The Current Research Landscape on the Artificial Intelligence Application in the Management of Depressive Disorders: A Bibliometric Analysis

 , , , and
, , , and 
Abstract
:1. Introduction
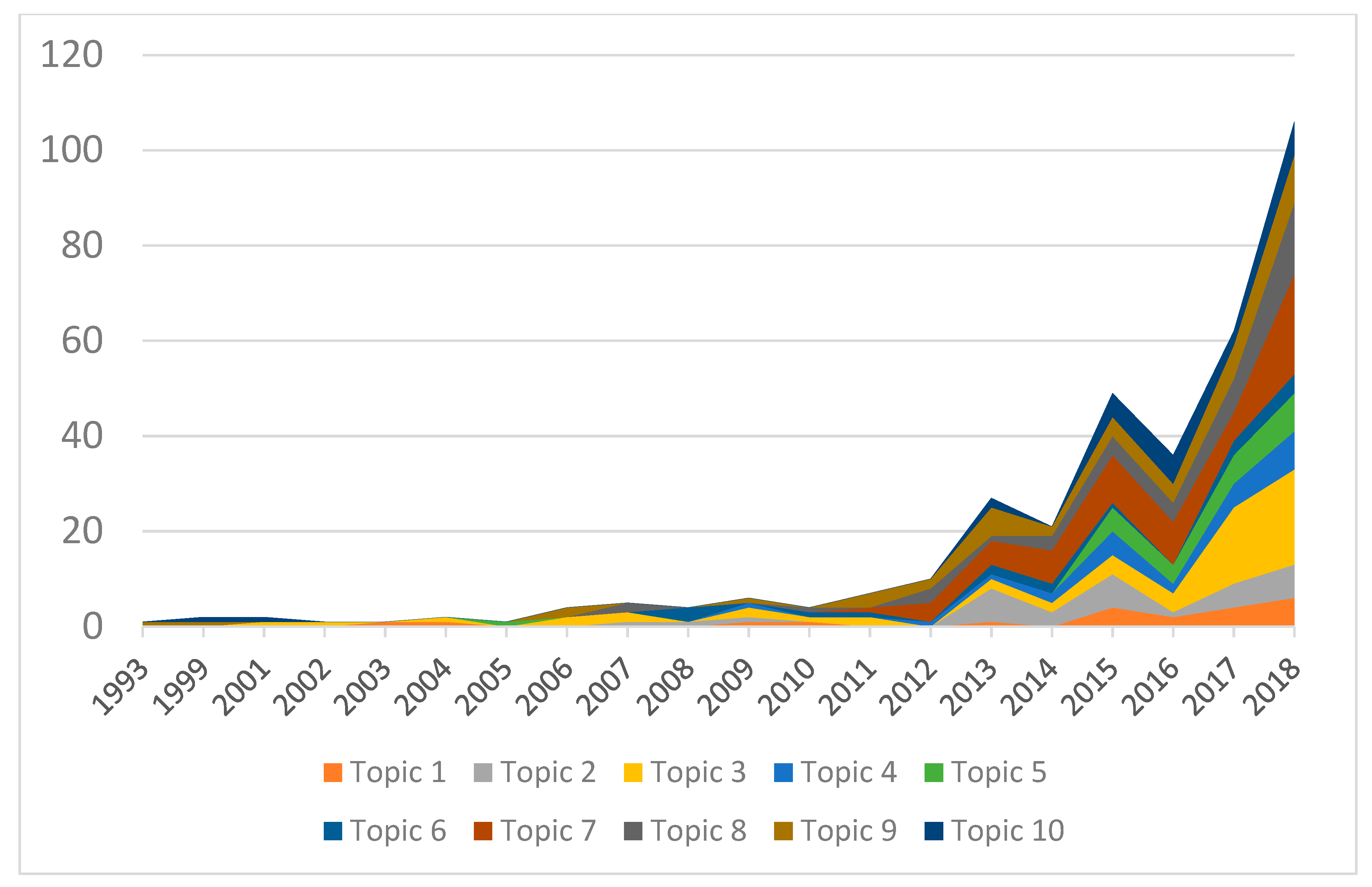
- The trend of published articles over time and international growth based on databases of existing literature were examined.
- Current research interests on AI application in depression were pointed out.
- The development and productivity of AI research in depression was evaluated.
- The research gaps in the application of AI in depression were identified.
