Do Progestin-Only Contraceptives Contribute to the Risk of Developing Depression as Implied by Beta-Arrestin 1 Levels in Leukocytes? A Pilot Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participant Recruitment
2.2. HAM-D Scores
2.3. Isolation of Mononuclear Leukocytes
2.4. Enzyme-Linked Immunosorbent Assay (ELISA)
2.5. Statistical Analyses
3. Results
3.1. Demographics
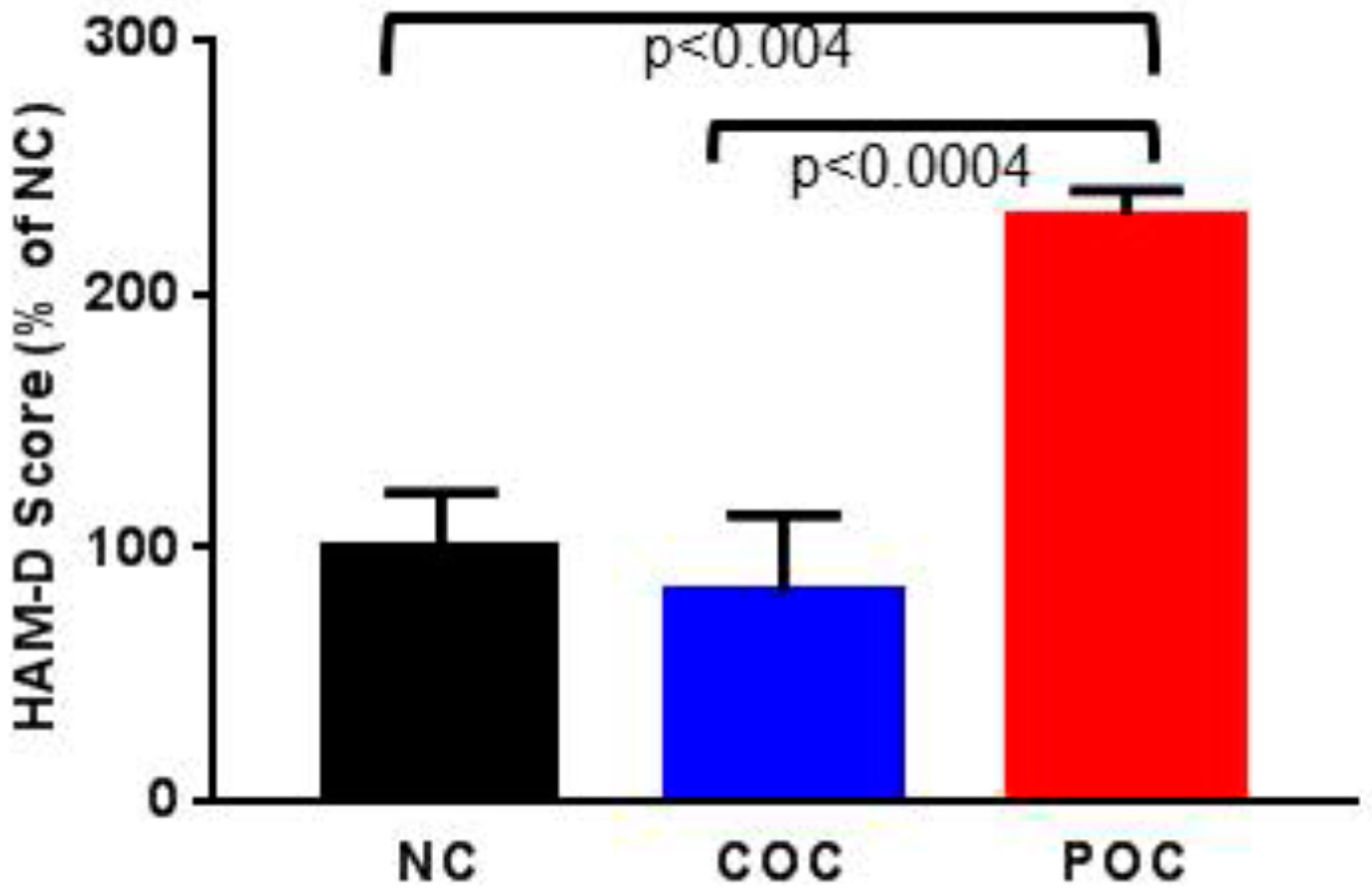
3.2. HAM-D Scores
3.3. β-AR 1 Protein Levels
3.4. Potential Confounders
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hammarstrom, A.; Lehti, A.; Danielsson, U.; Bengs, C.; Johansson, E.E. Gender-related explanatory models of depression: A critical evaluation of medical articles. Public Health 2009, 123, 689–693. [Google Scholar] [CrossRef] [PubMed]
- Farr, S.L.; Dietz, P.M.; Williams, J.R.; Gibbs, F.A.; Tregear, S. Depression screening and treatment among non-pregnant women of reproductive age in the United States, 1990–2010. Prev. Chronic Dis. 2011, 8, 1–15. [Google Scholar]
- Hall, K.S.; Steinberg, J.R.; Cwiak, C.A.; Allen, R.H.; Marcus, S.M. Contraception and mental health: A commentary on the evidence and principles for practice. Am. J. Obstet. Gynecol. 2015, 212, 740–746. [Google Scholar] [CrossRef] [PubMed]
- Skovlund, C.W.; Morch, L.S.; Kessing, L.V.; Lidegaard, O. Association of hormonal contraception with depression. JAMA Psychiatry 2016, 73, 1154–1162. [Google Scholar] [CrossRef] [PubMed]
- Duke, J.M.; Sibbritt, D.W.; Young, A.F. Is there an association between the use of oral contraception and depressive symptoms in young Australian women? Contraception 2007, 75, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Toffol, E.; Heikinheimo, O.; Koponen, P.; Luoto, R.; Partonen, T. Further evidence for lack of negative associations between hormonal contraception and mental health. Contraception 2012, 86, 470–480. [Google Scholar] [CrossRef] [PubMed]
- Keyes, K.M.; Cheslack-Postava, K.; Westhoff, C.; Heim, C.M.; Haloossim, M.; Walsh, K.; Koenen, K. Association of hormonal contraceptive use with reduced levels of depressive symptoms: A national study of sexually active women in the United States. Am. J. Epidemiol. 2013, 178, 1378–1388. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, M.J.; Waugh, M.S. Oral contraceptive discontinuation: A prospective evaluation of frequency and reasons. Am. J. Obstet. Gynecol. 1998, 179, 577–582. [Google Scholar] [CrossRef]
- Sanders, S.A.; Graham, C.A.; Bass, J.L.; Bancroft, J. A prospective study of the effects of oral contraceptives on sexuality and well-being and their relationship to discontinuation. Contraception 2001, 64, 51–58. [Google Scholar] [CrossRef]
- Poromaa, I.S.; Segebladh, B. Adverse mood symptoms with oral contraceptives. Acta Obstet. Gynecol. Scand. 2012, 91, 420–427. [Google Scholar] [CrossRef] [PubMed]
