Effect of an Oral Health Programme on Oral Health, Oral Intake, and Nutrition in Patients with Stroke and Dysphagia in Taiwan: A Randomised Controlled Trial

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Size Calculation
2.2. Design
2.3. Participants
2.4. Intervention
2.4.1. The Control Group
2.4.2. The Oral Care Group
2.5. Variables Measured/Calculated
2.5.1. Oral Health Assessment Tool (OHAT)
2.5.2. Functional Oral Intake Scale (FOIS)
2.5.3. Mini-Nutritional Assessment-Short Form (MNA-SF)
2.5.4. Rate of Nasogastric Tube Removal
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Two Groups
3.2. Impact of the Experimental Programme on the Outcomes
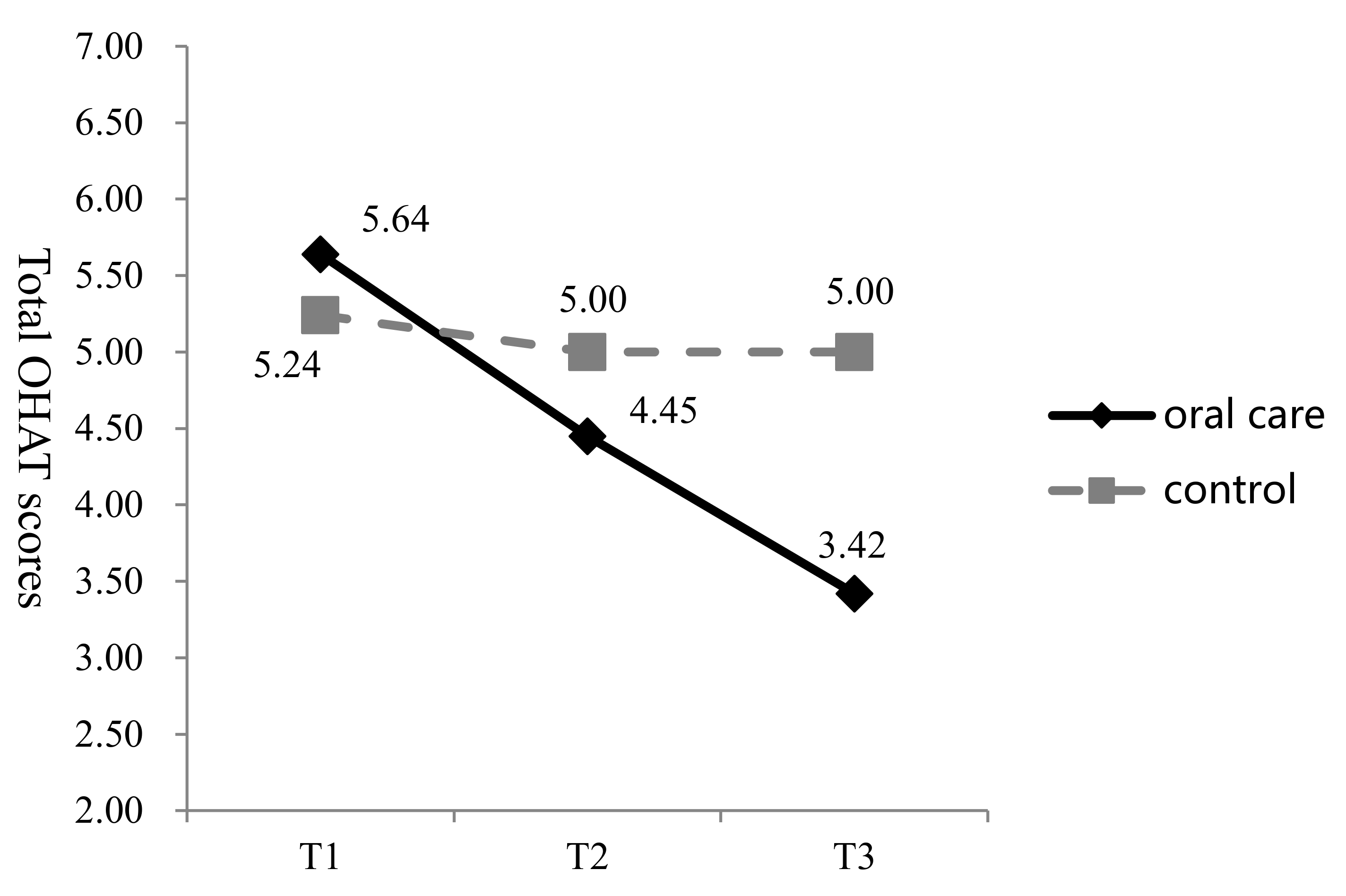
3.2.1. OHAT
3.2.2. FOIS
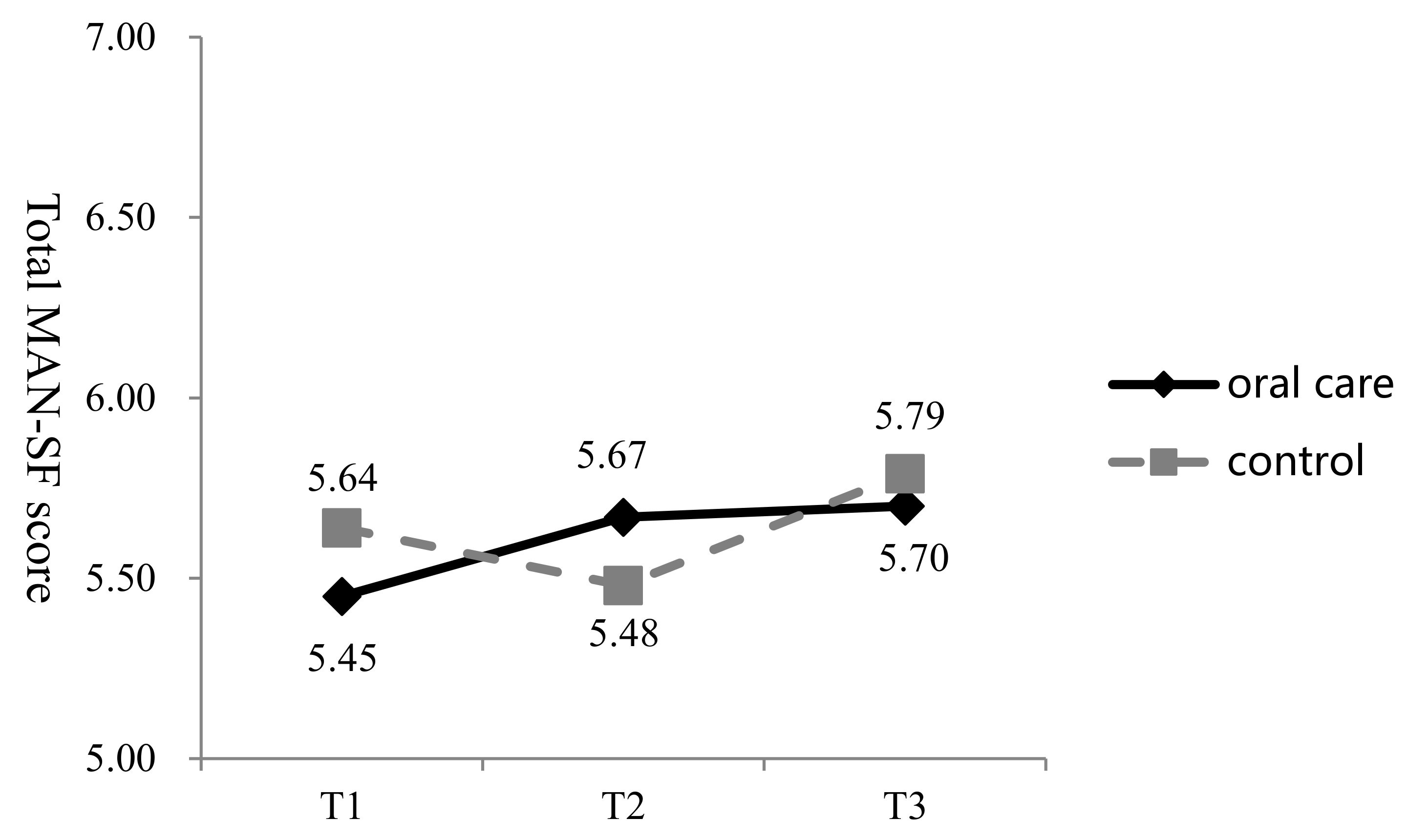
3.2.3. MNA-SF
3.2.4. Nasogastric Tube Removal
4. Discussion
4.1. Limitations
4.2. Future Directions
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Martino, R.; Foley, N.; Bhogal, S.; Diamant, N.; Speechley, M.; Teasell, R. Dysphagia after stroke: Incidence, diagnosis, and pulmonary complications. Stroke 2005, 36, 2756–2763. [Google Scholar] [CrossRef]
- Hu, H.H. Taiwan Guidelines for the Management of Stroke. Available online: http//www.stroke.org.tw/GoWeb2/include/pdf/08%20 (accessed on 15 January 2017).
- Lieber, A.C.; Hong, E.; Putrino, D. Nutrition, energy expenditure, dysphagia, and self-fficacy in stroke rehabilitation: A review of the literature. Brain Sci. 2018, 8, 218. [Google Scholar] [CrossRef] [PubMed]
- Wirth, R.; Smoliner, C.; Jager, M.; Warnecke, T.; Leischker, A.H.; Dziewas, R. Guideline clinical nutrition in patients with stroke. Exp. Transl. Stroke Med. 2013, 5, 14. [Google Scholar] [CrossRef] [PubMed]
