Relationship between the Well-Being of Elderly Men and Cohabiting with Women Who Have Had Experience as a Health Promotion Volunteer in Japan: A Cross-Sectional Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Area
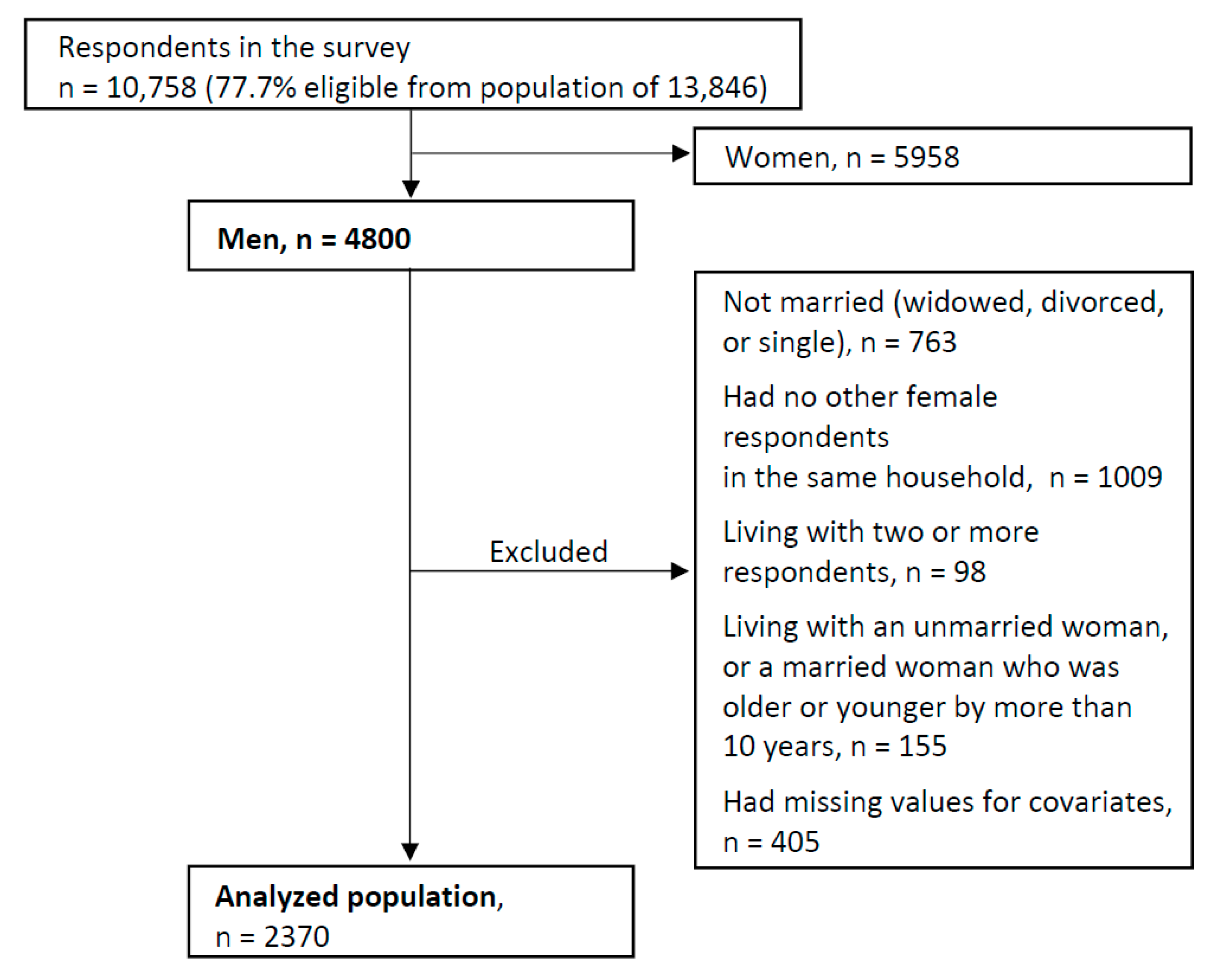
2.2. Study Population
2.3. Exposure Measurement
2.4. Outcome Measurement
2.5. Covariates
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ministry of Health Labour & Welfare, Japan. Overview of the Life Table by Prefecture; Ministry of Health Labour & Welfare, Japan: Tokyo, Japan, 2010. (In Japanese)
- Nagano Prefecture Healthy Longevity Project Study Team. Report on Nagano prefecture healty longevity project and research program (analysis of factors in healthy longevity). Available online: https://www.pref.nagano.lg.jp/kenko-fukushi/kenko/kenko/documents/saisyueiyaku.pdf (accessed on 6 November 2018).