2. Materials and Methods
2.1. Search Strategy
2.2. Data Extraction, Inclusion, and Exclusion Criteria
2.3. Data Analysis, Outcomes, and Data Synthesis
3. Results
3.1. Systematic Search Results
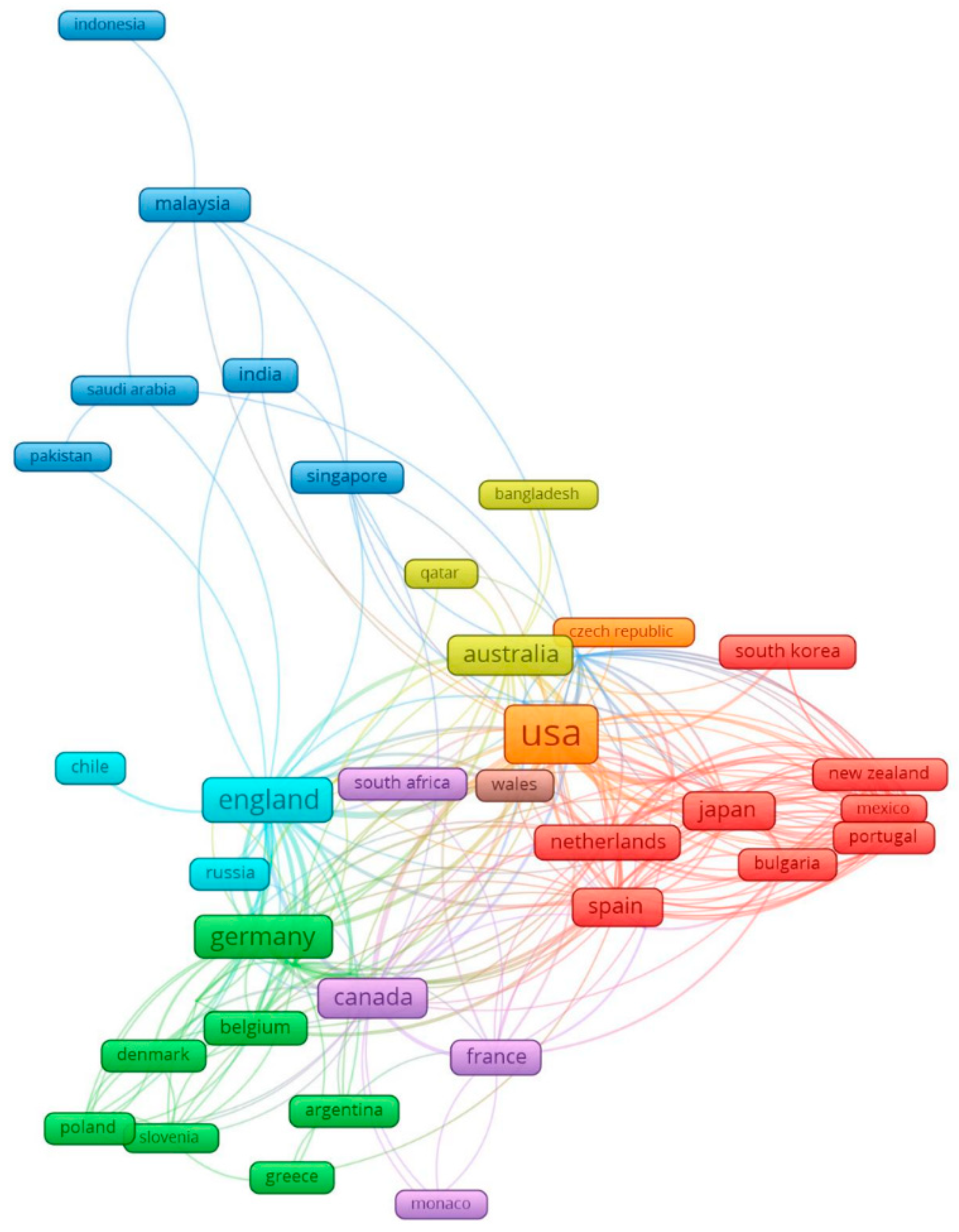
3.2. Global Network of AI Research in Depression
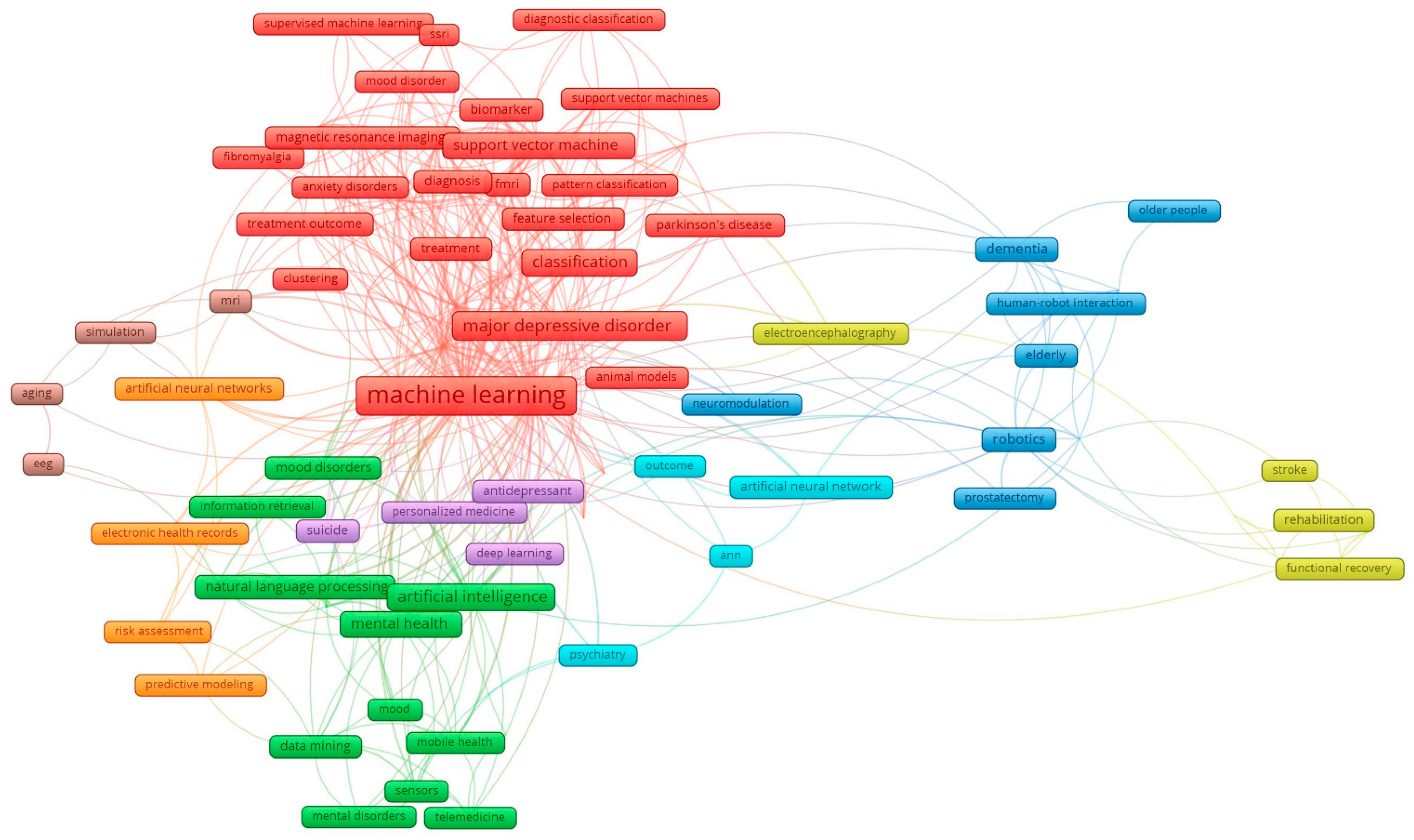
3.3. Key Research Subtopics in AI Research for Depression
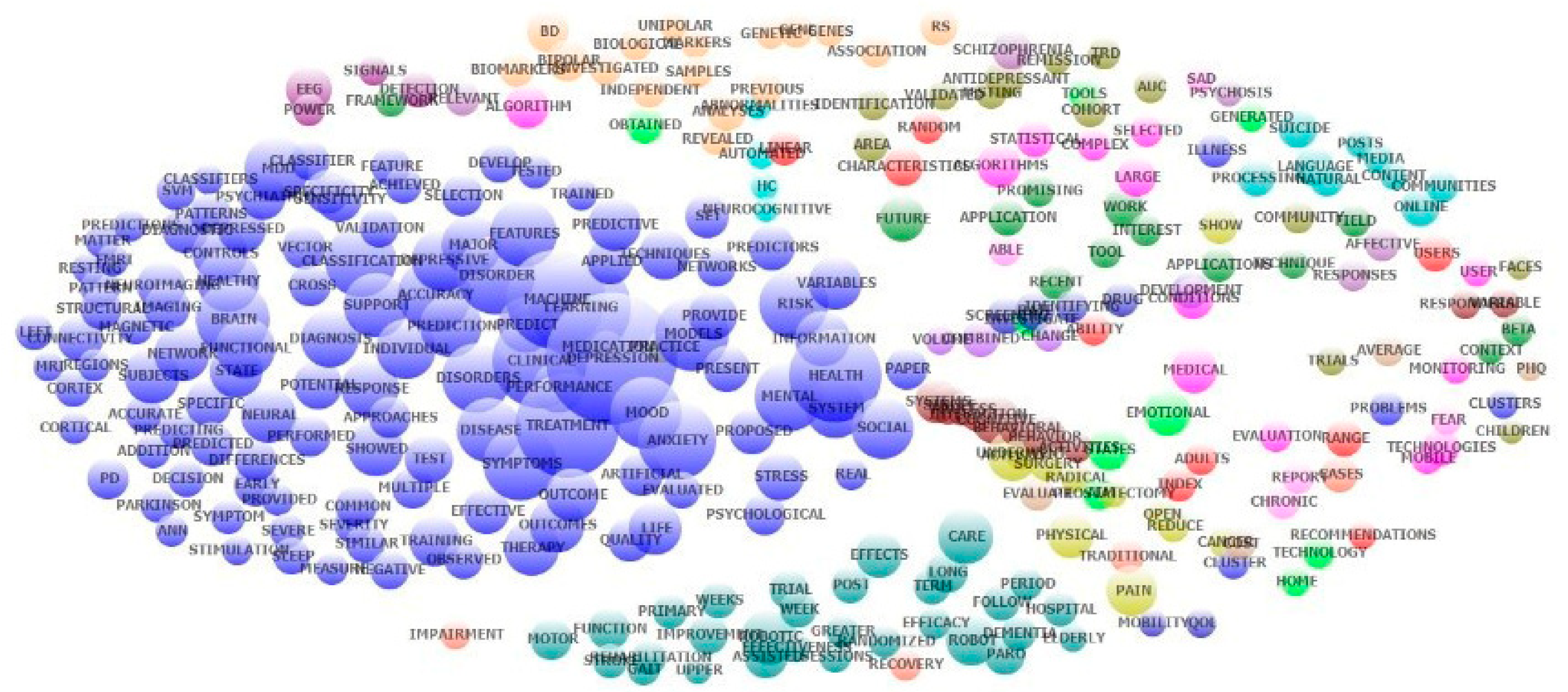
3.4. Exploratory Factor Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Lim, G.Y.; Tam, W.W.; Lu, Y.; Ho, C.S.; Zhang, M.W.; Ho, R.C. Prevalence of depression in the community from 30 countries between 1994 and 2014. Sci. Rep. 2018, 8, 2861. [Google Scholar] [CrossRef]
- Puri, B.; Hall, A.; Ho, R. Revision Notes in Psychiatry, 3rd ed.; CRC Press: New York, NY, USA, 2013. [Google Scholar]
- Marcus, M.; Yasamy, M.T.; Van Ommeren, M.; Chisholm, D.; Saxena, S. DEPRESSION: A Global Public Health Concern; WHO Department of Mental Health and Substance Abuse: Geneva, Switzerland, 2017. [Google Scholar]
- Quek, Y.H.; Tam, W.W.S.; Zhang, M.W.B.; Ho, R.C.M. Exploring the association between childhood and adolescent obesity and depression: A meta-analysis. Obes. Rev. 2017, 18, 742–754. [Google Scholar] [CrossRef] [PubMed]
- Vu, H.T.T.; Nguyen, T.X.; Nguyen, H.T.T.; Le, T.A.; Nguyen, T.N.; Nguyen, A.T.; Nguyen, T.T.H.; Nguyen, H.L.; Nguyen, C.T.; Tran, B.X.; et al. Depressive symptoms among elderly diabetic patients in Vietnam. Diabetes Metab. Syndr. Obes. 2018, 11, 659–665. [Google Scholar] [CrossRef] [PubMed]
- Vu, T.T.M.; Le, T.V.; Dang, A.K.; Nguyen, L.H.; Nguyen, B.C.; Tran, B.X.; Latkin, C.A.; Ho, C.S.H.; Ho, R.C.M. Socioeconomic vulnerability to depressive symptoms in patients with chronic hepatitis B. Int. J. Environ. Res. Public Health 2019, 16, 255. [Google Scholar] [CrossRef] [PubMed]
- Ho, R.C.M.; Chua, A.C.; Tran, B.X.; Choo, C.C.; Husain, S.F.; Vu, G.T.; McIntyre, R.S.; Ho, C.S.H. Factors associated with the risk of developing coronary artery disease in medicated patients with major depressive disorder. Int. J. Environ. Res. Public Health 2018, 15, 2073. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Rosenblat, J.D.; Lee, J.; Carmona, N.E.; Subramaniapillai, M.; Shekotikhina, M.; Mansur, R.B.; Brietzke, E.; Lee, J.H.; Ho, R.C.; et al. Efficacy of antidepressants on measures of workplace functioning in major depressive disorder: A systematic review. J. Affect. Disord. 2018, 227, 406–415. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Key facts. In Depression 2018; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- World Health Organization. Depression and Other Common Mental Disorders: Global Health Estimates; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- Dopico, M.; Gomez, A.; De la Fuente, D.; García, N.; Rosillo, R.; Puche Regaliza, J. A Vision of Industry 4.0 from an Artificial Intelligence; CSREA Press: Las Vegas, NV, USA, 2016. [Google Scholar]