- Arnold, M.; Liesirova, K.; Broeg-Morvay, A.; Meisterernst, J.; Schlager, M.; Mono, M.L.; El-Koussy, M.; Kagi, G.; Jung, S.; Sarikaya, H. Dysphagia in acute stroke: Incidence, burden and impact on clinical outcome. PLoS ONE 2016, 11, e0148424. [Google Scholar] [CrossRef] [PubMed]
- Xian, H.X.; Liu, W.C.; Yang, Y.H. Effectively improve the daily life function of stroke patients—Analysis of the effectiveness of acute post-care. Taiwan Geriatr. Gerontol. 2015, 10, 159–171. [Google Scholar]
- Salamone, K.; Yacoub, E.; Mahoney, A.M.; Edward, K.L. Oral care of hospitalised older patients in the acute medical setting. Nurs. Res. Pract. 2013, 2013, 827670. [Google Scholar] [CrossRef]
- Dodds, M.; Roland, S.; Edgar, M.; Thornhill, M. Saliva A review of its role in maintaining oral health and preventing dental disease. BDJ Team 2015, 2, 15123. [Google Scholar] [CrossRef]
- Toniolo, L.; Cancellara, P.; Maccatrozzo, L.; Patruno, M.; Mascarello, F.; Reggiani, C. Masticatory myosin unveiled: First determination of contractile parameters of muscle fibers from carnivore jaw muscles. Am. J. Physiol. Cell Physiol. 2008, 295, 1535–1542. [Google Scholar] [CrossRef]
- Isola, G.; Perillo, L.; Migliorati, M.; Matarese, M.; Dalessandri, D.; Grassia, V.; Alibrandi, A.; Matarese, G. The impact of temporomandibular joint arthritis on functional disability and global health in patients with juvenile idiopathic arthritis. Eur. J. Orthod. 2018, 41, 117–124. [Google Scholar] [CrossRef]
- Severo Alves, L.; Dam-Teixeira, N.; Susin, C.; Maltz, M. Association among quality of life, dental caries treatment and intraoral distribution in 12-year-old South Brazilian schoolchildren. Community Dent. Oral Epidemiol. 2013, 41, 22–29. [Google Scholar] [CrossRef]
