Intrinsic Motivation and Psychological Connectedness to Drug Abuse and Rehabilitation: The Perspective of Self-Determination



Abstract
:1. Introduction
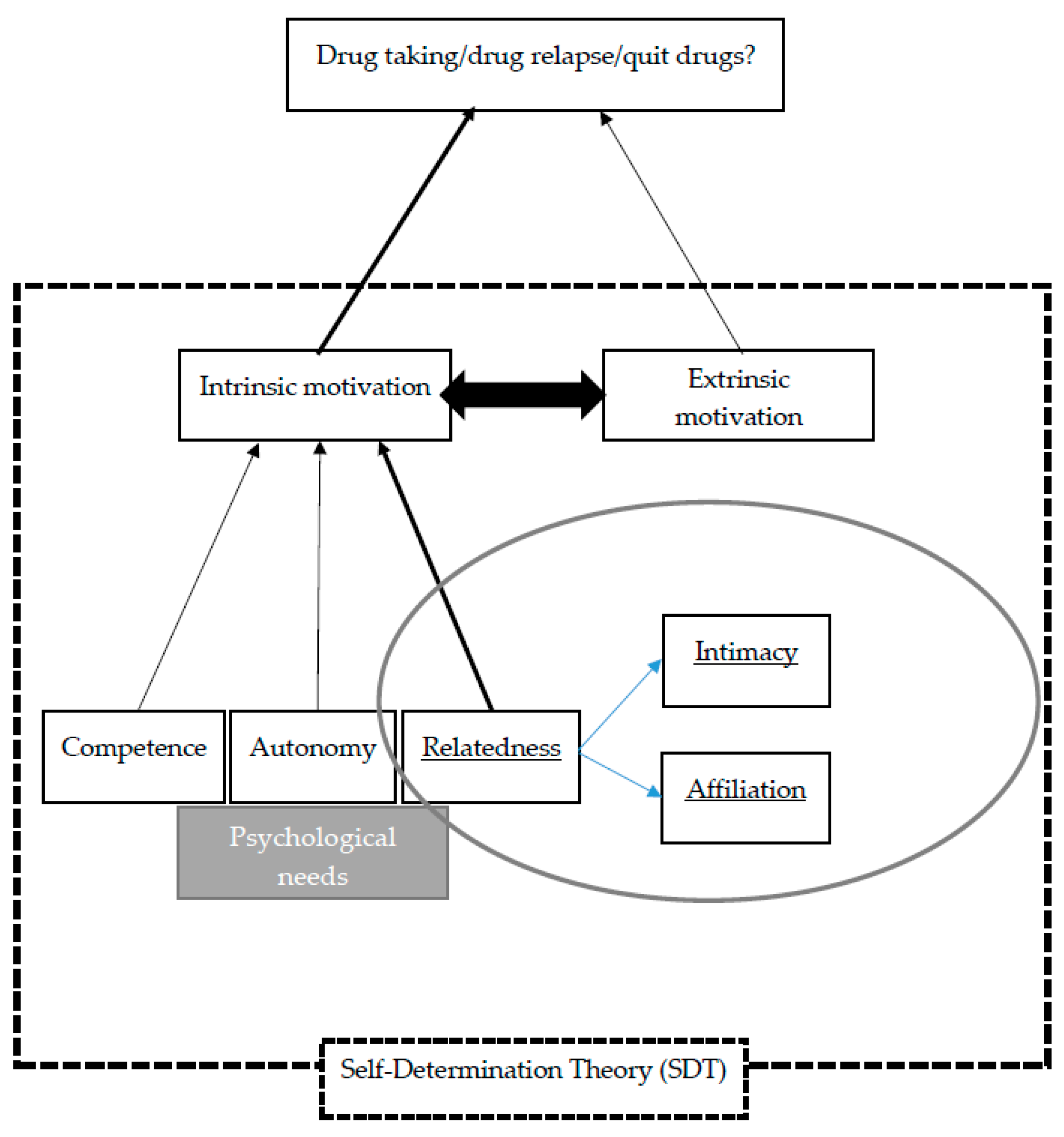
1.1. Self-Determination Theory
1.2. Application of SDT in the Context of Drug Use and Drug Relapse
1.3. Insights from the Literature
1.4. Present Study
2. Methodology
2.1. Procedure and Participants
2.2. Analyses
3. Results
3.1. Background of Participants
3.2. Introduction of the Themes
3.3. Analyses of the Themes and Quotes
3.3.1. Relatedness with Significant Others
3.3.2. Psychological Substitutes for the Lack of Connectedness in Life
3.3.3. As a Way to Maintain a Relationship or Affiliation
3.3.4. Significant Others are Usually a Double-Edged Sword
3.3.5. Connectedness with God
3.3.6. Sense of Competence and Connectedness to Work
3.3.7. Autonomy—Willingness to Quit
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A. Semi-Structured Interview Guideline
- When did you first start using drugs? What was the reason for doing so?