- Imamura, H.; Shonoda, S.; Kaneko, I. Komyuniti no Chikara: "Enryogachi na" sōsharu kyapitaru no hakken; Keio Gijuku Daigaku Shuppankai: Tokyo, Japan, 2010; ISBN 978-4-7664-1752-4. (In Japanese) [Google Scholar]
- Hoshino, A.; Katsura, T.; Naruki, H. Influence of continuing experience in hoken-suisinin activities of f-city on health behaviors of participants—comparison between non-hoken-suisinins and hoken-suisinins by differences in ages of this activity. J. Jpn. Health Med. Assoc. 2003, 12, 38–42. (In Japanese) [Google Scholar]
- Taguchi, A.; Murayama, H.; Murashima, S. Association between municipal health promotion volunteers’ health literacy and their level of outreach activities in Japan. PLoS ONE 2016, 11, e0164612. [Google Scholar] [CrossRef] [PubMed]
- Imamura, H.; Asano, A.; Nishiwaki, Y. Relationship between health promotion volunteer experience and adl in elderly women—results from a survey of Suzaka city, Nagano. Shinshu J. Public Health 2017, 11, 97–106. (In Japanese) [Google Scholar]
- Imamura, H.; Murakami, Y.; Okamura, T.; Nishiwaki, Y. Relationship between health promotion volunteer experience and medical costs: Hoken-hodouin activities in Suzaka, Nagano. Jpn. J. Public Health 2017, 64, 25–35. (In Japanese) [Google Scholar]
- Staehelin, K.; Schindler, C.; Spoerri, A.; Zemp, S.E. Marital status, living arrangement and mortality: Does the association vary by gender? J. Epidemiol. Community Health 2012, 66, e22. [Google Scholar] [CrossRef] [PubMed]
- Elwert, F.; Christakis, N.A. The effect of widowhood on mortality by the causes of death of both spouses. Am. J. Public Health 2008, 98, 2092–2098. [Google Scholar] [CrossRef] [PubMed]
- Dupre, M.E.; Beck, A.N.; Meadows, S.O. Marital trajectories and mortality among us adults. Am. J. Epidemiol. 2009, 170, 546–555. [Google Scholar] [CrossRef]
- Scafato, E.; Galluzzo, L.; Gandin, C.; Ghirini, S.; Baldereschi, M.; Capurso, A.; Maggi, S.; Farchi, G.; For the Ilsa Working Group. Marital and cohabitation status as predictors of mortality: A 10-year follow-up of an italian elderly cohort. Soc. Sci. Med. 2008, 67, 1456–1464. [Google Scholar] [CrossRef]
- Trevisan, C.; Veronese, N.; Maggi, S.; Baggio, G.; De Rui, M.; Bolzetta, F.; Zambon, S.; Sartori, L.; Perissinotto, E.; Crepaldi, G.; et al. Marital status and frailty in older people: Gender differences in the progetto veneto anziani longitudinal study. J. Womens Health 2016, 25, 630–637. [Google Scholar] [CrossRef]
- Ikeda, A.; Iso, H.; Toyoshima, H.; Fujino, Y.; Mizoue, T.; Yoshimura, T.; Inaba, Y.; Tamakoshi, A. Marital status and mortality among japanese men and women: The Japan collaborative cohort study. BMC Public Health 2007, 7, 73. [Google Scholar] [CrossRef]