- Abanto, J.; Paiva, S.M.; Sheiham, A.; Tsakos, G.; Mendes, F.M.; Cordeschi, T.; Vidigal, E.A.; Bonecker, M. Changes in preschool children’s OHRQoL after treatment of dental caries: Responsiveness of the B-ECOHIS. Int. J. Paediatr. Dent. 2016, 26, 259–265. [Google Scholar] [CrossRef] [PubMed]
- Samnieng, P.; Ueno, M.; Shinada, K.; Zaitsu, T.; Wright, F.A.; Kawaguchi, Y. Association of hyposalivation with oral function, nutrition and oral health in community-dwelling elderly Thai. Community Dent. Health 2012, 29, 117–123. [Google Scholar]
- Lam, O.L.; McMillan, A.S.; Samaranayake, L.P.; Li, L.S.; McGrath, C. Randomized clinical trial of oral health promotion interventions among patients following stroke. Arch. Phys. Med. Rehabi. 2013, 94, 435–443. [Google Scholar] [CrossRef] [PubMed]
- Chipps, E.; Gatens, C.; Genter, L.; Musto, M.; Dubis-Bohn, A.; Gliemmo, M.; Dudley, K.; Holloman, C.; Hoet, A.E.; Landers, T. Pilot study of an oral care protocol on poststroke survivors. Rehabil. Nurs. 2014, 39, 294–304. [Google Scholar] [CrossRef] [PubMed]
- Ohara, Y.; Yoshida, N.; Kono, Y.; Hirano, H.; Yoshida, H.; Mataki, S.; Sugimoto, K. Effectiveness of an oral health educational program on community-dwelling older people with xerostomia. Geriatr. Gerontol. Int. 2015, 15, 481–489. [Google Scholar] [CrossRef] [PubMed]
- Sumi, Y. The significance of oral care in dysphagia patients. Nihon Ronen Igakkai Zasshi 2013, 50, 465–468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ojo, O.; Brooke, J. The use of enteral nutrition in the management of stroke. Nutrients 2016, 8, 827. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.L.; Lin, F.Y.; Hwu, Y.J. The effectiveness of a complex care program on oral hygiene in a population of chronic psychiatric patients. J. Nurs. Healthc. Res. 2014, 10, 286–294. [Google Scholar]
