Parenting Stress and Broader Phenotype in Parents of Children with Attention Deficit Hyperactivity Disorder, Dyslexia or Typical Development


Abstract
:1. Introduction
1.1. Dyslexia and ADHD: Two Common and Often Comorbid Neurodevelopmental Disorders
1.2. The Broader Phenotypes of ADHD and Dyslexia
1.3. Parenting Stress in Parents of Children with ADHD or Dyslexia
1.4. The Present Study
- (1)
- To investigate group differences in cognitive and behavioral indexes of reading and attention impairments comparing three groups of parents: parents of children with ADHD (P-ADHD), parents of children with developmental dyslexia (P-DYS) and parents of children with typical development (P-TD). This first objective was intended to verify if the three groups of parents did indeed show endophenotypic patterns specific for their offspring developmental profile. Based on the literature review, P-DYS are expected to fail in reading related measures, whereas P-ADHD are expected to differ compared to the other groups in ANT task and in behavioural scales assessing ADHD symptoms in adulthood. Differences between mothers and fathers will be considered.
- (2)
- To investigate group differences in parenting stress. Based on previous studies higher levels of parenting stress have been reported for parents of children with dyslexia and parents of children with ADHD compared to parents of typically developing children. We therefore expect replying these findings and evaluating, for the first time, differences in parenting stress between parents of children with dyslexia or ADHD.
- (3)
- To analyse the relationships between cognitive indexes and parenting stress in the whole sample. Specifically, through a step-wise regression model the study aimed at evaluating which factors better predicted parental stress, an important index assessing parent-child interactions and known to correlate with parental styles. Cognitive measures are expected to significantly predict parenting stress, based on the assumption that parenting stress depends on parents’ ability to cope cognitively with offspring’s requests.
2. Methods
2.1. Participants
2.2. Measures
2.2.1. Background Information
2.2.2. Cognitive Measures
- (1)
- Kaufman Brief Intelligence Test-2. ([42]; Italian version adapted and standardized by [43]). This test assesses intellectual functioning and comprises Vocabulary (verbal knowledge and riddles) and Matrices subtests. It gives standardized measures of Verbal (VIQ), Performance (PIQ) and Composite Full Scale IQ.
