1. Introduction
In the last 100 years, earthquakes have claimed millions of lives and injured thousands of people [
1]. An effective and well-conceived emergency management system designed to reduce the mortality and morbidity associated with earthquakes is crucial for all the health care workers involved in disaster management [
2,
3]. Thus, the analysis and study of traumatic injuries in patients affected by major disasters is fundamental to assess the patterns of disaster-related injuries, in order both to enhance health care delivery in the event of a major disaster and to train emergency medical responders [
4]. Italy lies on the boundary where the African and Eurasian tectonic plates converge. The movement of these two big plates colliding results in the deformation and high amounts of energy that are occasionally released in earthquakes of different magnitude. Since 1900 to date, there have been 30 large earthquakes (Mw ≥ 5.8), some of which were devastating. The most powerful earthquakes recorded in the last few years hit Abruzzo on 6 April 2009, Mw = 6.1, Emilia-Romagna on 20 May 2012, Mw = 5.8 [
5], and Central Italy in 2016 and 2017.
The earthquake that struck the city of L’Aquila in 2009 consisted in a series of foreshocks, which began in December 2008 and ended in 2012 [
6], with epicenters in the L’Aquila city and province. The mainshock struck at 03:32 a.m., Central European Time, on 6 April 2009 [
7], with a moment magnitude (MMS) of 6.3 (5.8 or 5.9 as measured by the local magnitude scale), and with geographical coordinates of the epicenter 42°20′51.36″ N 13°22′48.4″ E, located in the hamlet of Colle Miruci, in Roio (L’Aquila), and was widely felt with varying degrees of intensity in a large part of Central Italy [
8]. Based on the local magnitude scale rating (the so-called Richter scale, which however does not provide accurate estimates for large magnitude earthquakes [
9]), the seismographs measured a magnitude 5.9 ML tremor, thus resulting in a moderate seismic event if compared to the maximum values that can be reached on this seismic magnitude scale [
10]. Indeed, the Peak Ground Acceleration [
11], which is the maximum acceleration of an earthquake on the ground surface, during the 6 April 2009 quake, reached values of up to 0.68 g, a value that can be theoretically assigned to 7.2–7.4 magnitude earthquakes [
12]. Based on the Mercalli intensity scale, which rates the observed structural damage of earthquakes, the initial estimate by the National Institute of Geophysics and Volcanology (INGV—Istituto Nazionale di Geofisica e Vulcanologia) ranged between the VIII and IX intensity level. The mainshock was followed by 256 aftershocks over the course of the next 48 h, of which more than 150 occurred on Tuesday, 7 April, with 56 aftershocks larger than magnitude 3.0 ML. Three events with magnitude greater than 5.0 occurred on 6, 7 and 9 April. The earthquake caused 309 casualties [
13], more than 1600 people were injured, 70,000 displaced from their homes, and the cost of the damage was estimated to be more than 10 billion Euros.
During the L’Aquila earthquake, the treatment of injured patients was delayed due to collapsed roadways and the severe structural damages of the main local hospital, the ‘Ospedale San Salvatore’ (following the mainshock, 90% of the hospital’s facilities were severely damaged) [
14,
15]. Generally, earthquakes cause a higher number of injuries and morbidity than mortality, and the most common earthquake injury pattern involves the musculoskeletal system [
16].
In their systematic literature review on the impact of earthquakes on human health, Doocy et al. reported that soft tissue injuries (including lacerations and contusions), fractures (in particular, limbs), and crush injury to head, thorax and abdomen caused by buildings collapsing, are the most common types of injury [
17]. They can abruptly result in death by asphyxiation, bleeding and acute kidney injury (due to crush syndrome) [
18,
19]. A body of studies has focused on the different patterns of fractures, as they represent half of the injury-related hospital admissions and a major reason of long-term disabilities [
12,
20]. Unlike other natural disasters, earthquakes are unpredictable, thus often causing catastrophic and uncontrollable events [
21]. However, to date, the patterns of earthquake-related injuries, and in particular the trauma caused by the earthquakes that struck Italy in the past years, have not yet been extensively studied [
16,
22].