- Hall, K.; Moreau, C.; Trussell, J.; Barber, J. Role of young women’s depression and stress symptoms in their weekly use and nonuse of contraceptive methods. J. Adolesc. Health 2013, 53, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Zethraeus, N.; Dreber, A.; Ranehill, E.; Blomberg, L.; Labrie, F.; von Schoultz, B.; Johannesson, M.; Hirschberg, A.L. A first-choice combined oral contraceptive influences general well-being in healthy women: A double-blind, randomized, placebo-controlled trial. Fertil. Steril. 2017, 107, 1238–1245. [Google Scholar] [CrossRef] [PubMed]
- Archer, B.; Irwin, D.; Jensen, K.; Johnson, M.E.; Rorie, J. Depot medroxyprogesterone. Management of side-effects commonly associated with its contraceptive use. J. Nurse Midwifery 1997, 42, 104–111. [Google Scholar] [CrossRef]
- Svendal, G.; Berk, M.; Pasco, J.A.; Jacka, F.N.; Lund, A.; Williams, L.J. The use of hormonal contraceptive agents and mood disorders in women. J. Affect. Disord. 2012, 140, 92–96. [Google Scholar] [CrossRef] [PubMed]
- St-Andre, M.; Stikarovska, I.; Gascon, S. Clinical case rounds in child and adolescent psychiatry: De novo self-mutilation and depressive symptoms in a 17-year-old adolescent girl receiving depot-medroxyprogesterone acetate. J. Can. Acad. Child Adolesc. Psychiatry 2012, 21, 59–62. [Google Scholar] [PubMed]
- Kuntz, K.; McCullough, S.; Beach, P. Do progesterone-only contraceptives lead to more mood changes than other types? J. Fam. Pract. 2016, 65, 938–943. [Google Scholar] [PubMed]
- Avissar, S.; Matuzany-Ruban, A.; Tzukert, K.; Schreiber, G. Beta-arrestin-1 levels: Reduced in leukocytes of patients with depression and elevated by antidepressants in rat brain. Am. J. Psychiatry 2004, 161, 2066–2072. [Google Scholar] [CrossRef] [PubMed]
- Schreiber, G.; Golan, M.; Avissar, S. Beta-arrestin signaling complex as a target for antidepressants and as a depression marker. Drug News Perspect. 2009, 22, 467–480. [Google Scholar] [PubMed]
- Golan, M.; Schreiber, G.; Avissar, S. Antidepressants increase beta-arrestin 2 ubiquitinylation and degradation by the proteasomal pathway in C6 rat glioma cells. J. Pharmacol. Exp. Ther. 2010, 332, 970–976. [Google Scholar] [CrossRef] [PubMed]
- David, D.J.; Samuels, B.A.; Rainer, Q.; Wang, J.W.; Marsteller, D.; Mendez, I.; Drew, M.; Craig, D.A.; Guiard, B.P.; Guilloux, J.P.; et al. Neurogenesis-dependent and -independent effects of fluoxetine in an animal model of anxiety/depression. Neuron 2009, 62, 479–493. [Google Scholar] [CrossRef] [PubMed]
- Alam, F.; Nayyar, S.; Richie, W.; Archibong, A.; Nayyar, T. Beta-arrestin 1 levels in mononuclear leukocytes support depression scores for women with premenstrual dysphoric disorder. Int. J. Environ. Res. Public Health 2016, 13, 43. [Google Scholar] [CrossRef] [PubMed]
- Mendez-David, I.; El-Ali, Z.; Hen, R.; Falissard, B.; Corruble, E.; Gardier, A.M.; Kerdine-Romer, S.; David, D.J. A method for biomarker measurements in peripheral blood mononuclear cells isolated from anxious and depressed mice: Beta-arrestin 1 protein levels in depression and treatment. Front. Pharmacol. 2013, 4, 124–128. [Google Scholar] [CrossRef] [PubMed]