- (2)
- Passage reading, taken from the “Reading tasks for the secondary schools” [44]. Participants were asked to read aloud a passage (729 words) and reading speed (syllables per second) and accuracy (number of errors) were recorded.
- (3)
- Non-word reading task, taken from the “Battery for the assessment of developmental dyslexia and dysorthographia” [45]. Participants are required to read aloud a list of 48 nonwords and reading speed (syllables per second) was recorded.
- (4)
- Semantic fluency: The participants were asked to produce as many words within the same semantic category (professions) in a test interval of 1 min.
- (5)
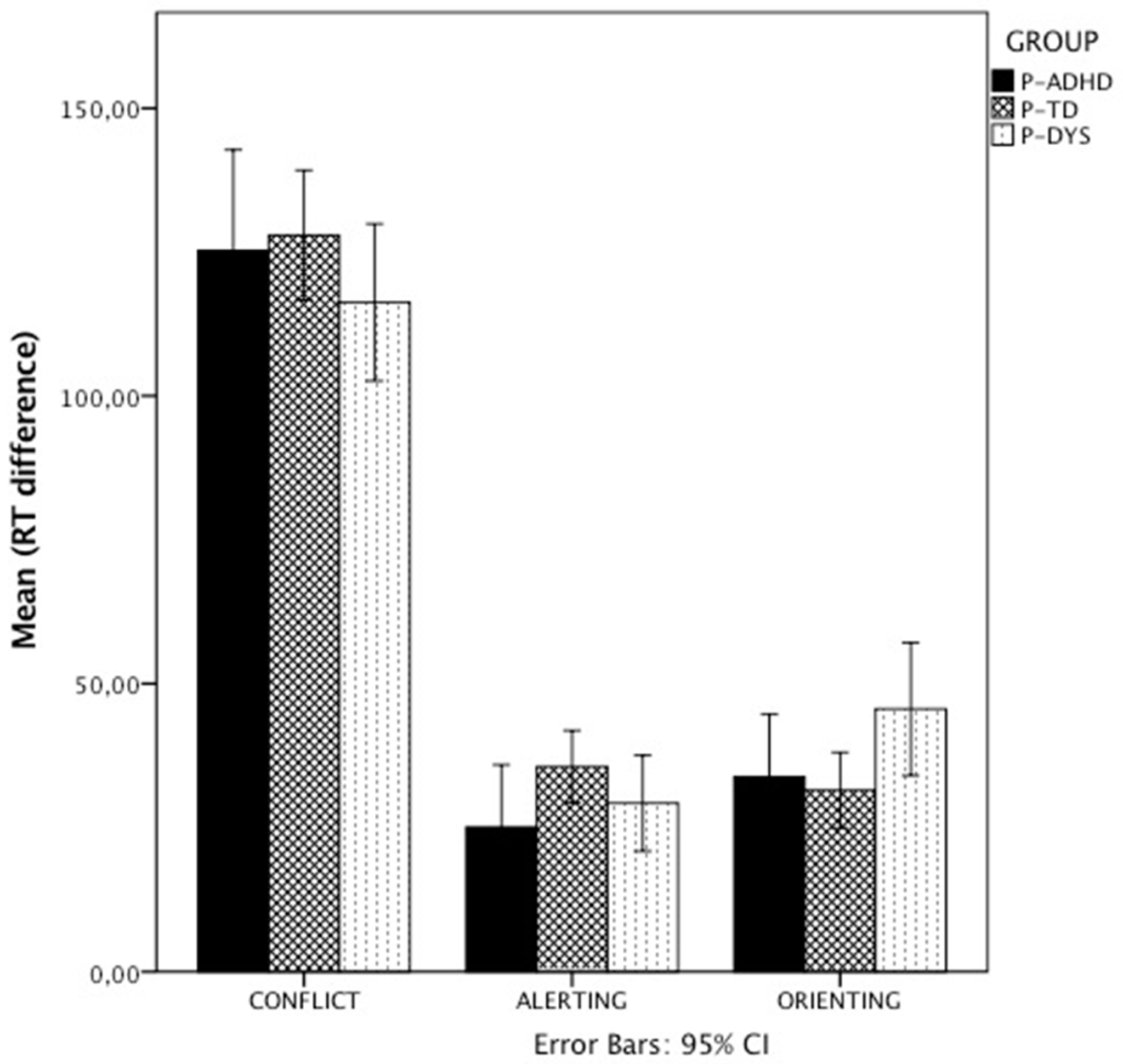
- Attentional Network Task (ANT) [13]. This task is a combination of a cue reaction time task, and a flanker task exploring attentional abilities divided into three components: executive control (conflict resolution), alerting and orienting. It requires participants to indicate whether a central arrow is oriented to the right or left. The arrow is presented between flanker arrows pointing either in the same direction (🡢🡢🡢🡢🡢; congruent condition) or in different directions (🡢🡢🡠🡢🡢; incongruent condition) from the target. Responses are expected to be slower for incongruent than for congruent conditions, showing that more cognitive effort is needed to resolve the conflict. The alerting component is explored by showing that faster responses occur when a cue is presented before the target stimulus compared to when it is not. Finally, orienting is studied by showing that responses are faster when a cue indicates the position of a target stimulus compared when it does not. The presentation of the stimuli was as follows: (a) a fixation point (+) appeared on the center of the screen for 400 ms; (b) a cue (*) was presented for 100 ms; (c) a fixation period was provided for 400 ms after the cue; (d) the target arrow and the flankers were presented simultaneously until the participant’s response or up to 1700 ms, (f) the target and flankers disappeared after response and the next trial began. Participants were instructed to focus on the fixation point and to respond by pressing a key on the computer keyboard, as quickly and accurately as possible, with their left hand when the arrow pointed to the left and with the right hand when it pointed to the right. A training phase consisting of 24 trials was administered.
