 |
| Height (m) | 1.52 | 1.92 | 1.74 | 0.06 |
| BMI (kg/m2) | 19.3 | 39.5 | 25.9 | 2.92 |
| SBP (mmHg) | 90 | 180 | 126.6 | 13.71 |
| DBP (mmHg) | 60 | 110 | 80.8 | 8.24 |
| Heart Rate (bpm) | 39 | 132 | 66.3 | 11.57 |
| Non-Parametric Scores | Median | Interquartile Range | ||
| WHO-5 index | 14 | 11–17 | ||
| CVD risk score | 7.7 | 5.02–12.47 | ||
| Job Demand score | 15 | 12–18 | ||
| Job Control score | 22 | 19–25 | ||
| Job Support score | 17 | 15–18 | ||
| Categorical Variables | N | % | ||
| Physical activity | Sporadic/none | 229 | 40.3 | |
| regular | 339 | 59.7 | ||
| Smoking habit | Never/former | 434 | 76.4 | |
| Smokers | 134 | 23.6 | ||
| Alcohol intake | abstinent | 278 | 48.9 | |
| weekend | 126 | 22.2 | ||
| regular | 164 | 28.9 | ||
| Coffee | Low | 170 | 29.9 | |
| Medium | 315 | 55.5 | ||
| High | 83 | 14.6 | ||
| Educational level | Low | 236 | 41.5 | |
| Medium | 314 | 55.3 | ||
| high | 17 | 3.0 | ||
| Shiftwork schedule | Fixed diurnal | 415 | 73.1 | |
| h12 | 104 | 18.3 | ||
| h24 | 49 | 8.6 | ||
| CVD risk class | Low < 10% | 365 | 64.3 | |
| Medium 10–20% | 163 | 28.7 | ||
| High > 20% | 40 | 7 | ||
| Jobs | Operative jobs | 447 | 78.7 | |
| Security personnel | 36 | 6.3 | ||
| Administrative jobs/flight control personnel | 82 | 14.4 | ||
| Missing | 3 | 0.5 | ||
| Karasek’s Categories | Low Job Support N. (%) | High Job Support N. (%) | All N. (%) |
|---|---|---|---|
| High strain | 100 (36.1) | 55 (18.9) | 155 (27.3) |
| Low strain | 58 (20.9) | 124 (42.6) | 182 (32.0) |
| Passive | 51 (18.4) | 41 (24.4) | 92 (16.2) |
| Active | 68 (24.5) | 71 (18.9) | 139 (24.5) |
| All | 277 (100) | 291 (100) | 568 (100) |
| Passive | Low Strain | Active | High Strain | Kruskal–Wallis | |||||
|---|---|---|---|---|---|---|---|---|---|
| N = 92 (16.2%) | N = 182 (32%) | N = 139 (24.5%) | N = 155 (27.3%) | p | |||||
| Med | IQR | Med | IQR | Med | IQR | Med | IQR | ||
| CVD risk score | 7.6 | 4.72–10.82 | 7.5 | 5.05–12.52 | 8.5 | 5–13.4 | 8.0 | 5.2–11.7 | 0.463 |
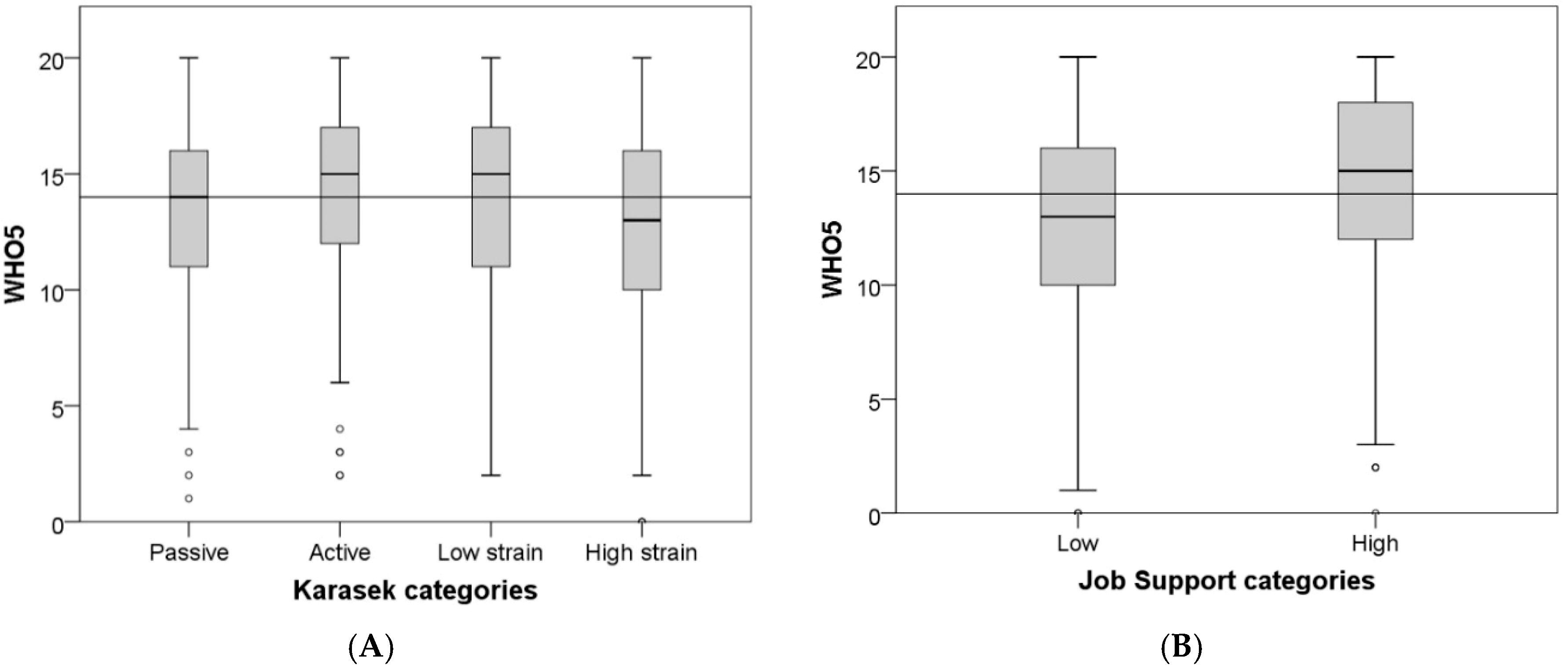
| WHO-5 | 14.0 | 11–16 | 15.00 | 11–17 | 15.0 | 12–17 | 13.0 | 10–17 | 0.005 |
| Low Support | High Support | p | |||||||
| N (%) = 277 (48.8) | N (%) = 291 (51.2) | ||||||||
| Median | IQR | Median | IQR | ||||||
| CVD Risk score | 8.4 | 5.45–12.4 | 7.3 | 4.4–12.6 | 0.042 | ||||
| WHO-5 | 13 | 10–16 | 15 | 12–18 | <0.001 | ||||
| CV RISK Score | Educational Level | Duration of Employment | Alcohol | Coffee | Physical Activity | WHO-5 | Heart Rate | Demand Score | Control Score | Support Score | DBP | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CVD RISK score | 1.000 | −0.286 ** | 0.061 | 0.096 * | 0.029 | −0.183 ** | −0.217 ** | 0.211 ** | 0.038 | 0.044 | −0.088 * | 0.415 ** |
