Association between Ambulatory Status and Functional Disability in Elderly People with Dementia

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
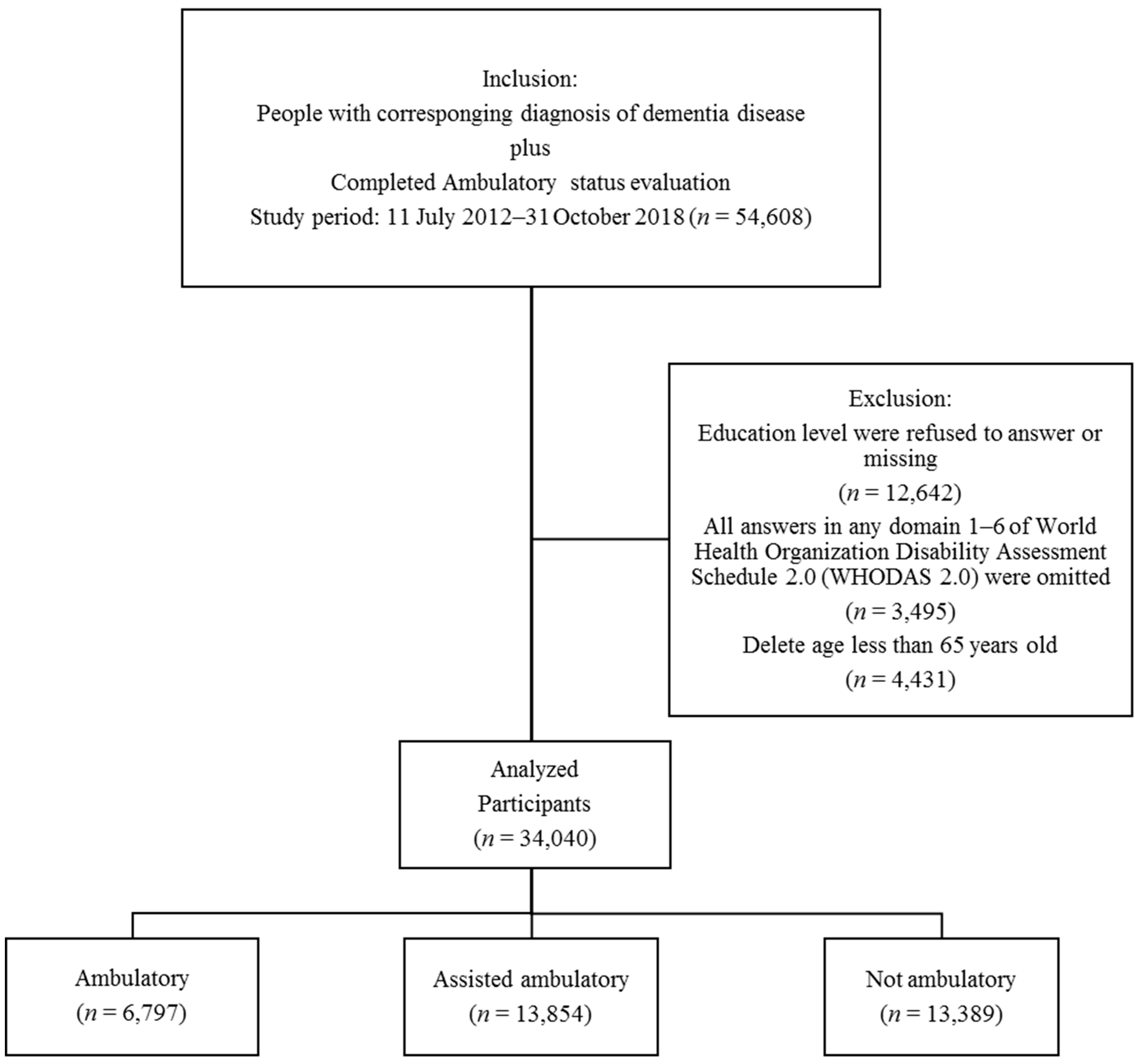
2.1. Participants
2.2. Research Tools
2.2.1. Clinical Dementia Rating
2.2.2. WHODAS 2.0
2.2.3. Ambulatory Status
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Ambulatory | Assisted Ambulatory | Nonambulatory | p Value | |
|---|---|---|---|---|
| 65–74 years | ||||
| Getting along (mean ± SD) | ||||
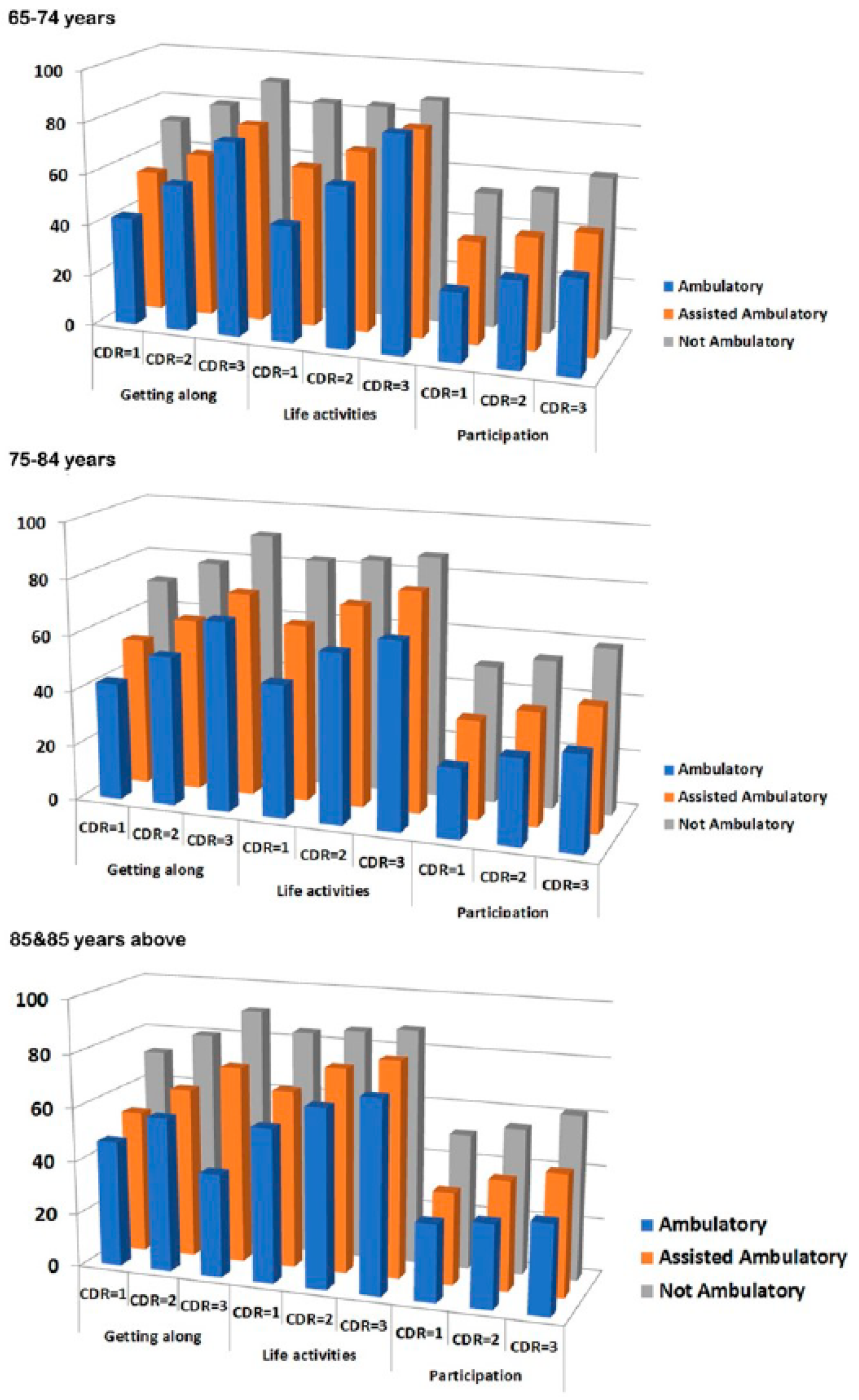
| CDR = 1 | 42.3 ± 27.8 | 55.4 ± 25.9 | 71.9 ± 24.9 | <0.0001 |
| CDR = 2 | 57.1 ± 26.5 | 64.0 ± 25.6 | 79.8 ± 22.5 | <0.0001 |
| CDR ≥ 3 | 75.5 ± 26.1 | 77.4 ± 23.7 | 90.5 ± 17.1 | <0.0001 |
| Life activities (mean ± SD) | ||||
| CDR = 1 | 45.5 ± 33.6 | 64.6 ± 33.6 | 83.6 ± 32.5 | <0.0001 |
| CDR = 2 | 62.6 ± 33.9 | 70.6 ± 35.0 | 83.7 ± 33.5 | <0.0001 |
| CDR ≥ 3 | 75.9 ± 34.1 | 80.9 ± 30.7 | 87.3 ± 30.6 | 0.0001 |
| Participation (mean ± SD) | ||||
| CDR = 1 | 27.0 ± 19.2 | 40.0 ± 21.3 | 53.1 ± 23.4 | <0.0001 |
| CDR = 2 | 33.8 ± 20.1 | 43.7 ± 21.5 | 55.5 ± 23.7 | <0.0001 |
| CDR ≥ 3 | 36.9 ± 19.3 | 47.3 ± 23.2 | 62.9 ± 25.8 | <0.0001 |
| 75–84 years | ||||
| Getting along (mean ± SD) | ||||
| CDR = 1 | 42.3 ± 27.1 | 53.1 ± 26.0 | 70.8 ± 26.2 | <0.0001 |
| CDR = 2 | 53.8 ± 27.5 | 62.1 ± 25.6 | 78.7 ± 23.3 | <0.0001 |
| CDR ≥ 3 | 68.1 ± 28.8 | 73.4 ± 23.8 | 90.3 ± 17.4 | <0.0001 |
| Life activities (mean ± SD) | ||||
| CDR = 1 | 47.8 ± 34.0 | 63.7 ± 34.9 | 82.6 ± 33.5 | <0.0001 |
| CDR = 2 | 60.8 ± 35.4 | 72.4 ± 33.8 | 84.2 ± 33.0 | <0.0001 |
| CDR ≥ 3 | 66.8 ± 38.3 | 79.0 ± 31.9 | 86.8 ± 31.2 | <0.0001 |
| Participation (mean ± SD) | ||||
| CDR = 1 | 25.0 ± 18.1 | 35.6 ± 20.9 | 49.4 ± 22.4 | <0.0001 |
| CDR = 2 | 30.9 ± 20.0 | 40.8 ± 21.4 | 53.4 ± 24.3 | <0.0001 |
| CDR ≥ 3 | 34.4 ± 22.1 | 44.7 ± 23.3 | 59.4 ± 26.1 | <0.0001 |
| ≥85 years | ||||
| Getting along (mean ± SD) | ||||
| CDR = 1 | 47.0 ± 30.2 | 53.3 ± 26.4 | 72.4 ± 25.8 | <0.0001 |