- What was the reason for your need to continue using drugs? What situation would you be triggered to think of using drugs?
- What does drug use mean to you? What do you gain from using drugs? Do you lose anything from using drugs?
- If you were to talk about your most painful experience of drug use, what would it be?
- How much does work/life stress affect your drug use?
- How much does your friend, boy/girlfriend, and family affect your drug use?
- Is drug use related to being deprived of faith or spirituality? What do you think?
- When you have urges to use drugs, what do you feel and what would you do?
- What is the most helpful method to help you handle the urges? What are the reasons when you cannot handle your urges?
- Who can help you resist from relapsing?
- In the past, have you tried to quit drug use? What methods have you tried? What was the longest period you were able to abstain? How could you sustain it?
- To you, what is the best reason or method to quit drug use?
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM), 5th ed.; American Psychiatric Pub.: Washington, DC, USA, 2013. [Google Scholar]
- Jedrzejczak, M. Family and environmental factors of drug addiction among young recruits. Mil. Med. 2005, 170, 688–690. [Google Scholar] [CrossRef]
- Miller, W.R.; Carroll, K.M. Rethinking Substance Abuse: What the Science Shows, and What We Should Do about It; Guilford Press: New York, NY, USA, 2006. [Google Scholar]
- Narcotics Division, Security Bureau. Reason for Current Drug Abuse: Newly/Previously Reported Drug Abusers by Age Group by Reason for Current Drug Use. 2018. Available online: http://www.nd.gov.hk/statistics_list/doc/tc/t7.pdf (accessed on 25 July 2018).
- Siegel, L.J. Criminology; Wadsworth: Belmont, CA, USA, 1995. [Google Scholar]
- Liu, Y.M. Research on the causes of Chinese drug abusers from the perspective of Social Psychology. Frontiers 2009, 11, 166–168. [Google Scholar]
- Arpawong, T.E.; Sussman, S.; Milam, J.E.; Unger, J.B.; Land, H.; Sun, P.; Rohrbach, L.A. Post-traumatic growth, stressful life events, and relationship with substance use behaviors among alternative high school students: A prospective study. Psychol. Health 2015, 30, 475–494. [Google Scholar] [CrossRef]
- Hirschi, T. Causes of Delinquency; University of California Press: Berkeley, CA, USA, 1969. [Google Scholar]
- Bandura, A. Self-efficacy: Toward a unifying theory of behavior change. Psychol. Rev. 1977, 84, 191–215. [Google Scholar] [CrossRef]
- Bickel, W.K.; Vuchinich, R.E. (Eds.) Reframing Health Behavior Change with Behavior Economics; Lawrence Erlbaum: Mahwah, NJ, USA, 2000. [Google Scholar]
- Tam, C.; Kwok, S.I.; Lo, T.W.; Lam, S.; Lee, G. Hidden drug abuse in Hong Kong: From social acquaintance to social isolation. Front. Psychiatry 2018, 9, 457. [Google Scholar] [CrossRef]
- Dittmar, M.; Ratnasingam, M.; Navaratnam, V. A Comparative Analysis of the Psychological Profile of Institusionalized Drug Using Population Minden; Pusat Penyelidikan Dadah Kebangsaan, Universiti Sains Malaysia: Penang, Malaysia, 1984. [Google Scholar]
- Hammer-Bacher, M.; Lyvers, M. Factors associated with relapse among clients in Australian substance disorder treatment facilities. J. Subst. Use 2006, 11, 387–394. [Google Scholar] [CrossRef] [Green Version]