| Educational level | 1.000 | −0.115 ** | −0.059 | −0.013 | 0.071 | 0.047 | −0.121 ** | −0.014 | 0.032 | 0.065 | −0.100 * | |
| Duration of employment | 1.000 | 0.033 | 0.016 | 0.011 | 0.002 | 0.024 | 0.097 * | 0.035 | 0.040 | −0.018 | ||
| Alcohol | 1.000 | 0.021 | −0.044 | −0.043 | −0.006 | −0.023 | −0.002 | −0.060 | 0.071 | |||
| Coffee | 1.000 | −0.022 | −0.047 | −0.015 | 0.002 | −0.011 | −0.091 * | −0.110 ** | ||||
| Physical activity | 1.000 | 0.089 * | −0.253 ** | −0.027 | −0.021 | −0.054 | −0.112 ** | |||||
| WHO-5 | 1.000 | −0.022 | −0.083 * | 0.162 ** | 0.319 ** | −0.032 | ||||||
| Heart Rate | 1.000 | 0.010 | −0.045 | 0.053 | 0.198 ** | |||||||
| Demand score | 1.000 | −0.232 ** | −0.235 ** | 0.071 | ||||||||
| Control score | 1.000 | 0.321 ** | −0.021 | |||||||||
| Support score | 1.000 | −0.051 | ||||||||||
| DBP | 1.000 |
| Variables | Regression Coefficient | Standard Error | p-Value |
|---|---|---|---|
| Intercept | −12.3432 | 3.5383 | 0.0005 |
| Job demand Score | −0.0055 | 0.0562 | 0.9218 |
| Job control Score | 0.0010 | 0.0642 | 0.9871 |
| Job support Score | −0.2003 | 0.0946 | 0.0348 |
| Education low | 3.0705 | 1.5274 | 0.0449 |
| Education medium | −0.1747 | 1.5076 | 0.9078 |
| Education high | 0 | ||
| Alcohol abstinent | −1.5613 | 0.6012 | 0.0097 |
| Alcohol weekend | −2.2325 | 0.7279 | 0.0023 |
| Alcohol regular | 0 | ||
| Physical activity no | 2.0583 | 0.5237 | <0.0001 |
| Physical activity yes | 0 | ||
| DBP | 0.3051 | 0.0313 | <0.0001 |
| Variables | Regression Coefficient | Standard Error | p-Value |
|---|---|---|---|
| Intercept | 9.227238 | 2.644922 | 0.0005 |
| Job demand Score | 0.016800 | 0.036697 | 0.6473 |
| Job control Score | 0.118277 | 0.041802 | 0.0048 |
| Job support Score | 0.350821 | 0.061604 | <0.0001 |
| Age | −0.144603 | 0.027782 | <0.0001 |
| Duration of employment | −0.018262 | 0.023119 | 0.4299 |
| BMI | −0.022687 | 0.059988 | 0.7054 |
| SBP | 0.008469 | 0.017112 | 0.6209 |
| DBP | 0.024156 | 0.028681 | 0.4000 |
| Education low | 0.020035 | 1.024678 | 0.9844 |
| Education medium | −0.360648 | 1.003554 | 0.7195 |
| Education high | 0 | ||
| Smoke yes | 0.551132 | 0.407182 | 0.1764 |
| Smoke no | 0 | ||
| Alcohol abstinent | 0.333081 | 0.389784 | 0.3932 |
| Alcohol weekend | 0.365157 | 0.473053 | 0.4405 |
| Alcohol regular | 0 | ||
| Physical activity no | −0.702412 | 0.347177 | 0.0435 |
| Physical activity yes | 0 |