2.3. Questionnaires
- (1)
- Adult Reading History Questionnaire-Revised (ARHQ-R) [46]: The ARHQ-R is aimed at evaluating the presence of a significant history of reading difficulties. Parents are required to respond to twenty-three questions on a five-point Likert scale (from 0 to 4), with higher values corresponding to more problems with reading skills, less print exposure, or poorer attitude towards reading. The participant’s score was calculated by dividing the total score by the maximum possible score (92). A score above 0.30 is indicative of a positive history of reading disorders.
- (2)
- Adult ADHD Self-Report Scale (ASRS-v1.1) Symptom Checklist. The Symptom Checklist is an instrument based on DSM-IV-TR criteria for ADHD, developed by World Health Organization (WHO). It includes 18 questions (e.g., How often do you have difficulty getting things in order when you have to do a task that requires organization?), based on a five points Likert-scale.
- (3)
- Parenting Stress Index (PSI) [33]. The PSI is addressed to the evaluation of parenting and family characteristics with the aim of identifying indexes of parental behavior problems and child adjustment difficulties within the family system. In this work we used the Italian PSI Short Form (PSI/SF), it includes 36 items (e.g., My son often wakes up in a bad mood) and yields a Total Stress score from three scales: Parental Distress, Parent-Child Dysfunctional Interaction, and Difficult Child. It also provides a Defensive Response scale. Higher scores are representative of higher levels of parenting stress.
2.4. Data Analysis
3. Results
3.1. Background Information
3.2. Cognitive Measures
3.3. Questionnaires
3.4. Regression Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Morton, J.; Frith, U. Causal modelling: A structural approach to developmental psychopathology. Manual Develop. Psychopathol. 1995, 1, 357–390. [Google Scholar]
- Westermann, G.; Mareschal, D.; Johnson, M.; Sirois, S.; Spratling, M.; Thomas, M. Neuroconstructivism. Dev. Sci. 2007, 10, 75–83. [Google Scholar] [CrossRef]
- van Bergen, E.; van der Leij, A.; de Jong, P.F. The intergenerational multiple deficit model and the case of dyslexia. Front. Hum. Neurosci. 2014, 8, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Snowling, M.J. Specific disorders and broader phenotypes: The case of dyslexia. Q. J. Exp. Psychol. 2008, 61, 142–156. [Google Scholar] [CrossRef] [PubMed]
- Gottesman, I.I.; Gould, T.D. The endophenotype concept in psychiatry: Etymology and strategic intentions. Am. J. Psychiatr. 2003, 160, 636–645. [Google Scholar] [CrossRef]
- Caspi, A.; Moffitt, T.E. Gene–environment interactions in psychiatry: Joining forces with neuroscience. Nat. Rev. Neurosci. 2006, 7, 583–590. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Pub: Washington, DC, USA, 2013. [Google Scholar]
- Vellutino, F.R.; Fletcher, J.M.; Snowling, M.J.; Scanlon, D.M. Specific reading disability (dyslexia): What have we learned in the past four decades? J. Child. Psychol. Psychiatry 2004, 45, 2–40. [Google Scholar] [CrossRef]
- Pennington, B.F. From single to multiple deficit models of developmental disorders. Cognition 2006, 101, 385–413. [Google Scholar] [CrossRef]
