Physical Activity and Sedentary Time in Active and Non-Active Adults with Intellectual Disability: A Comparative Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Procedures
2.3. Anthropometric Measurements
2.4. Physical Activity Level Measurements
2.5. Statistical Analysis
3. Results
3.1. Participants Characteristics, Anthropometrics, and PA Levels
3.2. Physical Activity and Sedentary Time Differences by Sex
3.3. Physical Activity and Sedentary Time Differences by Age
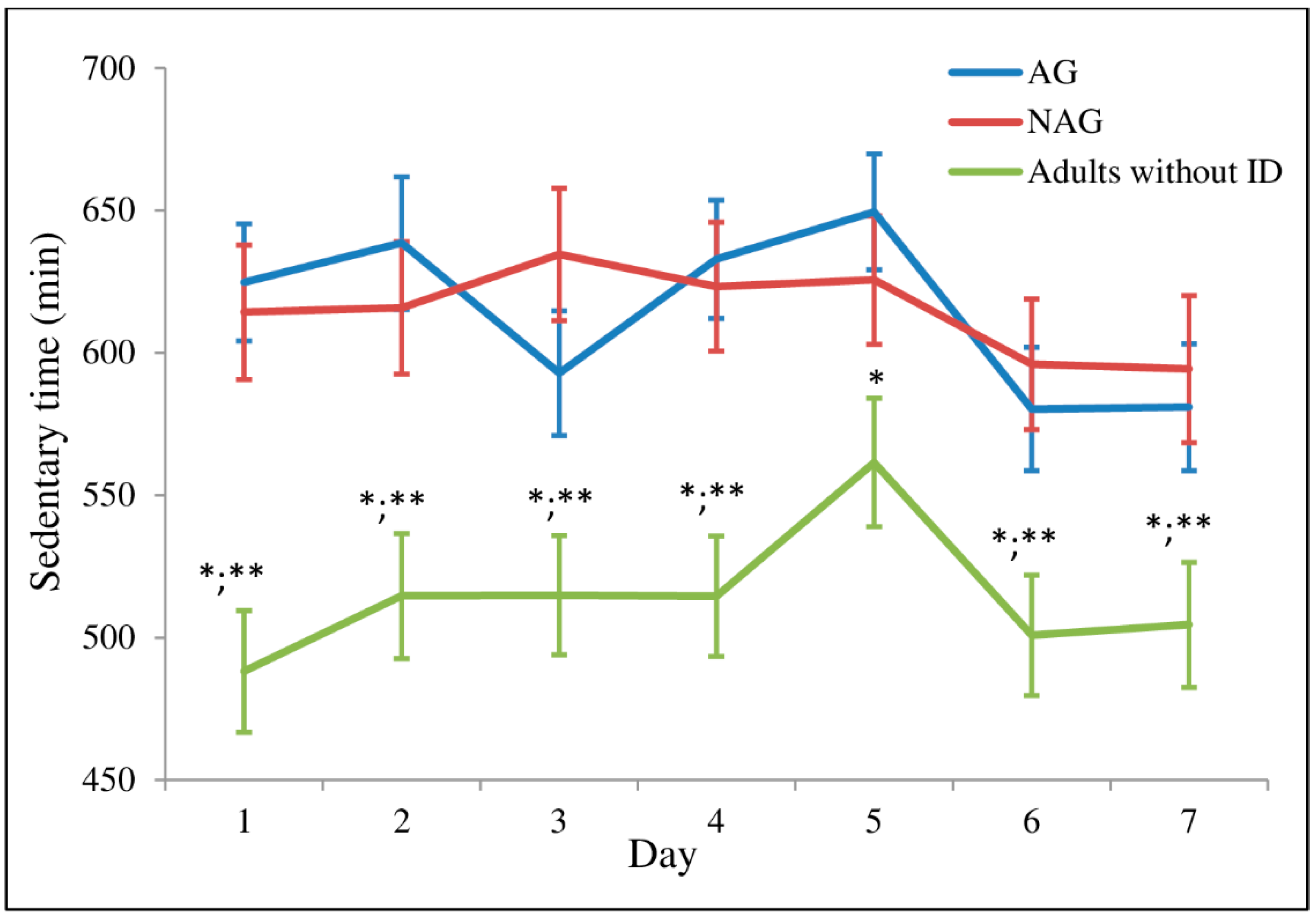
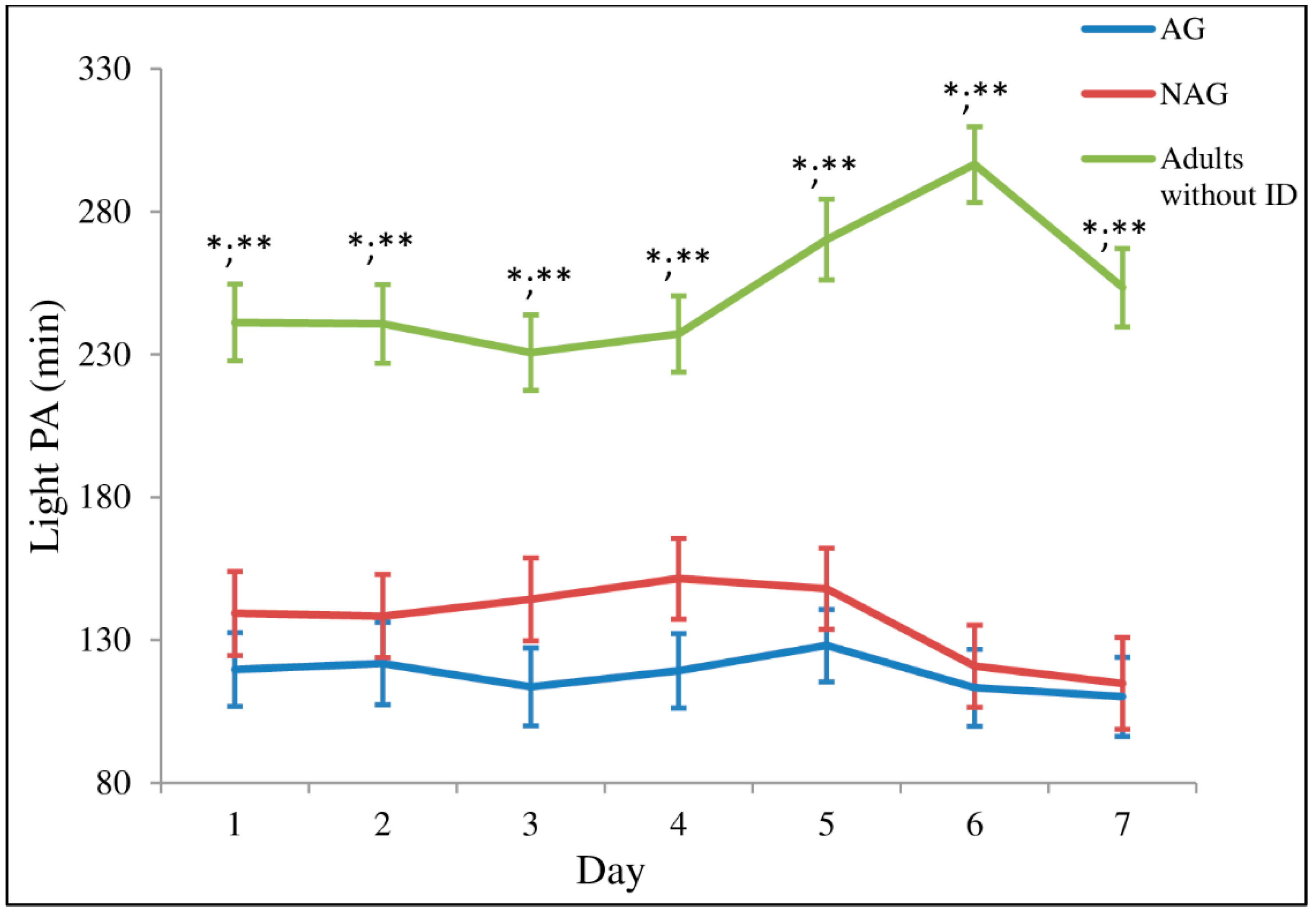
3.4. Physical Activity and Sedentary Time Throughout the Week
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription, 10th ed.; Lippincott Williams & Wilkins: Philapeldhia, PA, USA, 2017; ISBN 9781496339065. [Google Scholar]
- World Health Organization. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Kohl, H.W.; Craig, C.L.; Lambert, E.V.; Inoue, S.; Alkandari, J.R.; Leetongin, G.; Kahlmeier, S. The pandemic of physical inactivity: Global action for public health. Lancet 2012, 380, 294–305. [Google Scholar] [CrossRef]
- Esliger, D.W.; Tremblay, M.S. Establishing a profile of physical activity and inactivity: The next generation. Appl. Physiol. Nutr. Metab. 2007, 32, S217–S230. [Google Scholar] [CrossRef] [PubMed]
- Troiano, R.P.; Freedson, P.S. Promises and pitfalls of emerging measures of physical activity and the environment. Am. J. Prev. Med. 2010, 38, 682–683. [Google Scholar] [CrossRef] [PubMed]
- Eijsvogels, T.M.H.; George, K.P.; Thompson, P.D. Cardiovascular benefits and risks across the physical activity continuum. Curr. Opin. Cardiol. 2016, 31, 566–571. [Google Scholar] [CrossRef] [PubMed]
- Ortlieb, S.; Dias, A.; Gorzelniak, L.; Nowak, D.; Karrasch, S.; Peters, A.; Kuhn, K.; Horsch, A.; Schulz, H. Exploring patterns of accelerometry-assessed physical activity in elderly people. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 28. [Google Scholar] [CrossRef]
- Tremblay, M.S.; Aubert, S.; Barnes, J.D.; Saunders, T.J.; Carson, V.; Latimer-Cheung, A.E.; Chastin, S.F.M.; Altenburg, T.M.; Chinapaw, M.J.M.; Aminian, S.; et al. Sedentary Behavior Research Network (SBRN)—Terminology Consensus Project process and outcome. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 75. [Google Scholar] [CrossRef] [PubMed]
- De Rezende, L.F.M.; Rey-López, J.P.; Matsudo, V.K.R.; Luiz, O.D.C. Sedentary behavior and health outcomes among older adults: A systematic review. BMC Public Health 2014, 14, 333. [Google Scholar] [CrossRef]
