Comparison of Risk for End-Stage Renal Disease Between Physicians and the General Population: A Nationwide Population-Based Cohort Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
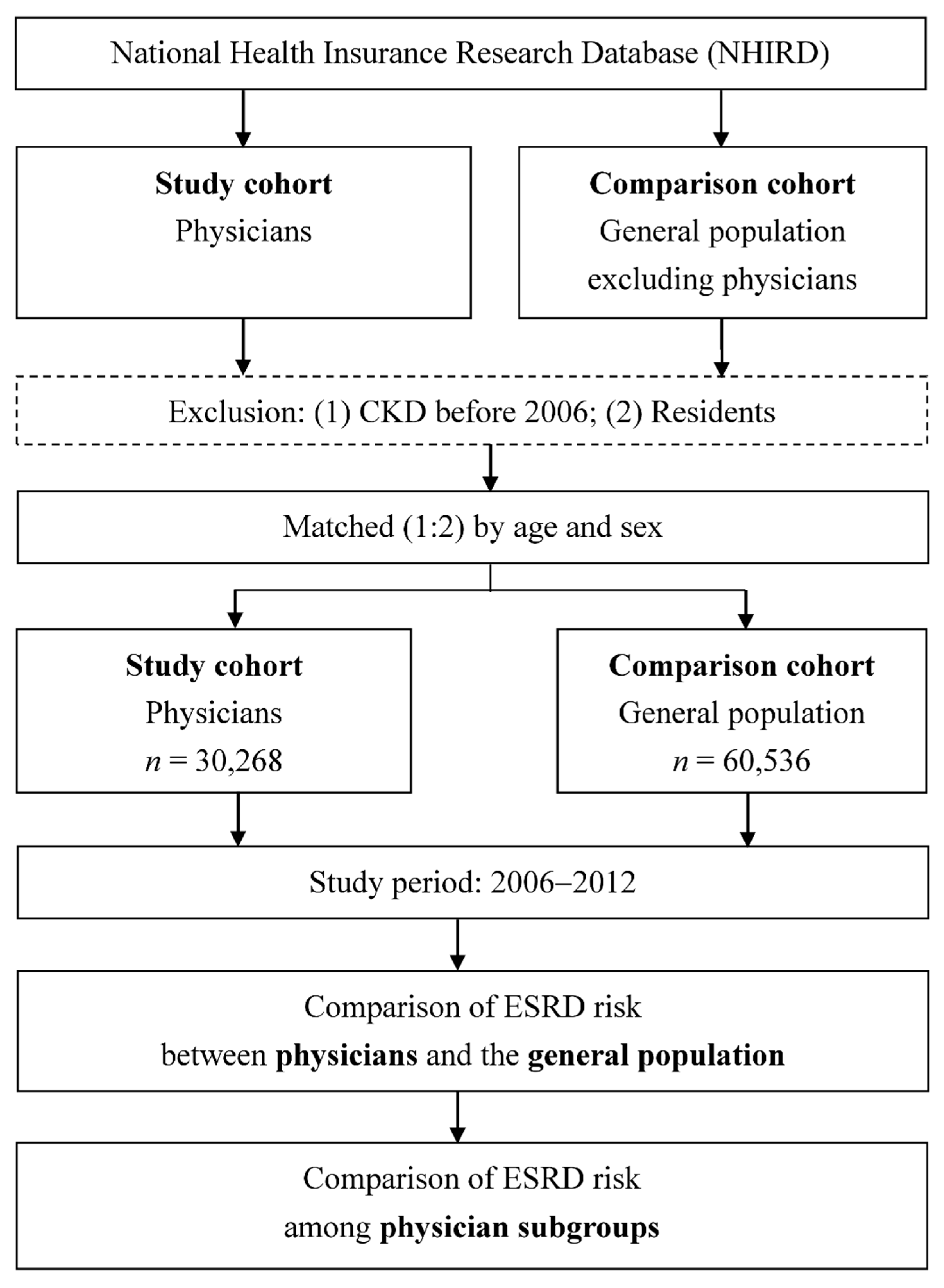
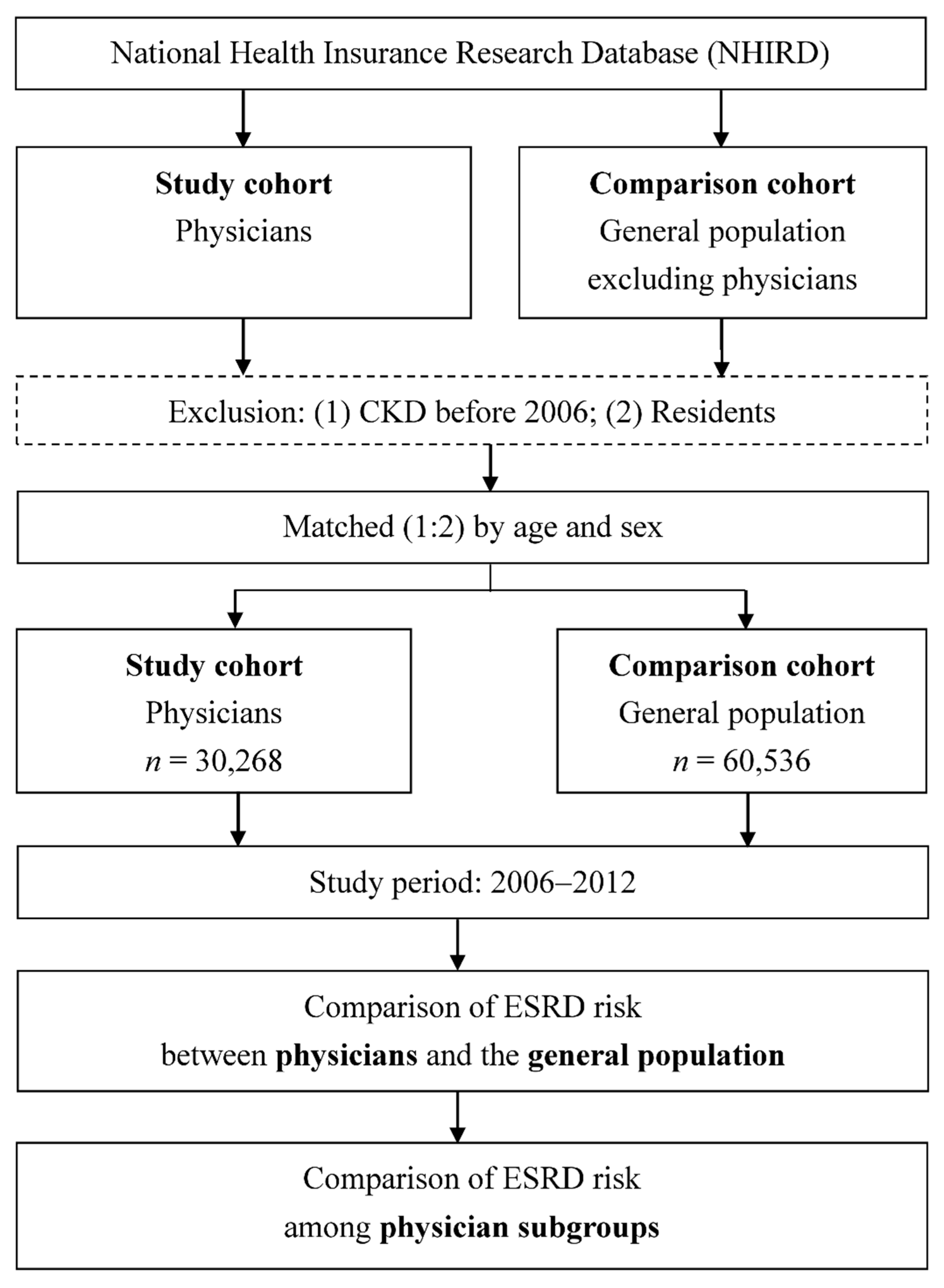
2.2. Identification of the Study Cohort (Physicians) and Comparison Cohort (General Population)
2.3. Comparison of ESRD Risk Between Physicians and the General Population and Among Physician Subgroups
2.4. Ethics Statement
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: Evaluation, classification, and stratification. Am. J. Kidney Dis. 2002, 39, S1–S266. [Google Scholar]
- United States Renal Data System. USRDS 2010 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States; National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2010.
- United States Renal Data System. USRDS 2013 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States; National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2013.
