Pilot Testing of a Patient Decision Aid for Adolescents with Severe Obesity in US Pediatric Weight Management Programs within the COMPASS Network

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Procedures
2.2. Measures
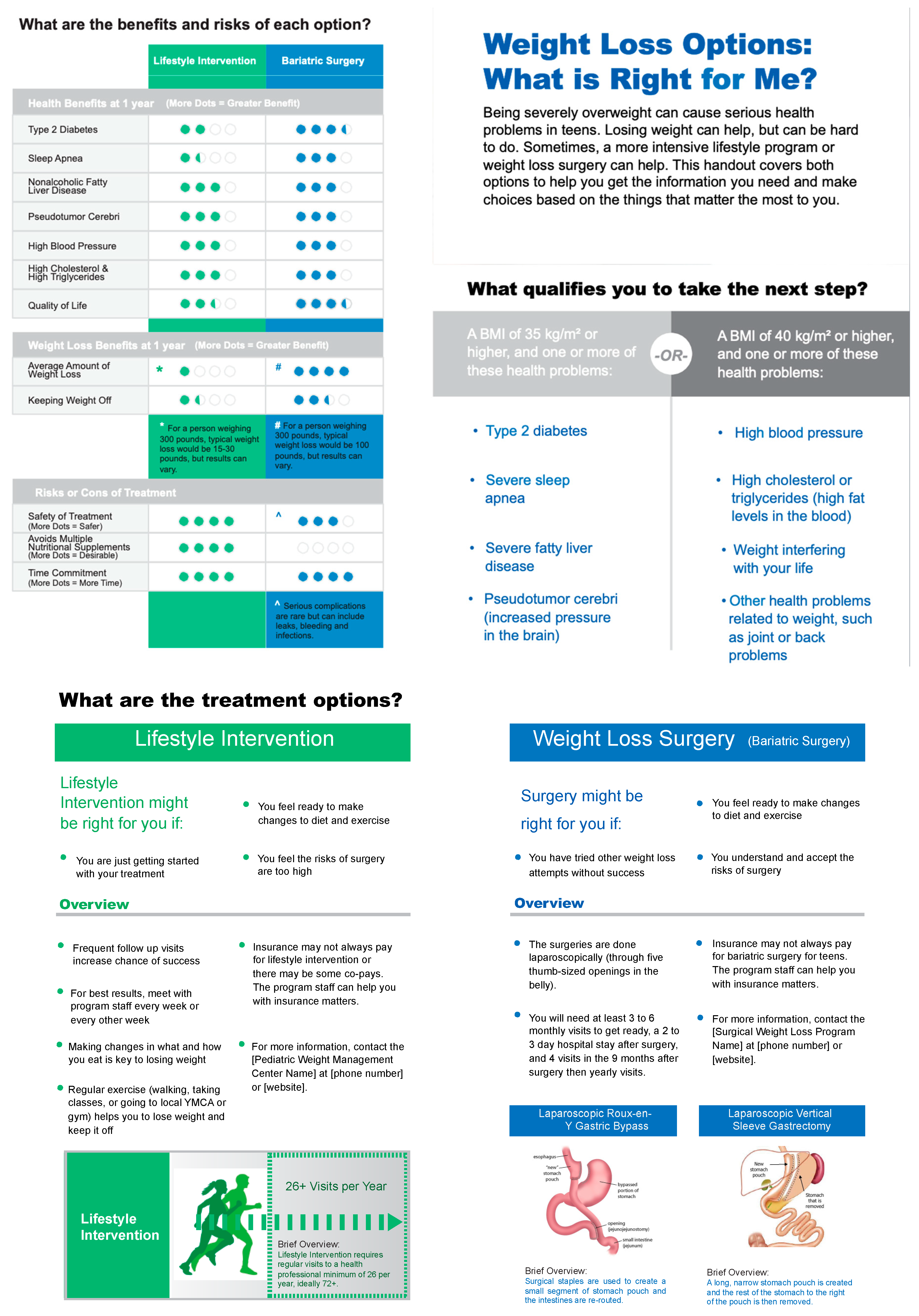
2.2.1. Patient Decision Aid
2.2.2. Patient/Family Survey
2.2.3. Provider Feedback Questionnaire
2.3. Analysis
3. Results
3.1. Missing Data
3.2. Patient/Family Survey Responses
3.3. Feasibility and Acceptability among Medical Providers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Skinner, A.C.; Ravanbakht, S.N.; Skelton, J.A.; Perrin, E.M.; Armstrong, S.C. Prevalence of Obesity and Severe Obesity in US Children, 1999–2016. Pediatrics 2018, 141, e20173459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelly, A.S.; Barlow, S.E.; Rao, G.; Inge, T.H.; Hayman, L.L.; Steinberger, J.; Urbina, E.M.; Ewing, L.J.; Daniels, S.R. American Heart Association Atherosclerosis, Hypertension, and Obesity in the Young Committee of the Council on Cardiovascular Disease in the Young, Council on Nutrition, Physical Activity and Metabolism, and Council on Clinical Cardiology. Severe obesity in children and adolescents: Identification, associated health risks, and treatment approaches: A scientific statement from the American Heart Association. Circulation 2013, 128, 1689–1712. [Google Scholar] [PubMed]
- Freedman, D.S.; Mei, Z.; Srinivasan, S.R.; Berenson, G.S.; Dietz, W.H. Cardiovascular risk factors and excess adiposity among overweight children and adolescents: The Bogalusa Heart Study. J. Pediatr. 2007, 150, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Pont, S.J.; Puhl, R.; Cook, S.R.; Slusser, W. Section on Obesity; Obesity Society. Stigma Experienced by Children and Adolescents with Obesity. Pediatrics 2017, 140, e20173034. [Google Scholar] [CrossRef]
