The Quality of Tuberculosis Care in Urban Migrant Clinics in China

 ,
, 
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
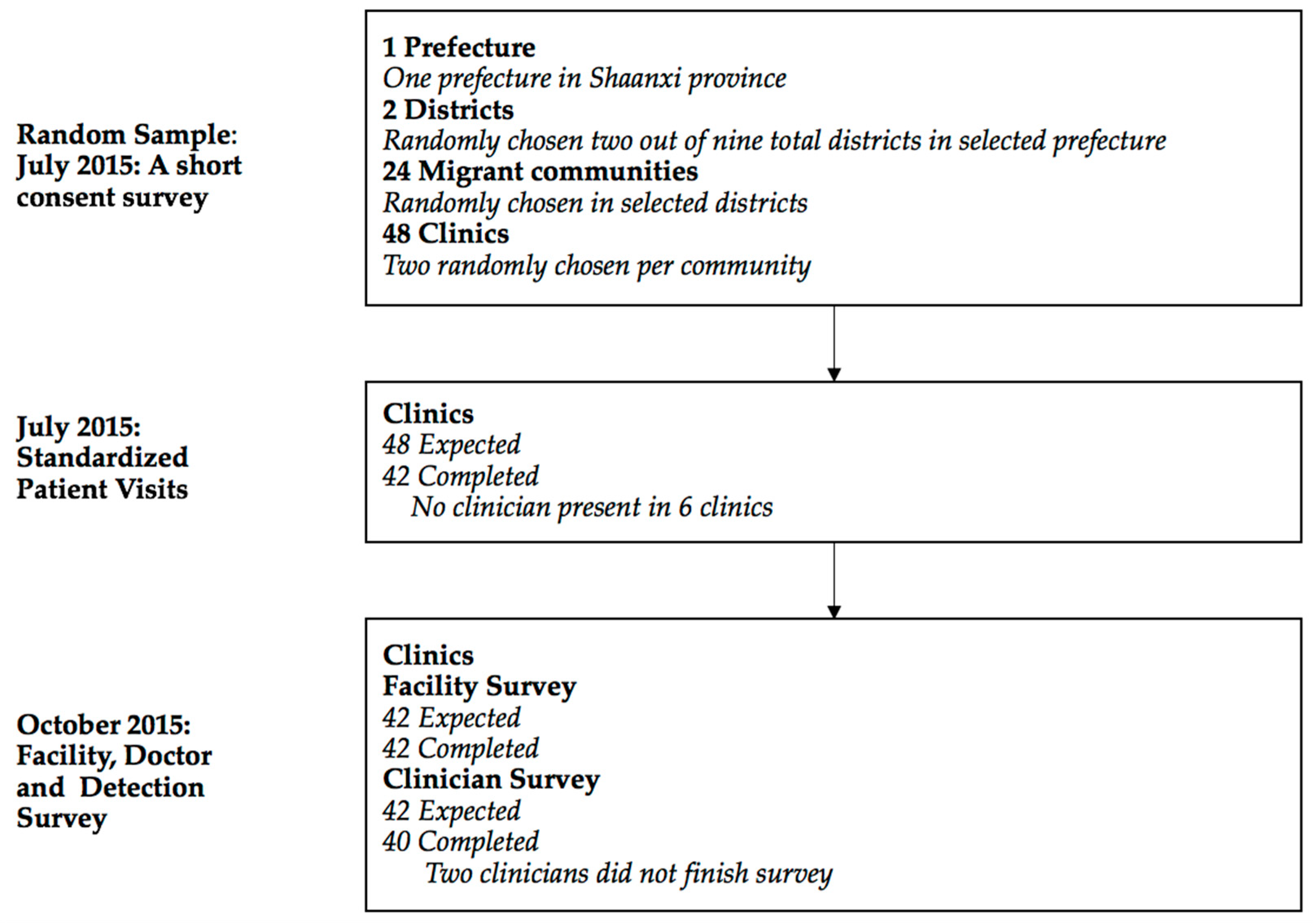
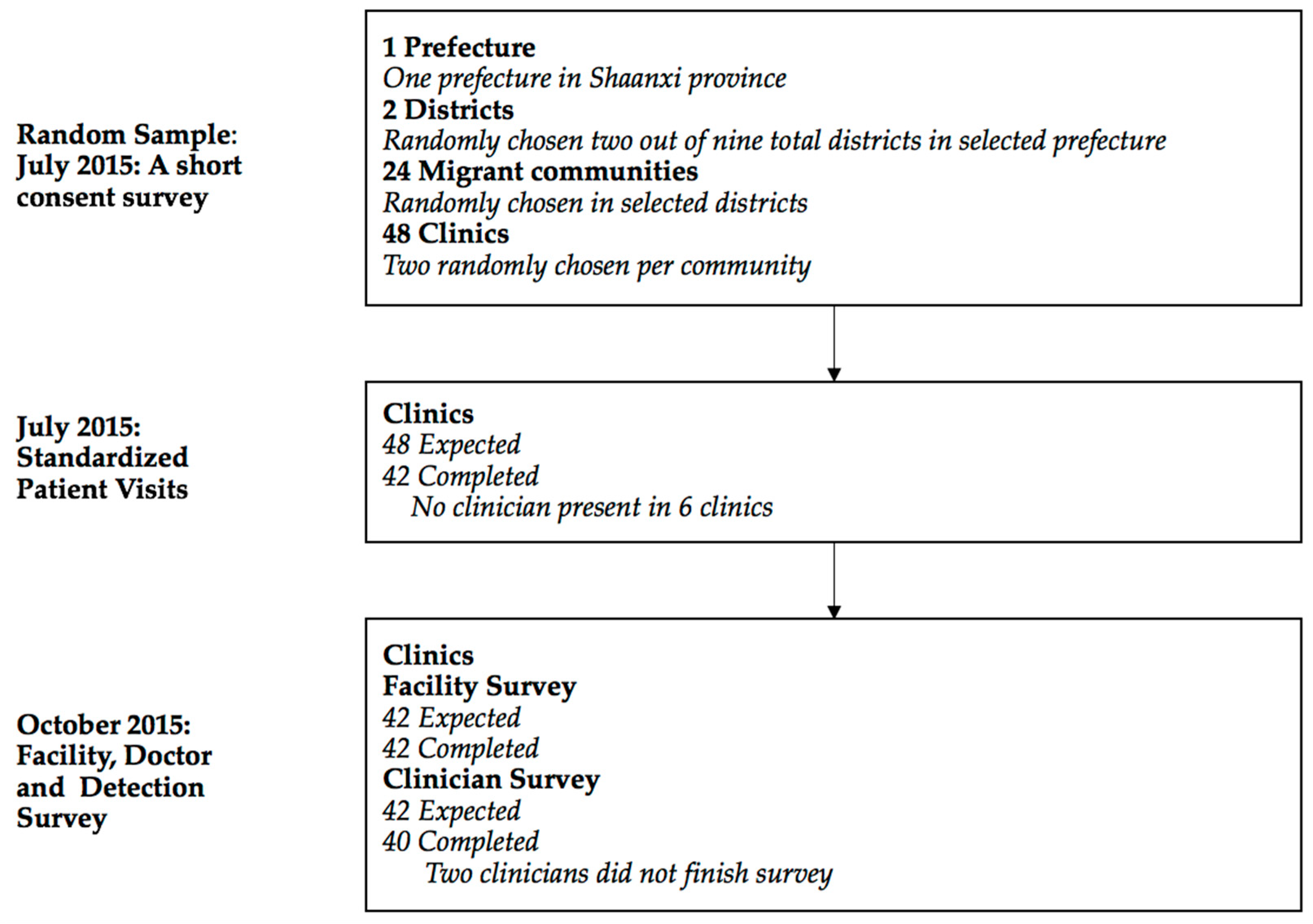
2.1. Selection of Facilities, Data Collection, and Study Size
2.2. Standardized Patients
2.3. Outcomes
2.4. Statistical Analysis
3. Results
3.1. Primary Description of Facilities
3.2. Case Management of SPs
3.3. Correlations Between the Quality of Tb Care and Clinic Characteristics
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Total | Local Clinics | Migrant Clinics | |
|---|---|---|---|
| Questions | |||
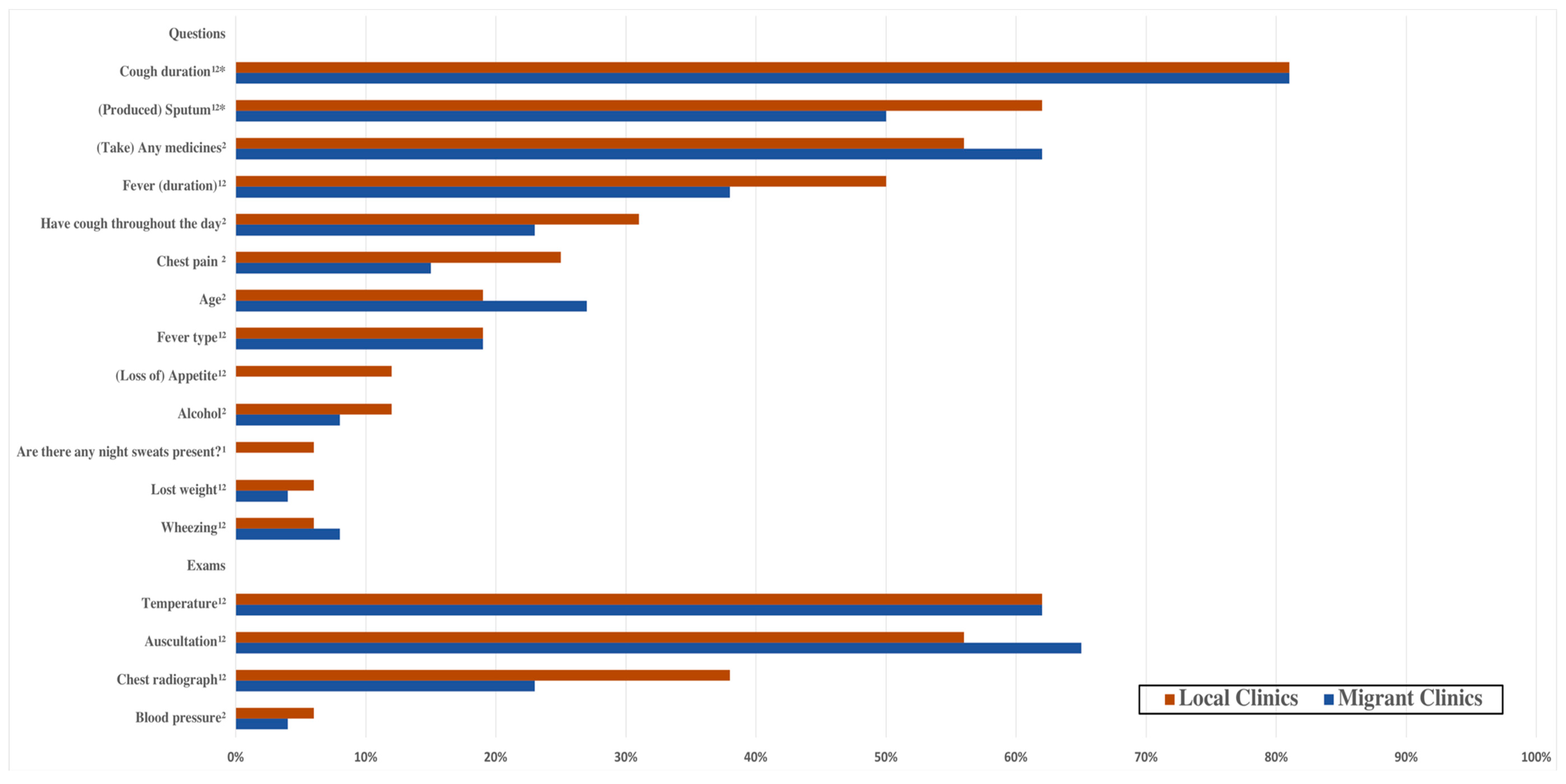
| Cough duration 1,2,* | 0.81 (0.40) | 0.81 (0.40) | 0.81 (0.40) |
| (Produced) Sputum 1,2,* | 0.55 (0.50) | 0.62 (0.50) | 0.50 (0.51) |
| Past tuberculosis 2,* | 0.00 (0.00) | 0.00 (0.00) | 0.00 (0.00) |
| Family tuberculosis 2,* | 0.00 (0.00) | 0.00 (0.00) | 0.00 (0.00) |
| Blood in sputum 1,2 | 0.02 (0.15) | 0.00 (0.00) | 0.04 (0.20) |
| Fever (duration) 1,2 | 0.43 (0.50) | 0.50 (0.52) | 0.38 (0.50) |
| Fever type 1,2 | 0.19 (0.40) | 0.19 (0.40) | 0.19 (0.40) |