- Elsevier. ArtificiaI Intelligence: How Knowledge Is Created, Transferred, and Used; Elsevier: Amsterdam, The Netherlands, 2018. [Google Scholar]
- Moor, J. The dartmouth college artificial intelligence conference: The next fifty years. In AI Magazine; American Association for Artificial Intelligence: Menlo Park, CA, USA, 2006; pp. 87–91. [Google Scholar]
- McCarthy, J. A proposal for the dartmouth summer research project on artificial intelligence. In AI Magazine; American Association for Artificial Intelligence: Menlo Park, CA, USA, 2006; Volume 27, pp. 12–14. [Google Scholar]
- Kaplana, A.; Haenleinb, M. Siri, siri, in my hand: Who’s the fairest in the land? On the interpretations, illustrations, and implications of artificial intelligence. Bus. Horiz. 2018, 62, 15–25. [Google Scholar] [CrossRef]
- Danks, D.; Vincze, M.; Wachsmuth, S.; Sagerer, G.; Amir, E.; Wilks, Y.; Alonso, E.; Scheutz, M. Dimensions. In The Cambridge Handbook of Artificial Intelligence; Frankish, K., Ramsey, W.M., Eds.; Cambridge University Press: Cambridge, UK, 2014. [Google Scholar]
- Ledley, R.S.; Lusted, L.B. Reasoning foundations of medical diagnosis. Science 1959, 130, 9–21. [Google Scholar] [CrossRef]
- Liew, C. The future of radiology augmented with artificial intelligence: A strategy for success. Eur. J. Radiol. 2018, 102, 152–156. [Google Scholar] [CrossRef]
- Qiu, J.X.; Yoon, H.J.; Fearn, P.A.; Tourassi, G.D. Deep learning for automated extraction of primary sites from cancer pathology reports. IEEE J. Biomed. Health Inform. 2018, 22, 244–251. [Google Scholar] [CrossRef]
- Prado, G.; Kovarik, C. Cutting edge technology in dermatology: Virtual reality and artificial intelligence. Cutis 2018, 101, 236–237. [Google Scholar] [PubMed]
- Gao, S.; Calhoun, V.D.; Sui, J. Machine learning in major depression: From classification to treatment outcome prediction. CNS Neurosci. Ther. 2018, 24, 1037–1052. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dinga, R.; Marquand, A.F.; Veltman, D.J.; Beekman, A.T.F.; Schoevers, R.A.; van Hemert, A.M.; Penninx, B.W.J.H.; Schmaal, L. Predicting the naturalistic course of depression from a wide range of clinical, psychological, and biological data: A machine learning approach. Transl. Psychiatry 2018, 8, 241. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.J.; Khalaf, A.; Aizenstein, H.J. Studying depression using imaging and machine learning methods. NeuroImage Clin. 2015, 10, 115–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laksshman, S.; Bhat, R.R.; Viswanath, V.; Li, X. DeepBipolar: Identifying genomic mutations for bipolar disorder via deep learning. Hum. Mutat. 2017, 38, 1217–1224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Senders, J.T.; Staples, P.C.; Karhade, A.V.; Zaki, M.M.; Gormley, W.B.; Broekman, M.L.D.; Smith, T.R.; Arnaout, O. Machine learning and neurosurgical outcome prediction: A systematic review. World Neurosurg. 2018, 109, 476–486. [Google Scholar] [CrossRef]