- Fontaine, K.R.; Redden, D.T.; Wang, C.; Westfall, A.O.; Allison, D.B. Years of life lost due to obesity. JAMA 2003, 289, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Al-Khudairy, L.; Loveman, E.; Colquitt, J.L.; Mead, E.; Johnson, R.E.; Fraser, H.; Olajide, J.; Murphy, M.; Velho, R.M.; O’Malley, C.; et al. Diet, physical activity and behavioural interventions for the treatment of overweight or obese adolescents aged 12 to 17 years. Cochrane Database Syst. Rev. 2017, 6, CD012691. [Google Scholar] [CrossRef]
- Inge, T.H.; Courcoulas, A.P.; Jenkins, T.M.; Michalsky, M.P.; Helmrath, M.A.; Brandt, M.L.; Harmon, C.M.; Zeller, M.H.; Chen, M.K.; Xanthakos, S.A.; et al. Weight Loss and Health Status 3 Years after Bariatric Surgery in Adolescents. N. Engl. J. Med. 2016, 374, 113–123. [Google Scholar] [CrossRef]
- Olbers, T.; Beamish, A.J.; Gronowitz, E.; Flodmark, C.-E.; Dahlgren, J.; Bruze, G.; Ekbom, K.; Friberg, P.; Göthberg, G.; Järvholm, K.; et al. Laparoscopic Roux-en-Y gastric bypass in adolescents with severe obesity (AMOS): A prospective, 5-year, Swedish nationwide study. Lancet Diabetes Endocrinol. 2017, 5, 174–183. [Google Scholar] [CrossRef]
- Inge, T.H.; Jenkins, T.M.; Xanthakos, S.A.; Dixon, J.B.; Daniels, S.R.; Zeller, M.H.; Helmrath, M.A. Long-term outcomes of bariatric surgery in adolescents with severe obesity (FABS-5+): A prospective follow-up analysis. Lancet Diabetes Endocrinol. 2017, 5, 165–173. [Google Scholar] [CrossRef]
- Colquitt, J.L.; Pickett, K.; Loveman, E.; Frampton, G.K. Surgery for weight loss in adults. Cochrane Database Syst. Rev. 2014, 8, CD003641. [Google Scholar] [CrossRef]
- Bureau, U.S.C. American FactFinder—Results. Available online: https://factfinder.census.gov/faces/tableservices/jsf/pages/productview.xhtml?pid=PEP_2017_PEPSYASEX&prodType=table (accessed on 12 December 2018).
