Innovating New Rural Cooperative Medical Scheme (NCMS) for Better Patient Satisfaction in Rural China

Abstract
:1. Introduction
2. Literature Review
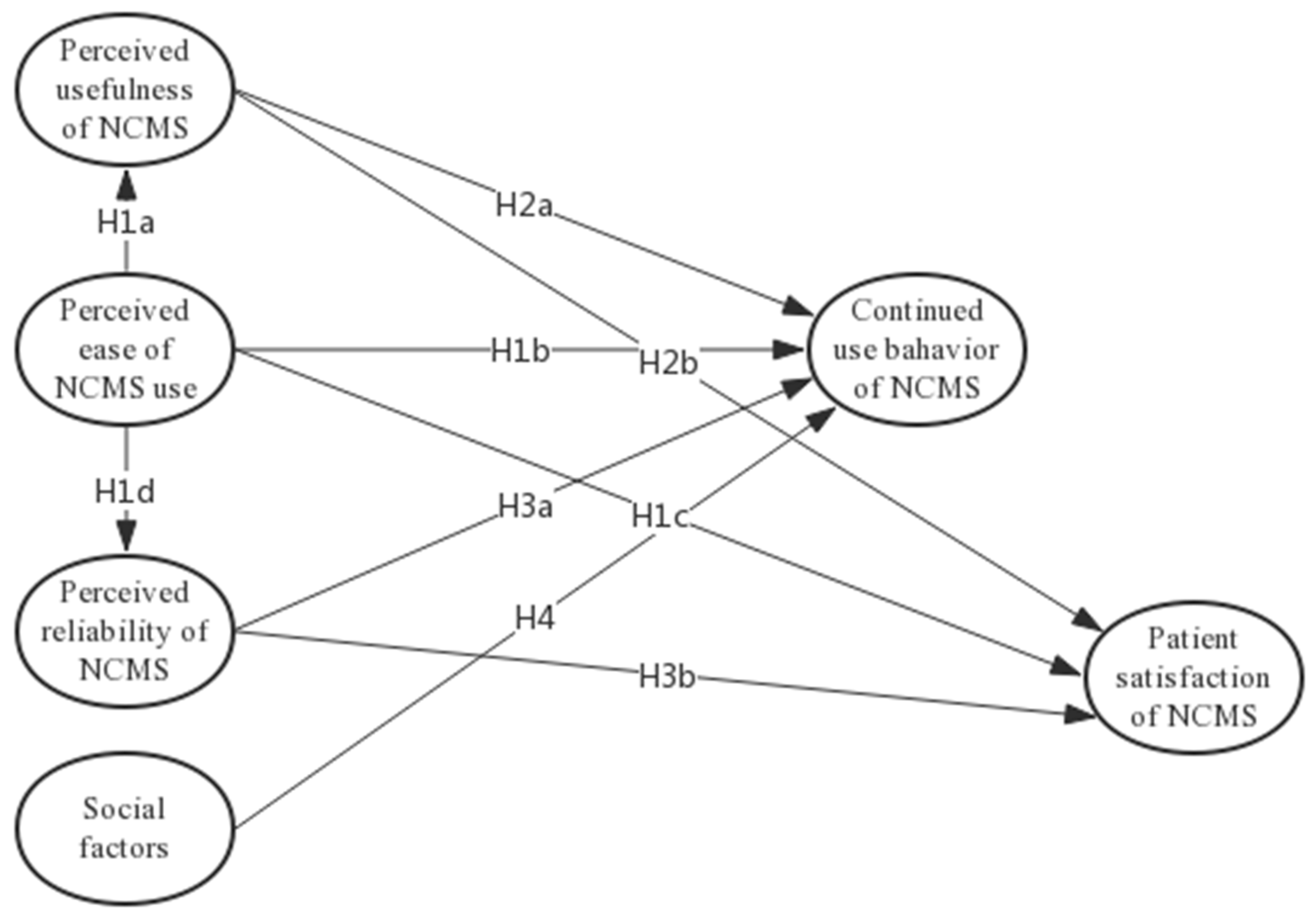
3. Model and Hypotheses Development
3.1. PU, PE and CUB, PS
3.2. PR and CUB, PS
3.3. SF and CUB, PS
4. Methodology
4.1. Measures
4.2. Data Collection
5. Results
5.1. Measurement Model
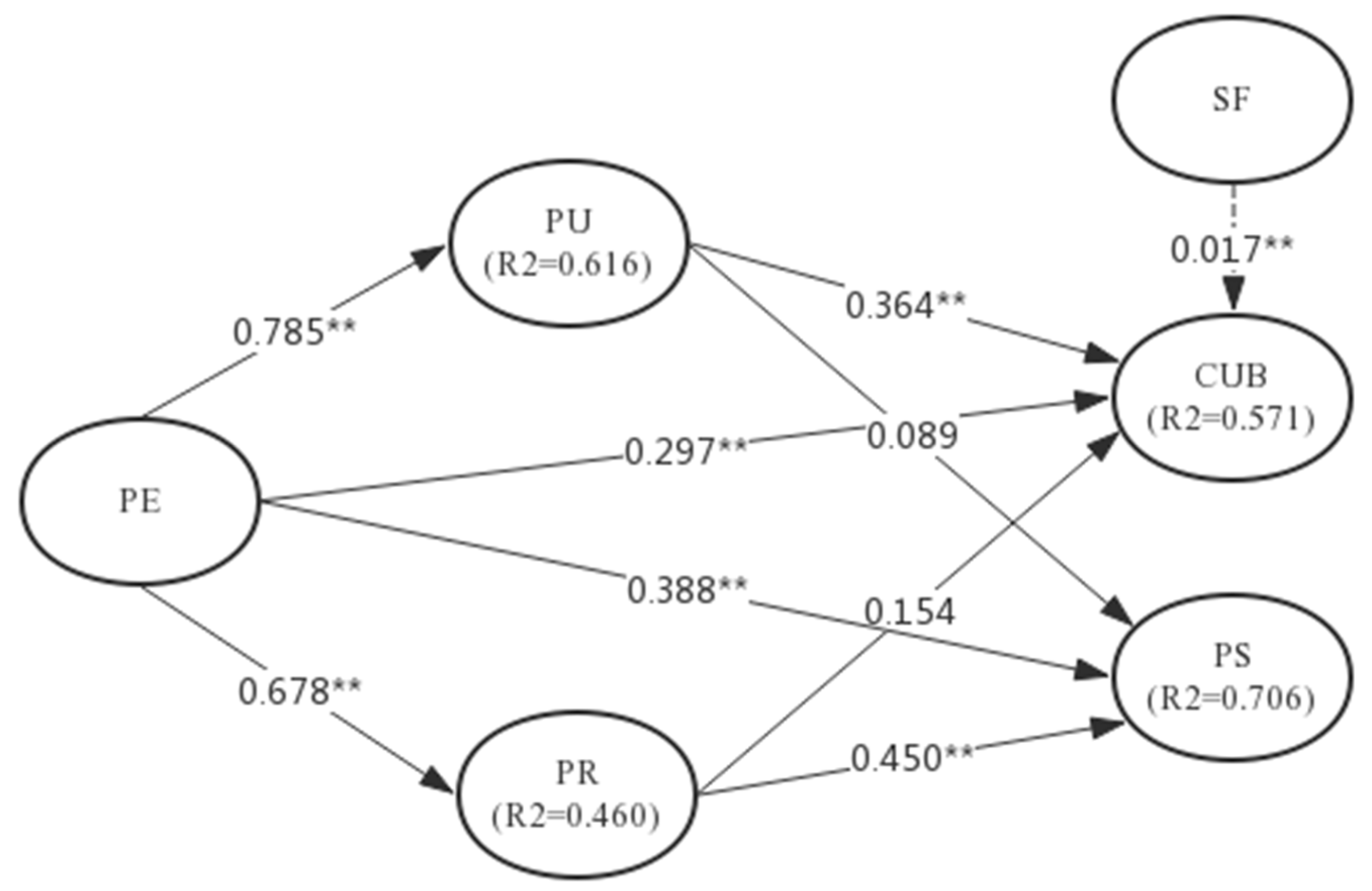
5.2. Structural Model
6. Discussions
7. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Construct | Item Statistics | |||
|---|---|---|---|---|
| Construct Items | Mean | Std. Deviation | Loading 1 | |
| Perceived Usefulness of NCMS(PU) | PU01 | 6.11 | 1.102 | 0.8301 |
| PU02 | 6.03 | 1.128 | 0.8182 | |
| PU03 | 5.92 | 1.169 | 0.8220 | |
| PU04 | 5.85 | 1.195 | 0.7553 | |
| Perceived Ease of NCMS Use(PE) | PE01 | 5.73 | 1.285 | 0.8143 |
| PE02 | 5.76 | 1.221 | 0.7841 | |
| PE03 | 5.88 | 1.194 | 0.8425 | |
| PE04 | 5.66 | 1.287 | 0.8053 | |
| Perceived Reliability of NCMS(PR) | PR01 | 5.62 | 1.366 | 0.7938 |
| PR02 | 5.39 | 1.461 | 0.7496 | |
| PR03 | 5.47 | 1.301 | 0.8057 | |
| PR04 | 5.70 | 1.194 | 0.8504 | |
| PR05 | 5.91 | 1.179 | 0.8565 | |
| Social Factors(SF) | SF01 | 5.55 | 1.377 | 0.7575 |
| SF02 | 5.64 | 1.422 | 0.7845 | |
| SF03 | 5.53 | 1.449 | 0.8496 | |
| SF04 | 5.64 | 1.323 | 0.8355 | |
| Continued use of NCMS(CUB) | BI01 | 5.69 | 1.224 | 0.9084 |
| BI02 | 5.60 | 1.343 | 0.8421 | |
| BI03 | 5.70 | 1.273 | 0.9539 | |
| Patient Satisfaction with NCMS(PS) | PS01 | 5.82 | 1.199 | 0.7538 |
| PS02 | 6.04 | 1.101 | 0.8069 | |
| PS03 | 5.89 | 1.186 | 0.8349 | |
| PS04 | 6.08 | 1.076 | 0.8464 | |
| PS05 | 5.72 | 1.225 | 0.8127 | |
References
- Liang, Y.; Lu, P. Medical insurance policy organized by Chinese government and the health inequity of the elderly: Longitudinal comparison based on effect of New Cooperative Medical Scheme on health of rural elderly in 22 provinces and cities. Int. J. Equity Health 2014, 13, 37. [Google Scholar] [CrossRef] [PubMed]
- Dong, H.; Duan, S.; Bogg, L.; Wu, Y.; You, H.; Chen, J.; Ye, X.; Seccombe, K.; Yu, H. The impact of expanded health system reform on governmental contributions and individual copayments in the new Chinese rural cooperative medical system. Int. J. Health Plan. Manag. 2016, 31, 36–48. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Hou, Y.; Sun, M.; Lu, J.; Wang, Y.; Li, X.; Chang, F.; Hao, M. An evaluation of China’s new rural cooperative medical system: Achievements and inadequacies from policy goals. BMC Public Health 2015, 15, 1079. [Google Scholar] [CrossRef] [PubMed]