- Tressoldi, P.E.; Stella, G.; Faggella, M. The development of reading speed in Italians with dyslexia a longitudinal study. J. Learn. Disabil. 2001, 34, 414–417. [Google Scholar] [CrossRef]
- Karam, R.; Breda, V.; Picon, F.; Rovaris, D.; Victor, M.; Salgado, C.; Vitola, E.; Silva, K.L.; Guimarães-da-Silva, P.O.; Mota, N.R.; et al. Persistence and remission of ADHD during adulthood: A 7-year clinical follow-up study. Psychol. Med. 2015, 45, 2045–2056. [Google Scholar] [CrossRef] [PubMed]
- Castellanos, X.; Tannock, R. Neuroscience of attention-deficit/hyperactivity disorder: The search for endophenotypes. Nat. Rev. Neurosci. 2002, 3, 617–628. [Google Scholar] [CrossRef]
- Fan, J.; McCandliss, B.D.; Sommer, T.; Raz, A.; Posner, M.I. Testing the efficiency and independence of attentional networks. J. Cogn. Neurosci. 2002, 14, 340–347. [Google Scholar] [CrossRef]
- Fan, J.; Wu, Y.; Fossella, J.A.; Posner, M.I. Assessing the heritability of attentional networks. BMC Neurosci. 2001, 2, 1. [Google Scholar] [CrossRef]
- Johnson, K.A.; Robertson, I.H.; Barry, E.; Mulligan, A.; Dáibhis, A.; Daly, M.; Watchorn, A.; Gill, M.; Bellgrove, M.A. Impaired conflict resolution and alerting in children with ADHD: Evidence from the Attention Network Task (ANT). J. Child Psychol. Psychiatry 2008, 49, 1339–1347. [Google Scholar] [CrossRef]
- Thompson, P.; Hulme, C.; Nash, H.; Gooch, D.; Hayiou-Thomas, E.; Snowling, M. Developmental dyslexia: Predicting individual risk. J. Child Psychol. Psychiatry 2015, 56, 976–987. [Google Scholar] [CrossRef] [PubMed]
- Willcutt, E.; Betjemann, R.; McGrath, L.; Chhabildas, N.; Olson, R.; DeFries, J.; Pennington, B. Etiology and neuropsychology of comorbidity between RD and ADHD: The case for multiple-deficit models. Cortex 2010, 46, 1345–1361. [Google Scholar] [CrossRef] [Green Version]
- Pennington, B.F.; Lefly, D.L. Early reading development in children at family risk for dyslexia. Child Dev. 2001, 72, 816–833. [Google Scholar] [CrossRef]
- Snowling, M.J.; Gallagher, A.M.; Frith, U. Family risk of dyslexia is continuous: Individual differences in the precursors of reading skill. Child Dev. 2003, 74, 358–373. [Google Scholar] [CrossRef]
- Biederman, J.; Faraone, S.V.; Mick, E.; Spencer, T.; Wilens, T.; Keily, K.; Guite, J.; Ablon, J.S.; Reed, E.; Warburton, R. High risk for attention deficit hyperactivity disorder among children of parents with childhood onset of the disorder: A pilot study. Am. J. Psychiatry 1995, 152, 431–435. [Google Scholar]
- Cuevas, K.; Deater-Deckard, K.; Kim-Spoon, J.; Wang, Z.; Morasch, K.C.; Bell, M.A. A longitudinal intergenerational analysis of executive functions during early childhood. Br. J. Dev. Psychol. 2014, 32, 50–64. [Google Scholar] [CrossRef] [PubMed]
- Goos, L.M.; Crosbie, J.; Payne, S.; Schachar, R. Validation and extension of the endophenotype model in ADHD patterns of inheritance in a family study of inhibitory control. Am. J. Psychiatry 2009, 166, 711–717. [Google Scholar] [CrossRef] [PubMed]
- Nigg, J.T.; Blaskey, L.G.; Stawicki, J.A.; Sachek, J. Evaluating the endophenotype model of ADHD neuropsychological deficit: Results for parents and siblings of children with ADHD combined and inattentive subtypes. J. Abnorm. Psychol. 2004, 11, 614–625. [Google Scholar] [CrossRef]