- Kuo, Y.W.; Yen, M.; Fetzer, S.; Lee, J.D.; Chiang, L.C. Effect of family caregiver oral care training on stroke survivor oral and respiratory health in Taiwan: A randomised controlled trial. Community Dent. Health 2015, 32, 137–142. [Google Scholar] [PubMed]
- Makino, T.; Yamasaki, M.; Fujii, N.; Tanaka, N.; Nohara, K.; Doki, Y. Perioperative oral management for esophageal cancer patients. Kyobu Geka Jpn. J. Thorac. Surg. 2016, 69, 35–39. [Google Scholar]
- Barbe, A.G.; Bock, N.; Derman, S.H.; Felsch, M.; Timmermann, L.; Noack, M.J. Self-assessment of oral health, dental health care and oral health-related quality of life among Parkinson’s disease patients. Gerodontology 2017, 34, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Seedat, J.; Penn, C. Implementing oral care to reduce aspiration pneumonia amongst patients with dysphagia in a South African setting. S. Afr. J. Commun. Disord. 2016, 63, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Sorensen, R.T.; Rasmussen, R.S.; Overgaard, K.; Lerche, A.; Johansen, A.M.; Lindhardt, T. Dysphagia screening and intensified oral hygiene reduce pneumonia after stroke. J. Neurosci. Nurs. 2013, 45, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.Y. Drug induced oral reactions in elderly individuals of long-term care facility. J. Long-Term Care 2015, 19, 1–12. [Google Scholar]
- Manabe, T.; Teramoto, S.; Tamiya, N.; Okochi, J.; Hizawa, N. Risk factors for aspiration pneumonia in older adults. PLoS ONE 2015, 10, e0140060. [Google Scholar] [CrossRef]
- Taiwan Dental Association. Oral Care for Special Needs. 2018. Available online: http://www.cda.org.tw/ (accessed on 22 October 2018).