This study aimed to analyze the trauma admissions within the first 96 h after the mainshock, with a focus on the injury patterns, the features of earthquake-related injury admissions, the in-hospital mortality rates, and other related health outcomes. Although an analysis of the patterns of injury admissions following the L’Aquila earthquake has not yet been conducted, it may be relevant to enhance the assistance capability in high-income countries with high-standard health care services, and to provide recommendations to improve the Italian health care system during and after major disasters. On an international level, research studies that specifically target the injury patterns following high-magnitude earthquakes have not yet been conducted at a high level of scientific standards, due to the scarcity and poor quality of the data collected. As reported by Bortolin et al., the characterization of a specific disaster-related injury pattern is crucial to build an effective disaster preparedness and response system, including the development of guidelines and the definition of standards-of-care (SOC) specific to any, natural or man-made, mass casualty event [
4].
2. Materials and Methods
This is an observational and descriptive study based on current data. We reviewed the hospital discharge forms of 171 patients involved in the L’Aquila city earthquake, and from the so-called “seismic crater” geographic area (arbitrarily comprising of the city of L’Aquila and 41 smaller municipalities struck by the 03:32 a.m. earthquake and by the aftershocks), who were admitted to 30 regional and extra-regional hospitals [
8]. We conducted a retrospective analysis of all inpatient hospitalizations recorded in the large discharge database of the Abruzzo region [
23]. We excluded from the study outpatient surgeries, rehabilitation hospital stays, and long-stay hospital patients. Moreover, we did not report all the injury-related admissions to the ‘Ares Marche’ field hospital, as no hospital discharge forms were released [
24]. We used the primary diagnosis codes from the chapter titled “Injury and Poisoning” with ICD-9-CM codes from 800–959 of the Italian version of the ICD-9-CM “International Classification of Diseases—9th revision—Clinical Modification” 2007 (although they are part of the same chapter, the ICD-9-CM diagnosis codes in the range 960–999 have not been taken into account as they were not reported as a cause of hospitalization and they are also related to poisoning). Data include injury-related hospital admissions, age, gender, type of discharge, in-hospital mortality and average length of stay (LOS). We also analyzed the secondary diagnoses and whether they reported any injury code (800–959 ICD9-CM) to identify multiple-injured patients. We compared the inpatient admissions and the types of discharge from 6 to 9 April 2009 with all the years following the earthquake (2010–2016) in order to determine any difference between the earthquake-related admissions and discharges and those following the event.
2.1. Statistics
Data on the admissions of the population from the seismic crater area (L’Aquila city and province), were collected from file A of the HDRs (hospital discharge records), and they refer to the time period from 6 April 2009 to 9 April 2009. The hospital discharge forms were retrieved from the information and health statistics management service of the Abruzzo Region Health System. For the analysis of data expressed in terms of frequencies, we used the χ2-Test and the Fisher Test. To perform the analyses of numerical data, such as the LOS, we used the T-Test or the Wilcoxon test if the normality requirement was not respected. Furthermore, we used the Cramér’s V test to measure the association between two nominal variables. For the statistical analysis, we used software R, version 3.4.3 (The R Foundation, Vienna, Austria) for Windows.
2.2. Seismic Crater Area
It is a geographical subset of the province of L’Aquila, which comprises of the city of L’Aquila, with a population of 72,696 inhabitants, and 41 smaller municipalities (a total of 38,874 inhabitants) [
8]. Such selection was based on the earthquake-related structural damages. Although some municipalities of the neighboring provinces were struck by the earthquake, they were not included in the study as they are regulated by different local health authorities with different hospital admission policies.
2.3. Ethical Considerations
This study was approved by all of the participating researchers and the Ethical Committee (IRB: Internal review board) of the University of L’Aquila on 16 January 2018 and registered on 1 February 2018 with no. 4904.
2.4. Methodological Limitations
The use of HDRs in epidemiology has strengths, limitations and may introduce biases. The most important strengths are that data already exist, are large and are collected independently from research purposes. The limitations are that data are pre-collected by non-researchers, with a low or unknown quality. Biases may be also introduced, like misclassification as the result of unclear or erroneous clinical documentation, or like the fact that expensive medical procedures are usually documented better than those less costly.