- Thissen, A.; Rommelse, N.; Hoekstra, P.; Hartman, C.; Heslenfeld, D.; Luman, M.; Lieshout, M.; Franke, B.; Oosterlaan, J.; Buitelaar, J.K. Attention deficit hyperactivity disorder (ADHD) and executive functioning in affected and unaffected adolescents and their parents: Challenging the endophenotype construct. Psychol. Med. 2013, 44, 881–892. [Google Scholar] [CrossRef]
- Rommelse, N.; Arias-Vásquez, A.; Altink, M.; Buschgens, C.; Fliers, E.; Asherson, P.; Faraone, S.; Buitelaar, J.K.; Sergeant, J.A.; Oosterlaan, J.; et al. Neuropsychological Endophenotype Approach to Genome-wide Linkage Analysis Identifies Susceptibility Loci for ADHD on 2q21.1 and 13q12.11. Am. J. Hum. Genet. 2008, 83, 99–105. [Google Scholar] [CrossRef] [Green Version]
- Bitsakou, P.; Psychogiou, L.; Thompson, M.; Sonuga-Barke, E.J. Delay aversion in attention deficit/hyperactivity disorder: An empirical investigation of the broader phenotype. Neuropsychologia 2009, 47, 446–456. [Google Scholar] [CrossRef] [PubMed]
- Deater-Deckard, K. Family matters: Intergenerational and interpersonal processes of executive function and attentive behavior. Curr. Dir. Psychol. Sci. 2014, 23, 230–236. [Google Scholar] [CrossRef]
- Black, J.M.; Tanaka, H.; Stanley, L.; Nagamine, M.; Zakerani, N.; Thurston, A.; Kesler, S.; Hulme, C.; Lyytinen, H.; Glover, G.H.; et al. Maternal history of reading difficulty is associated with reduced language-related gray matter in beginning readers. NeuroImage 2012, 59, 3021–3032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Bergen, E.; de Jong, P.F.; Plakas, A.; Maassen, B.; van der Leij, A. Child and parental literacy levels within families with a history of dyslexia. J. Child. Psychol. Psychiatry 2012, 53, 28–36. [Google Scholar] [CrossRef]
- Torppa, M.; Eklund, K.; van Bergen, E.; Lyytinen, H. Parental literacy predicts children’s literacy: A longitudinal family-risk study. Dyslexia 2011, 17, 339–355. [Google Scholar] [CrossRef]
- Bonifacci, P.; Montuschi, M.; Lami, L.; Snowling, M.J. Parents of children with dyslexia: Cognitive, emotional and behavioural profile. Dyslexia 2014, 20, 175–190. [Google Scholar] [CrossRef]
- Deater-Deckard, K. Parenting stress and child adjustment: Some old hypotheses and new questions. Clin. Psychol. Sci. Pract. 1998, 5, 314–332. [Google Scholar] [CrossRef]
- Abidin, R.R. Parenting Stress Index: Professional Manual, 3rd ed.; Psychological Assessment Resources: Odessa, FL, USA, 1995. [Google Scholar]
- Theule, J.; Wiener, J.; Jenkins, J.; Tannock, R. Parenting stress in families of children with ADHD: A meta-analysis. J. Emot. Behav. Disord. 2013, 21, 3–17. [Google Scholar] [CrossRef]
- Wiener, J.; Biondic, D.; Grimbos, T.; Herbert, M. Parenting Stress of Parents of Adolescents with Attention-Deficit Hyperactivity Disorder. J. Abnorm. Child Psychiatry 2015, 44, 561–574. [Google Scholar] [CrossRef]
- Fuller, G.B.; Rankin, R.E. Differences in the levels of parental stress among mothers of learning disabled, emotionally impaired and regular school children. Percept Motor Skill 1994, 78, 583–592. [Google Scholar] [CrossRef]
- Margalit, M.; Heiman, T. Family climate and anxiety in families with learning disabled boys. J. Am. Acad. Child. Psychiatry 1986, 25, 841–846. [Google Scholar] [CrossRef]