- Polit, F.D.; Beck, T.C. Nursing Research: Principles and Methods; Lippincott, Williams and Wilkins: Philadelphia, PA, USA, 2004; ISBN 986784037214. [Google Scholar]
- Lai-Chu See. Nursing Research: Principles and Methods; Laurel: Taipei, Taiwan, 2002; ISBN 9577301983. [Google Scholar]
- Chang, C.M.; Tsai, C.N. Comprehensive geriatric assessment. J. Formos. Med. Assoc. 2003, 7, 364–374. [Google Scholar]
- Zeng, S.F. Chewing and swallowing disorders of nursing. In Proceedings of the Rehabilitation Training for Chewing and Swallowing Disorders Symposium, Kaohsiung, Taiwan, 3 December 2016. [Google Scholar]
- World Health Organization. World Health Organization Fluorides and Oral Health: Technical Report Series (Document No. WHO/846) Global Report; World Health Organization: Geneva, Switzerland, 1994. [Google Scholar]
- Chalmers, J.; Johnson, V.; Tang, J.H.; Titler, M.G. Evidence-based protocol: Oral hygiene care for functionally dependent and cognitively impaired older adults. J. Gerontol. Nurs. 2004, 30, 5–12. [Google Scholar] [CrossRef]
- Tsai, Y.Y.; Liu, Y.J.; Li, J.L.; Yang, Y.Y.; Chiu, Y.Z. Validation of the Chinese version in oral health assessment tool (OHAT) for clinical non-dentist professionals. Chang Gung Nurs. 2015, 26, 401–409. [Google Scholar]
- Sallum, R.A.; Duarte, A.F.; Cecconello, I. Analytic review of dysphagia scales. Arq. Bras. Cir. Dig. 2012, 25, 279–282. [Google Scholar] [CrossRef]
- Takahata, H.; Tsutsumi, K.; Baba, H.; Nagata, I.; Yonekura, M. Early intervention to promote oral feeding in patients with intracerebral hemorrhage: A retrospective cohort study. BMC Neurol. 2011, 11, 6. [Google Scholar] [CrossRef]
- Hsu, Y.F.; Lin, W.C.; Hu, C.I.; Ko, M.J.; Chang, C.Y.; Wu, H.M.; Chou, W. Recovery of oral intake function in elderly patients with first-ever acute ischemic stroke. Taiwan J. Phys. Med. Rehab. 2015, 43, 33–40. [Google Scholar]
- Chen, H.J.; Hsu, Y.H.; Chou, M.Y.; Tu, M.S. Nutrition assessment and screening for the elderly. Fam. Med. Prim. Med. Care 2014, 29, 65–74. [Google Scholar]
- Kaiser, M.J.; Bauer, J.M.; Ramsch, C.; Uter, W.; Guigoz, Y.; Cederholm, T.; Thomas, D.R.; Anthony, P.; Charlton, K.E.; Maggio, M.; et al. Validation of the Mini Nutritional Assessment short-form (MNA-SF): A practical tool for identification of nutritional status. J. Nutr. Health Aging 2009, 13, 782–788. [Google Scholar] [CrossRef] [PubMed]
- Yasuyuki, I. Oral health care for elderly in 2018. In Proceedings of the Senior Oral Care Taiwan-Japan Dental Symposium, Taipei, Taiwan, 23 December 2018. [Google Scholar]