- Moos, R.H.; King, M.J. Participation in community residential treatment and substance abuse patients’ outcomes at discharge. J. Subst. Abuse Treat. 1997, 14, 71–80. [Google Scholar] [CrossRef]
- Rasmussen, S. Addiction Treatment: Theory and Practice; Sage Publication, Inc.: Beverly Hills, CA, USA, 2000. [Google Scholar]
- Marlatt, G.A.; Gordon, J.R. Relapse Prevention: Maintenance Strategies in the Treatment of Addictive Behaviors; Guilford Press: New York, NY, USA, 1985. [Google Scholar]
- Wang, X.H. Psychotherapy for preventing drug relapse. Chin. J. Clin. Rehabil. 2005, 9, 138–140. [Google Scholar]
- Hwang, K.K. Face and favor: The Chinese power fame. Am. J. Sociol. 1987, 92, 944–974. [Google Scholar] [CrossRef]
- Jacobs, B.J. A preliminary model of particularistic ties in Chinese political alliances: Kan-ching and Kuan-his in a rural Taiwanese township. Chin. Q. 1979, 8, 237–273. [Google Scholar] [CrossRef]
- Leung, T.K.P.; Wong, Y.H.; Wong, S. A study of Hong Kong businessmen’s perceptions of the role “Guanxi” in the People’s Republic of China. J. Bus. Ethics 1996, 15, 749–758. [Google Scholar] [CrossRef]
- Pye, L.W. Faction and the politics of Guanxi: Paradox in Chinese administrative and political behavior. Chin. J. 1995, 34, 35–53. [Google Scholar] [CrossRef]
- Xin, C.R.; Pearce, J.L. Guanxi: Connections as substitutes for formal institutional support. Acad. Manag. J. 1996, 39, 1641–1658. [Google Scholar]
- Yeung, I.Y.M.; Tung, R.L. Achieving business success in Confucian societies: The importance of Guanxi. Organ. Dyn. 1996, 25, 54–65. [Google Scholar] [CrossRef]
- Jiang, G.; Lo, T.W.; Garris, C.P. Formation and trend of Guanxi practice and Guanxi phenomenon. Int. J. Criminol. Sociol. 2012, 1, 207–220. [Google Scholar] [CrossRef]
- Deci, E.L.; Ryan, R.M. The “what” and “why” of goal pursuits: Human needs and the self-determination of behavior. Psychol. Inq. 2000, 11, 227–268. [Google Scholar] [CrossRef]
- Patrick, H.; Williams, G.C. Self-determination theory: Its application to health behavior and complementarity with motivational interviewing. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 18. [Google Scholar] [CrossRef] [PubMed]
- Ryan, R.M.; Deci, E.L. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am. Psychol. 2000, 55, 68–78. [Google Scholar] [CrossRef]
- Deci, E.L.; Ryan, R.M. Intrinsic Motivation and Self-Determination in Human Behavior; Plenum: New York, NY, USA, 1985. [Google Scholar]
- Baumeister, R.F.; Leary, M.R. The need to belong: Desire for interpersonal attachments as a fundamental human motivation. Psychol. Bull. 1995, 117, 497–529. [Google Scholar] [CrossRef] [PubMed]
- Deci, E.L.; Nezlek, J.; Sheinman, L. Characteristics of the rewarder and intrinsic motivation of the rewardee. J. Pers. Soc. Psychol. 1981, 40, 1–10. [Google Scholar] [CrossRef]
- Grolnick, W.S.; Ryan, R.M. Parent styles associated with children’s self-regulation and competence in schools. J. Educ. Psychol. 1989, 81, 143–154. [Google Scholar] [CrossRef]
- Klag, S.M.L.; Creed, P.; O’Callaghan, F. Early motivation, well-being, and treatment engagement of chronic substance users undergoing treatment in a therapeutic community setting. Subst. Use Misuse 2010, 45, 1112–1130. [Google Scholar] [CrossRef]