- Golan, M.; Schreiber, G.; Avissar, S. Antidepressant-induced differential ubiquitination of beta-arrestins 1 and 2 in mononuclear leucocytes of patients with depression. Int. J. Neuropsychopharmacol. 2013, 16, 1745–1754. [Google Scholar] [CrossRef] [PubMed]
- Cullberg, J. Mood changes and menstrual symptoms with different gestagen/estrogen combinations. A double blind comparison with a placebo. Acta Psychiatr. Scand. Suppl. 1972, 236, 1–86. [Google Scholar] [PubMed]
- Backstrom, T.; Hansson-Malmstrom, Y.; Lindhe, B.A.; Cavalli-Bjorkman, B.; Nordenstrom, S. Oral contraceptives in premenstrual syndrome: A randomized comparison of triphasic and monophasic preparations. Contraception 1992, 46, 253–268. [Google Scholar] [CrossRef]
- Sheehan, D.V.; Lecrubier, Y.; Sheehan, K.H.; Amorim, P.; Janavs, J.; Weiller, E.; Hergueta, T.; Baker, R.; Dunbar, G.C. The Mini-International Neuropsychiatric Interview (M.I.N.I.): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J. Clin. Psychiatry 1998, 59, 22–33. [Google Scholar] [PubMed]
- Hamilton, M. A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Sangi-Haghpeykar, H.; Poindexter, I.I.I.A.N.; Bateman, L.; Ditmore, J.R. Experiences of injectable contraceptive users in an urban setting. Obstet. Gynecol. 1996, 88, 227–233. [Google Scholar] [CrossRef]
- Fraser, I.S.; Dennerstein, G.J. Depo-Provera use in an Australian metropolitan practice. Med. J. Aust. 1994, 160, 553–556. [Google Scholar] [PubMed]
- Dominguez, R.; Hu, E.; Zhou, M.; Baudry, M. 17beta-estradiol-mediated neuroprotection and ERK activation require a pertussis toxin-sensitive mechanism involving GRK2 and beta-arrestin-1. J. Neurosci. 2009, 29, 4228–4238. [Google Scholar] [CrossRef] [PubMed]
- Bethea, C.L.; Lu, N.Z.; Gundlah, C.; Streicher, J.M. Diverse actions of ovarian steroids in the serotonin neural system. Front. Neuroendocrinol. 2002, 23, 41–100. [Google Scholar] [CrossRef] [PubMed]
- Lu, N.Z.; Eshleman, A.J.; Janowsky, A.; Bethea, C.L. Ovarian steroid regulation of serotonin reuptake transporter (SERT) binding, distribution, and function in female macaques. Mol. Psychiatry 2003, 8, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.J.; Henderson, J.A.; Abell, C.W.; Bethea, C.L. Effects of ovarian steroids and raloxifene on proteins that synthesize, transport, and degrade serotonin in the raphe region of macaques. Neuropsychopharmacology 2004, 29, 2035–2045. [Google Scholar] [CrossRef] [PubMed]
- Muller, N.; Schwarz, M.J. The immune-mediated alteration of serotonin and glutamate: Towards an integrated view of depression. Mol. Psychiatry 2007, 12, 988–1000. [Google Scholar] [CrossRef] [PubMed]
- Millan, M.J.; Marin, P.; Bockaert, J.; la Cour, C.M. Signaling at G-protein-coupled serotonin receptors: Recent advances and future research directions. Trends Pharmacol. Sci. 2008, 29, 454–464. [Google Scholar] [CrossRef] [PubMed]