- Filipski, M.J.; Zhang, Y.; Chen, K.Z. Making health insurance pro-poor: Evidence from a household panel in rural China. BMC Health Serv. Res. 2015, 15, 210. [Google Scholar] [CrossRef] [PubMed]
- Ying, Y.; Pan, W.; Zhang, Z. Increasing insurance protection efforts and improving the fairness of health care services: A-nalysis on the convergence mechanism between New Rural Cooperative Medical Scheme and Healthcare Financial Assistance Program. Chin. J. Health Policy 2015, 8, 3–8. [Google Scholar] [CrossRef]
- Babiarz, K.S.; Miller, G.; Yi, H.; Zhang, L.; Rozelle, S. New evidence on the impact of China’s New Rural Cooperative Medical Scheme and its implications for rural primary healthcare: Multivariate difference-in-difference analysis. BMJ 2010, 341, c5617. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Jackson, S.; Carmichael, G.A.; Sleigh, A.C. Prescribing behaviour of village doctors under China’s New Cooperative Medical Scheme. Soc. Sci. Med. 2009, 68, 1775–1779. [Google Scholar] [CrossRef] [PubMed]
- Yip, W.; Hsiao, W.C. Non-evidence-based policy: How effective is China’s new cooperative medical scheme in reducing medical impoverishment? Soc. Sci. Med. 2009, 68, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Xu, J.; Zhang, Z.; Wang, J. New cooperative medical scheme decreased financial burden but expanded the gap of income-related inequity: Evidence from three provinces in rural China. Int. J. Equity Health 2016, 15, 72. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.; Cen, Y. Public Health Insurance System Reform and Its Impact on Health Service Utilization in Rural China: Evidence from CHNS 2000 and 2011. Chin. Stud. 2017, 6, 85. [Google Scholar] [CrossRef]
- You, X.; Kobayashi, Y. The new cooperative medical scheme in China. Health Policy 2009, 91, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Lei, X.; Lin, W. The new cooperative medical scheme in rural China: Does more coverage mean more service and better health? Health Econ. 2009, 18, S25–S46. [Google Scholar] [CrossRef] [PubMed]
- Linder-Pelz, S. Toward a theory of patient satisfaction. Soc. Sci. Med. 1982, 16, 577–582. [Google Scholar] [CrossRef]
- Li, J.G.; Yang, Z.; Meng, F. A Summary of patient satisfaction research and assessment tools. Mod. Hosp. Manag. 2010, 6, 4–7. [Google Scholar]