- Jang, S.N.; Kawachi, I.; Chang, J.; Boo, K.; Shin, H.G.; Lee, H.; Cho, S.I. Marital status, gender, and depression: Analysis of the baseline survey of the Korean longitudinal study of ageing (klosa). Soc. Sci. Med. 2009, 69, 1608–1615. [Google Scholar] [CrossRef] [PubMed]
- Monin, J.; Doyle, M.; Levy, B.; Schulz, R.; Fried, T.; Kershaw, T. Spousal associations between frailty and depressive symptoms: Longitudinal findings from the cardiovascular health study. J. Am. Geriatr. Soc. 2016, 64, 824–830. [Google Scholar] [CrossRef] [PubMed]
- Meyler, D.; Stimpson, J.P.; Peek, M.K. Health concordance within couples: A systematic review. Soc. Sci. Med. 2007, 64, 2297–2310. [Google Scholar] [CrossRef] [PubMed]
- Japanese Organization for International Cooperation in Family Planning (JOICFP). Where There Is a Will: The Story of a Countryside Health Nurse [Suzaka no Ka-Chan Ganbaru]; JOICFP: Tokyo, Japan, 1981. [Google Scholar]
- Suzaka City Hall. Hoken-hodouin hassho no chi Suzaka city. Available online: https://www.city.suzaka.nagano.jp/contents/item.php?id=5949e17d9a52e (accessed on 6 November 2018). (In Japanese).
- Tsutsui, T.; Muramatsu, N. Care-needs certification in the long-term care insurance system of Japan. J. Am. Geriatr. Soc. 2005, 53, 522–527. [Google Scholar] [CrossRef] [PubMed]
- Koyano, W.; Shibata, H.; Nakazato, K.; Haga, H.; Suyama, Y. Measurement of competence: Reliability and validity of the TMIG index of competence. Arch. Gerontol. Geriatr. 1991, 13, 103–116. [Google Scholar] [CrossRef]
- Koyano, W.; Hashimoto, M.; Fukawa, T.; Shibata, H.; Gunji, A. Functional capacity of the elderly: Measurement by the tmig index of competence. Jpn. J. Public Health 1993, 40, 468–474. (In Japanese) [Google Scholar]
- Hoyl, M.T.; Alessi, C.A.; Harker, J.O.; Josephson, K.R.; Pietruszka, F.M.; Koelfgen, M.; Mervis, J.R.; Fitten, L.J.; Rubenstein, L.Z. Development and testing of a five-item version of the geriatric depression scale. J. Am. Geriatr. Soc. 1999, 47, 873–878. [Google Scholar] [CrossRef]
- Rinaldi, P.; Mecocci, P.; Benedetti, C.; Ercolani, S.; Bregnocchi, M.; Menculini, G.; Catani, M.; Senin, U.; Cherubini, A. Validation of the five-item geriatric depression scale in elderly subjects in three different settings. J. Am. Geriatr. Soc. 2003, 51, 694–698. [Google Scholar] [CrossRef]
- Zou, G. A modified poisson regression approach to prospective studies with binary data. Am. J. Epidemiol. 2004, 159, 702–706. [Google Scholar] [CrossRef]
- Nakamura, T.; Michikawa, T.; Imamura, H.; Takebayashi, T.; Nishiwaki, Y. Relationship between depressive symptoms and activity of daily living dependence in older Japanese: The kurabuchi study. J. Am. Geriatr. Soc. 2017, 65, 2639–2645. [Google Scholar] [CrossRef]