- Schmid, D.; Ricci, C.; Baumeister, S.E.; Leitzmann, M.F. Replacing sedentary time with physical activity in relation to mortality. Med. Sci. Sport. Exerc. 2016, 48, 1312–1319. [Google Scholar] [CrossRef]
- Balogh, R.S.; Lake, J.K.; Lin, E.; Wilton, A.; Lunsky, Y. Disparities in diabetes prevalence and preventable hospitalizations in people with intellectual and developmental disability: A population-based study. Diabet. Med. 2015, 32, 235–242. [Google Scholar] [CrossRef]
- Day, S.M.; Strauss, D.J.; Shavelle, R.M.; Reynolds, R.J. Mortality and causes of death in persons with Down syndrome in California. Dev. Med. Child. Neurol. 2005, 47, 171–176. [Google Scholar] [CrossRef]
- Draheim, C.C. Cardiovascular disease prevalence and risk factors of persons with mental retardation. Ment. Retard. Dev. Disabil. Res. Rev. 2006, 12, 3–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Emerson, E.; Glover, G.; Hatton, C.; Wolstenholme, J. Trends in age-standardised mortality rates and life expectancy of people with learning disabilities in Sheffield over a 33-year period. Tizard Learn. Disabil. Rev. 2014, 19, 90–95. [Google Scholar] [CrossRef]
- Kim, J.-Y.; Yi, E.-S. Analysis of the relationship between physical activity and metabolic syndrome risk factors in adults with intellectual disabilities. J. Exerc. Rehabil. 2018, 14, 592–597. [Google Scholar] [CrossRef]
- Baynard, T.; Pitetti, K.H.; Guerra, M.; Unnithan, V.B.; Fernahall, B. Age-related changes in aerobic capacity in individuals with mental retardation: A 20-yr review. Med. Sci. Sports Exerc. 2008, 40, 1984–1989. [Google Scholar] [CrossRef] [PubMed]
- Dairo, Y.M.; Collett, J.; Dawes, H.; Oskrochi, G.R. Physical activity levels in adults with intellectual disabilities: A systematic review. Prev. Med. Rep. 2016, 4, 209–219. [Google Scholar] [CrossRef] [Green Version]
- Humphries, K.; Traci, M.A.; Seekins, T. Nutrition and adults with intellectual or developmental disabilities: Systematic literature review results. Intellect. Dev. Disabil. 2009, 47, 163–185. [Google Scholar] [CrossRef] [PubMed]
- Oviedo, G.R.; Travier, N.; Guerra-Balic, M. Sedentary and Physical Activity Patterns in Adults with Intellectual Disability. Int. J. Environ. Res. Public Health 2017, 14, 1027. [Google Scholar] [CrossRef]
- Cardol, M.; Rijken, M.; van Schrojenstein Lantman-de Valk, H. People with mild to moderate intellectual disability talking about their diabetes and how they manage. J. Intellect. Disabil. Res. 2012, 56, 351–360. [Google Scholar] [CrossRef]