- Schoenfelder, T.; Klewer, J.; Kugler, J. Factors associated with patient satisfaction in surgery: The role of patients’ perceptions of received care, visit characteristics, and demographic variables. J. Surg. Res. 2010, 164, e53–e59. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Gu, D.; Dupre, M.E. Factors associated with enrollment, satisfaction, and sustainability of the New Cooperative Medical Scheme program in six study areas in rural Beijing. Health Policy 2008, 85, 32–44. [Google Scholar] [CrossRef] [PubMed]
- Tasso, K.; Behar-Horenstein, L.S.; Aumiller, A.; Gamble, K.; Grimaudo, N.; Guin, P.; Ramey, B. Assessing patient satisfaction and quality of care through observation and interview. Hosp. Top. 2002, 80, 4–10. [Google Scholar] [CrossRef] [PubMed]
- McEachan, R.; Taylor, N.; Harrison, R.; Lawton, R.; Gardner, P.; Conner, M. Meta-analysis of the reasoned action approach (RAA) to understanding health behaviors. Ann. Behav. Med. 2016, 50, 592–612. [Google Scholar] [CrossRef] [PubMed]
- Kalolo, A.; Kibusi, S.M. The influence of perceived behaviour control, attitude and empowerment on reported condom use and intention to use condoms among adolescents in rural Tanzania. Reprod. Health 2015, 12, 105. [Google Scholar] [CrossRef] [PubMed]
- Davis, F.D. Perceived usefulness, perceived ease of use, and user acceptance of information technology. MIS Q. 1989, 319–340. [Google Scholar] [CrossRef]
- Fishbein, M.; Ajzen, I. Belief, attitude, intention and behaviour: An introduction to theory and research. Philos. Rhetor. 1975, 41, 842–844. [Google Scholar]
- Davis, F.D. User acceptance of information technology: System characteristics, user perceptions and behavioral imparts. Int. J. Man-Mach. Stud. 1993, 38, 475–487. [Google Scholar] [CrossRef]
- Segars, A.H.; Grover, V. Re-examining perceived ease of use and usefulness: A confirmatory factor analysis. MIS Q. 1993, 517–525. [Google Scholar] [CrossRef]
- Agarwal, R.; Karahanna, E. Time flies when you’re having fun: Cognitive absorption and beliefs about information technology usage. MIS Q. 2000, 665–694. [Google Scholar] [CrossRef]
- Deng, Z.; Mo, X.; Liu, S. Comparison of the middle-aged and older users’ adoption of mobile health services in China. Int. J. Med. Inform. 2014, 83, 210–224. [Google Scholar] [CrossRef] [PubMed]
- Mackert, M.; Mabry-Flynn, A.; Champlin, S.; Donovan, E.E.; Pounders, K. Health literacy and health information technology adoption: The potential for a new digital divide. J. Med. Internet Res. 2016, 18, e264. [Google Scholar] [CrossRef] [PubMed]