- Nilsen, J.; Brinton, R.D. Divergent impact of progesterone and medroxyprogesterone acetate (Provera) on nuclear mitogen-activated protein kinase signaling. Proc. Natl. Acad. Sci. USA 2003, 100, 10506–10511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simoncini, T.; Mannella, P.; Fornari, L.; Caruso, A.; Willis, M.Y.; Garibaldi, S.; Baldacci, C.; Genazzani, A.R. Differential signal transduction of progesterone and medroxyprogesterone acetate in human endothelial cells. Endocrinology 2004, 145, 5745–5756. [Google Scholar] [CrossRef] [PubMed]
- Bitran, D.; Shiek, M.; McLeod, M. Anxiolytic effect of progesterone is mediated by the neurosteroid allopregnanolone at brain GABAA receptors. J. Neuroendocrinol. 1995, 7, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Gabbay, V.; Mao, X.; Klein, R.G.; Ely, B.A.; Babb, J.S.; Panzer, A.M.; Alonso, C.M.; Shungu, D.C. Anterior cingulate cortex {gamma}-aminobutyric acid in depressed adolescents: Relationship to anhedonia. Arch. Gen. Psychiatry 2012, 69, 139–149. [Google Scholar] [CrossRef] [PubMed]
- Klaiber, E.L.; Broverman, D.M.; Vogel, W.; Peterson, L.G.; Snyder, M.B. Individual differences in changes in mood and platelet monoamine oxidase (MAO) activity during hormonal replacement therapy in menopausal women. Psychoneuroendocrinology 1996, 21, 575–592. [Google Scholar] [CrossRef]
- Sherwin, B.B. Hormones, mood, and cognitive functioning in post-menopausal women. Obstet. Gynecol. 1996, 87, 20S–26S. [Google Scholar] [CrossRef]
- Archer, J.S. NAMS/Solvay Resident Essay Award. Relationship between estrogen, serotonin, and depression. Menopause 1999, 6, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Kruijver, F.P.; Balesar, R.; Espila, A.M.; Unmehopa, U.A.; Swaab, D.F. Estrogen-receptor-beta distribution in the human hypothalamus: Similarities and differences with ER alpha distribution. J. Comp. Neurol. 2003, 466, 251–277. [Google Scholar] [CrossRef] [PubMed]
- Backman, T.; Huhtala, S.; Blom, T.; Luoto, R.; Rauramo, I.; Koskenvuo, M. Length of use and symptoms associated with premature removal of the levonorgestrel intrauterine system: A nation-wide study of 17,360 users. Br. J. Obstet. Gynaecol. 2000, 107, 335–339. [Google Scholar] [CrossRef]
- Pagano, H.P.; Zapata, L.B.; Berry-Bibee, E.N.; Nanda, K.; Curtis, K.M. Safety of hormonal contraception and intrauterine devices among women with depressive and bipolar disorders: A systematic review. Contraception 2016, 94, 641–649. [Google Scholar] [CrossRef] [PubMed]
- Lopez, L.M.; Kaptein, A.A.; Helmerhorst, F.M. Oral contraceptives containing drospirenone for premenstrual syndrome. Cochrane Database Syst. Rev. 2012, CD006586. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Women (n) = 29 | NC (n = 7, 24%) | COC (n = 10, 34%) | POC (n = 12, 41%) |
|---|---|---|---|
| Black | 5 | 8 | 12 |
| White | 2 | 2 | - |
| Age (Average, Range) | 31 (32–38) | 28 (24–36) | 29 (19–38) |
| Weight (Average, Range) | 237 (170–360) | 188 (126–240) | 173 (116–254) |
| NC vs. POC, p = 0.05 * | |||
| NC vs. COC, p = 0.19 | |||