- Wongkoblap, A.; Vadillo, M.A.; Curcin, V. Researching mental health disorders in the era of social media: Systematic review. J. Med. Internet Res. 2017, 19, e228. [Google Scholar] [CrossRef]
- Gong, B.; Mohammed, M.F.; Nicolaou, S.; Nasrullah, M.; Forster, B.B.; Khosa, F. Diagnostic imaging in disasters: A bibliometric analysis. Disaster Med. Public Health Prep. 2018, 12, 265–277. [Google Scholar] [CrossRef]
- Tran, B.X.; Vu, G.T.; Ha, G.H.; Vuong, Q.H.; Ho, T.M.; Vuong, T.-T.; La, V.-P.; Ho, M.-H.; Nghiem, K.-C.P.; Nguyen, H.L.T.; et al. Global evolution of research in artificial intelligence in health and medicine: A bibliometric study. J. Clin. Med. 2019, 8, 360. [Google Scholar] [CrossRef]
- De Araújo, C.C.S.; Pedron, C.D.; Picoto, W.N. What’s Behind CRM Research? A bibliometric analysis of publications in the CRM research field. J. Relatsh. Mark. 2018, 17, 29–51. [Google Scholar] [CrossRef]
- Li, Y.; Rapkin, B.; Atkinson, T.M.; Schofield, E.; Bochner, B.H. Leveraging latent dirichlet allocation in processing free-text personal goals among patients undergoing bladder cancer surgery. Qual. Life Res. 2019, 28, 1441–1455. [Google Scholar] [CrossRef] [PubMed]
- Valle, D.; Albuquerque, P.; Zhao, Q.; Barberan, A.; Fletcher, R.J., Jr. Extending the latent dirichlet allocation model to presence/absence data: A case study on north american breeding birds and biogeographical shifts expected from climate change. Glob. Chang. Biol. 2018, 24, 5560–5572. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Zare, A.; Trinh, H.N.; Omotara, G.O.; Cobb, J.T.; Lagaunne, T.A. Partial membership latent dirichlet allocation for soft image segmentation. IEEE Trans. Image Process. 2017, 26, 5590–5602. [Google Scholar] [CrossRef] [PubMed]
- Lu, H.M.; Wei, C.P.; Hsiao, F.Y. Modeling healthcare data using multiple-channel latent Dirichlet allocation. J. Biomed. Inform. 2016, 60, 210–223. [Google Scholar] [CrossRef] [PubMed]
- Gross, A.; Murthy, D. Modeling virtual organizations with latent Dirichlet allocation: A case for natural language processing. Neural Netw. 2014, 58, 38–49. [Google Scholar] [CrossRef] [PubMed]
- Krittanawong, C. The rise of artificial intelligence and the uncertain future for physicians. Eur. J. Intern. Med. 2018, 48, e13–e14. [Google Scholar] [CrossRef] [PubMed]
- Marr, B. 5 Important Artificial Intelligence Predictions (For 2019) Everyone Should Read. 2018. Available online: https://www.forbes.com/sites/bernardmarr/2018/12/03/5-important-artificial-intelligence-predictions-for-2019-everyone-should-read/ (accessed on 15 March 2019).