- Buimer, H.P.; Tabak, M.; Van Velsen, L.; Van Der Geest, T.; Hermens, H. Exploring Determinants of Patient Adherence to a Portal-Supported Oncology Rehabilitation Program: Interview and Data Log Analyses. JMIR Rehabilit. Assist. Technol. 2017, 4, e12. [Google Scholar] [CrossRef] [PubMed]
- Davis, F.D.; Bagozzi, R.P.; Warshaw, P.R. User acceptance of computer technology: A comparison of two theoretical models. Manag. Sci. 1989, 35, 982–1003. [Google Scholar] [CrossRef]
- Gulati, R.; Galino, J. Get the right mix of bricks and clicks. Harv. Bus. Rev. 2000, 78, 107–114. [Google Scholar] [PubMed]
- Pan, B.; Yuan, Z.; Zou, J.; Cook, D.M.; Yang, W. Elderly hospitalization and the New-type Rural Cooperative Medical Scheme (NCMS) in China: Multi-stage cross-sectional surveys of Jiangxi province. BMC Health Serv. Res. 2016, 16, 436. [Google Scholar] [CrossRef] [PubMed]
- Yan, Z.; Wan, D.; Li, L. Patient satisfaction in two Chinese provinces: Rural and urban differences. Int. J. Qual. Health Care 2011, 23, 384–389. [Google Scholar] [CrossRef] [PubMed]
- Bauer, R.A. Consumer behavior as risk taking. In Proceedings of the 43rd National Conference of the American Marketing Assocation, Chicago, IL, USA, 15–17 June 1960. [Google Scholar]
- Malhotra, N.K.; Kim, S.S.; Agarwal, J. Internet users’ information privacy concerns (IUIPC): The construct, the scale, and a causal model. Inf. Syst. Res. 2004, 15, 336–355. [Google Scholar] [CrossRef]
- Van der Heijden, H.; Verhagen, T.; Creemers, M. Understanding online purchase intentions: Contributions from technology and trust perspectives. Eur. J. Inf. Syst. 2003, 12, 41–48. [Google Scholar] [CrossRef]
- Green, D.T.; Pearson, J.M. Integrating website usability with the electronic commerce acceptance model. Behav. Inf. Technol. 2011, 30, 181–199. [Google Scholar] [CrossRef]
- Gefen, D.; Karahanna, E.; Straub, D.W. Trust and TAM in online shopping: An integrated model. MIS Q. 2003, 27, 51–90. [Google Scholar] [CrossRef]
- Oster, E.; Thornton, R. Determinants of technology adoption: Peer effects in menstrual cup take-up. J. Eur. Econ. Assoc. 2012, 10, 1263–1293. [Google Scholar] [CrossRef]
- Venkatesh, V.; Morris, M.G.; Davis, G.B.; Davis, F.D. User acceptance of information technology: Toward a unified view. MIS Q. 2003, 425–478. [Google Scholar] [CrossRef]