- Kuijken, N.M.J.; Naaldenberg, J.; Nijhuis-van der Sanden, M.W.; van Schrojenstein-Lantman de Valk, H.M.J. Healthy living according to adults with intellectual disabilities: Towards tailoring health promotion initiatives. J. Intellect. Disabil. Res. 2016, 60, 228–241. [Google Scholar] [CrossRef]
- O’Leary, L.; Taggart, L.; Cousins, W. Healthy lifestyle behaviours for people with intellectual disabilities: An exploration of organizational barriers and enablers. J. Appl. Res. Intellect. Disabil. 2018, 31, 122–135. [Google Scholar] [CrossRef]
- Lin, J.-D.; Wu, C.-L.; Lin, P.-Y.; Lin, L.-P.; Chu, C.M. Early onset ageing and service preparation in people with intellectual disabilities: Institutional managers’ perspective. Res. Dev. Disabil. 2011, 32, 188–193. [Google Scholar] [CrossRef]
- World Health Organization. Ageing and Intellectual Disabilities—Improving Longevity and Promoting Healthy Ageing: Summative Report; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- Berjano Peirats, E.; García Burgos, E. Discapacidad Intelectual y Envejecimiento: Un Problema Social del Siglo XXI; FEAPS: Madrid, Spain, 2010. [Google Scholar]
- Melville, C.A.; Oppewal, A.; Schäfer Elinder, L.; Freiberger, E.; Guerra-Balic, M.; Hilgenkamp, T.I.M.; Einarsson, I.; Izquierdo-Gómez, R.; Sansano-Nadal, O.; Rintala, P.; et al. Definitions, measurement and prevalence of sedentary behaviour in adults with intellectual disabilities—A systematic review. Prev. Med. 2017, 97, 62–71. [Google Scholar] [CrossRef]
- Spain Royal Decree Law 1971/1999, December the 23th, Procedure for Recognition, Declaration and Qualification of the Degree of Disability. Available online: http://www.seg-social.es/Internet_1/Normativa/ 097360 (accessed on 30 November 2016).
- Troiano, R.P.; Berrigan, D.; Dodd, K.W.; Masse, L.C.; Tilert, T.; McDowell, M. Physical activity in the United States measured by accelerometer. Med. Sci. Sports Exerc. 2008, 40, 181–188. [Google Scholar] [CrossRef]
- Matthews, C.E.; Chen, K.Y.; Freedson, P.S.; Buchowski, M.S.; Beech, M.; Pate, R.R.; Troiano, R.P.; Beech, B.M. Amount of time spent in sedentary behaviors in the United States, 2003–2004. Am. J. Epidemiol. 2008, 167, 875–881. [Google Scholar] [CrossRef]
- Matthews, C.E.; Hagströmer, M.; Pober, D.M.; Bowles, H.R. Best practices for using physical activity monitors in population-based research. Med. Sci. Sport. Exerc. 2012, 44, S68–S76. [Google Scholar] [CrossRef]