- Lopez Espuela, F.; Portilla Cuenca, J.C.; Holguin Mohedas, M.; Parraga Sanchez, J.M.; Cordovilla-Guardia, S.; Casado Naranjo, I. Nutritional status and the relationship regarding functional status after stroke. Nutr. Hosp. 2017, 34, 1353–1360. [Google Scholar] [PubMed]
- Flowers, H.L.; AlHarbi, M.A.; Mikulis, D.; Silver, F.L.; Rochon, E.; Streiner, D.; Martino, R. MRI-based neuroanatomical predictors of dysphagia, dysarthria, and aphasia in patients with first acute ischemic stroke. Cereb. Dis. Extra 2017, 7, 21–34. [Google Scholar] [CrossRef] [PubMed]
- Hsiao, H.C.; Chao, H.C.; Wang, J.J. Features of problematic eating behaviors among community-dwelling older adults with dementia: Family caregivers’ experience. Geriatr. Nurs. 2013, 34, 361–365. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Total (n = 66) | Oral Care Group (n = 33) | Control Group (n = 33) | χ2 | p | |||
|---|---|---|---|---|---|---|---|---|
| Frequency (%) | Frequency (%) | Frequency (%) | ||||||
| Sex | 1.67 | 0.196 | ||||||
| Male | 43 | 65.2 | 19 | 57.6 | 24 | 72.7 | ||
| Female | 23 | 34.8 | 14 | 42.4 | 9 | 27.3 | ||
| Age | 0.000 | 1.000 | ||||||
| ≥65 years | 36 | 54.5 | 18 | 54.5 | 18 | 54.5 | ||
| <65 years | 30 | 45.5 | 15 | 45.5 | 15 | 45.5 | ||
| Stroke type | 0.061 | 0.805 | ||||||
| Infarction | 35 | 53.0 | 18 | 54.5 | 17 | 51.5 | ||
| Haemorrhagic | 31 | 47.0 | 15 | 45.5 | 16 | 48.5 | ||
| Unilateral location | 2.63 | 0.295 a | ||||||
| Right | 34 | 51.5 | 20 | 60.6 | 14 | 42.4 | ||
| Left | 28 | 42.4 | 12 | 36.4 | 16 | 48.5 | ||
| Non-unilateral | 4 | 9.1 | 1 | 3.0 | 3 | 9.1 | ||
| Interval of OHP b (months) | 0.5 (0.5–2) | 0.5 (0.5–2) | 0.5 (0.5–2) | −0.373 | 0.709 | |||
| Swallowing severity | 0.000 | 1.000 | ||||||
| Mild | 24 | 36.4 | 12 | 36.4 | 12 | 36.4 | ||
| Moderate | 28 | 42.4 | 14 | 42.4 | 14 | 42.4 | ||
| Severe | 14 | 21.2 | 7 | 21.2 | 7 | 21.2 | ||
| Active denture | 2.16 | 0.142 | ||||||
| No | 51 | 77.3 | 23 | 69.7 | 28 | 84.8 | ||
| Yes | 15 | 22.7 | 10 | 30.3 | 5 | 15.2 | ||
| Actively wearing dentures (n = 15) | 0.68 | 0.560 a | ||||||
| No | 11 | 73.3 | 8 | 80.0 | 3 | 60.0 | ||
| Yes | 4 | 26.7 | 2 | 20.0 | 2 | 40.0 | ||
| Outcome | Group | Pre-Oral Care | t | p | |
|---|---|---|---|---|---|
| Mean (SD) | n | ||||
| OHAT | oral care | 5.64 (2.54) | 33 | 0.732 | 0.467 |
| control | 5.24 (1.77) | 33 | |||
| FOIS | oral care | 3.15 (2.06) | 33 | 0.000 | 1.000 |
| control | 3.15 (1.79) | 33 | |||
| MAN-SF | oral care | 5.45 (2.48) | 33 | −0.326 | 0.745 |
| control | 5.64 (2.03) | 33 | |||
| Variables | Regression Coefficients | Standard Error | 95% CI of B | Wald χ2 | p |