| COC vs. POC, p = 0.75 | |||
| Smoker | 3 | - | 2 |
| Nonsmoker | 4 | 10 | 10 |
| Pregnancies (Average, Range) | 2 (0–5) | 0 (0–1) | 2 (0–5) |
| Children # (Average, Range) | 2 (0–4) | 0 | 2 (0–4) |
| Contraceptives (Name, Number) | Essure® 1 | Orthro Tri-Cyclen® 3 | Mini-Pill (Norethindrone) 2 |
| Paragard® 1 | Necon 1/35® 2 | IUD (Mirena®) 4 | |
| No contraceptive 5 | Junel Fe 1/20® 2 | IUD (Kyleena®) 1 | |
| Generic Yaz 1 | Implant (Nexplanon®) 4 | ||
| Lo Loestrin Fe® 2 | Injection (Depo Provera®) 1 |
| Core Symptoms | NC | COC | POC | NC/COC (p Value) | NC/POC p Value) | COC/POC (p Value) |
|---|---|---|---|---|---|---|
| Depressed mood | 1.0 ± 0.25 | 0.88 ± 0.35 | 2.0 ± 0.37 | >0.99 | 0.12 | 0.07 |
| Work & activities | 0.83 ± 0.4 | 0.44 ± 0.17 | 1.44 ± 0.37 | >0.99 | 0.64 | 0.08 |
| Feelings of guilt | 0.33 ± 0.21 | 0.33 ± 0.23 | 1.2 ± 0.32 | >0.99 | 0.12 | 0.07 |
| Agitation | 0.5 ± 0.34 | 0.5 ± 0.33 | 1.0 ± 0.23 | >0.99 | 0.85 | 0.86 |
| Early insomnia | 0.16 ± 0.16 | 0.44 ± 0.17 | 1.11 ± 0.3 | >0.99 | 0.04 * | 0.15 |
| Middle insomnia | 0.16 ± 0.16 | 0.33 ± 0.16 | 1.2 ± 0.27 | >0.99 | 0.01 * | 0.02 * |
| Late insomnia | 0.16 ± 0.16 | 0.55 ± 0.24 | 0.77 ± 0.22 | 0.78 | 0.25 | >0.99 |
| Psychological anxiety | 0.33 ± 0.21 | 0.44 ± 0.24 | 1.6 ± 0.37 | >0.99 | 0.02 * | 0.01 * |
| Somatic anxiety | 0.66 ± 0.33 | 0.77 ± 0.32 | 2.0 ± 0.4 | >0.99 | 0.07 | 0.06 |
| Somatic symptoms | >0.99 | 0.22 ± 0.14 | 0.77 ± 0.22 | >0.99 | 0.02 * | 0.07 |
| Outcomes | NC | COC | POC |
|---|---|---|---|
| β-AR 1 (Mean ± SEM) | 4.44 ± 0.40 | 3.57 ± 0.76 | 2.87 ± 0.39 |
| NC vs. POC, p = 0.03 * | |||
| NC vs. COC, p = 0.81 | |||
| COC vs. POC, p = 0.052 | |||
| HAM-D (Mean ± SEM) | 6.0 ± 1.3 | 6.4 ± 2.04 | 17.6 ± 2.15 |
| NC vs. POC, p = 0.004 ** | |||
| NC vs. COC, p = 0.42 | |||
| COC vs. POC, p = 0.0004 *** |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smith, K.; Nayyar, S.; Rana, T.; Archibong, A.E.; Looney, K.R.; Nayyar, T. Do Progestin-Only Contraceptives Contribute to the Risk of Developing Depression as Implied by Beta-Arrestin 1 Levels in Leukocytes? A Pilot Study. Int. J. Environ. Res. Public Health 2018, 15, 1966. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15091966
Smith K, Nayyar S, Rana T, Archibong AE, Looney KR, Nayyar T. Do Progestin-Only Contraceptives Contribute to the Risk of Developing Depression as Implied by Beta-Arrestin 1 Levels in Leukocytes? A Pilot Study. International Journal of Environmental Research and Public Health. 2018; 15(9):1966. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15091966
Chicago/Turabian StyleSmith, Keisha, Sanket Nayyar, Tanu Rana, Anthony E. Archibong, Kimberly R. Looney, and Tultul Nayyar. 2018. "Do Progestin-Only Contraceptives Contribute to the Risk of Developing Depression as Implied by Beta-Arrestin 1 Levels in Leukocytes? A Pilot Study" International Journal of Environmental Research and Public Health 15, no. 9: 1966. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15091966