- Berlin, J.E.; Storti, K.L.; Brach, J.S. Using activity monitors to measure physical activity in free-living conditions. Phys. Ther. 2006, 86, 1137–1145. [Google Scholar]
- Tudor-Locke, C.; Camhi, S.M.; Troiano, R.P. A catalog of rules, variables, and definitions applied to accelerometer data in the National Health and Nutrition Examination Survey, 2003–2006. Prev. Chronic Dis. 2012, 9, E113. [Google Scholar] [CrossRef]
- Finlayson, J.; Jackson, A.; Cooper, S.; Morrison, J.; Melville, C.; Smiley, E.; Allan, L.; Mantry, D. Understanding predictors of low physical activity in adults with intellectual disabilities. J. Appl. Res. Intellect. Disabil. 2009, 22, 236–247. [Google Scholar] [CrossRef]
- Dixon-Ibarra, A.; Lee, M.; Dugala, A. Physical activity and sedentary behavior in older adults with intellectual disabilities: A comparative study. Adapt. Phys. Act. Q. 2013, 30, 1–19. [Google Scholar] [CrossRef]
- Melville, C.A.; McGarty, A.; Harris, L.; Hughes-McCormack, L.; Baltzer, M.; McArthur, L.A.; Morrison, J.; Allan, L.; Cooper, S.A. A population-based, cross-sectional study of the prevalence and correlates of sedentary behaviour of adults with intellectual disabilities. J. Intellect. Disabil. Res. 2018, 62, 60–71. [Google Scholar] [CrossRef]
- Shields, N.; Plant, S.; Warren, C.; Wollersheim, D.; Peiris, C. Do adults with Down syndrome do the same amount of physical activity as adults without disability? A proof of principle study. J. Appl. Res. Intellect. Disabil. 2018, 31, 459–465. [Google Scholar] [CrossRef] [PubMed]
- European Commission. Special Eurobarometer 472: Sport and Physical Activity. Available online: http://ec.europa.eu/commfrontoffice/publicopinion/index.cfm/survey/getsurveydetail/instruments/special/surveyky/2164#p=1&instruments=FLASH&surveyKy=2164 (accessed on 22 December 2018).
- Melville, C.A.; Boyle, S.; Miller, S.; Macmillan, S.; Penpraze, V.; Pert, C.; Spanos, D.; Matthews, L.; Robinson, N.; Murray, H.; et al. An open study of the effectiveness of a multi-component weight-loss intervention for adults with intellectual disabilities and obesity. Br. J. Nutr. 2011, 105, 1553. [Google Scholar] [CrossRef] [PubMed]
- Phillips, A.C.; Holland, A.J. Assessment of objectively measured physical activity levels in individuals with intellectual disabilities with and without Down’s syndrome. PLoS ONE 2011, 6, e28618. [Google Scholar] [CrossRef]