| Variables | Regression Coefficient | Standard Error | p-Value |
|---|---|---|---|
| Intercept | 17.582239 | 2.460948 | <0.0001 |
| Passive job | 0.384755 | 0.531633 | 0.4695 |
| Low strain job | 1.107803 | 0.451790 | 0.0145 |
| Active job | 1.334118 | 0.472754 | 0.0049 |
| High strain job | 0 | ||
| Low support | −1.752851 | 0.349728 | <0.0001 |
| High support | 0 | ||
| BMI | 0.003551 | 0.061233 | 0.9538 |
| Age | −0.154161 | 0.028269 | <0.0001 |
| Duration of employment | −0.015653 | 0.023584 | 0.5071 |
| SBP | 0.009537 | 0.017722 | 0.5907 |
| DBP | 0.026729 | 0.029447 | 0.3644 |
| Education low | −0.217933 | 1.044671 | 0.8348 |
| Education medium | −0.611723 | 1.023010 | 0.5501 |
| Education high | 0 | ||
| Alcohol abstinent | 0.422055 | 0.398017 | 0.2894 |
| Alcohol weekend | 0.573967 | 0.483081 | 0.2353 |
| Alcohol regular | 0 | ||
| Physical activity no | −0.755701 | 0.354033 | 0.0332 |
| Physical activity yes | 0 | ||
| Smoke yes | 0.631464 | 0.413891 | 0.1277 |
| Smoke no | 0 | ||
| Daily shift | −0.244642 | 0.614323 | 0.6906 |
| H12 shift | −0.157054 | 0.698115 | 0.8221 |
| H24 shift | 0 |
| Karasek’s Categories | Low Job Support Median Predicted CVD Risk (IQR) | High Job Support Median Predicted CVD Risk (IQR) |
|---|---|---|
| Passive | 10.18 (7.28–11.94) | 8.93 (5.78–11.59) |
| Low strain | 9.87 (8.33–12.39) | 8.54 (6.59–11.32) |
| Active | 10.11 (7.54–12.47) | 9.85 (5.78–11.63) |
| High strain | 10.29 (7.39–12.93) | 8.44 (6.85–12.14) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lecca, L.I.; Campagna, M.; Portoghese, I.; Galletta, M.; Mucci, N.; Meloni, M.; Cocco, P. Work Related Stress, Well-Being and Cardiovascular Risk among Flight Logistic Workers: An Observational Study. Int. J. Environ. Res. Public Health 2018, 15, 1952. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15091952
Lecca LI, Campagna M, Portoghese I, Galletta M, Mucci N, Meloni M, Cocco P. Work Related Stress, Well-Being and Cardiovascular Risk among Flight Logistic Workers: An Observational Study. International Journal of Environmental Research and Public Health. 2018; 15(9):1952. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15091952
Chicago/Turabian StyleLecca, Luigi Isaia, Marcello Campagna, Igor Portoghese, Maura Galletta, Nicola Mucci, Michele Meloni, and Pierluigi Cocco. 2018. "Work Related Stress, Well-Being and Cardiovascular Risk among Flight Logistic Workers: An Observational Study" International Journal of Environmental Research and Public Health 15, no. 9: 1952. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15091952