The Distribution of Available Prevention and Management Interventions for Fetal Alcohol Spectrum Disorder (2007 to 2017): Implications for Collaborative Actions



Abstract
:1. Introduction
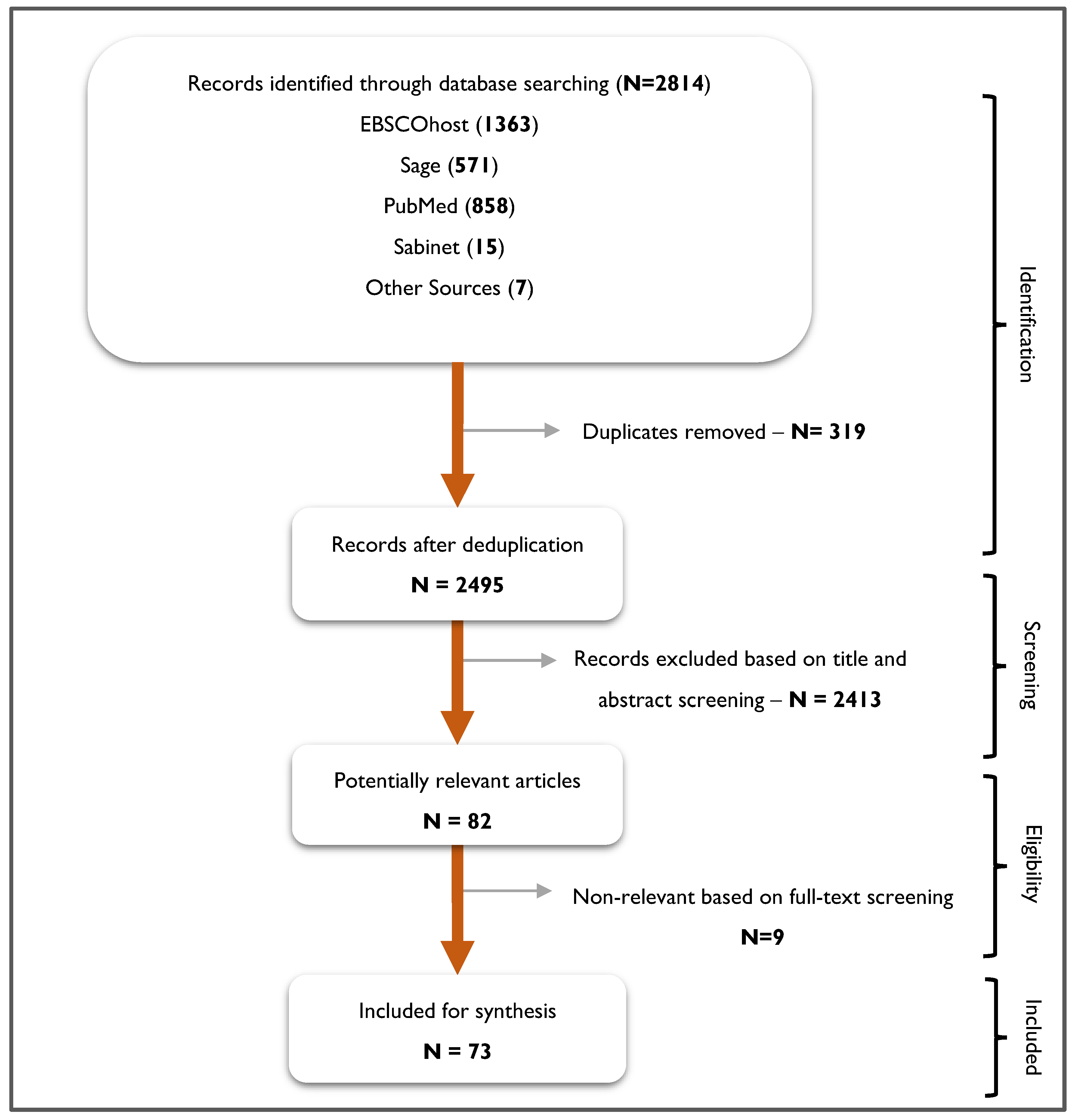
2. Materials and Methods
- The interventions (both pharmacological and non-pharmacological) must aim at preventing or improving the outcome of prenatal exposure to alcohol;
- Articles published in the English Language;
- Articles published from 2007 to 2017 (we chose this period to provide current information to help inform policy development);
- The target population must be women, young people, and individuals with FASD;
- All the types (randomized controlled trials (RCT), quasi RCT, non-randomized controlled trials and cohort studies with pre- and post-intervention);
- Interventions targeting any age group.