- Frey, G.C. Comparison of physical activity levels between adults with and without mental retardation. J. Phys. Act. Health 2004, 1, 235–245. [Google Scholar] [CrossRef]
- Powell, K.E.; Paluch, A.E.; Blair, S.N. Physical activity for health: What kind? How much? How intense? On top of what? Annu. Rev. Public Health 2011, 32, 349–365. [Google Scholar] [CrossRef]
- Ekelund, U.; Steene-Johannessen, J.; Brown, W.J.; Fagerland, M.W.; Owen, N.; Powell, K.E.; Bauman, A.; Lee, I.-M. Does physical activity attenuate, or even eliminate, the detrimental association of sitting time with mortality? A harmonised meta-analysis of data from more than 1 million men and women. Lancet 2016, 6736, 1–10. [Google Scholar] [CrossRef]
- Loprinzi, P.D.; Cardinal, B.J. Association Between Biologic Outcomes and Objectively Measured Physical Activity Accumulated in ≥ 10-Minute Bouts and < 10-Minute Bouts. Am. J. Heal. Promot. 2013, 27, 143–151. [Google Scholar]
- Loprinzi, P.D. Light-intensity physical activity and all-cause mortality. Am. J. Heal. Promot. 2017, 31, 340–342. [Google Scholar] [CrossRef] [PubMed]
- Carmeli, E.; Merrick, J.; Imam, B.; Levy, R. Exercises and sports participation in healthy older adults with intellectual disability—A pilot study. Health 2012, 4, 769–774. [Google Scholar] [CrossRef]
- Cartwright, L.; Reid, M.; Hammersley, R.; Walley, R.M. Barriers to increasing the physical activity of people with intellectual disabilities. Br. J. Learn. Disabil. 2017, 45, 47–55. [Google Scholar] [CrossRef]
- Ainsworth, B.E.; Haskell, W.L.; Herrmann, S.D.; Meckes, N.; Bassett, D.R.; Tudor-Locke, C.; Greer, J.L.; Vezina, J.; Whitt-Glover, M.C.; Leon, A.S. 2011 compendium of physical activities: A second update of codes and MET values. Med. Sci. Sports Exerc. 2011, 43, 1575–1581. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Level of ID | AG (n = 37) | NAG (n = 29) | p-Value |
|---|---|---|---|
| Participants with mild ID level | 11 | 7 | 0.613 |
| Participants with moderate ID level | 26 | 22 |
| Variables | Adults without ID (n = 31) | AG (n = 37) | NAG (n = 29) | F | p-Value |
|---|---|---|---|---|---|
| Characteristics ‡ | |||||
| Age (years) | 43 (11) | 41 (11) | 46 (12) | 1.657 | 0.196 |
| Gender (male/female) | 14/17 | 22/15 | 17/12 | ||
| Anthropometry ‡ | |||||
| Height (cm) * | 167.90 (7.79) | 160.43 (10.87) | 162.03 (9.30) | 4.241 | 0.017 |
| Weight (kg) | 73.64 (12.04) | 70.07 (13.55) | 74.24 (12.52) | 1.061 | 0.350 |
| BMI (kg/m2) | 26.08 (3.71) | 27.38 (5.00) | 28.56 (6.35) | 1.780 | 0.174 |