- Waggoner, K.; Wilgosh, L. Concerns of families of children with learning disabilities. J. Learn. Disabil. 1990, 23, 97–113. [Google Scholar] [CrossRef] [PubMed]
- Snowling, M.J.; Muter, V.; Carroll, J. Children at family risk of dyslexia: A follow-up in early adolescence. J. Child. Psychol. Psychiatry 2007, 48, 609–618. [Google Scholar] [CrossRef] [PubMed]
- Karande, S.; Kumbhare, N.; Kulkarni, M.; Shah, N. Anxiety levels in mothers of children with specific learning disability. J. Postgrad. Med. 2009, 55, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Bonifacci, P.; Storti, M.; Tobia, V.; Suardi, A. Specific learning disorders: A look inside children’s and parents’ psychological well-being and relationships. J. Learn. Disabil. 2016, 49, 532–545. [Google Scholar] [CrossRef]
- Kaufman, A.S.; Kaufman, N.L. Kaufman Brief Intelligence Test, 2nd ed.; Pearson: Bloomington, MN, USA, 2004. [Google Scholar]
- Bonifacci, P.; Nori, R. Kaufman Brief Intelligence Test, 2nd ed; Italian Standardization; Giunti OS: Firenze, Italy, 2016. [Google Scholar]
- Cornoldi, C.; Colpo, G. Nuove Prove di Lettura MT per la Scuola Media Inferiore; Giunti OS: Firenze, Italy, 1995. [Google Scholar]
- Sartori, G.; Job, R.; Tressoldi, P.E. DDE-2. In Batteria per La Valutazione Della Dislessia E Della Disortografia Evolutiva; Giunti OS: Firenze, Italy, 2007. [Google Scholar]
- Lefly, D.L.; Pennington, B. Reliability and validity of the Adult Reading History Questionnaire. J. Learn. Disabil. 2000, 33, 286–296. [Google Scholar] [CrossRef] [PubMed]
- van Bergen, E.; de Jong, P.F.; Regtvoort, A.; Oort, F.; van Otterloo, S.; van der Leij, A. Dutch children at family risk of dyslexia: Precursors, reading development, and parental effects. Dyslexia 2011, 17, 2–18. [Google Scholar] [CrossRef] [PubMed]
- Faraone, S.V.; Biederman, J.; Lehman, B.K.; Keenan, K.; Norman, D.; Seidman, L.J.; Kolodny, R.; Kraus, I.; Perrin, J.; Chen, W.J. Evidence for the independent familial transmission of attention deficit hyperactivity disorder and learning disabilities: Results from a family genetic study. Am. J. Psychiat. 1993, 150, 891–895. [Google Scholar] [PubMed]
- Schlarb, A.; Starck, M.; Grünwald, J. Occurrence of ADHD in parents of ADHD children in a clinical sample. Neuropsychiatr. Dis. Treat. 2016, 12, 581–588. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Measures | P-ADHD | P-TD | P-DYS | p-Values | Bonferroni Post-Hoc Comparisons | |||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | |||
| Children age | 9.3 | 1.5 | 9.8 | 1.8 | 10.3 | 1.7 | 0.06 | NS |
| Parents age | 43.3 | 5.7 | 44.1 | 5 | 43.7 | 4.9 | 0.7 | NS |
| SES | 35.24 | 11.04 | 43.82 | 9.32 | 36.68 | 12.42 | <0.001 | TD > DYS = ADHD |
| Reading * | 2.05 | 0.38 | 2.26 | 0.44 | 1.45 | 0.6 | <0.001 | TD = ADHD > DISL |
| Writing * | 1.81 | 0.68 | 2.25 | 0.43 | 1.61 | 0.64 | <0.001 | TD > DYS = ADHD |
| Grammar * | 1.95 | 0.5 | 2.25 | 0.53 | 1.5 | 0.6 | <0.001 | TD = ADHD > DYS |
| History * | 2.05 | 0.5 | 2.37 | 0.55 | 1.89 | 0.77 | <0.001 | TD > DYS |
| Mathematics * | 1.9 | 0.77 | 2.28 | 0.55 | 1.58 | 0.76 | <0.001 | TD > DYS |
| Science * | 2.1 | 0.54 | 2.29 | 0.52 | 1.84 | 0.69 | <0.001 | TD > DYS |
| Measure | P-ADHD | P-TD | P-DYS | p-Values | Bonferroni Post-Hoc Comparisons | |||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | |||