| Chest pain 2 | 0.19 (0.40) | 0.25 (0.45) | 0.15 (0.37) |
| (Loss of) Appetite 1,2 | 0.05 (0.22) | 0.12 (0.34) | 0.00 (0.00) |
| Lost weight 1,2 | 0.05 (0.22) | 0.06 (0.25) | 0.04 (0.20) |
| Breathing difficulty 1,2 | 0.05 (0.22) | 0.00 (0.00) | 0.08 (0.27) |
| Wheezing 1,2 | 0.07 (0.26) | 0.06 (0.25) | 0.08 (0.27) |
| (Take) Any medicines 2 | 0.60 (0.50) | 0.56 (0.51) | 0.62 (0.50) |
| Smoking 2 | 0.10 (0.30) | 0.00 (0.00) | 0.15 (0.37) |
| Diabetes 2 | 0.00 (0.00) | 0.00 (0.00) | 0.00 (0.00) |
| High blood pressure or hypertension 2 | 0.00 (0.00) | 0.00 (0.00) | 0.00 (0.00) |
| HIV/AIDS 2 | 0.00 (0.00) | 0.00 (0.00) | 0.00 (0.00) |
| Alcohol 2 | 0.10 (0.30) | 0.12 (0.34) | 0.08 (0.27) |
| Age 2 | 0.24 (0.43) | 0.19 (0.40) | 0.27 (0.45) |
| Family symptoms 2 | 0.00 (0.00) | 0.00 (0.00) | 0.00 (0.00) |
| Have cough throughout the day 2 | 0.26 (0.45) | 0.31 (0.48) | 0.23 (0.43) |
| Weakness 1 | 0.02 (0.15) | 0.00 (0.00) | 0.04 (0.20) |
| Are there any night sweats present? 1 | 0.02 (0.15) | 0.06 (0.25) | 0.00 (0.00) |
| Exams | |||
| Weight 1,2 | 0.00 (0.00) | 0.00 (0.00) | 0.00 (0.00) |
| Pulse 2 | 0.10 (0.30) | 0.06 (0.25) | 0.12 (0.33) |