- United States Renal Data System. Chapter 10: International Comparisons. Available online: http://www.usrds.org/2014/view/v2_10.aspx (accessed on 19 January 2016).
- Weiner, D.E. Risk factors for ESRD: Lessons from a community study and implications for public health. Am. J. Kidney Dis. 2010, 55, 5–7. [Google Scholar] [CrossRef] [PubMed]
- Rubinstein, S.; Wang, C.; Qu, W. Occupational risk and chronic kidney disease: A population-based study in the United States adult population. Int. J. Nephrol. Renovasc. Dis. 2013, 6, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Guh, J.Y.; Chen, H.C.; Tsai, J.F.; Chuang, L.Y. Herbal therapy is associated with the risk of CKD in adults not using analgesics in Taiwan. Am. J. Kidney Dis. 2007, 49, 626–633. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.T.; Huang, C.C.; Weng, S.F.; Hsu, C.C.; Wang, J.J.; Lin, H.J.; Su, S.B.; Guo, H.R.; Juan, C.W. Acute myocardial infarction: A comparison of the risk between physicians and the general population. Biomed. Res. Int. 2015, 2015, 904328. [Google Scholar] [CrossRef]
- Shen, H.N.; Lu, C.L.; Li, C.Y. Do physicians have lower risk of severe sepsis and associated mortality? A matched cohort study. Crit. Care Med. 2014, 42, 816–823. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.S.; Hsu, C.C.; Weng, S.F.; Lin, H.J.; Wang, J.J.; Su, S.B.; Huang, C.C.; Guo, H.R. Cancer incidence in physicians: A Taiwan national population-based cohort study. Medicine 2015, 94, e2059. [Google Scholar] [CrossRef]
- Stavem, K.; Hofoss, D.; Aasland, O.G.; Loge, J.H. The self-perceived health status of Norwegian physicians compared with a reference population and foreign physicians. Scand. J. Public Health 2001, 29, 194–199. [Google Scholar] [CrossRef]
- Chiou, S.J.; Kung, P.T.; Naessens, J.M.; Huang, K.H.; Chang, Y.C.; Wang, Y.H.; Tsai, W.C. Do physicians with diabetes have differences in dialysis use and survival than other patients with diabetes. Diabetes Res. Clin. Pract. 2014, 105, 382–390. [Google Scholar] [CrossRef]
- Van Amelsvoort, L.G.; Schouten, E.G.; Maan, A.C.; Swenne, C.A.; Kok, F.J. Occupational determinants of heart rate variability. Int. Arch. Occup Environ. Health 2000, 73, 255–262. [Google Scholar] [CrossRef]
- Pickering, T.G. Mental stress as a causal factor in the development of hypertension and cardiovascular disease. Curr. Hypertens. Rep. 2001, 3, 249–254. [Google Scholar] [CrossRef]
- Grassi, G.; Bertoli, S.; Seravalle, G. Sympathetic nervous system: Role in hypertension and in chronic kidney disease. Curr. Opin. Nephrol. Hypertens. 2012, 21, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Grassi, G.; Quarti-Trevano, F.; Seravalle, G.; Arenare, F.; Volpe, M.; Furiani, S.; Dell’Oro, R.; Mancia, G. Early sympathetic activation in the initial clinical stages of chronic renal failure. Hypertension 2011, 57, 846–851. [Google Scholar] [CrossRef] [PubMed]
- Grassi, G.; Seravalle, G.; Arenare, F.; Buccianti, G.; Furiani, S.; Ilardo, V.; Bolla, G.; Mancia, G. Behaviour of regional adrenergic outflow in mild-to-moderate renal failure. J. Hypertens. 2009, 27, 562–566. [Google Scholar] [CrossRef] [PubMed]
- Schlaich, M.P. Sympathetic activation in chronic kidney disease: Out of the shadow. Hypertension 2011, 57, 683–685. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.Y.; Yang, C.M.; Lien, C.H.; Chiou, H.Y.; Lin, M.R.; Chang, H.R.; Chiu, W.T. Burnout, job satisfaction, and medical malpractice among physicians. Int. J. Med. Sci. 2013, 10, 1471–1478. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.F.; Lee, C.H.; Chang, R.E. Workload of attending physicians at an academic center in Taiwan. J. Chin. Med. Assoc. 2010, 73, 425–430. [Google Scholar] [CrossRef]
- Occupational Safety and Health Administration, Ministry of Labor. Working Time. Available online: http://www.mol.gov.tw/media/1544 (accessed on 16 January 2016).