- Delponte, L. European Artificial Intelligence (AI) Leadership, the Path for an Integrated Vision; European Parliament’s Committee on Industry, Research and Energy: Strasbourg, France, 2018. [Google Scholar]
- European Comission. Digital Transformation Monitor USA-China-EU Plans for AI: Where Do We Stand? European Comission: Strasbourg, France, 2018. [Google Scholar]
- Walch, K. Is South Korea Poised to Be a Leader in AI? 2018. Available online: https://www.forbes.com/sites/cognitiveworld/2018/09/07/is-south-korea-poised-to-be-a-leader-in-ai/#258bc6bdfa2f (accessed on 16 March 2019).
- Chitturu, S.; Lin, D.-Y.; Sneader, K.; Tonby, O.; Woetzel, J. Artificial intelligence and Southeast Asia’s future. In Singapore Summit 2017; McKinsey Global Institute: Washington, DC, USA, 2017. [Google Scholar]
- Bastanlar, Y.; Ozuysal, M. Introduction to machine learning. Methods Mol. Biol. 2014, 1107, 105–128. [Google Scholar] [PubMed]
- Chekroud, A.M.; Zotti, R.J.; Shehzad, Z.; Gueorguieva, R.; Johnson, M.K.; Trivedi, M.H.; Cannon, T.D.; Krystal, J.H.; Corlett, P.R. Cross-trial prediction of treatment outcome in depression: A machine learning approach. Lancet Psychiatry 2016, 3, 243–250. [Google Scholar] [CrossRef]
- Tamboer, P.; Vorst, H.C.M.; Ghebreab, S.; Scholte, H.S. Machine learning and dyslexia: Classification of individual structural neuro-imaging scans of students with and without dyslexia. Neuroimage Clin. 2016, 11, 508–514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathotaarachchi, S.; Pascoal, T.A.; Shin, M.; Benedet, A.L.; Kang, M.S.; Beaudry, T.; Fonov, V.S.; Gauthier, S.; Rosa-Neto, P. Alzheimer’s disease neuroimaging, I. Identifying incipient dementia individuals using machine learning and amyloid imaging. Neurobiol. Aging 2017, 59, 80–90. [Google Scholar] [CrossRef]
- Lee, Y.; Ragguett, R.M.; Mansur, R.B.; Boutilier, J.J.; Rosenblat, J.D.; Trevizol, A.; Brietzke, E.; Lin, K.; Pan, Z.; Subramaniapillai, M.; et al. Applications of machine learning algorithms to predict therapeutic outcomes in depression: A meta-analysis and systematic review. J. Affect. Disord. 2018, 241, 519–532. [Google Scholar] [CrossRef] [PubMed]
- Cochran, G.L.; Lander, L.; Morien, M.; Lomelin, D.E.; Brittin, J.; Reker, C.; Klepser, D.G. Consumer opinions of health information exchange, e-prescribing, and personal health records. Perspect. Health Inf. Manag. 2015, 12, 1e. [Google Scholar] [PubMed]
- Nunan, D.; Di Domenico, M. Market research and the ethics of big data. Int. J. Mark. Res. 2013, 55, 505–520. [Google Scholar] [CrossRef]
- Mittelstadt, B.D.; Floridi, L. The ethics of big data: Current and foreseeable issues in biomedical contexts. Sci. Eng. Ethics 2016, 22, 303–341. [Google Scholar] [CrossRef] [PubMed]
- Puschmann, C.; Burgess, J. Metaphors of big data. Int. J. Commun. 2014, 8, 1690–1709. [Google Scholar]
- Choudhury, S.; Fishman, J.R.; McGowan, M.L.; Juengst, E.T. Big data, open science and the brain: Lessons learned from genomics. Front. Hum. Neurosci. 2014, 8, 239. [Google Scholar] [CrossRef] [PubMed]
- King, T.C.; Aggarwal, N.; Taddeo, M.; Floridi, L. Artificial intelligence crime: An interdisciplinary analysis of foreseeable threats and solutions. Sci. Eng. Ethics 2019. [Google Scholar] [CrossRef]
- Tene, O.; Polonetsky, J. Big data for all: Privacy and user control in the age of analytics. Northwestern J. Technol. Intellect. Prop. 2013, 11, 240–273. [Google Scholar]
- Zhang, M.W.; Ho, R.C.; McIntyre, R.S. The ‘WikiGuidelines’smartphone application: Bridging the gaps in availability of evidence-based smartphone mental health applications. Technol. Health Care 2016, 24, 587–590. [Google Scholar] [CrossRef]
- Zhang, M.W.; Tsang, T.; Cheow, E.; Ho, C.; Yeong, N.B.; Ho, R.C. Enabling psychiatrists to be mobile phone app developers: Insights into app development methodologies. JMIR mHealth uHealth 2014, 2, e53. [Google Scholar] [CrossRef]