| Blood pressure 2 | 0.05 (0.22) | 0.06 (0.25) | 0.04 (0.20) |
| Temperature 1,2 | 0.62 (0.49) | 0.62 (0.50) | 0.62 (0.50) |
| Auscultation 1,2 | 0.62 (0.49) | 0.56 (0.51) | 0.65 (0.49) |
| Chest radiograph 1,2 | 0.29 (0.46) | 0.38 (0.50) | 0.23 (0.43) |
| Sputum smear test (Sputum AFB) 1,2 | 0.02 (0.15) | 0.00 (0.00) | 0.04 (0.20) |
| HIV test 2 | 0.00 (0.00) | 0.00 (0.00) | 0.00 (0.00) |
| Diabetes test 2 | 0.00 (0.00) | 0.00 (0.00) | 0.00 (0.00) |
| Mantoux Tuberculin Skin Test (TST) 1,2 | 0.00 (0.00) | 0.00 (0.00) | 0.00 (0.00) |
| Sputum culture test 1 | 0.00 (0.00) | 0.00 (0.00) | 0.00 (0.00) |
References
- Wang, L.; Zhang, H.; Ruan, Y.; Chin, D.P.; Xia, Y.; Cheng, S.; Chen, M.; Zhao, Y.; Jiang, S.; Du, X.; et al. Tuberculosis prevalence in China, 1990–2010: A longitudinal analysis of national survey data. Lancet 2014, 383, 2057–2064. [Google Scholar] [CrossRef]
- Liu, G.G.; Vortherms, S.A.; Hong, X.Z. China’s Health Reform Update. Annu. Rev. Public Health 2017, 38, 431–448. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global Tuberculosis Report 2017. Available online: http://www.who.int/tb/publications/global_report/en/ (accessed on 14 September 2018).