- Schwarzbach, M.; Luppa, M.; Forstmeier, S.; Konig, H.H.; Riedel-Heller, S.G. Social relations and depression in late life-a systematic review. Int. J. Geriatr. Psychiatry 2014, 29, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Koizumi, Y.; Awata, S.; Kuriyama, S.; Ohmori, K.; Hozawa, A.; Seki, T.; Matsuoka, H.; Tsuji, I. Association between social support and depression status in the elderly: Results of a 1-year community-based prospective cohort study in japan. Psychiatry Clin. Neurosci. 2005, 59, 563–569. [Google Scholar] [CrossRef] [PubMed]
- Vyncke, V.; Hardyns, W.; Peersman, W.; Pauwels, L.; Groenewegen, P.; Willems, S. How equal is the relationship between individual social capital and psychological distress? A gendered analysis using cross-sectional data from Ghent (Belgium). BMC Public Health 2014, 14, 960. [Google Scholar] [CrossRef] [PubMed]
- Okabayashi, H.; Liang, J.; Krause, N.; Akiyama, H.; Sugisawa, H. Mental health among older adults in Japan: Do sources of social support and negative interaction make a difference? Soc. Sci. Med. 2004, 59, 2259–2270. [Google Scholar] [CrossRef] [PubMed]
- Noguchi, M.; Iwase, T.; Suzuki, E.; Takao, S. Home visits by commissioned welfare volunteers and psychological distress: A population-based study of 11,312 community-dwelling older people in japan. Int. J. Geriatr. Psychiatry 2015, 30, 1156–1163. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Experience as Health Promotion Volunteer of Cohabiting Woman | ||||
|---|---|---|---|---|---|
| No n = 936 | Yes n = 1434 | p-value c | |||
| Age (years) | |||||
| 65–69 | 219 | (23.4%) | 237 | (16.5%) | < 0.001 |
| 70–74 | 335 | (35.8%) | 482 | (33.6%) | |
| 75–79 | 203 | (21.7%) | 366 | (25.5%) | |
| 80–84 | 128 | (13.7%) | 242 | (16.9%) | |
| ≥85 | 51 | (5.4%) | 107 | (7.5%) | |
| (Mean ± standard deviation years) | (74.0 ± 5.7) | (75.2 ± 5.8) | |||
| Educational attainment (years) | |||||
| ≥10 | 595 | (63.6%) | 961 | (67.0%) | 0.08 |
| <10 | 341 | (36.4%) | 473 | (33.0%) | |
| Equivalent household income a | |||||
| 1st quartile (–2.00 million yen) | 124 | (13.2%) | 169 | (11.8%) | 0.06 |
| 2nd quartile (2.00–3.10 million yen) | 257 | (27.5%) | 378 | (26.4%) | |
| 3rd quartile (3.10–4.24 million yen) | 292 | (31.2%) | 410 | (28.6%) | |
| 4th quartile (4.24– million yen) | 263 | (28.1%) | 477 | (33.3%) | |
| History of major diseases b | |||||
| No | 506 | (54.1%) | 782 | (54.5%) | 0.82 |
| Yes | 430 | (45.9%) | 652 | (45.5%) | |
| Exercise habits | |||||
| One hour or more per week | 515 | (55.0%) | 794 | (55.4%) | 0.87 |
| Less than one hour per week | 421 | (45.0%) | 640 | (44.6%) | |
| Consciousness of healthy eating habits | |||||
| Conscious | 827 | (88.4%) | 1296 | (90.4%) | 0.12 |
| Not conscious | 109 | (11.6%) | 138 | (9.6%) | |
| Current drinking | |||||
| No | 333 | (35.6%) | 464 | (32.4%) | 0.11 |
| Yes | 603 | (64.4%) | 970 | (67.6%) | |
| Current smoking | |||||