| CDR = 2 | 57.6 ± 28.5 | 63.6 ± 25.3 | 80.2 ± 23.0 | <0.0001 |
| CDR ≥ 3 | 68.8 ± 32.8 | 73.6 ± 24.8 | 90.7 ± 16.9 | <0.0001 |
| Life activities (mean ± SD) | ||||
| CDR = 1 | 57.5 ± 37.5 | 66.3 ± 35.8 | 84 ± 33.1 | <0.0001 |
| CDR = 2 | 66.7 ± 36.2 | 76.4 ± 33.3 | 86 ± 31.4 | <0.0001 |
| CDR ≥ 3 | 71.8 ± 37.7 | 80.7 ± 30.6 | 87.7 ± 30.5 | 0.0005 |
| Participation (mean ± SD) | ||||
| CDR = 1 | 28.9 ± 20.3 | 34.4 ± 20.1 | 50.4 ± 23.2 | <0.0001 |
| CDR = 2 | 31.2 ± 18.9 | 40.8 ± 21.7 | 54.5 ± 24.0 | <0.0001 |
| CDR ≥ 3 | 33.5 ± 24.3 | 45.3 ± 22.8 | 61.2 ± 25.6 | <0.0001 |
References
- Prince, M.J. World Alzheimer Report 2015: The Global Impact of Dementia: An Analysis of Prevalence, Incidence, Cost and Trends; Alzheimer’s Disease International: London, UK, 2015. [Google Scholar]
- Ferri, C.P.; Prince, M.; Brayne, C.; Brodaty, H.; Fratiglioni, L.; Ganguli, M.; Hall, K.; Hasegawa, K.; Hendrie, H.; Huang, Y.; et al. Global prevalence of dementia: A Delphi consensus study. Lancet 2005, 366, 2112–2117. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Pub: Washington, DC, USA, 2013. [Google Scholar]
- Caselli, R.J. (Ed.) Current issues in the diagnosis and management of dementia. In Seminars in Neurology; Thieme Medical Publishers: New York, NY, USA, 2003. [Google Scholar]
- Sun, M.; Mainland, B.J.; Ornstein, T.J.; Mallya, S.; Fiocco, A.J.; Sin, G.L.; Shulman, K.I.; Herrmann, N. The association between cognitive fluctuations and activities of daily living and quality of life among institutionalized patients with dementia. Int. J. Geriatr. Psychiatry 2018, 33, e280–e285. [Google Scholar] [CrossRef] [PubMed]
- Verghese, J.; Holtzer, R.; Lipton, R.B.; Wang, C. Quantitative gait markers and incident fall risk in older adults. J. Gerontol. Ser. A 2009, 64, 896–901. [Google Scholar] [CrossRef] [PubMed]
- Rogers, C. Presbyastasis: A multifactorial cause of balance problems in the elderly. S. Afr. Fam. Pract. 2010, 52, 431–434. [Google Scholar] [CrossRef]