In the few days following the earthquake under investigation, the Abruzzo hospitals and in particular the L’Aquila hospital, focused on the management of the emergencies related to the event. All other emergencies were redirected to other hospitals like the ‘Ares Marche’ field hospital. However, there is no written note on the HDRs that may guarantee that all admissions are directly due to the earthquake, and—for privacy reasons—we could not contact the patients involved in the study for a confirmation.
4. Discussion
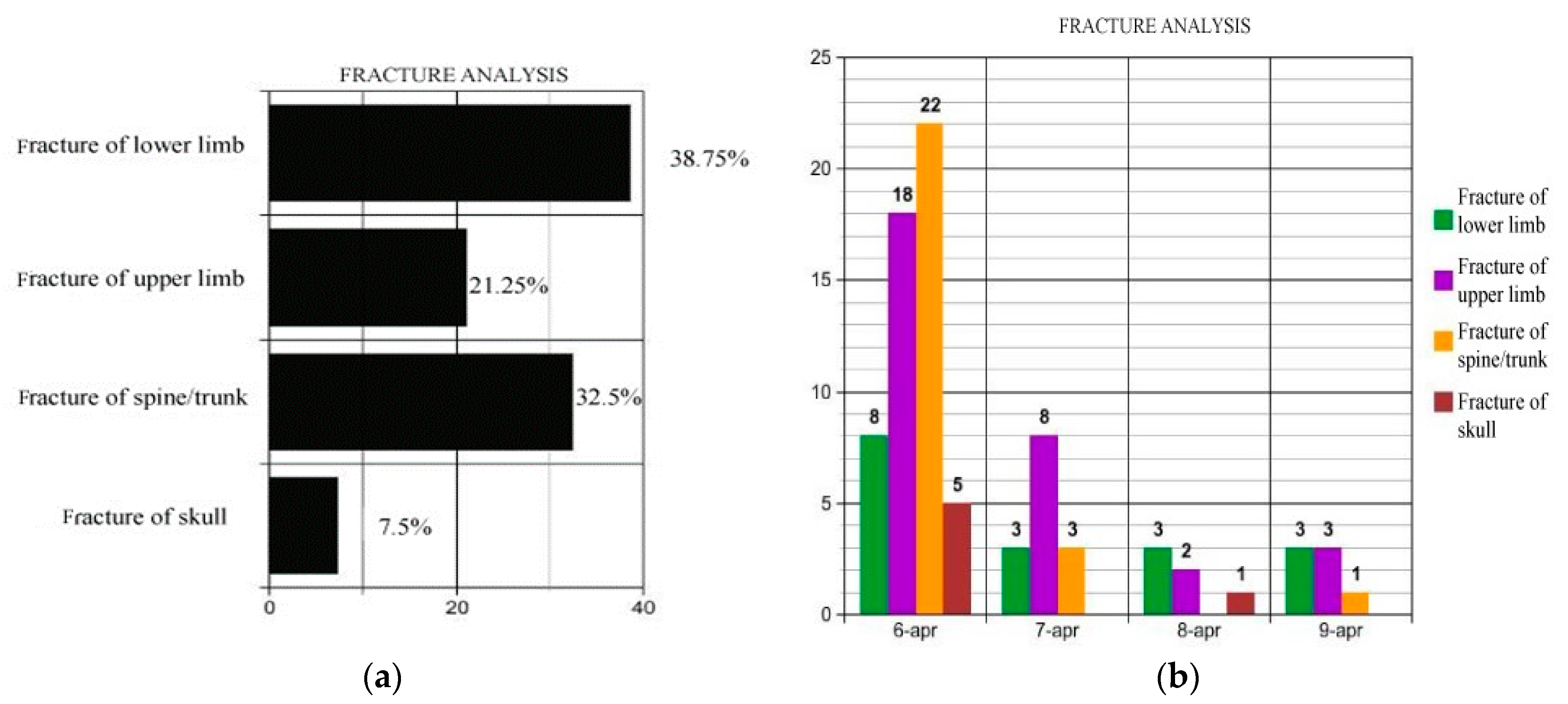
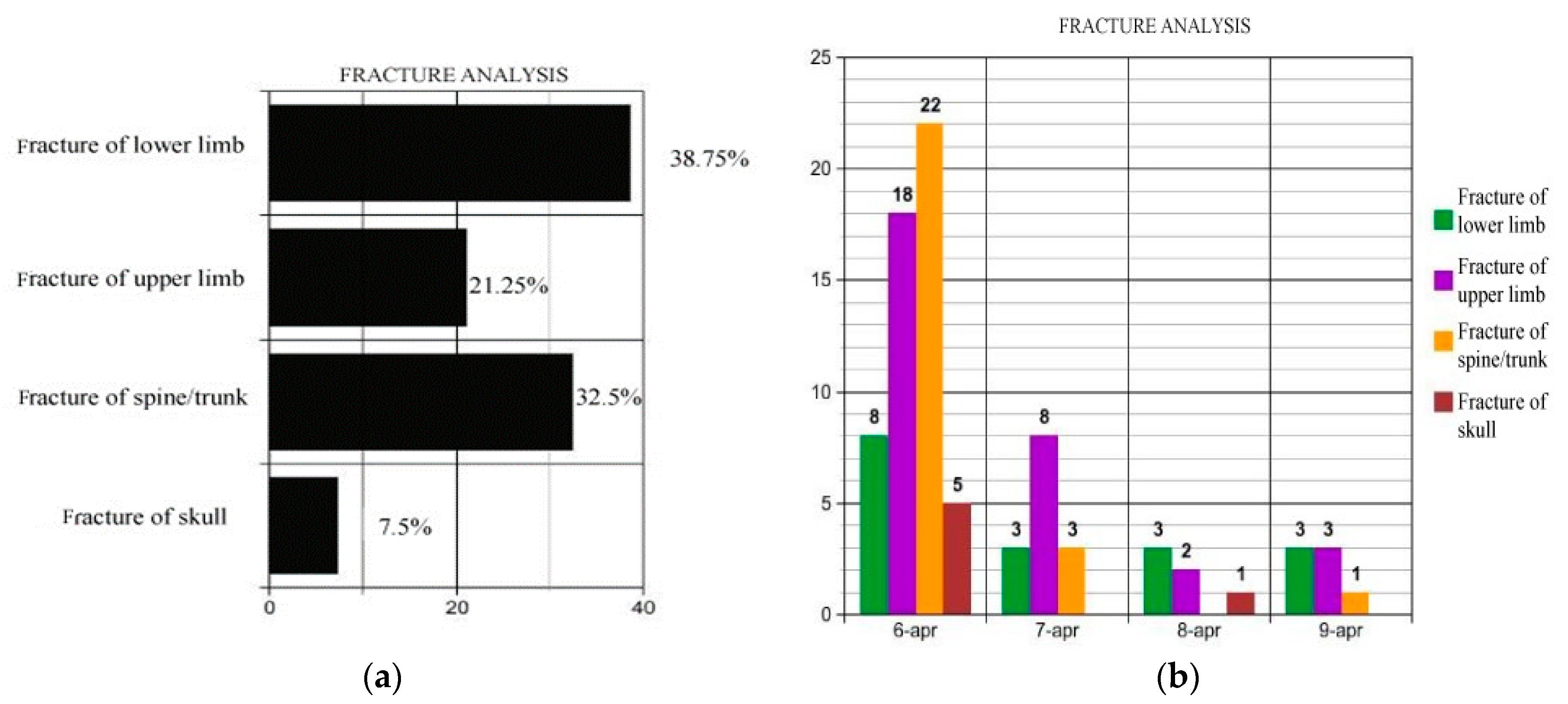
On 6 April 2009, approximately 50% of patients (
Table 1) were admitted to hospital with injury as principal diagnosis. This data highlights the importance of exploring injury patterns from major natural disasters, such as earthquakes, and the high number of medical response resources deployed to provide assistance to patients with similar needs. As in the Bam earthquake (Iran) [
25], fractures were the most common type of injury, with lower extremities being the major site of injury (ICD-9: 820–829), as also reported in the earthquakes that hit Yushu county (China) in 2010 [
20] and West Sumatra (Indonesia) in 2009 [
26]. Our review of the fractures classified by their anatomic locations show that the frequency rates and the average LOSs were higher for the fracture of lower limbs with ICD-9: 820–829 (38.8% and 11.5 days of average length of stay), and for fractures of spine and trunk with ICD-9: 805-–809 (32.5% and 18.4 days of average length of stay). Specifically, fractures of vertebral column and of femur were the most frequent injuries and with the longest LOS. Females sustained a higher rate of injuries than males (F:68.75% vs. M:31.25%—
Table 5).