|---|---|---|---|---|---|
| OHAT | 5.24 | 0.30 | 4.65–5.84 | 299.11 | 0.000 |
| Group (OC) † | 0.39 | 0.53 | −0.64–1.43 | 0.55 | 0.457 |
| Time 3 ‡ | −0.24 | 0.25 | −0.73–0.24 | 0.97 | 0.325 |
| Time 2 ‡ | −0.24 | 0.21 | −0.66–0.18 | 1.28 | 0.258 |
| Interaction | |||||
| Group (OC) × Time 3 § | −1.97 | 0.36 | −2.69-(−1.25) | 29.02 | 0.000 |
| Group (OC) × Time 2 § | −0.94 | 0.30 | −1.54-(−0.34) | 9.52 | 0.002 |
| FOIS | 2.74 | 0.27 | 2.21–3.27 | 101.92 | 0.000 |
| Group (OC)† | −0.27 | 0.43 | −1.11–0.56 | 0. 41 | 0.523 |
| Time 3‡ | 0.17 | 0.16 | −0.14–0.49 | 1.22 | 0.270 |
| Time 2‡ | −0.05 | 0.10 | 0.10–0.15 | 0.24 | 0.625 |
| Interaction | |||||
| Group (OC) × Time 3 § | 0.37 | 0.27 | −0.16–0.89 | 1.86 | 0.172 |
| Group (OC) × Time 2 § | 0.35 | 0.19 | −0.02–0.71 | 3.36 | 0.067 |
| MNA-SF | 5.64 | 0.35 | 4.96–6.32 | 262.82 | 0.000 |
| Group (OC)† | −0.18 | 0.55 | −1.26–0.89 | 0.11 | 0.740 |
| Time 3‡ | 0.15 | 0.18 | −0.20–0.50 | 0.73 | 0.393 |
| Time 2‡ | −0.15 | 0.16 | −0.46–0.15 | 0.95 | 0.329 |
| Interaction | |||||
| Group (OC) × Time 3 § | 0.09 | 0.22 | −0.35–0.53 | 0.17 | 0.684 |
| Group (OC) × Time 2 § | 0.36 | 0.20 | −0.03–0.76 | 3.29 | 0.070 |
| Variable | Control (n = 33) n | % | Oral Care (n = 33) n | % | χ2 | p |
|---|---|---|---|---|---|---|
| NG removal (T2) | 2 | 6.1 | 6 | 18.2 | 2.28 | 0.131 |
| NG removal (T3) | 2 | 6.1 | 7 | 21.2 | 3.22 | 0.073 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, H.-J.; Chen, J.-L.; Chen, C.-Y.; Lee, M.; Chang, W.-H.; Huang, T.-T. Effect of an Oral Health Programme on Oral Health, Oral Intake, and Nutrition in Patients with Stroke and Dysphagia in Taiwan: A Randomised Controlled Trial. Int. J. Environ. Res. Public Health 2019, 16, 2228. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16122228
Chen H-J, Chen J-L, Chen C-Y, Lee M, Chang W-H, Huang T-T. Effect of an Oral Health Programme on Oral Health, Oral Intake, and Nutrition in Patients with Stroke and Dysphagia in Taiwan: A Randomised Controlled Trial. International Journal of Environmental Research and Public Health. 2019; 16(12):2228. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16122228
Chicago/Turabian StyleChen, Hsiao-Jung, Jean-Lon Chen, Chung-Yao Chen, Megan Lee, Wei-Han Chang, and Tzu-Ting Huang. 2019. "Effect of an Oral Health Programme on Oral Health, Oral Intake, and Nutrition in Patients with Stroke and Dysphagia in Taiwan: A Randomised Controlled Trial" International Journal of Environmental Research and Public Health 16, no. 12: 2228. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16122228