- Pratt, J.S.A.; Browne, A.; Browne, N.T.; Bruzoni, M.; Cohen, M.; Desai, A.; Inge, T.; Linden, B.C.; Mattar, S.G.; Michalsky, M.; et al. ASMBS pediatric metabolic and bariatric surgery guidelines, 2018. Surg. Obes. Relat. Dis. 2018, 14, 882–901. [Google Scholar] [CrossRef] [PubMed]
- Campoverde Reyes, K.J.; Misra, M.; Lee, H.; Stanford, F.C. Weight Loss Surgery Utilization in Patients Aged 14–25 with Severe Obesity among Several Healthcare Institutions in the United States. Front. Pediatr. 2018, 6, 251. [Google Scholar] [CrossRef] [PubMed]
- Zwintscher, N.P.; Azarow, K.S.; Horton, J.D.; Newton, C.R.; Martin, M.J. The increasing incidence of adolescent bariatric surgery. J. Pediatr. Surg. 2013, 48, 2401–2407. [Google Scholar] [CrossRef] [PubMed]
- Childerhose, J.E.; Eneli, I.; Steele, K.E. Adolescent bariatric surgery: A qualitative exploratory study of US patient perspectives. Clin. Obes. 2018, 8, 345–354. [Google Scholar] [CrossRef] [PubMed]
- Charles, C.; Gafni, A.; Whelan, T. Decision-making in the physician-patient encounter: Revisiting the shared treatment decision-making model. Soc. Sci. Med. 1999, 49, 651–661. [Google Scholar] [CrossRef]
- Dwamena, F.; Holmes-Rovner, M.; Gaulden, C.M.; Jorgenson, S.; Sadigh, G.; Sikorskii, A.; Lewin, S.; Smith, R.C.; Coffey, J.; Olomu, A. Interventions for providers to promote a patient-centred approach in clinical consultations. Cochrane Database Syst. Rev. 2012, 12, CD003267. [Google Scholar] [CrossRef]
- Stacey, D.; Légaré, F.; Lewis, K.; Barry, M.J.; Bennett, C.L.; Eden, K.B.; Holmes-Rovner, M.; Llewellyn-Thomas, H.; Lyddiatt, A.; Thomson, R.; et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst. Rev. 2017, 4, CD001431. [Google Scholar] [CrossRef]
- Volk, R.J.; Llewellyn-Thomas, H.; Stacey, D.; Elwyn, G. Ten years of the International Patient Decision Aid Standards Collaboration: Evolution of the core dimensions for assessing the quality of patient decision aids. BMC Med. Inform. Decis. Mak. 2013, 13 (Suppl. S20), S1. [Google Scholar] [CrossRef]
- Shared Decision Making | Evidence-Based Decision Making | Anderson Center. Available online: https://www.cincinnatichildrens.org/service/j/anderson-center/evidence-based-care/shared (accessed on 23 December 2018).