- WHO. Global Strategy and Targets for Tuberculosis Prevention, Care and Control After 2015. Available online: http://www.who.int/tb/post2015_strategy/en/ (accessed on 14 September 2018).
- The National Health and Family Planning Commission of the Floating Population Family Planning Service Management: China Floating Population Development Report 2016. Available online: http://www.nhfpc.gov.cn/ldrks/s7847/201610/d17304b7b9024be38facb5524da48e78.shtml (accessed on 14 September 2018).
- Yang, C.; Lu, L.; Warren, J.L.; Wu, J.; Jiang, J.; Zuo, T.; Gan, M.; Liu, M.; Liu, Q.; DeRiemer, K.; et al. Internal migration and transmission dynamics of tuberculosis in Shanghai, China: An epidemiological, spatial, genomic analysis. Lancet Infect. Dis. 2018, 18, 788–795. [Google Scholar] [CrossRef]
- Li, X.; Yang, Q.; Feng, B.; Xin, H.; Zhang, M.; Deng, Q.; Deng, G.; Shan, W.; Yue, J.; Zhang, H.; et al. Tuberculosis infection in rural labor migrants in Shenzhen, China: Emerging challenge to tuberculosis control during urbanization. Sci. Rep. 2017, 7, 4457. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.; Cook, S.; Salazar, M.A. Internal migration and health in China. Lancet 2008, 372, 1717–1719. [Google Scholar] [CrossRef]
- Jia, Z.W.; Jia, X.W.; Liu, Y.X.; Dye, D.; Chen, F.; Chen, C.S.; Zhang, W.Y.; Li, X.W.; Cao, W.C.; Liu, H.L. Spatial analysis of tuberculosis cases in migrants and permanent residents, Beijing, 2000–2006. Emerg. Infect. Dis. 2008, 14, 1413–1419. [Google Scholar] [CrossRef] [PubMed]
- Peng, X. China’s demographic history and future challenges. Science 2011, 333, 581–587. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Jiang, Q.; Abdullah, A.S.; Xu, B. Barriers in accessing to tuberculosis care among non-residents in Shanghai: A descriptive study of delays in diagnosis. Eur. J. Public Health 2007, 17, 419–423. [Google Scholar] [CrossRef] [PubMed]
- Zhou, C.; Tobe, R.G.; Chu, J.; Gen, H.; Wang, X.; Xu, L. Detection delay of pulmonary tuberculosis patients among migrants in China: A cross-sectional study. Int. J. Tuberc. Lung Dis. 2012, 16, 1630–1636. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.; Zhao, M.; Wang, Y.; Gong, Y.; Yin, X.; Zhao, A.; Zheng, J.; Liu, Z.; Jian, X.; Wang, W.; et al. Non-adherence to anti-tuberculosis treatment among internal migrants with pulmonary tuberculosis in Shenzhen, China: A cross-sectional study. BMC Public Health 2015, 15, 474. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Ehiri, J.; Tang, S.; Li, D.; Bian, Y.; Lin, H.; Marshall, C.; Cao, J. Factors associated with patient, and diagnostic delays in Chinese TB patients: A systematic review and meta-analysis. BMC Med. 2013, 11, 156. [Google Scholar] [CrossRef] [PubMed]
- Mou, J.; Griffiths, S.M.; Fong, H.; Dawes, M.G. Health of China’s rural-urban migrants and their families: A review of literature from 2000 to 2012. Br. Med. Bull. 2013, 106, 19–43. [Google Scholar] [CrossRef] [PubMed]
- WHO. The World Health Report 2008—Primary Health Care (Now More Than Ever). Available online: http://www.who.int/whr/2008/en/ (accessed on 14 September 2018).