- Razee, H.; Whittaker, M.; Jayasuriya, R.; Yap, L.; Brentnall, L. Listening to the rural health workers in Papua New Guinea–the social factors that influence their motivation to work. Soc. Sci. Med. 2012, 75, 828–835. [Google Scholar] [CrossRef] [PubMed]
- Yoon, C. The Effects of National Culture Values on Consumer Acceptance of E-Commerce: Online Shoppers in China. Inf. Manag. 2009, 46, 294–301. [Google Scholar] [CrossRef]
- Limayem, M.; Hirt, S.G. Force of Habit and Information Systems Usage: Theory and Initial Validation. J. Assoc. Inf. Syst. 2003, 4, 65–97. [Google Scholar] [CrossRef] [Green Version]
- Gu, D.X.; Li, P.P.; Yang, X.J. Investigating Users’ No-Show Behavior during using Hospital Online Appointment Registration System. J. Inf. Sci, 2017, 6, 99–106. [Google Scholar]
- Song, J.; Zahedi, F.M. Internet market strategies: Antecedents and implications. Inf. Manag. 2006, 43, 222–238. [Google Scholar] [CrossRef]
- Dinev, T.; Hart, P. An Extended Privacy Calculus Model for E-Commerce Transactions. Inf. Syst. Res. 2006, 17, 61–80. [Google Scholar] [CrossRef]
- Bansal, G.; Gefen, D. The impact of personal dispositions on information sensitivity, privacy concern and trust in disclosing health information online. Decis. Support Syst. 2010, 49, 138–150. [Google Scholar] [CrossRef]
- Sun, J.; Sheng, D.; Gu, D.; Du, J.T.; Min, C. Understanding link sharing tools continuance behavior in social media. Online Inf. Rev. 2017, 41, 119–133. [Google Scholar] [CrossRef]
- Liang, C.; Gu, D.X.; Tao, F.J.; Jain, H.K.; Zhao, Y.; Ding, B. Influence of mechanism of patient-accessible hospital information system implementation on doctor–patient relationships: A service fairness perspective. Inf. Manag. 2017, 54, 57–72. [Google Scholar] [CrossRef]
- Hair, J.F.; Anderson, R.E.; Tatham, R.L.; Black, W.C. Multivariate Data Analysis, 5th ed.; Prentice Hall: Upper Saddle River, NJ, USA; New York, NY, USA, 1998; pp. 125–136. [Google Scholar]
- Sanders, N.R.; Premus, R. Modeling the relationship between firm IT capability, collaboration, and performance. J. Bus. Logist. 2005, 26, 1–23. [Google Scholar] [CrossRef]
- Nunnally, J.C.; Bernstein, I.H. Psychometric Theory, 2nd ed.; McGraw-Hill: New York, NY, USA, 1978. [Google Scholar]
- Bagozzi, R.P. Causal Models in Marketing; John Wiley & Sons: New York, NY, USA, 1980; pp. 126–128. [Google Scholar]
- Nunnally, J.C.; Bernstein, I.H. Psychological Theory, 3rd ed.; McGraw-Hill: New York, NY, USA, 1994. [Google Scholar]
- Fornell, C.; Larcker, D.F. Evaluating structural equation models with unobservable variables and measurement error. J. Mark. Res. 1981, 18, 39–50. [Google Scholar] [CrossRef]