- Barlow, S.E. Expert Committee. Expert committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: Summary report. Pediatrics 2007, 120 (Suppl. S4), S164–S192. [Google Scholar] [CrossRef]
- Coulter, A.; Stilwell, D.; Kryworuchko, J.; Mullen, P.D.; Ng, C.J.; van der Weijden, T. A systematic development process for patient decision aids. BMC Med. Inform. Decis. Mak. 2013, 13 (Suppl. S2), S2. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, A.S.; Sepucha, K.R.; Abhyankar, P.; Sheridan, S.; Bekker, H.; LeBlanc, A.; Levin, C.; Ropka, M.; Shaffer, V.; Stacey, D.; et al. Explanation and elaboration of the Standards for UNiversal reporting of patient Decision Aid Evaluations (SUNDAE) guidelines: Examples of reporting SUNDAE items from patient decision aid evaluation literature. BMJ Qual. Saf. 2018, 27, 389–412. [Google Scholar] [CrossRef]
- Brinkman, W.B.; Hartl, J.; Rawe, L.M.; Sucharew, H.; Britto, M.T.; Epstein, J.N. Physicians’ shared decision-making behaviors in attention-deficit/hyperactivity disorder care. Arch. Pediatr. Adolesc. Med. 2011, 165, 1013–1019. [Google Scholar] [CrossRef]
- Brinkman, W.B.; Hartl Majcher, J.; Poling, L.M.; Shi, G.; Zender, M.; Sucharew, H.; Britto, M.T.; Epstein, J.N. Shared decision-making to improve attention-deficit hyperactivity disorder care. Patient Educ. Couns. 2013, 93, 95–101. [Google Scholar] [CrossRef] [Green Version]
- Elwyn, G.; Lloyd, A.; Joseph-Williams, N.; Cording, E.; Thomson, R.; Durand, M.-A.; Edwards, A. Option Grids: Shared decision making made easier. Patient Educ. Couns. 2013, 90, 207–212. [Google Scholar] [CrossRef]
- Styne, D.M.; Arslanian, S.A.; Connor, E.L.; Farooqi, I.S.; Murad, M.H.; Silverstein, J.H.; Yanovski, J.A. Pediatric Obesity-Assessment, Treatment, and Prevention: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2017, 102, 709–757. [Google Scholar] [CrossRef]
- Kelly, A.S.; Fox, C.K.; Rudser, K.D.; Gross, A.C.; Ryder, J.R. Pediatric obesity pharmacotherapy: Current state of the field, review of the literature and clinical trial considerations. Int. J. Obes. 2016, 40, 1043–1050. [Google Scholar] [CrossRef]
- State Medical Board of Ohio State Medical Board of Ohio: FAQs Regarding Short-Term Weight Loss Anorexiants 2015. Available online: https://www.pharmacy.ohio.gov/Documents/Pubs/Special/ControlledSubstances/Short-term%20Weight%20Loss%20Anorexiants%20FAQ.pdf (accessed on 10 April 2019).
- Srivastava, G.; Fox, C.K.; Kelly, A.S.; Jastreboff, A.M.; Browne, A.F.; Browne, N.T.; Pratt, J.S.A.; Bolling, C.; Michalsky, M.P.; Cook, S.; et al. Clinical Considerations Regarding the Use of Obesity Pharmacotherapy in Adolescents with Obesity. Obesity 2019, 27, 190–204. [Google Scholar] [CrossRef]
- Elwyn, G.; Barr, P.J.; Grande, S.W.; Thompson, R.; Walsh, T.; Ozanne, E.M. Developing CollaboRATE: A fast and frugal patient-reported measure of shared decision making in clinical encounters. Patient Educ. Couns. 2013, 93, 102–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barr, P.J.; Thompson, R.; Walsh, T.; Grande, S.W.; Ozanne, E.M.; Elwyn, G. The psychometric properties of CollaboRATE: A fast and frugal patient-reported measure of the shared decision-making process. J. Med. Internet Res. 2014, 16, e2. [Google Scholar] [CrossRef] [PubMed]
- Forcino, R.C.; Barr, P.J.; O’Malley, A.J.; Arend, R.; Castaldo, M.G.; Ozanne, E.M.; Percac-Lima, S.; Stults, C.D.; Tai-Seale, M.; Thompson, R.; et al. Using CollaboRATE, a brief patient-reported measure of shared decision making: Results from three clinical settings in the United States. Health Expect 2018, 21, 82–89. [Google Scholar] [CrossRef]