- Hu, R.; Liao, Y.; Du, Z.; Hao, Y.; Liang, H.; Shi, L. Types of health care facilities and the quality of primary care: A study of characteristics and experiences of Chinese patients in Guangdong Province, China. BMC Health Serv. Res. 2016, 16, 335. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Chung, R.Y.N.; Wei, X.; Mou, J.; Wong, S.Y.S.; Wong, M.C.S.; Zhang, D.; Zhang, Y.; Griffiths, S. Comparison of perceived quality amongst migrant and local patients using primary health care delivered by community health centres in Shenzhen, China. BMC Fam. Pract. 2014, 15, 76. [Google Scholar] [CrossRef] [PubMed]
- Zeng, J.; Shi, L.; Zou, X.; Chen, W.; Ling, L. Rural-urban Migrants’ Experiences with Primary Care under Different Types of Medical Institutions in Guangzhou, China. PLoS ONE 2015, 10, e0140922. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Lu, J.; Hu, S.; Cheng, K.K.; De Maeseneer, J.; Meng, Q.; Mossialos, E.; Xu, D.R.; Yip, W.; Zhang, H.; et al. The primary health-care system in China. Lancet 2017, 390, 2584–2594. [Google Scholar] [CrossRef]
- Yip, W.C.-M.; Hsiao, W.C.; Chen, W.; Hu, S.; Ma, J.; Maynard, A. Early appraisal of China’s huge and complex health-care reforms. Lancet 2012, 379, 833–842. [Google Scholar] [CrossRef]
- Sylvia, S.; Xue, H.; Zhou, C.; Shi, Y.; Yi, H.; Zhou, H.; Rozelle, S.; Pai, M.; Das, J. Tuberculosis detection and the challenges of integrated care in rural China: A cross-sectional standardized patient study. PLoS Med. 2017, 14, e1002405. [Google Scholar] [CrossRef] [PubMed]
- Xu, D.R.; Hu, M.Y.; He, W.J.; Liao, J.; Cai, Y.Y.; Sylvia, S.Y.; Hanson, K.; Pan, Y.L.; Zhou, Z.L.; Zhang, N.; et al. Assessing Quality of Primary Health Care in 7 Chinese Provinces with Unannounced Standardized Patients: Protocol of a Cross-Sectional Survey. BMJ Open 2018. accepted. [Google Scholar] [CrossRef]
- Barrows, H.S. An overview of the uses of standardized patients for teaching and evaluating clinical skills. Acad. Med. 1993, 68, 443. [Google Scholar] [CrossRef] [PubMed]
- Das, J.; Holla, A.; Das, V.; Mohanan, M.; Tabak, D.; Chan, B. In Urban and Rural India, A Standardized Patient Study Showed Low Levels of Provider Training and Huge Quality Gaps. Health Aff. 2012, 31, 2774–2784. [Google Scholar] [CrossRef] [PubMed]
- Das, J.; Kwan, A.; Daniels, B.; Satyanarayana, S.; Satyanarayana, S.; Subbaraman, R.; Bergkvist, S.; Das, R.K.; Das, V.; Pai, M. Use of standardised patients to assess quality of tuberculosis care: A pilot, cross-sectional study. Lancet Infect. Dis. 2015, 15, 1305–1313. [Google Scholar] [CrossRef]
- Daniels, B.; Dolinger, A.; Bedoya, G.; Rogo, K.; Goicoechea, A.; Coarasa, J.; Wafula, F.; Mwaura, N.; Kimeu, R.; Das, J. Use of standardised patients to assess quality of healthcare in Nairobi, Kenya: A pilot, cross-sectional study with international comparisons. BMJ Glob. Health 2017, 2, e000333. [Google Scholar] [CrossRef] [PubMed]
- Das, J.; Holla, A.; Mohpal, A.; Muralidharan, K. Quality and Accountability in Health Care Delivery: Audit-Study Evidence from Primary Care in India. Am. Econ. Rev. 2016, 106, 3765–3799. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Das, J.; Chowdhury, A.; Hussam, R.; Banerjee, A.V. The impact of training informal health care providers in India: A randomized controlled trial. Science 2016, 354, aaf7384. [Google Scholar] [CrossRef] [PubMed]
- Das, J.; Woskie, L.; Rajbhandari, R.; Abbasi, K.; Jha, A. Rethinking assumptions about delivery of healthcare: Implications for universal health coverage. BMJ 2018, 361, k1716. [Google Scholar] [CrossRef] [PubMed]
- Sylvia, S.; Shi, Y.; Xue, H.; Tian, X.; Wang, H.; Liu, Q.; Medina, A.; Rozelle, S. Survey using incognito standardized patients shows poor quality care in China’s rural clinics. Health Policy Plan. 2015, 30, 322–333. [Google Scholar] [CrossRef] [PubMed]
- Peabody, J.W.; Luck, J.; Glassman, P.; Dresselhaus, T.R.; Lee, M. Comparison of Vignettes, Standardized Patients, and Chart Abstraction: A Prospective Validation Study of 3 Methods for Measuring Quality. JAMA 2000, 283, 1715–1722. [Google Scholar] [CrossRef] [PubMed]
- Glassman, P.A.; Luck, J.; O’Gara, E.M.; Peabody, J.W. Using Standardized Patients to Measure Quality: Evidence from the Literature and a Prospective Study. Joint Comm. J. Qual. Improv. 2000, 26, 644–653. [Google Scholar] [CrossRef]
- Leonard, K.L.; Masatu, M.C. Using the Hawthorne effect to examine the gap between a doctor’s best possible practice and actual performance. J. Dev. Econ. 2010, 93, 226–234. [Google Scholar] [CrossRef]
- Woodward, C.A.; McConvey, G.A.; Neufeld, V.; Norman, G.R.; Walsh, A. Measurement of physician performance by standardized patients: refining techniques for undetected entry in physicians’ offices. Med. Care 1985, 23, 1019–1027. [Google Scholar] [CrossRef] [PubMed]
- TB CARE I. International Standards for Tuberculosis Care, Edition 3. 2014. Available online: http://www.istcweb.org (accessed on 14 September 2018).
- National Health and Family Planning Commission of the People’s Republic of China. Standards of Out-Patient Diagnosis and Treatment of Pulmonary Tuberculosis. 2012. Available online: http://www.moh.gov.cn/mohyzs/s3586/201202/54119.shtml (accessed on 14 September 2018).