- Azadian, E.; Torbati, H.R.T.; Kakhki, A.R.S.; Farahpour, N. The effect of dual task and executive training on pattern of gait in older adults with balance impairment: A Randomized controlled trial. Arch. Gerontol. Geriatr. 2016, 62, 83–89. [Google Scholar] [CrossRef]
- Prevention, O.F.; Panel, O.S. Guideline for the prevention of falls in older persons. J. Am. Geriatr. Soc. 2001, 49, 664–672. [Google Scholar]
- Manckoundia, P.; Pfitzenmeyer, P.; d’Athis, P.; Dubost, V.; Mourey, F. Impact of cognitive task on the posture of elderly subjects with Alzheimer’s disease compared to healthy elderly subjects. Mov. Disord. 2006, 21, 236–241. [Google Scholar] [CrossRef]
- Wang, L.; Larson, E.B.; Bowen, J.D.; van Belle, G. Performance-based physical function and future dementia in older people. Arch. Intern. Med. 2006, 166, 1115–1120. [Google Scholar] [CrossRef]
- Verghese, J.; Wang, C.; Lipton, R.B.; Holtzer, R.; Xue, X. Quantitative gait dysfunction and risk of cognitive decline and dementia. J. Neurol. Neurosurg. Psychiatry 2007, 78, 929–935. [Google Scholar] [CrossRef]
- Allali, G.; Assal, F.; Kressig, R.W.; Dubost, V.; Herrmann, F.R.; Beauchet, O. Impact of impaired executive function on gait stability. Dement. Geriatr. Cogn. Disord. 2008, 26, 364–369. [Google Scholar] [CrossRef]
- IJmker, T.; Lamoth, C.J. Gait and cognition: The relationship between gait stability and variability with executive function in persons with and without dementia. Gait Posture 2012, 35, 126–130. [Google Scholar] [CrossRef] [PubMed]
- Üstün, T.B.; Chatterji, S.; Kostanjsek, N.; Rehm, J.; Kennedy, C.; Epping-Jordan, J.; Saxena, S.; Korff, M.V.; Pull, C. Developing the World Health Organization disability assessment schedule 2.0. Bull. World Health Organ. 2010, 88, 815–823. [Google Scholar] [CrossRef] [PubMed]
- Gold, L.H. DSM-5 and the assessment of functioning: The World Health Organization Disability Assessment Schedule 2.0 (WHODAS 2.0). J. Am. Acad. Psychiatry Law Online 2014, 42, 173–181. [Google Scholar]