- Sepucha, K.R.; Borkhoff, C.M.; Lally, J.; Levin, C.A.; Matlock, D.D.; Ng, C.J.; Ropka, M.E.; Stacey, D.; Joseph-Williams, N.; Wills, C.E.; et al. Establishing the effectiveness of patient decision aids: Key constructs and measurement instruments. BMC Med. Inform. Decis. Mak. 2013, 13 (Suppl. S2), S12. [Google Scholar] [CrossRef]
- O’Connor, A.M. Validation of a decisional conflict scale. Med. Decis. Mak. 1995, 15, 25–30. [Google Scholar] [CrossRef]
- Kebbe, M.; Perez, A.; Ball, G.D.C. Is there a role for shared decision-making in pediatric weight management? Obes. Res. Clin. Pract. 2018, 12, 246–248. [Google Scholar] [CrossRef]
- Arterburn, D.E.; Westbrook, E.O.; Bogart, T.A.; Sepucha, K.R.; Bock, S.N.; Weppner, W.G. Randomized trial of a video-based patient decision aid for bariatric surgery. Obesity 2011, 19, 1669–1675. [Google Scholar] [CrossRef]
- Ogden, C.L.; Fryar, C.D.; Hales, C.M.; Carroll, M.D.; Aoki, Y.; Freedman, D.S. Differences in Obesity Prevalence by Demographics and Urbanization in US Children and Adolescents, 2013–2016. JAMA 2018, 319, 2410–2418. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Survey Question | Response Rate | Percentage “yes” or mean (SD) for questions on a 0–9 Likert scale 1 |
|---|---|---|
| 3. Did your clinician show you the shared decision-making tool during your visit? | 31/31 | 100% |
| 5. How much effort was made to help you understand your (child’s) health issues? | 28/31 | 8.6 (0.7) |
| 6. How much effort was made to listen to the things that matter most to you about your (child’s) health issues? | 28/31 | 8.8 (0.4) |
| 7. How much effort was made to include what matters most to you in choosing what to do next? | 28/31 | 8.7 (0.5) |
| 8. Did you discuss intensive lifestyle changes to treat your (child’s) weight? | 27/31 | 100% |
| 9. Did you discuss bariatric surgery (surgical weight loss) to treat your (child’s) weight? | 28/31 | 100% |
| 10. Do you know the benefits and risks of each option? | 28/31 | 96% |
| 11. Are you clear about which benefits and risks matter most to you and your child? | 28/31 | 96% |
| 12. Do you have enough support and advice to make a choice? | 28/31 | 93% |
| 13. Do you feel sure about the best choice for you (your child)? | 28/31 | 89% |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moore, J.; Haemer, M.; Mirza, N.; Z Weatherall, Y.; Han, J.; Mangarelli, C.; Hawkins, M.J.; Xanthakos, S.; Siegel, R. Pilot Testing of a Patient Decision Aid for Adolescents with Severe Obesity in US Pediatric Weight Management Programs within the COMPASS Network. Int. J. Environ. Res. Public Health 2019, 16, 1776. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16101776
Moore J, Haemer M, Mirza N, Z Weatherall Y, Han J, Mangarelli C, Hawkins MJ, Xanthakos S, Siegel R. Pilot Testing of a Patient Decision Aid for Adolescents with Severe Obesity in US Pediatric Weight Management Programs within the COMPASS Network. International Journal of Environmental Research and Public Health. 2019; 16(10):1776. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16101776
Chicago/Turabian StyleMoore, Jaime, Matthew Haemer, Nazrat Mirza, Ying Z Weatherall, Joan Han, Caren Mangarelli, Mary Jane Hawkins, Stavra Xanthakos, and Robert Siegel. 2019. "Pilot Testing of a Patient Decision Aid for Adolescents with Severe Obesity in US Pediatric Weight Management Programs within the COMPASS Network" International Journal of Environmental Research and Public Health 16, no. 10: 1776. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16101776