- National Center for Tuberculosis Control and Prevention, China CDC. Diagnostic Criteria for Pulmonary Tuberculosis (WS 288-2008). 2008. Available online: http://tb.chinacdc.cn/zcfg/dfzcfg/201208/t20120814_66809.htm (accessed on 14 September 2018).
- National Health and Family Planning Commission of the People’s Republic of China. China Health Statistics Yearbook 2015. Available online: http://www.stats.gov.cn/tjsj/ndsj/2015/indexeh.htm (accessed on 14 September 2018).
- Shaanxi Bureau of Statistics. Shaanxi Statistical Yearbook; Shaanxi Statistics Press: Xian, China, 2016; Available online: http://www.shaanxitj.gov.cn/upload/2016/tongjinianj/2015/indexch.htm (accessed on 14 September 2018).
- Wang, J.; Wang, P.; Wang, X.; Zheng, Y.; Xiao, Y. Use and Prescription of Antibiotics in Primary Health Care Settings in China. JAMA Intern. Med. 2014, 174, 1914–1920. [Google Scholar] [CrossRef] [PubMed]
- Xue, H.; Shi, Y.J.; Huang, L.; Yi, H.M.; Zhou, C.C.; Zhou, H.; Kotb, S.; Tucker, J.D.; Sylvia, S.Y. Drivers of Inappropriate Antibiotic Prescriptions: A Quasi-Experimental Study of Primary Care Providers in Rural China. J. Antimicrob. Chemother. 2018. Forthcoming. [Google Scholar] [CrossRef]
- Hogan, C.A.; Puri, L.; Gore, G.; Pai, M. Impact of fluoroquinolone treatment on delay of tuberculosis diagnosis: A systematic review and meta-analysis. J Clin. Tuberc. Mycobact. Dis. 2017, 6, 1–7. [Google Scholar] [CrossRef]
- Yip, W.C.-M.; Hsiao, W.; Meng, Q.; Chen, W.; Sun, X. Realignment of incentives for health-care providers in China. Lancet 2010, 375, 1120–1130. [Google Scholar] [CrossRef]
- Currie, J.; Lin, W.; Meng, J. Addressing antibiotic abuse in China: An experimental audit study. J. Dev. Econ. 2014, 110, 39–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]


| Full Sample | Local Clinics | Migrant Clinics | Local vs. Migrant p-Value | |
|---|---|---|---|---|
| (N = 42) | (N = 16) | (N = 26) | ||
| Panel A: Facility Characteristics | ||||
| Number of patients received in 2014 | 7866.73 (2666.13–13,067.34) | 5857.5 (3578.6–8136.4) | 9152.64 (527.52–17,777.76) | 0.539 |
| Average distance to patients who visit clinic | 1.59 (1.18–2.01) | 1.43 (0.89–1.96) | 1.7 (1.09–2.31) | 0.517 |
| Number of staffs working full time at the facility | 3.27 (2.47–4.07) | 3.06 (2.01–4.12) | 3.4 (2.21–4.59) | 0.684 |
| Number of clinicians working full time at the facility | 2.07 (1.59–2.56) | 2.38 (1.44–3.31) | 1.88 (1.3–2.46) | 0.321 |
| Total value of equipment (10,000 RMB) | 1.2 (0.79–1.6) | 1.48 (0.65–2.31) | 1.01 (0.57–1.46) | 0.266 |
| Physicians who own their own facilities | 5 (12%, 5–26%) | 3 (19%, 7–43%) | 2 (8%, 2–25%) | 0.318 |
| Panel B: Clinician Characteristics | ||||
| Age (years) | 28 (70%, 55–82%) | 10 (63%, 39–82%) | 18 (75%, 55–88%) | 0.792 |
| Male clinicians | 32 (80%, 65–90%) | 11 (69%, 44–86%) | 21 (88%, 69–96%) | 0.401 |