- Tung, F.C.; Chang, S.C.; Chou, C.M. An extension of trust and TAM model with IDT in the adoption of the electronic logistics information system in HIS in the medical industry. Int. J. Med. Inform. 2008, 77, 324–335. [Google Scholar] [CrossRef] [PubMed]
- Deng, S.L.; Guan, X. Research on Influencing Factors of Users’ Health Information Acquisition Willingness Based on Question and Answer Platform. J. Inf. Sci. 2016, 34, 53–59. [Google Scholar]


| Measures of Variables | Reference | |
|---|---|---|
| Perceived Usefulness | As a rural household, NCMS is useful to protect me from the financial risk posed by health care costs. NCMS makes me not worry much about a big medical bill during seeking medical service and can save me much money. NCMS enables me to get medical care timelier. NCMS can save me money in medical care. | [40] |
| Perceived Ease of Use | It is easy to participate in NCMS. Learning to using NCMS is easy. My interaction with NCMS is clear and understandable. The procedure of NCMS is very simple. | |
| Social Factors | My relatives think it is important to participate in NCMS. My friends around me think it is important to participate in NCMS. My family members think it is important to participate in NCMS. My neighbours think it is important to participate in NCMS. | [41] |
| Perceived Reliability | I believe that NCMS is dependable and trustworthy. I believe that NCMS provides good service The level of my trust for NCMS is very high. I trust the NCMS administrators to keep my personal information safe and will not share or sold it to companies for business purpose. I trust the NCMS administrators will not misuse my personal information. | [42,43,44,45] |
| Continued use behaviour | I was participated in NCMS in the past 12 months. I recommended NCMS to my friends or other people to whom I am familiar. When I seek medical care, I used NCMS. I continued to use NCMS for medical risk protection. | [46] |
| Patient satisfaction | I am satisfied for that NCMS increase my use of health care services. I feel the NCMS is more consistent with my expectation With NCMS, I feel I am more satisfied with the healthcare in the hospital. NCMS is generally beneficial for the improvement of the quality of care, and I like it. With NCMS, I feel the out-of-pocket spending on medical care are more reasonable. | [47] |
| Item | Category | N | % |
|---|---|---|---|