- Cleverly, K.; Grenville, M.; Henderson, J. Youths perceived parental influence on substance use changes and motivation to seek treatment. J. Behav. Health Serv. Res. 2018, 45, 640–650. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. A self-determination theory approach to psychotherapy: The motivational basis for effective change. Can. Psychol. 2008, 49, 186–193. [Google Scholar] [CrossRef]
- Zeldman, A.; Ryan, R.; Fiscella, K. Motivation, autonomy support, and entity beliefs: Their role in methadone maintenance treatment. J. Soc. Clin. Psychol. 2004, 23, 675–696. [Google Scholar] [CrossRef]
- Lo, T.W.; Tse, J.; Cheng, C.; Chan, G.H.Y. The association between substance abuse and sexual misconduct among Macau youths. Int. J. Environ. Res. Public Health 2019, 16, 1643. [Google Scholar] [CrossRef]
- Hofer, J.; Busch, H. Satisfying one’s needs for competence and relatedness: Consequent domain-specific well-being depends on strength of implicit motives. Pers. Soc. Psychol. Bull. 2011, 37, 1147–1158. [Google Scholar] [CrossRef]
- McIntosh, J.; McKeganey, N. Addicts’ narratives of recovery from drug use: Constructing a non-addict identity. Soc. Sci. Med. 2000, 50, 1501–1510. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using Thematic Analysis in Psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Tam, H.L.; Shik, A.W.Y.; Lam, S.S.L. Using expressive arts in relapse prevention of young psychotropic substance abusers in Hong Kong. Child. Youth Serv. Rev. 2016, 60, 88–100. [Google Scholar] [CrossRef]
- Sampson, R.J.; Laub, J.H. Crime in the Making: Pathways and Turning Points through Life; Harvard University Press: Cambridge, MA, USA, 1993. [Google Scholar]
- Sampson, R.J.; Laub, J.H. A life course view of the development of crime. Ann. Am. Acad. Political Soc. Sci. 2005, 602, 12–45. [Google Scholar] [CrossRef]
- Ploeger, M. Youth employment and delinquency: Reconsidering a problematic relationship. Criminology 1997, 35, 659–675. [Google Scholar] [CrossRef]
- Ainsworth, M.D.S. The development of infant-mother attachment. In Review of Child Development Research; Cardwell, B., Ricciuti, H., Eds.; University of Chicago Press: Chicago, IL, USA, 1973; pp. 1–94. [Google Scholar]
- Bowlby, J. The nature of the child’s tie to his mother. Int. J. Psychoanal. 1958, 39, 350–371. [Google Scholar]
- Bowlby, J. Attachment. Attachment and Loss; Basic Books: New York, NY, USA, 1969. [Google Scholar]
- Maslow, A.H. Toward a Psychology of Being; Van Nostrand: New York, NY, USA, 1968. [Google Scholar]
- Hofer, J.; Hagemeyer, B. Social bonding: Affiliation motivation and intimacy motivation. In Motivation and Action; Heckhausen, J., Heckhausen, H., Eds.; Springer International: Basel, Switzerland, 2018; pp. 305–334. [Google Scholar]
- Weiss, R.S. Loneliness: The Experience of Emotional and Social Isolation; MIT Press: Cambridge, MA, USA, 1973. [Google Scholar]
- Cullum, J.; O’Grady, M.; Tennen, H. Affiliation goals and health behaviors. Soc. Pers. Psychol. Compass 2011, 5, 694–705. [Google Scholar] [CrossRef] [PubMed]
- Mikulincer, M.; Shaver, P.R. Attachment in Adulthood Structure Dynamics and Change; The Guilford Press: New York, NY, USA, 2007. [Google Scholar]
- Shaver, P.R.; Mikulincer, M. Attachment bonds in romantic relationships. In the Herzliya Series on Personality and Social Psychology. Mechanisms of Social Connection: From Brain to Group; Mikulincer, M., Shaver, P.R., Eds.; American Psychological Association: Washington, DC, USA, 2014; pp. 273–290. [Google Scholar]