Earthquake-related injuries were mostly caused by the collapse of buildings, like in the 2013 Lushan earthquake (China) [
21]. This finding is particularly relevant as it has been demonstrated that during an earthquake the incidence of certain injuries and the anatomic location of the fracture are related to the body posture and the activities the victims were performing when the disaster occurred [
20,
27]. During the day, victims are generally standing or sitting at the time of the disaster, therefore the most frequent observed fractures will involve the vertebral column. Conversely, if the disaster occurs during the night, as in the L’Aquila earthquake (03:32 a.m.), but also in Northridge, California (04:30 a.m. local time), Bam (05:26 a.m. local time), and in Hanshin-Awaji (05:46 a.m. local time), patients are lying in supine or lateral positions at the time of the earthquake, thus the lower extremities (including the pelvis) and the thoracic cage (both fractures and injuries) will be the most common injured sites [
28]. As it occurred in the 2011 Van earthquake (Turkey), also in L’Aquila more than 70% of the patients were admitted to hospitals on the first day [
1] through the deployment of regional and extra-regional rescue teams from the urgent and emergency care network. As highlighted by Schulz et al. [
29], the greatest demand for patient care occurs during the first 24 to 48 h after the disaster (maximum within 4 days after the mainshock). Indeed, the other 46 patients (26.90%) were admitted within the three days following 6 April. After the fifth day, the injury-related emergencies rapidly decreased, thus proving that immediate provision of emergency lifesaving care is fundamental [