| Sex | Male | 229 | 47.41 |
| Female | 254 | 52.59 | |
| Age | 18–28 years old | 104 | 21.53 |
| 28–48 years old | 164 | 33.95 | |
| 48–60 years old | 97 | 20.09 | |
| >60 years old | 118 | 24.43 | |
| Education background | Primary school | 68 | 14.08 |
| Middle school | 277 | 57.35 | |
| High school | 124 | 25.67 | |
| College or other | 14 | 2.90 |
| Construct | C.A. | C.R. | AVE | CUB | PE | PR | PS | PU | SF |
|---|---|---|---|---|---|---|---|---|---|
| CUB | 0.8847 | 0.9293 | 0.8146 | 0.9025 | |||||
| PE | 0.8279 | 0.8854 | 0.6591 | 0.7124 | 0.8118 | ||||
| PR | 0.8703 | 0.9062 | 0.6596 | 0.6156 | 0.6782 | 0.8121 | |||
| PS | 0.8701 | 0.9059 | 0.6585 | 0.6254 | 0.6984 | 0.7736 | 0.8115 | ||
| PU | 0.8211 | 0.8818 | 0.6513 | 0.6980 | 0.7846 | 0.6787 | 0.7631 | 0.8070 | |
| SF | 0.8214 | 0.8822 | 0.6523 | 0.5673 | 0.6479 | 0.7873 | 0.7371 | 0.6519 | 0.8076 |
| Hypothesized Path | Standardized Path Coefficients | t-Value | p-Value | Results |
|---|---|---|---|---|
| H1a: PE → PU | 0.785 | 30.929 | p < 0.01 | Supported |
| H1b: PE → CUB | 0.364 | 6.081 | p < 0.01 | Supported |
| H1c: PE → PS | 0.089 | 1.790 | p < 0.01 | Supported |
| H1d: PE → PR | 0.678 | 21.440 | p < 0.01 | Supported |
| H2a: PU → CUB | 0.297 | 5.508 | p < 0.01 | Supported |
| H2b: PU → PS | 0.388 | 7.436 | p < 0.01 | Supported |
| H3a: PR → CUB | 0.154 | 2.400 | p < 0.05 | Supported |
| H3b: PR → PS | 0.450 | 9.517 | p < 0.01 | Supported |
| H4: SF → CUB | 0.017 | 0.287 | Not significant | Unsupported |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gu, D.; Yang, X.; Li, X.; Liang, C.; Zhong, J.; Feng, N. Innovating New Rural Cooperative Medical Scheme (NCMS) for Better Patient Satisfaction in Rural China. Int. J. Environ. Res. Public Health 2018, 15, 2007. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15092007
Gu D, Yang X, Li X, Liang C, Zhong J, Feng N. Innovating New Rural Cooperative Medical Scheme (NCMS) for Better Patient Satisfaction in Rural China. International Journal of Environmental Research and Public Health. 2018; 15(9):2007. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15092007
Chicago/Turabian StyleGu, Dongxiao, Xuejie Yang, Xingguo Li, Changyong Liang, Jinhong Zhong, and Nanping Feng. 2018. "Innovating New Rural Cooperative Medical Scheme (NCMS) for Better Patient Satisfaction in Rural China" International Journal of Environmental Research and Public Health 15, no. 9: 2007. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15092007