| No | 782 | (83.5%) | 1220 | (85.1%) | 0.32 |
| Yes | 154 | (16.5%) | 214 | (14.9%) | |
| Experience as Health Promotion Volunteer of Cohabiting Woman | Outcome/Study Population (%) | Model 1 a | Model 2 b | Model 3 c | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PR (95% CI)d | p-Value | PR (95% CI) | p-Value | PR (95% CI) | p-Value | ||||||||
| Presence of experience | |||||||||||||
| Not experienced | 165 | / | 885 | (18.6%) | 1.00 | 1.00 | 1.00 | ||||||
| Experienced | 249 | / | 1362 | (18.3%) | 0.94 | (0.78–1.12) | 0.46 | 0.97 | (0.81–1.16) | 0.74 | 1.02 | (0.87–1.21) | 0.79 |
| Years since experience | |||||||||||||
| Not experienced | 165 | / | 885 | (18.6%) | 1.00 | 1.00 | 1.00 | ||||||
| Experienced: 0–19 years | 99 | / | 572 | (17.3%) | 1.01 | (0.80–1.27) | 0.93 | 1.07 | (0.85–1.34) | 0.57 | 1.12 | (0.90–1.39) | 0.30 |
| : 20–39 years | 121 | / | 639 | (18.9%) | 0.90 | (0.73–1.12) | 0.35 | 0.94 | (0.76–1.16) | 0.55 | 1.00 | (0.82–1.23) | 0.98 |
| : 40 years or more | 16 | / | 85 | (18.8%) | 0.75 | (0.48–1.19) | 0.22 | 0.78 | (0.49–1.25) | 0.30 | 0.86 | (0.55–1.35) | 0.52 |
| : no response | 13 | / | 66 | (19.7%) | 0.92 | (0.55–1.52) | 0.73 | 0.85 | (0.52–1.38) | 0.52 | 0.77 | (0.50–1.21) | 0.26 |
| Leadership role | |||||||||||||
| Not experienced | 165 | / | 885 | (18.6%) | 1.00 | 1.00 | 1.00 | ||||||
| Experienced: no | 186 | / | 985 | (18.9%) | 0.98 | (0.81–1.18) | 0.84 | 1.01 | (0.84–1.22) | 0.92 | 1.06 | (0.89–1.26) | 0.54 |
| : yes | 40 | / | 267 | (15.0%) | 0.77 | (0.56–1.06) | 0.10 | 0.85 | (0.62–1.16) | 0.31 | 0.90 | (0.67–1.22) | 0.51 |
| : no response | 23 | / | 110 | (20.9%) | 0.94 | (0.64–1.38) | 0.74 | 0.90 | (0.61–1.33) | 0.59 | 0.98 | (0.68–1.42) | 0.93 |
| Satisfaction with the experience | |||||||||||||
| Not experienced | 165 | / | 885 | (18.6%) | 1.00 | 1.00 | 1.00 | ||||||
| Experienced: low | 37 | / | 152 | (24.3%) | 1.30 | (0.96–1.77) | 0.10 | 1.29 | (0.96–1.75) | 0.09 | 1.27 | (0.95–1.70) | 0.11 |
| : medium | 161 | / | 842 | (19.1%) | 0.98 | (0.80–1.19) | 0.83 | 1.02 | (0.84–1.24) | 0.84 | 1.08 | (0.90–1.30) | 0.39 |
| : high | 43 | / | 311 | (13.8%) | 0.70 | (0.51–0.95) | 0.02 | 0.74 | (0.54–1.00) | 0.05 | 0.81 | (0.60–1.10) | 0.18 |
| : no response | 8 | / | 57 | (14.0%) | 0.68 | (0.35–1.30) | 0.24 | 0.65 | (0.34–1.24) | 0.19 | 0.62 | (0.35–1.10) | 0.10 |
| Experience as Health Promotion Volunteer of Cohabiting Woman | Outcome/Study Population (%) | Model 1 a | Model 2 b | Model 3 c | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PR (95% CI) d | p-Value | PR (95% CI) | p-Value | PR (95% CI) | p-Value | ||||||||
| Presence of experience | |||||||||||||
| Not experienced | 232 | / | 917 | (25.3%) | 1.00 | 1.00 | 1.00 | ||||||
| Experienced | 300 | / | 1399 | (21.4%) | 0.81 | (0.70–0.94) | 0.01 | 0.82 | (0.71–0.95) | 0.01 | 0.84 | (0.73–0.97) | 0.02 |