- Tran, B.X.; Zhang, M.W.; Le, H.T.; Nguyen, H.D.; Nguyen, L.H.; Nguyen, Q.L.T.; Tran, T.D.; Latkin, C.A.; Ho, R.C. What drives young vietnamese to use mobile health innovations? Implications for health communication and behavioral interventions. JMIR mHealth uHealth 2018, 6, e194. [Google Scholar] [CrossRef] [PubMed]
- Do, T.T.T.; Le, M.D.; Van Nguyen, T.; Tran, B.X.; Le, H.T.; Nguyen, H.D.; Nguyen, L.H.; Nguyen, C.T.; Tran, T.D.; Latkin, C.A.; et al. Receptiveness and preferences of health-related smartphone applications among Vietnamese youth and young adults. BMC Public Health 2018, 18, 764. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.W.; Ward, J.; Ying, J.J.; Pan, F.; Ho, R.C. The alcohol tracker application: An initial evaluation of user preferences. BMJ Innov. 2016, 2, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Cheow, E.; Ho, C.; Ng, B.Y.; Ho, R.; Cheok, C.C. Application of low-cost methodologies for mobile phone app development. JMIR mHealth uHealth 2014, 2, e55. [Google Scholar] [CrossRef] [PubMed]
- Peek, N.; Combi, C.; Marin, R.; Bellazzi, R. Thirty years of artificial intelligence in medicine (AIME) conferences: A review of research themes. Artif. Intell. Med. 2015, 65, 61–73. [Google Scholar] [CrossRef] [PubMed]
- Patel, V.L.; Shortliffe, E.H.; Stefanelli, M.; Szolovits, P.; Berthold, M.R.; Bellazzi, R.; Abu-Hanna, A. The coming of age of artificial intelligence in medicine. Artif. Intell. Med. 2009, 46, 5–17. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Data | Unit of Analysis | Analytical Methods | Presentations of Results |
|---|---|---|---|
| Keywords, countries | Words | Frequency of co-occurrence | Map of keywords clusters |
| Abstracts | Words | Exploratory factors analyses | Top 50 constructed research domains. Clustering map of the landscapes constructed by these domains. |
| Abstracts | Papers | Latent Dirichlet Allocation | 10 classifications of research topics |
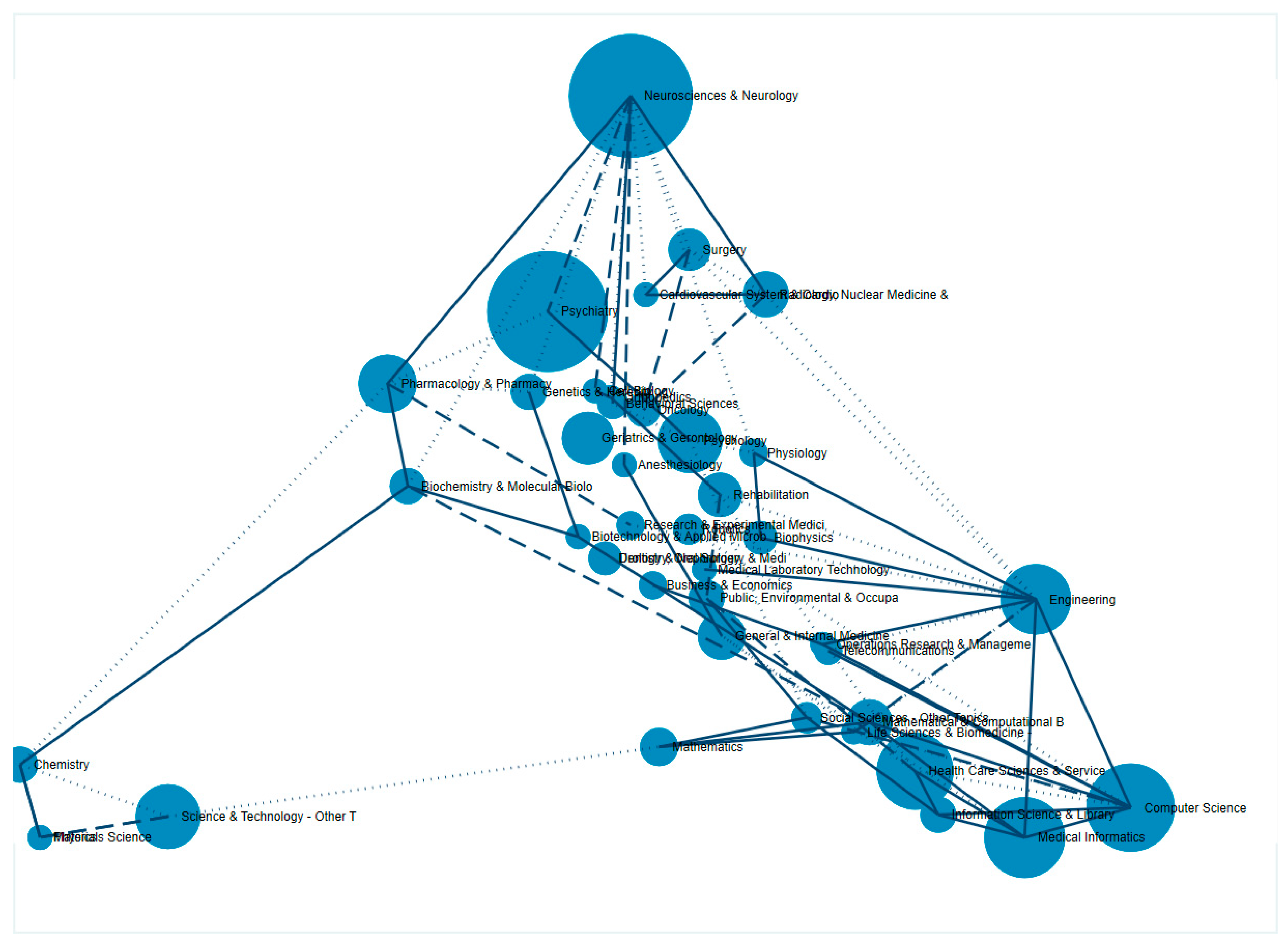
| WoS classification of research areas | WoS research areas | Frequency of co-occurrence | Dendrogram of research disciplines |
| Year Published | Total Number of Papers | Total Citations | Mean Cite Rate Per Year 1 | Total Usage 2 Last 6 Month | Total Usage 2 Last 5 Years | Mean Use Rate Last 6 Month 3 | Mean Use Rate Last 5 Year 4 |
|---|---|---|---|---|---|---|---|
| 2018 | 117 | 126 | 738 | 1121 | 6.31 | 1.92 | |
| 2017 | 68 | 296 | 4.35 | 210 | 2076 | 3.09 | 6.11 |
| 2016 | 43 | 476 | 5.53 | 117 | 1019 | 2.72 | 4.74 |
| 2015 | 55 | 934 | 5.66 | 88 | 984 | 1.60 | 3.58 |
| 2014 | 27 | 577 | 5.34 | 33 | 478 | 1.22 | 3.54 |
| 2013 | 29 | 676 | 4.66 | 39 | 743 | 1.34 | 5.12 |
| 2012 | 12 | 871 | 12.10 | 41 | 522 | 3.42 | 8.70 |
| 2011 | 10 | 403 | 5.76 | 15 | 227 | 1.50 | 4.54 |
| 2010 | 6 | 159 | 3.31 | 1 | 40 | 0.17 | 1.33 |
| 2009 | 6 | 91 | 1.69 | 4 | 42 | 0.67 | 1.40 |
| 2008 | 4 | 30 | 0.75 | 0 | 16 | 0.00 | 0.80 |
| 2007 | 5 | 98 | 1.78 | 3 | 39 | 0.60 | 1.56 |
| 2006 | 4 | 10 | 0.21 | 0 | 5 | 0.00 | 0.25 |
| 2005 | 1 | 1 | 0.08 | 0 | 0 | 0.00 | 0.00 |
| 2004 | 2 | 44 | 1.57 | 0 | 7 | 0.00 | 0.70 |
| 2003 | 1 | 31 | 2.07 | 0 | 4 | 0.00 | 0.80 |
| 2002 | 2 | 31 | 0.97 | 0 | 4 | 0.00 | 0.40 |
| 2001 | 2 | 25 | 0.74 | 0 | 9 | 0.00 | 0.90 |
| 1999 | 2 | 20 | 0.53 | 0 | 6 | 0.00 | 0.60 |
| 1993 | 1 | 9 | 0.36 | 0 | 0 | 0.00 | 0.00 |
| Country Settings | Frequency | % | |
|---|---|---|---|
| 1 | United States | 26 | 32.9% |
| 2 | Ireland | 10 | 12.7% |
| 3 | United Kingdom | 8 | 10.1% |
| 4 | Australia | 3 | 3.8% |
| 5 | India | 3 | 3.8% |
| 6 | New Zealand | 3 | 3.8% |
| 7 | Spain | 3 | 3.8% |
| 8 | China | 2 | 2.5% |
| 9 | France | 2 | 2.5% |
| 10 | Japan | 2 | 2.5% |
| 11 | Netherlands | 2 | 2.5% |
| 12 | Taiwan | 2 | 2.5% |