| Clinicians with upper secondary or higher education | 21 (53%, 37–67%) | 8 (50%, 28–72%) | 13 (54%, 35–72%) | 0.158 |
| Clinicians with Practicing Physician Certificate | 5 (13%, 5–26%) | 2 (13%, 3–36%) | 3 (13%, 4–31%) | 0.796 |
| Clinicians with Assistant Practicing Physician Certificate | 11 (28%, 16–43%) | 6 (38%, 18–61%) | 5 (21%, 9–40%) | –– |
| Clinicians with Rural Physician Certificate | 28 (70%, 55–82%) | 11 (69%, 44–86%) | 17 (71%, 51–85%) | 0.253 |
| Clinicians receiving base salary | 28 (70%, 55–82%) | 10 (63%, 39–82%) | 18 (75%, 55–88%) | 0.888 |
| Monthly salary (1000 RMB) | 5.51 (1.25–9.76) | 3.06 (1.55–4.56) | 7.15 (–0.02–14.31) | 0.347 |
| Clinicians who received Tuberculosis-specific training in 2014 | 17 (43%, 29–58%) | 9 (56%, 33–77%) | 8 (33%, 18–53%) | 0.155 |
| Full Sample | Local Clinics | Migrant Clinics | Local vs. Migrant p-Value | |
|---|---|---|---|---|
| Patient-clinician interactions | 42 | 16 | 26 | |
| Case management | ||||
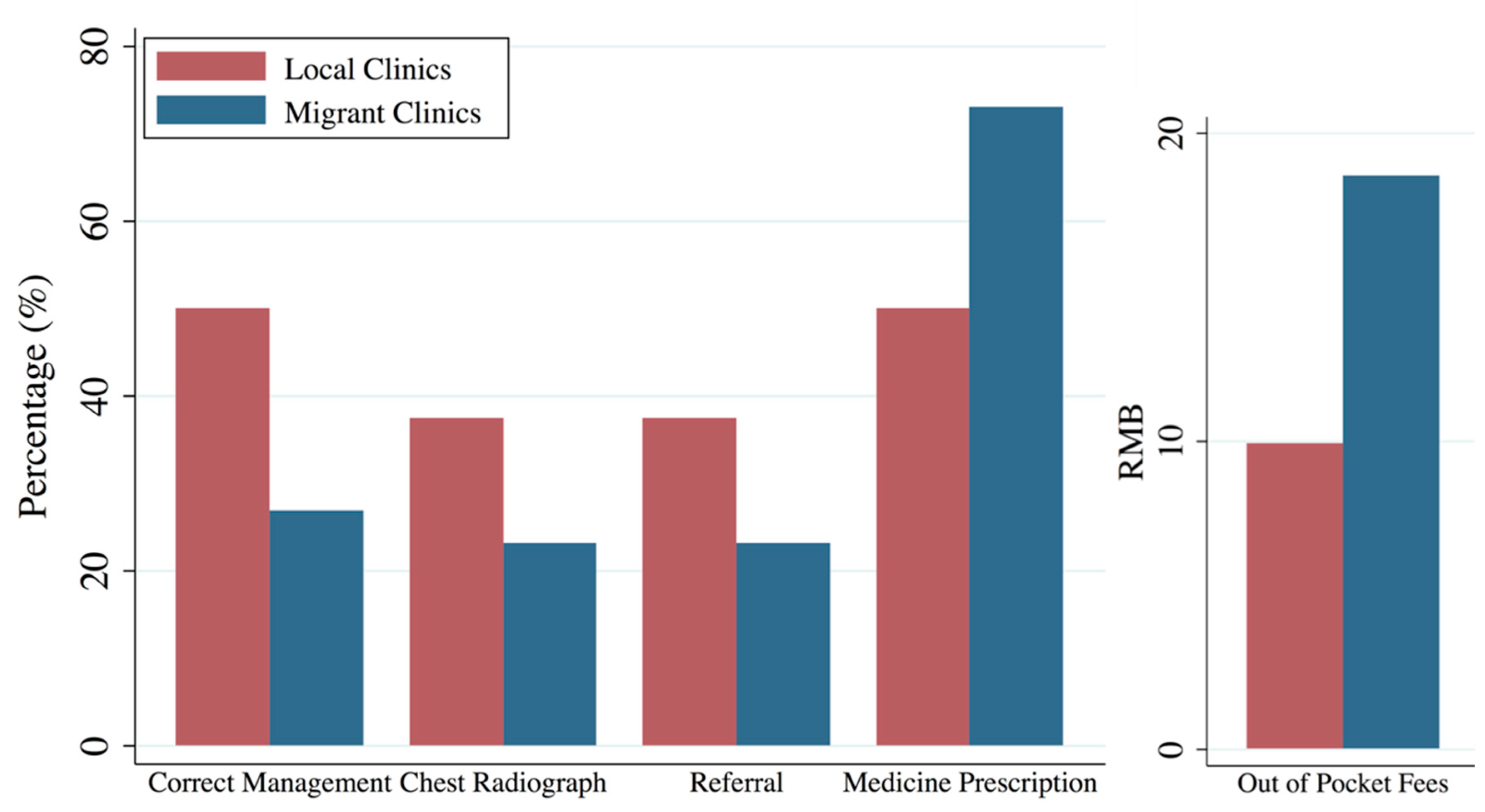
| Correctly managed the case § | 36 | 50 | 27 | 0.086 |
| (23–51) | (28–72) | (14–46) | ||
| Ordered a chest radiograph | 29 | 38 | 23 | 0.290 |
| (17–44) | (18–61) | (11–42) | ||
| Ordered a sputum smear test | 2 | 0 | 4 | 0.497 |
| (0–12) | (0–19) | (1–19) | ||
| Referred to higher level hospitals | 29 | 38 | 23 | 0.179 |
| (17–44) | (18–61) | (11–42) | ||
| Referred to CDC or DOTs, if referral | 2 | 0 | 4 | 0.497 |
| (0–12) | (0–19) | (1–19) | ||
| Medicine Prescribed | 64 | 50 | 73 | 0.024 |
| (49–77) | (28–72) | (54–86) | ||
| Asked patient to return | 17 | 6 | 23 | 0.141 |
| (8–31) | (1–28) | (11–42) | ||
| Gave any antibiotic | 57 | 50 | 62 | 0.282 |
| (42–71) | (28–72) | (43–78) | ||
| Gave any fluoroquinolone | 5 | 6 | 4 | 0.907 |
| (1–16) | (1–28) | (1–19) | ||
| Process | ||||
| Time with clinician (min) | 9.44 | 9.16 | 9.61 | 0.449 |
| (7.23–11.65) | (5.47–12.85) | (6.66–12.57) | ||
| Number of questions and examinations (ISTC) | 5.38 | 5.5 | 5.31 | 0.828 |
| (4.48–6.28) | (3.75–7.25) | (4.22–6.4) | ||
| % of questions and examinations (ISTC) | 17 | 18 | 17 | 0.828 |
| (14–20) | (12–23) | (14–21) | ||
| Number of questions and examinations (China) | 3.81 | 4 | 3.69 | 0.663 |
| (3.18–4.44) | (2.77–5.23) | (2.95–4.44) | ||
| % of questions and examinations (China) | 21 | 22 | 21 | 0.663 |
| (18–25) | (15–29) | (16–25) | ||
| % of essential history checklist asked by clinician (Both Standards) | 34 | 36 | 33 | 0.739 |
| (29–39) | (26–46) | (26–40) | ||
| Out of pocket fees of consultation and medicines combined (RMB) | 15.31 | 9.94 | 18.62 | 0.024 |
| (8.52–22.1) | (1.21–18.67) | (8.82–28.41) | ||
| Out of pocket fees of consultation and medicines combined (US dollars) * | 2.36 | 1.53 | 2.86 | 0.024 |
| (1.31–3.4) | (0.19–2.87) | (1.36–4.37) | ||
| Diagnosis | ||||
| Mentioned tuberculosis | 5 | 6 | 4 | 0.182 |
| (1–16) | (1–28) | (1–19) |