- Bretherton, I. Attachment theory: Retrospect and prospect. Monogr. Soc. Res. Child. Dev. 1985, 50, 3–35. [Google Scholar] [CrossRef]
- Kougiali, Z.G.; Fasulo, A.; Needs, A.; Van Laar, D. Planting the seeds of change: Directionality in the narrative construction of recovery from addiction. Psychol. Health 2017, 32, 639–664. [Google Scholar] [CrossRef] [Green Version]
- Tracy, K.; Wallace, S.P. Benefits of peer support groups in the treatment of addiction. Subst. Abus. Rehabil. 2016, 7, 143–154. [Google Scholar] [CrossRef]


{kind=link}
| Variable | n | % |
|---|---|---|
| Gender (n = 103) | ||
| Male | 52 | 50.5 |
| Female | 51 | 49.5 |
| Age (n = 102) | ||
| 11−20 | 18 | 17.6 |
| 21−30 | 41 | 40.2 |
| 31−40 | 24 | 23.5 |
| 41−50 | 13 | 12.7 |
| 51 and above | 6 | 5.9 |
| Frequency of taking drugs (n = 101) | ||
| Less than once per month | 1 | 1.0 |
| Once per month | 1 | 1.0 |
| 2−3 times per month | 9 | 8.9 |
| 1−2 times per week | 14 | 13.9 |
| 3−6 times per week | 10 | 9.9 |
| More than 6 times a week | 66 | 65.3 |
| Types of drugs taken (multiple options) | ||
| Crystal methamphetamine (Ice) | 69 | 67.0 |
| Cocaine | 36 | 35.0 |
| Ketamine | 33 | 32.4 |
| Heroin | 23 | 22.3 |
| Nimetazepam | 14 | 13.6 |
| Cannabis | 11 | 10.7 |
| Ecstasy | 10 | 9.7 |
| Others (Triazolam, Methaqualone, cough medicine) | 12 | 11.6 |
| Age of first drug−taking (n = 99) | ||
| 11−20 | 77 | 77.8 |
| 21−30 | 15 | 15.2 |
| 31−50 | 7 | 7.1 |
| Duration of taking drugs (n = 102) | ||
| Less than 3 years | 20 | 19.6 |
| 3−5 years | 15 | 14.7 |
| Between 5 and 10 years | 17 | 16.7 |
| More than 10 years | 32 | 31.4 |
| More than 20 years | 18 | 17.6 |
| Variable | n | % |
|---|---|---|
| Most important reason for taking drugs (n = 103) | ||
| Peer influence | 32 | 31.1 |
| Feeling bored or depressed | 28 | 27.2 |
| Release pressure | 10 | 9.7 |
| Refreshing | 9 | 8.7 |
| Curious | 9 | 8.7 |
| To avoid feeling discomfort when not taking drugs | 4 | 3.9 |
| Seeking excitement/pleasure | 3 | 2.9 |
| Family influence | 2 | 1.9 |
| Others | 6 | 5.9 |
| Themes | Subthemes |
|---|---|
| Intrinsic motivation: Competence | Reasons for taking drugs:
|
| Intrinsic motivation: Autonomy | Reasons for taking drugs:
|
| Intrinsic motivation: Relatedness | Reasons for taking drugs:
|
| Extrinsic motivation | Reasons for taking drugs:
|
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chan, G.H.Y.; Lo, T.W.; Tam, C.H.L.; Lee, G.K.W. Intrinsic Motivation and Psychological Connectedness to Drug Abuse and Rehabilitation: The Perspective of Self-Determination. Int. J. Environ. Res. Public Health 2019, 16, 1934. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16111934
Chan GHY, Lo TW, Tam CHL, Lee GKW. Intrinsic Motivation and Psychological Connectedness to Drug Abuse and Rehabilitation: The Perspective of Self-Determination. International Journal of Environmental Research and Public Health. 2019; 16(11):1934. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16111934
Chicago/Turabian StyleChan, Gloria H. Y., T. Wing Lo, Cherry H. L. Tam, and Gabriel K. W. Lee. 2019. "Intrinsic Motivation and Psychological Connectedness to Drug Abuse and Rehabilitation: The Perspective of Self-Determination" International Journal of Environmental Research and Public Health 16, no. 11: 1934. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16111934