| PA data †; ‡‡ | |||||
| Total PA (counts·min−1) **; *** | 316.86 (78.71) | 306.86 (85.71) | 236.54 (107.90) | 6.701 | 0.002 |
| ST (min·day−1) *; ** | 513.71 (81.88) | 614.98 (106.77) | 615.04 (80.57) | 44.225 | <0.001 |
| LPA (min·day−1) *; ** | 252.39 (69.78) | 117.37 (39.57) | 136.69 (49.92) | 57.346 | <0.001 |
| MPA (min·day−1) *** | 33.92 (17.35) | 37.48 (26.29) | 25.26 (19.87) | 2.759 | 0.069 |
| VPA (min·day−1) *; *** | 0.69 (1.08) | 1.24 (0.99) | 0.67 (0.45) | 3.240 | 0.044 |
| MVPA (min·day−1) *** | 34.61 (17.08) | 38.72 (26.64) | 25.95 (20.58) | 2.929 | 0.059 |
| Sedentary bouts >1 min per day *; ** | 99.76 (23.64) | 123.34 (20.13) | 124.69 (20.79) | 6.636 | 0.002 |
| Sedentary breaks/sedentary hour | 11.26 (2.16) | 11.64 (1.80) | 12.37 (2.15) | 1.608 | 0.206 |
| Accelerometer wearing time (min·day−1) | 800.72 (76.14) | 771.08 (111.52) | 777.68 (73.10) | 0.886 | 0.416 |
| Variables | Adults Without ID | AG | NAG | F | p-Value | |||
|---|---|---|---|---|---|---|---|---|
| Males (n = 14) | Females (n = 17) | Males (n = 21) | Females (n = 14) | Males (n = 17) | Females (n = 11) | |||
| Total PA (counts·min−1) *; ***; † | 325.11 (74.24) | 310.06 (83.85) | 314.61 (96.18) | 295.24 (68.85) | 245.25 (126.56) | 223.09 (74.03) | 2.814 | 0.021 |
| ST (min·day−1) **** | 505.29 (57.93) | 520.65 (98.65) | 620.14 (100.49) | 607.23 (119.05) | 600.26 (86.47) | 637.87 (67.96) | 17.951 | <0.001 |
| LPA (min·day−1) **** | 234.14 (67.41) | 267.41 (70.05) | 121.51 (47.83) | 111.14 (22.48) | 140.64 (58.29) | 130.57 (35.01) | 23.251 | <0.001 |
| MPA (min·day−1) † | 33.93 (15.33) | 33.92 (19.33) | 43.49 (30.48) | 28.47 (15.24) | 24.72 (23.22) | 26.10 (14.22) | 1.746 | 0.133 |
| VPA (min·day−1) **; ††; ††† | 1.17 (1.83) | 0.29 (0.69) | 1.40 (1.12) | 1.00 (0.74) | 0.66 (.49) | 0.69 (0.39) | 2.824 | 0.021 |
| MVPA (min·day−1) † | 35.10 (14.31) | 34.21 (19.51) | 44.89 (30.79) | 29.47 (15.62) | 25.46 (24.07) | 26.70 (14.72) | 1.857 | 0.110 |
| Sedentary bouts >1 min per day **** | 98.47 (22.99) | 100.81 (25.87) | 124.16 (19.56) | 122.15 (21.58) | 125.60 (24.30) | 123.28 (17.81) | 2.593 | 0.031 |
| Sedentary breaks/sedentary hour | 11.86 (2.35) | 10.77 (1.93) | 11.41 (1.96) | 11.97 (1.57) | 12.33 (2.39) | 12.43 (4.21) | 1.038 | 0.400 |
| Accelerometer wearing time (min·day−1) | 794.55 (69.65) | 802.27 (76.39) | 786.56 (110.17) | 747.85 (116.77) | 766.77 (73.57) | 795.16 (72.24) | 1.183 | 0.324 |
| Variables | Adults Without ID | AG | NAG | F | p-Value | |||