| 13 | Afghanistan | 1 | 1.3% |
| 14 | Chile | 1 | 1.3% |
| 15 | Germany | 1 | 1.3% |
| 16 | Hong Kong | 1 | 1.3% |
| 17 | Iran | 1 | 1.3% |
| 18 | Italy | 1 | 1.3% |
| 19 | Malaysia | 1 | 1.3% |
| 20 | Mexico | 1 | 1.3% |
| 21 | Portugal | 1 | 1.3% |
| 22 | South Africa | 1 | 1.3% |
| 23 | Sweden | 1 | 1.3% |
| 24 | Switzerland | 1 | 1.3% |
| 25 | Wallis and Futuna | 1 | 1.3% |
| Number | Name | Keywords | Eigenvalue | Frequency | % Cases |
|---|---|---|---|---|---|
| 1 | Predictors; Predicted | predictors; predicted; prediction; predict; predicting; clinical; characteristics; predictive; variables | 1.56 | 568 | 63.0% |
| 2 | Machine Learning | learning; machine; algorithms; techniques | 1.99 | 511 | 61.2% |
| 3 | Resting-State; Functional Connectivity | resting; state; connectivity; functional magnetic resonance imaging (fMRI); controls; power; classifiers; functional; linear; healthy | 2.40 | 408 | 50.4% |
| 4 | Mental Health | mental; health; stress; real; problems; psychological | 2.12 | 333 | 50.1% |
| 5 | Depressive | depressive; major; major depressive disorder (MDD); disorder; remission | 2.69 | 352 | 45.8% |
| 6 | Diagnosis; Accuracy | diagnosis; accuracy; predictions; accurate | 1.72 | 247 | 43.3% |
| 7 | Antidepressant; Treatment Response | antidepressant; response; treatment-resistant depression (TRD); treatment; remission | 2.90 | 241 | 39.3% |
| 8 | Bipolar; Mood Disorders | bipolar; mood; bipolar disorder (BD); disorders | 3.12 | 229 | 38.3% |
| 9 | Imaging; Structural | imaging; structural; magnetic; magnetic resonance imaging (MRI); matter; brain; functional; neuroimaging; volume | 16.70 | 366 | 37.3% |
| 10 | Stroke; Rehabilitation | stroke; rehabilitation; robotic; assisted; upper; motor; function; gait; therapy; effectiveness; sessions; stimulation | 5.43 | 308 | 36.8% |
| 11 | Feature Selection; Features | feature; selection; features; framework; validation | 2.40 | 233 | 34.0% |
| 12 | Fear; Report | fear; report; anxiety; sad | 1.67 | 163 | 33.8% |
| 13 | Field; Application | field; applications; application; future; recent | 1.82 | 201 | 33.5% |
| 14 | Pain; Quality of Life (Qol) | pain; qol; follow; outcome; hospital; surgery; week; robotic; mobility | 1.99 | 240 | 33.5% |
| 15 | Artificial Neural | neural; artificial; artificial neural networks (ANN); network; networks | 2.66 | 232 | 31.5% |
| 16 | Trial; Randomized | trial; randomized; week; trials; outcomes; efficacy; weeks | 2.57 | 232 | 31.2% |
| 17 | Faces; Fmri | faces; fmri; pattern; independent; depressed; sad; samples | 2.03 | 181 | 30.2% |
| 18 | Human-Computer; Abnormalities | human-computer; abnormalities; neurocognitive; controls; healthy; automated | 2.07 | 181 | 28.5% |
| 19 | Support Vector | vector; support; support vector machine (SVM); classifier | 3.39 | 200 | 27.5% |
| 20 | Parkinson | parkinson; Parkinson’s disease (PD); disease; motor | 2.21 | 146 | 27.0% |
| 21 | Investigated; Previous | investigated; previous; risk | 1.96 | 133 | 27.0% |
| 22 | Effective; Cost | effective; cost; provided; psychological | 1.91 | 137 | 26.2% |
| 23 | Paro; Dementia | paro; dementia; elderly; robot; care; sessions | 2.98 | 148 | 24.7% |
| 24 | Classifiers; Process | classifiers; process; applied | 1.65 | 118 | 23.9% |
| 25 | Negative Symptoms | symptoms; negative | 2.19 | 105 | 22.7% |
| 26 | Behavior; Systems | behavior; systems; mobile; monitoring; technologies | 2.26 | 127 | 22.2% |
| 27 | Biomarkers; Markers | biomarkers; markers; neuroimaging; patterns | 2.05 | 122 | 21.9% |
| 28 | Statistical; Complex | statistical; complex; index | 1.77 | 100 | 20.4% |
| 29 | Posts; Social Media | posts; media; communities; content; online; social | 3.77 | 134 | 19.9% |
| 30 | Schizophrenia; Psychiatric | schizophrenia; psychiatric; illness | 1.76 | 98 | 19.7% |