- National Health Insurance Administration. National Health Insurance Annual Report 2014–2015; Ministry of Health and Welfare: Taiwan, China, 2014.
- Davis, J.W.; Chung, R.; Juarez, D.T. Prevalence of comorbid conditions with aging among patients with diabetes and cardiovascular disease. Hawaii Med. J. 2011, 70, 209–213. [Google Scholar] [PubMed]
- Guiding principles for the care of older adults with multimorbidity: An approach for clinicians. Guiding principles for the care of older adults with multimorbidity: An approach for clinicians: American Geriatrics Society Expert Panel on the Care of Older Adults with Multimorbidity. J. Am. Geriatr. Soc. 2012, 60, E1–E25. [Google Scholar] [CrossRef] [PubMed]
- Imai, E.; Yamagata, K.; Iseki, K.; Iso, H.; Horio, M.; Mkino, H.; Hishida, A.; Matsuo, S. Kidney disease screening program in Japan: History, outcome, and perspectives. Clin. J. Am. Soc. Nephrol. 2007, 2, 1360–1366. [Google Scholar] [CrossRef]
- Sinnakirouchenan, R.; Holley, J.L. Peritoneal dialysis versus hemodialysis: Risks, benefits, and access issues. Adv. Chronic Kidney Dis. 2011, 18, 428–432. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Characteristic | Physician Cohort (n = 30,268) | Comparison Cohort (n = 60,536) | p Value | |
|---|---|---|---|---|
| Age (years) | 46.7 (11.3) | 46.7 (11.3) | 0.957 | |
| Age (years) | 0.994 | |||
| Younger (<35) | 4633 (15.3) | 9249 (15.3) | ||
| Middle (35–64) | 23,630 (78.1) | 47,274 (78.1) | ||
| Older (≥65) | 2005 (6.6) | 4013 (6.6) | ||
| Sex | >0.999 | |||
| Male | 26,159 (86.4) | 52,318 (86.4) | ||
| Female | 4109 (13.6) | 8218 (13.6) | ||
| Comorbidity | ||||
| HTN | 8656 (28.6) | 15,367 (25.4) | <0.001 | |
| DM | 5518 (18.2) | 13,389 (22.1) | <0.001 | |
| Hyperlipidemia | 8603 (28.4) | 11,912 (19.7) | <0.001 | |
| Hyperuricemia | 4003 (13.2) | 7404 (12.2) | <0.001 | |
| Anemia | 1382 (4.6) | 3507 (5.8) | <0.001 | |
| CAD | 2990 (9.9) | 6018 (9.9) | 0.775 | |
| Characteristic | Number of ESRD (%) | OR (95% CI) | AOR (95% CI) * | p Value † |
|---|---|---|---|---|
| Overall analysis | ||||
| Physician cohort | 54 (0.2) | 0.4 (0.3–0.6) | 0.5 (0.4–0.7) | <0.001 |
| Comparison cohort | 243 (0.4) | 1.0 | 1.0 | |
| Stratified analysis | ||||
| Age subgroup | ||||
| Younger (<35 years) | ||||
| Physician cohort | 1 (0.02) | 0.199 (0.03–1.6) | 0.2 (0.03–2.0) | 0.180 |
| Comparison cohort | 10 (0.1) | 1.0 | 1.0 | |
| Middle (35–64 years) | ||||
| Physician cohort | 33 (0.1) | 0.3 (0.2–0.5) | 0.4 (0.3–0.7) | <0.001 |
| Comparison cohort | 193 (0.4) | 1.0 | 1.0 | |
| Older (≥65 years) | ||||
| Physician cohort | 20 (1.0) | 1.0 (0.6–1.7) | 1.0 (0.6–1.7) | 0.958 |
| Comparison cohort | 40 (1.0) | 1.0 | 1.0 | |
| Sex | ||||
| Male | ||||
| Physician cohort | 52 (0.2) | 0.5 (0.3–0.6) | 0.6 (0.4–0.8) | <0.001 |
| Comparison cohort | 229 (0.4) | 1.0 | 1.0 | |
| Female | ||||