| Years since experience | |||||||||||||
| Not experienced | 232 | / | 917 | (25.3%) | 1.00 | 1.00 | 1.00 | ||||||
| Experienced: 0–19 years | 104 | / | 579 | (18.0%) | 0.77 | (0.62–0.95) | 0.01 | 0.78 | (0.63–0.96) | 0.02 | 0.80 | (0.65–0.99) | 0.04 |
| : 20–39 years | 157 | / | 660 | (23.8%) | 0.85 | (0.71–1.01) | 0.07 | 0.86 | (0.72–1.03) | 0.10 | 0.89 | (0.75–1.06) | 0.20 |
| : 40 years or more | 26 | / | 94 | (27.7%) | 0.83 | (0.58–1.18) | 0.30 | 0.84 | (0.59–1.21) | 0.36 | 0.87 | (0.61–1.24) | 0.46 |
| : no response | 13 | / | 66 | (19.7%) | 0.70 | (0.43–1.14) | 0.16 | 0.67 | (0.41–1.09) | 0.11 | 0.64 | (0.40–1.02) | 0.06 |
| Leadership role | |||||||||||||
| Not experienced | 232 | / | 917 | (25.3%) | 1.00 | 1.00 | 1.00 | ||||||
| Experienced: no | 218 | / | 1,008 | (21.6%) | 0.83 | (0.71–0.97) | 0.02 | 0.84 | (0.72–0.99) | 0.03 | 0.86 | (0.73–1.00) | 0.05 |
| : yes | 55 | / | 271 | (20.3%) | 0.77 | (0.59–0.99) | 0.05 | 0.79 | (0.61–1.03) | 0.08 | 0.83 | (0.64–1.08) | 0.16 |
| : no response | 27 | / | 120 | (22.5%) | 0.74 | (0.52–1.03) | 0.08 | 0.72 | (0.51–1.02) | 0.06 | 0.76 | (0.54–1.06) | 0.11 |
| Satisfaction with the experience | |||||||||||||
| Not experienced | 232 | / | 917 | (25.3%) | 1.00 | 1.00 | 1.00 | ||||||
| Experienced: low | 35 | / | 160 | (21.9%) | 0.85 | (0.63–1.16) | 0.31 | 0.85 | (0.63–1.16) | 0.31 | 0.83 | (0.62–1.11) | 0.20 |
| : medium | 189 | / | 858 | (22.0%) | 0.83 | (0.70–0.98) | 0.03 | 0.84 | (0.71–1.00) | 0.05 | 0.88 | (0.74–1.03) | 0.12 |
| : high | 65 | / | 324 | (20.1%) | 0.74 | (0.58–0.95) | 0.02 | 0.76 | (0.60–0.97) | 0.03 | 0.79 | (0.62–1.01) | 0.06 |
| : no response | 11 | / | 57 | (19.3%) | 0.70 | (0.41–1.20) | 0.20 | 0.68 | (0.40–1.16) | 0.16 | 0.68 | (0.40–1.13) | 0.13 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Imamura, H.; Nakamura, H.; Nishiwaki, Y. Relationship between the Well-Being of Elderly Men and Cohabiting with Women Who Have Had Experience as a Health Promotion Volunteer in Japan: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2019, 16, 65. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16010065
Imamura H, Nakamura H, Nishiwaki Y. Relationship between the Well-Being of Elderly Men and Cohabiting with Women Who Have Had Experience as a Health Promotion Volunteer in Japan: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2019; 16(1):65. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16010065
Chicago/Turabian StyleImamura, Haruhiko, Hideki Nakamura, and Yuji Nishiwaki. 2019. "Relationship between the Well-Being of Elderly Men and Cohabiting with Women Who Have Had Experience as a Health Promotion Volunteer in Japan: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 16, no. 1: 65. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16010065