30], as it occurred in L’Aquila as a result of a joint relief effort by the urgent care and medical emergency services.
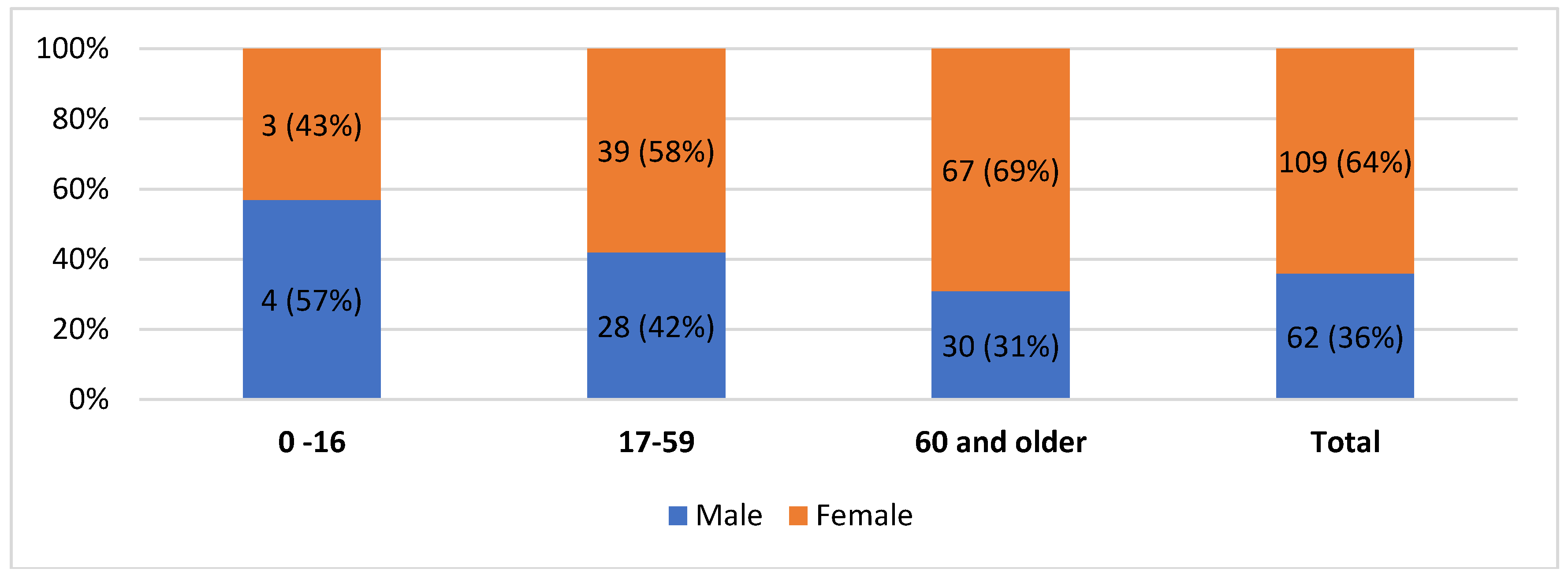
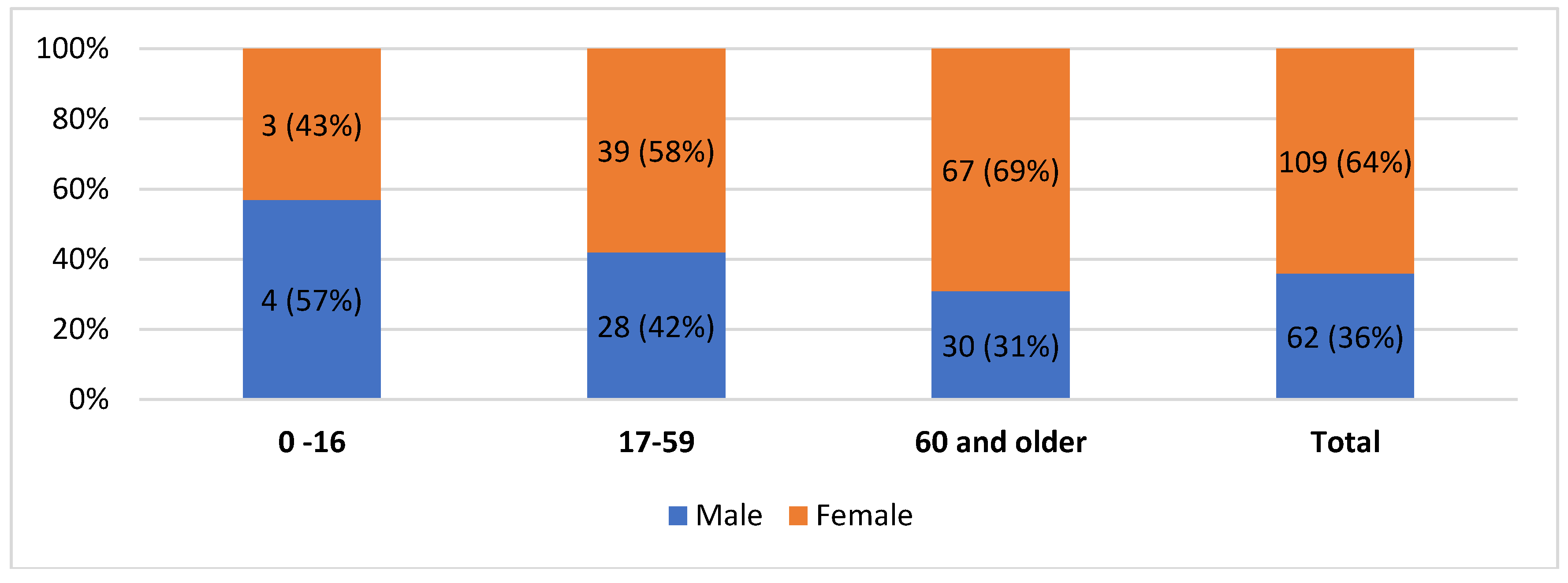
Further, the review of the medical records of patients admitted with an injury diagnosis highlighted a recurring injury pattern in the L’Aquila city earthquake: It outlined how females had almost a two times higher incidence of injuries than males (
Table 3, all injuries, 36% vs. 64%), whereas injuries in the period 2010–2016 occur in males and females with similar percentages (48% vs. 52%), which are inline—according to the National census data—with the gender distribution in the Abruzzo population (48.6% males and 51.4% females). A breakdown in terms of age groups actually shows a higher frequency of females than males in almost all age groups. However, the association is quite weak (V = 0.14) and therefore the age difference should be considered only a part of the explanation of such a high proportion. This point is also well substantiated by the literature review; most authors claim that women are more at risk for injury and death in earthquakes [
25,
31,
32]. Different studies have pointed out that there may be different approaches between males and females in dealing with a sudden catastrophic event, e.g., due to both traditional stereotyping or cognitive appraisal of threat, and our study seems to support this finding [
33,
34,
35].