| Physician cohort | 2 (0.1) | 0.3 (0.1–1.3) | 0.4 (0.1–1.3) | 0.115 |
| Comparison cohort | 14 (0.2) | 1.0 | 1.0 |
| Number of ESRD (%) | OR (95% CI) | AOR (95% CI) * | p Value † | |
|---|---|---|---|---|
| Specialty | ||||
| Internal medicine | 9 (0.2) | 1.5 (0.7–3.3) | 1.3 (0.6–3.0) | 0.512 |
| Surgery | 7 (0.3) | 2.2 (0.9–5.1) | 1.0 (0.4–2.4) | 0.965 |
| Ob/gyn | 7 (0.3) | 2.1 (0.9–4.9) | 1.0 (0.4–2.4) | 0.995 |
| Pediatrics | 4 (0.1) | 0.9 (0.3–2.5) | 0.9 (0.3–2.8) | 0.853 |
| Emergency medicine | 0 (0.0) | – | – | – |
| Family medicine | 6 (0.3) | 1.8 (0.7–4.6) | 0.7 (0.3–1.9) | 0.493 |
| Other specialties | 2 (0.1) | 1 (reference) | 1 (reference) | – |
| Age subgroup (years) | ||||
| Younger (<35) | 1 (0.02) | 0.02 (0.003–0.2) | 1.0 (0.1–8.7) | 0.966 |
| Middle (35–64) | 33 (0.1) | 0.1 (0.1–0.2) | 1.1 (0.6–2.1) | 0.760 |
| Older (≥65) | 21 (1.0) | 1 (reference) | 1 (reference) | – |
| Sex | ||||
| Male | 52 (0.2) | 4.1 (1.0–16.8) | 3.3 (0.8–14.5) | 0.109 |
| Female | 2 (0.1) | 1 (reference) | 1 (reference) | – |
| Treatment | Physician cohort with ESRD (n = 54) | Comparison cohort with ESRD (n = 243) | p Value |
|---|---|---|---|
| Peritoneal dialysis | 34 (63.0%) | 27 (11.1%) | < 0.001 |
| Hemodialysis | 10 (18.5%) | 188 (77.4%) | |
| Renal transplantation | 3 (5.6%) | 4 (1.7%) |
| Age (years) | Physician cohort with ESRD (n = 54) | Comparison cohort with ESRD (n = 243) | p-Value |
|---|---|---|---|
| Age at first diagnosis of ESRD | 61.21 ± 10.54 | 55.95 ± 11.23 | 0.002 |
| Age at first peritoneal dialysis | 61.44 ± 10.37 | 48.72 ± 10.38 | <0.001 |
| Age at first hemodialysis | 59.16 ± 12.08 | 57.26 ± 10.84 | 0.526 |
| Age at renal transplantation | 54.61 ± 3.49 | 40.17 ± 8.60 | 0.037 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yen, C.-K.; Tan, T.-H.; Feng, I.-J.; Ho, C.-H.; Hsu, C.-C.; Lin, H.-J.; Wang, J.-J.; Huang, C.-C. Comparison of Risk for End-Stage Renal Disease Between Physicians and the General Population: A Nationwide Population-Based Cohort Study. Int. J. Environ. Res. Public Health 2019, 16, 2211. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16122211
Yen C-K, Tan T-H, Feng I-J, Ho C-H, Hsu C-C, Lin H-J, Wang J-J, Huang C-C. Comparison of Risk for End-Stage Renal Disease Between Physicians and the General Population: A Nationwide Population-Based Cohort Study. International Journal of Environmental Research and Public Health. 2019; 16(12):2211. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16122211
Chicago/Turabian StyleYen, Chin-Kai, Tian-Hoe Tan, I-Jung Feng, Chung-Han Ho, Chien-Chin Hsu, Hung-Jung Lin, Jhi-Joung Wang, and Chien-Cheng Huang. 2019. "Comparison of Risk for End-Stage Renal Disease Between Physicians and the General Population: A Nationwide Population-Based Cohort Study" International Journal of Environmental Research and Public Health 16, no. 12: 2211. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16122211