- Hughes, C.P.; Berg, L.; Danziger, W.; Coben, L.A.; Martin, R.L. A new clinical scale for the staging of dementia. Br. J. Psychiatry 1982, 140, 566–572. [Google Scholar] [CrossRef] [PubMed]
- Chiu, T.Y.; Yen, C.F.; Chou, C.H.; Lin, J.D.; Hwang, A.W.; Liao, H.F.; Chi, W.C. Development of traditional Chinese version of World Health Organization Disability Assessment Schedule 2.0 36–item (WHODAS 2.0) in Taiwan: Validity and reliability analyses. Res. Dev. Disabil. 2014, 35, 2812–2820. [Google Scholar] [CrossRef] [PubMed]
- Gabell, A.; Nayak, U. The effect of age on variability in gait. J. Gerontol. 1984, 39, 662–666. [Google Scholar] [CrossRef]
- Snijders, A.H.; Van De Warrenburg, B.P.; Giladi, N.; Bloem, B.R. Neurological gait disorders in elderly people: Clinical approach and classification. Lancet Neurol. 2007, 6, 63–74. [Google Scholar] [CrossRef]
- Woollacott, M.; Shumway-Cook, A. Attention and the control of posture and gait: A review of an emerging area of research. Gait Posture 2002, 16, 1–14. [Google Scholar] [CrossRef]
- Beauchet, O.; Allali, G.; Berrut, G.; Hommet, C.; Dubost, V.; Assal, F. Gait analysis in demented subjects: Interests and perspectives. Neuropsychiatr. Dis. Treat. 2008, 4, 155. [Google Scholar] [CrossRef]
- Almazán-Isla, J.; Comín-Comín, M.; Damián, J.; Alcalde-Cabero, E.; Ruiz, C.; Franco, E.; Martín, G.; Larrosa-Montañés, L.A.; de Pedro-Cuesta, J.; DISCAP-ARAGON Research Group. Analysis of disability using WHODAS 2.0 among the middle-aged and elderly in Cinco Villas, Spain. Disabil. Health J. 2014, 7, 78–87. [Google Scholar] [CrossRef]
- Huang, S.W.; Chang, K.H.; Escorpizo, R.; Hu, C.J.; Chi, W.C.; Yen, C.F.; Liao, H.F.; Chiu, W.T.; Liou, T.H. Using the World Health Organization Disability Assessment Schedule 2.0 (WHODAS 2.0) for predicting institutionalization of patients with dementia in Taiwan. Medicine 2015, 94, e2155. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.; Ye, B.; Chen, P.; Wang, Q.; Fan, C.; Shu, Y.; Xiang, M. Cognitive Decline, dementia, Alzheimer’s disease and presbycusis: Examination of the possible molecular mechanism. Front. Neurzosci. 2018, 12, 394. [Google Scholar] [CrossRef] [PubMed]