| Correct Case Management | Chest Radiograph | Referral | Medicine Prescription | Out of Pocket Fees | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | (9) | (10) | |
| Service for migrant workers | −0.29 ** | −0.29 * | −0.28 * | −0.36 ** | −0.24 * | −0.30 * | 0.29 ** | 0.32 ** | 15.52 * | 13.30 * |
| (0.11) | (0.12) | (0.13) | (0.14) | (0.11) | (0.12) | (0.10) | (0.12) | (6.14) | (6.20) | |
| Clinician age (years) | −0.01 | −0.01 | −0.01 | 0.00 | −0.00 | 0.00 | 0.01 | 0.01 | 0.34 | 0.38 |
| (0.01) | (0.01) | (0.01) | (0.01) | (0.01) | (0.01) | (0.01) | (0.01) | (0.28) | (0.27) | |
| Male clinician | 0.06 | 0.04 | 0.03 | 0.06 | 0.19 | 0.17 | −0.06 | −0.07 | −4.27 | −8.42 |
| (0.16) | (0.15) | (0.17) | (0.17) | (0.16) | (0.14) | (0.17) | (0.16) | (7.19) | (7.29) | |
| Clinician education, upper secondary or higher | 0.12 | 0.04 | 0.08 | 0.29 | 0.19 | 0.20 | −0.23 | −0.24 | −23.48 * | −20.22 * |
| (0.22) | (0.24) | (0.27) | (0.34) | (0.22) | (0.23) | (0.23) | (0.26) | (8.62) | (8.59) | |
| Practicing physician certificate | −0.24 * | −0.22 | −0.35 ** | −0.41 ** | −0.21 | −0.21 | 0.13 | 0.15 | 4.73 | 10.81 |
| (0.12) | (0.12) | (0.12) | (0.15) | (0.13) | (0.12) | (0.14) | (0.14) | (6.17) | (6.33) | |
| Clinician has base salary | 0.28 | 0.41 * | -- | -- | 0.21 | 0.48 ** | −0.01 | −0.18 | −9.13 | −22.00 * |
| (0.15) | (0.21) | -- | -- | (0.15) | (0.18) | (0.16) | (0.22) | (6.95) | (8.39) | |
| Number of clinicians in a clinic | 0.06 | −0.14 | 0.12 * | −0.07 | −6.52 * | |||||
| (0.06) | (0.09) | (0.05) | (0.07) | (2.63) | ||||||
| Total value of equipment (10,000 RMB) | −0.05 | 0.06 | −0.12 * | 0.07 | 0.00 | |||||
| (0.06) | (0.06) | (0.05) | (0.06) | (2.38) | ||||||
| Building of clinic owned by clinicians | 0.15 | −0.34 | 0.04 | −0.05 | 12.99 | |||||
| (0.23) | (0.25) | (0.18) | (0.23) | (10.19) | ||||||
| Number of Observations | 40 | 40 | 28 | 28 | 40 | 40 | 40 | 40 | 40 | 40 |
| Mean of Outcome | 0.36 | 0.29 | 0.29 | 0.64 | 15.31 | |||||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xue, H.; Hager, J.; An, Q.; Liu, K.; Zhang, J.; Auden, E.; Yang, B.; Yang, J.; Liu, H.; Nie, J.; et al. The Quality of Tuberculosis Care in Urban Migrant Clinics in China. Int. J. Environ. Res. Public Health 2018, 15, 2037. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15092037
Xue H, Hager J, An Q, Liu K, Zhang J, Auden E, Yang B, Yang J, Liu H, Nie J, et al. The Quality of Tuberculosis Care in Urban Migrant Clinics in China. International Journal of Environmental Research and Public Health. 2018; 15(9):2037. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15092037
Chicago/Turabian StyleXue, Hao, Jennifer Hager, Qi An, Kai Liu, Jing Zhang, Emma Auden, Bingyan Yang, Jie Yang, Hongyan Liu, Jingchun Nie, and et al. 2018. "The Quality of Tuberculosis Care in Urban Migrant Clinics in China" International Journal of Environmental Research and Public Health 15, no. 9: 2037. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15092037