| 31 | Quality | quality; life; qol; mobility | 2.48 | 128 | 19.7% |
| 32 | Physical Activity | activity; physical | 1.69 | 94 | 19.7% |
| 33 | Cognitive Impairment | impairment; greater; cognitive | 1.72 | 99 | 19.7% |
| 34 | Radical Prostatectomy; Surgery | radical; prostatectomy; surgery; cancer; underwent; open; assisted | 3.35 | 116 | 18.1% |
| 35 | Area Under Curve; Area | auc; area; achieved | 1.81 | 90 | 17.9% |
| 36 | Investigate | investigate; aim | 1.63 | 78 | 17.1% |
| 37 | Technology; Home | technology; home; technologies; reduce | 1.71 | 87 | 16.4% |
| 38 | Natural Language | language; natural; processing; suicide | 2.35 | 111 | 16.1% |
| 39 | Testing | testing; identification; cohort | 1.97 | 75 | 15.4% |
| 40 | Gene | genes; gene; genetic; refSNP (rs); association; interaction | 4.06 | 96 | 15.1% |
| 41 | Drug | drug; development | 1.62 | 63 | 14.1% |
| 42 | Sensitivity | sensitivity; specificity; suicide | 2.27 | 101 | 13.9% |
| 43 | Medical | medical | 1.61 | 48 | 12.1% |
| 44 | Single | single | 1.55 | 45 | 11.3% |
| 45 | Detection; EEG Signals | detection; signals; electroencephalography (EEG) | 1.68 | 58 | 11.1% |
| 46 | Responses; Psychosis | responses; psychosis; affective | 1.91 | 53 | 10.8% |
| 47 | Beta; Adults | beta; adults; context | 1.86 | 50 | 10.8% |
| 48 | Addition | addition | 1.64 | 37 | 9.3% |
| 49 | Ability; Responders | ability; responders | 1.58 | 39 | 9.1% |
| 50 | Primary | primary | 1.53 | 36 | 9.1% |
| Number | Research Areas | Frequency | Percent |
|---|---|---|---|
| 1 | Genomics and computational modeling in depression | 21 | 6.0% |
| 2 | Depression as an outcome in AI and robotic assisted surgery | 33 | 9.4% |
| 3 | The use of AI and electroencephalography in the diagnosis of depression | 60 | 17.1% |
| 4 | The impact of social media and online communities on depression | 25 | 7.1% |
| 5 | The use of AI in the psychological intervention for depression | 24 | 6.8% |
| 6 | The use of AI to assess the use of alternative treatment | 17 | 4.8% |
| 7 | The use of pattern recognition by artificial intelligence, neuro-morphometric, and neuro-imaging in the diagnosis of depression | 63 | 17.9% |
| 8 | The use of biomarkers and machine learning in clinical risk stratification of depression | 40 | 11.4% |
| 9 | Behavioral pattern monitoring and possible interventions for depression through telehealth and mobile applications | 43 | 12.3% |
| 10 | The use of AI in electronic health records to predict the outcome of depression and suicide | 25 | 7.1% |
| Total | 351 | 100% |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tran, B.X.; McIntyre, R.S.; Latkin, C.A.; Phan, H.T.; Vu, G.T.; Nguyen, H.L.T.; Gwee, K.K.; Ho, C.S.H.; Ho, R.C.M. The Current Research Landscape on the Artificial Intelligence Application in the Management of Depressive Disorders: A Bibliometric Analysis. Int. J. Environ. Res. Public Health 2019, 16, 2150. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16122150
Tran BX, McIntyre RS, Latkin CA, Phan HT, Vu GT, Nguyen HLT, Gwee KK, Ho CSH, Ho RCM. The Current Research Landscape on the Artificial Intelligence Application in the Management of Depressive Disorders: A Bibliometric Analysis. International Journal of Environmental Research and Public Health. 2019; 16(12):2150. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16122150
Chicago/Turabian StyleTran, Bach Xuan, Roger S. McIntyre, Carl A. Latkin, Hai Thanh Phan, Giang Thu Vu, Huong Lan Thi Nguyen, Kenneth K. Gwee, Cyrus S. H. Ho, and Roger C. M. Ho. 2019. "The Current Research Landscape on the Artificial Intelligence Application in the Management of Depressive Disorders: A Bibliometric Analysis" International Journal of Environmental Research and Public Health 16, no. 12: 2150. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16122150