- Brandt, T. Vertigo, Dizziness, and Falls in the Elderly; Vertigo Springer: New York, NY, USA, 2003; pp. 385–392. [Google Scholar]


| Ambulatory (n = 6797) | Assisted Ambulatory (n = 13,854) | Nonambulatory (n = 13,389) | p-Value | |
|---|---|---|---|---|
| Sex (n, %) | 0.5100 | |||
| Male | 2592, 38.1% | 5398, 39.0% | 5192, 38.8% | |
| Female | 4205, 61.9% | 8456, 61.0% | 8197, 61.2% | |
| Age (years) (n, %) | <0.0001 | |||
| 65–74 | 2413, 35.5% | 3348, 24.2% | 2545, 19.0% | |
| 75–84 | 3969, 58.4% | 8618, 62.2% | 7778, 59.1% | |
| ≥85 | 415, 6.1% | 1888, 13.6% | 3066, 22.9% | |
| Total (mean ± SD) | 76.8 ± 5.7 | 79.0 ± 6.1 | 80.6 ± 6.6 | <0.0001 |
| Education level (n, %) | <0.0001 | |||
| Above college | 54, 0.8% | 132, 1.0% | 133, 1.0% | |
| Senior high | 315, 4.6% | 663, 4.8% | 606, 4.5% | |
| Junior high | 264, 3.9% | 578, 4.2% | 617, 4.6% | |
| Primary | 5217, 76.8% | 9712, 70.1% | 8092, 60.4% | |
| Illiterate | 947, 13.9% | 2769, 20.0% | 3941, 29.4% | |
| Residence (n, %) | <0.0001 | |||
| Community dwelling | 6469, 95.2% | 12,158, 87.8% | 8196, 61.2% | |
| Institution | 328, 4.8% | 1696, 12.2% | 5193, 38.8% | |
| Urbanization level (n, %) | <0.0001 | |||
| Rural | 914, 13.5% | 2106, 15.2% | 2084, 15.6% | |
| Suburban | 2320, 34.1% | 5117, 36.9% | 5522, 41.2% | |
| Urban | 3563, 52.4% | 6631, 47.9% | 5783, 43.2% | |
| Clinical Dementia Rating | <0.0001 | |||
| 1 | 4255, 62.6% | 5715, 41.3% | 1969, 14.7% | |
| 2 | 2209, 32.5% | 6054, 43.7% | 4727, 35.3% | |
| ≥3 | 333, 4.9% | 2085, 15.1% | 6693, 50.0% | |
| WHODAS 2.0 (mean ± SD) | ||||
| Cognition (domain 1) | 46.9 ± 24.7 | 56.6 ± 23.6 | 79.3 ± 22.3 | <0.0001 |
| Mobility (domain 2) | 17.3 ± 18.6 | 45.1 ± 23.6 | 77.7 ± 22.9 | <0.0001 |
| Self-care (domain 3) | 16.7 ± 18.3 | 32.4 ± 25.4 | 53.0 ± 35.1 | <0.0001 |
| Getting along (domain 4) | 48.0 ± 28.6 | 60.8 ± 26.5 | 83.6 ± 22.1 | <0.0001 |