|---|---|---|---|---|---|---|---|---|
| <40 years (n = 15) | ≥40 years (n = 16) | <40 years (n = 18) | ≥40 years (n = 17) | <40 years (n = 16) | ≥40 years (n = 12) | |||
| Total PA (counts·min−1) *; **; † | 335.53 (89.09) | 299.35 (65.63) | 329.79 (97.13) | 282.57 (66.07) | 242.74 (96.43) | 228.28 (125.56) | 3.546 | 0.006 |
| ST (min·day−1) *** | 497.76 (79.61) | 528.67 (83.67) | 601.01 (106.98) | 631.54 (87.09) | 617.61 (80.17) | 611.61 (84.54) | 18.731 | <0.001 |
| LPA (min·day−1) *** | 267.74 (60.69) | 237.99 (76.45) | 110.74 (39.62) | 124.38 (39.45) | 125.27 (45.35) | 151.91 (53.58) | 23.995 | <0.001 |
| MPA (min·day−1) | 36.72 (20.64) | 31.34 (13.47) | 40.69 (32.25) | 34.08 (18.44) | 27.93 (22.34) | 21.69 (16.27) | 2.115 | 0.071 |
| VPA (min·day−1) †; †† | 0.99 (1.76) | 0.36 (0.74) | 1.48 (0.90) | 0.99 (1.01) | 0.72 (0.45) | 0.62 (0.46) | 2.467 | 0.039 |
| MVPA (min·day−1) | 37.71 (20.79) | 31.71 (12.72) | 42.17 (32.41) | 35.07 (19.10) | 28.80 (23.19) | 22.15 (16.71) | 2.219 | 0.059 |
| Sedentary bouts >1 min per day *** | 94.04 (18.23) | 104.80 (26.60) | 115.04 (18.69) | 132.67 (17.87) | 120.69 (14.96) | 128.15 (24.79) | 4.240 | 0.002 |
| Sedentary breaks/sedentary hour | 11.17 (1.77) | 11.35 (2.53) | 11.79 (2.12) | 11.47 (1.41) | 12.09 (2.76) | 12.59 (3.33) | 1.467 | 0.209 |
| Accelerometer wearing time (min·day−1) | 803.22 (84.71) | 798.37 (69.89) | 753.53 (106.18) | 791.01 (112.80) | 771.69 (81.24) | 785.68 (63.21) | 1.357 | 0.239 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oviedo, G.R.; Tamulevicius, N.; Guerra-Balic, M. Physical Activity and Sedentary Time in Active and Non-Active Adults with Intellectual Disability: A Comparative Study. Int. J. Environ. Res. Public Health 2019, 16, 1761. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16101761
Oviedo GR, Tamulevicius N, Guerra-Balic M. Physical Activity and Sedentary Time in Active and Non-Active Adults with Intellectual Disability: A Comparative Study. International Journal of Environmental Research and Public Health. 2019; 16(10):1761. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16101761
Chicago/Turabian StyleOviedo, Guillermo R., Nauris Tamulevicius, and Myriam Guerra-Balic. 2019. "Physical Activity and Sedentary Time in Active and Non-Active Adults with Intellectual Disability: A Comparative Study" International Journal of Environmental Research and Public Health 16, no. 10: 1761. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16101761