This point concurs with our results that, in the L’Aquila earthquake, the most common fractures (femur and vertebral column) were accounted for by females, who also had longer median LOS (with a higher severity score), and half of the inpatients were older than 60 years at the time of admission to the hospital.
The paediatric population constituted only 4% of all inpatient admissions, differently from other earthquakes, such as the Kocaeli earthquake of 1999, in Turkey [
36], where the proportion of children who reported injuries was significantly higher.
Much of the extant literature has highlighted that multiple-injured patients are an important component of the injury pattern following earthquakes [
37], as, compared to the victims of large-scale disasters, they are at increased risk of suffering from disabilities, they require longer health care and injury-related surgical procedures that often may be difficult to perform immediately after the event [
21]. Our analysis revealed that in the L’Aquila earthquake, multiple-injured patients accounted for almost 50% of all admissions. However, 75% of them were admitted to the hospital within the 24 h after the earthquake [
29,
38]. Moreover, the ratio of females to males in this group was still approximately 2:1, with 66% of the patients being older than 60 years, and 28% with an age range between 17–59 years. The analysis of the median LOS of the multiple trauma patients (
Table 9) indicates an average LOS similar to those presenting with single injuries (11.2 days vs. 12.1 days). Furthermore, multiple-injured male patients had a longer average LOS than females (M:12.3 days vs. F:11.2 days); conversely, among the single-injury patients, females had a longer median LOS (M:11.5 days vs. F:12.4 days).
Although fracture-related admissions were the main cause in both periods (2009:46.8% vs. 2010–2016: 45.6%), the comparison with the period 2010–2016 shows that the average LOS for the fracture-related admissions was longer in 2009 (+2.9 days). Moreover, the types of injuries treated by the clinical surgery units after the earthquake had frequencies different from the average rates reported for the period 2010–2016: internal injury of thorax, abdomen, and pelvis (ICD-9: 860–869), +5.1%; intracranial injury (ICD-9: 850–854), +7.2%. These findings, if supported by further studies on the earthquakes occurring in Italy over the past years, have important implications for the regional and national health care system preparedness, in order to ensure the provision of critical public health and medical services during an earthquake, and the adequate clinical and surgical management of the injured (Preparedness).
Notwithstanding the overloading of health care delivery due to the immediate surge of injury-related admissions (
Table 1), compounded by the evacuation of the main hospital in L’Aquila, the analysis of the average LOS shows a longer-than-average LOS for surgery patients (12.11 days vs. 10 days). The median stay in hospital decreased progressively within the four days after the earthquake, with men spending an average of 1.5 days less in hospital than women, while average LOSs were longer as patient age increased (13.8 days of average LOS for adults aged older than 60 years compared to the 3.4 days reported for ages 0–16).
The analysis of patient discharge disposition and the comparison with 2010–2016 showed no significant difference between in-hospital mortality percentages (2009:1.8% vs. 2010–2016:1.3%). Discharges to patient’s home (no.2) decreased by 15%, while a rise was observed in the number of interhospital and intrahospital transfers for both acute and rehabilitation care (no.6–8) compared to 2010–2016. This highlights an increased need for health care and rehabilitation in the earthquake-related patients (possibly due to the severity of the injuries) with respect to the patients admitted in the years following the earthquake. Furthermore, a longer-than-average LOS is to be related to psychological trauma and to logistical difficulties due to the collapse or damage of buildings.

 ,
, 

{kind=link}
{kind=link}