| Life activities (domain 5) | 53.3 ± 35.4 | 70.2 ± 34.4 | 85.6 ± 32.0 | <0.0001 |
| Participation (domain 6) | 28.3 ± 19.5 | 40.1 ± 21.8 | 56.7 ± 25.2 | <0.0001 |
| Summary | 34.4 ± 17.0 | 49.7 ± 18.2 | 71.5 ± 17.9 | <0.0001 |
| β | Odds Ratio | 95% Wald Confidence Limits | p Value | ||
|---|---|---|---|---|---|
| Intercept | −2.1371 | <0.0001 | |||
| Sex (ref = Female) | |||||
| Male | 0.0144 | 1.014 | 0.963 | 1.069 | 0.5910 |
| Age (years) (ref = 65–74) | |||||
| 75–84 | 0.3239 | 1.383 | 1.298 | 1.473 | <0.0001 |
| ≥85 | 0.7842 | 2.191 | 2.016 | 2.380 | <0.0001 |
| Residence (ref = Community dwelling) | |||||
| Institution | 1.3374 | 3.809 | 3.576 | 4.058 | <0.0001 |
| Urbanization level (ref = Urban) | |||||
| Rural | 0.0742 | 1.077 | 0.999 | 1.161 | 0.0538 |
| Suburban | 0.1479 | 1.159 | 1.097 | 1.225 | <0.0001 |
| CDR (ref = 1) | |||||
| 2 | 0.8972 | 2.453 | 2.305 | 2.610 | <0.0001 |
| ≥3 | 2.2822 | 9.798 | 9.138 | 10.506 | <0.0001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, H.-H.; Hong, C.-T.; Wu, D.; Chi, W.-C.; Yen, C.-F.; Liao, H.-F.; Chan, L.; Liou, T.-H. Association between Ambulatory Status and Functional Disability in Elderly People with Dementia. Int. J. Environ. Res. Public Health 2019, 16, 2168. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16122168
Lee H-H, Hong C-T, Wu D, Chi W-C, Yen C-F, Liao H-F, Chan L, Liou T-H. Association between Ambulatory Status and Functional Disability in Elderly People with Dementia. International Journal of Environmental Research and Public Health. 2019; 16(12):2168. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16122168
Chicago/Turabian StyleLee, Hsun-Hua, Chien-Tai Hong, Dean Wu, Wen-Chou Chi, Chia-Feng Yen, Hua-Fang Liao, Lung Chan, and Tsan-Hon Liou. 2019. "Association between Ambulatory Status and Functional Disability in Elderly People with Dementia" International Journal of Environmental Research and Public Health 16, no. 12: 2168. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16122168