| Verbal IQ | 100.10 | 7.50 | 108.40 | 9.60 | 105.20 | 10.30 | <0.001 | TD > ADHD DYS = ADHD; DYS = TD |
| Non Verbal IQ | 96.80 | 17.00 | 108.90 | 13.80 | 104.70 | 11.80 | <0.001 | TD > ADHD; DYS = ADHD; DYS = TD |
| Semantic Fluency | 14.70 | 3.40 | 19.20 | 4.60 | 16.20 | 4.50 | <0.001 | TD > ADHD = DYS |
| Passage reading speed (syll/sec) | 5.38 | 1.21 | 6.10 | 1.04 | 4.91 | 0.98 | <0.001 | TD > ADHD = DYS |
| Non word reading speed (syll/sec) | 2.65 | 0.76 | 3.03 | 0.71 | 2.41 | 0.69 | <0.001 | TD > DYS = ADHD |
| ARHQ Total | 0.35 | 0.11 | 0.26 | 0.09 | 0.37 | 0.17 | <0.001 | TD > ADHD = DYS |
| ASRS Total | 6.76 | 4.34 | 3.91 | 3.18 | 5.13 | 4.06 | <0.01 | ADHD > DYS = C |
| * PSI Defensive Scale | 1.08 | 1.31 | −0.08 | 0.95 | −0.03 | 1.15 | <0.001 | ADHD > DYS = C |
| PSI Parent distress | 0.96 | 1.34 | −0.25 | 0.86 | −0.15 | 1.11 | <0.001 | ADHD > DYS = C |
| PSI Difficult Child Interaction | 1.49 | 1.77 | 0.12 | 0.88 | 0.62 | 1.30 | <0.001 | ADHD > DYS = C |
| PSI Difficult Child | 1.74 | 1.58 | 0.21 | 0.96 | 0.57 | 1.06 | <0.001 | ADHD > DYS = C |
| PSI Total Score | 1.76 | 1.42 | 0.02 | 0.83 | 0.39 | 1.22 | <0.001 | ADHD > DYS = C |
| Step | Measure | B | SE B | β |
|---|---|---|---|---|
| 1 (R2 = 0.137) | SES | −0.6 | 0.176 | −0.31 ** |
| Number family members | −4.679 | 1.677 | −0.25 ** | |
| Parents’ age | 0.008 | 0.395 | 0.002 | |
| 2 (ΔR2 = 0.047. p = 0.21) | SES | −0.481 | 0.193 | −0.251 * |
| Number family members | −4.818 | 1.777 | −0.264 ** | |
| Parents’ age | −0.027 | 0.398 | −0.006 | |
| Non-word reading speed | −3.493 | 2.958 | −0.116 | |
| Verbal fluency | −0.67 | 0.432 | −0.157 | |
| ANT-Conflict (RTs) | 0.024 | 0.046 | 0.046 | |
| Composite IQ | 0.001 | 0.189 | 0.001 | |
| 3 (ΔR2 = 0.084. p < 0.01) (R2 = 0.268) | SES | −0.453 | 0.197 | −0.236 * |
| Number family members | −4.23 | 1.709 | −0.231 * | |
| Parents’ age | −0.072 | 0.382 | −0.017 | |
| Non-word reading speed | −3.968 | 2.949 | −0.132 | |
| Verbal fluency | −0.581 | 0.415 | −0.137 | |
| ANT-Conflict (RTs) | 0.019 | 0.045 | 0.037 | |
| Composite IQ | 0.076 | 0.182 | 0.042 | |
| ARHD (reading history) | 0.083 | 17.701 | 0 | |
| ASRS (ADHD symptoms) | 1.771 | 0.534 | 0.299 ** |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bonifacci, P.; Massi, L.; Pignataro, V.; Zocco, S.; Chiodo, S. Parenting Stress and Broader Phenotype in Parents of Children with Attention Deficit Hyperactivity Disorder, Dyslexia or Typical Development. Int. J. Environ. Res. Public Health 2019, 16, 1878. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16111878
Bonifacci P, Massi L, Pignataro V, Zocco S, Chiodo S. Parenting Stress and Broader Phenotype in Parents of Children with Attention Deficit Hyperactivity Disorder, Dyslexia or Typical Development. International Journal of Environmental Research and Public Health. 2019; 16(11):1878. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16111878
Chicago/Turabian StyleBonifacci, Paola, Laura Massi, Veronica Pignataro, Sara Zocco, and Simona Chiodo. 2019. "Parenting Stress and Broader Phenotype in Parents of Children with Attention Deficit Hyperactivity Disorder, Dyslexia or Typical Development" International Journal of Environmental Research and Public Health 16, no. 11: 1878. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16111878