- Studies that do not report on the effectiveness or promising outcome of the interventions;
- Animal studies;
- Other systematic, scoping and literature reviews;
- Unpublished prevention and management interventions;
- Articles published before 2007 and after 2017.
3. Results
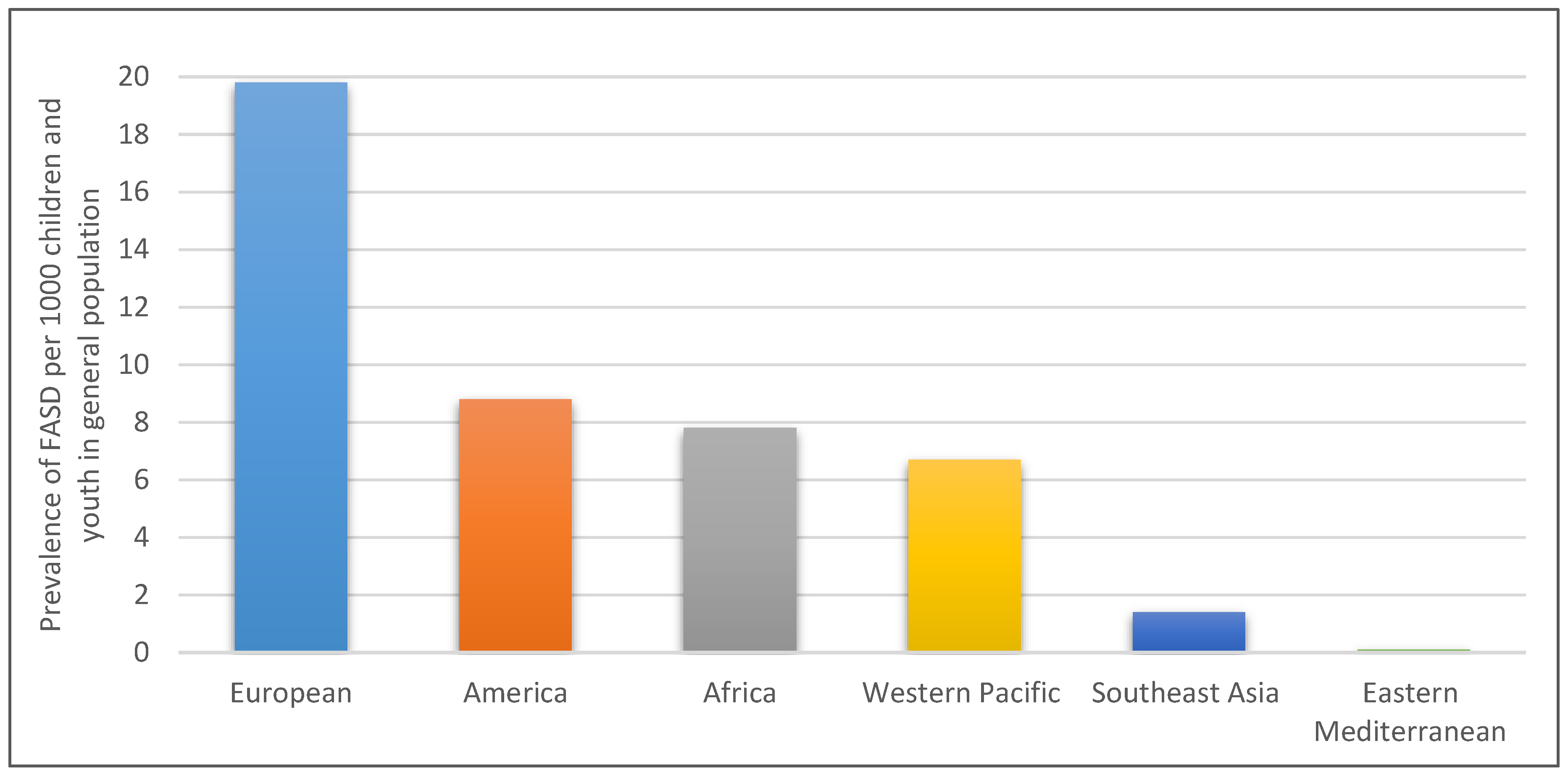
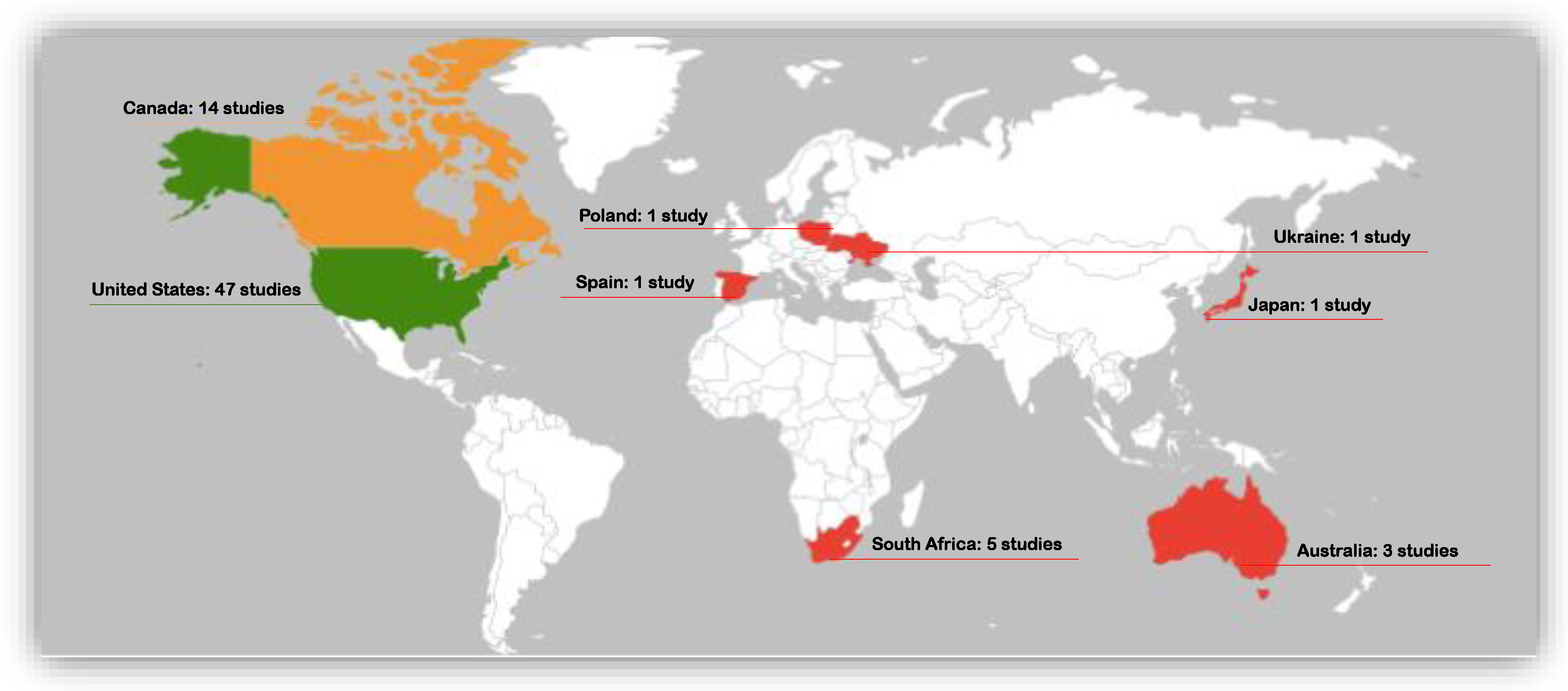
3.1. Global Distribution of FASD Prevention and Management Interventions
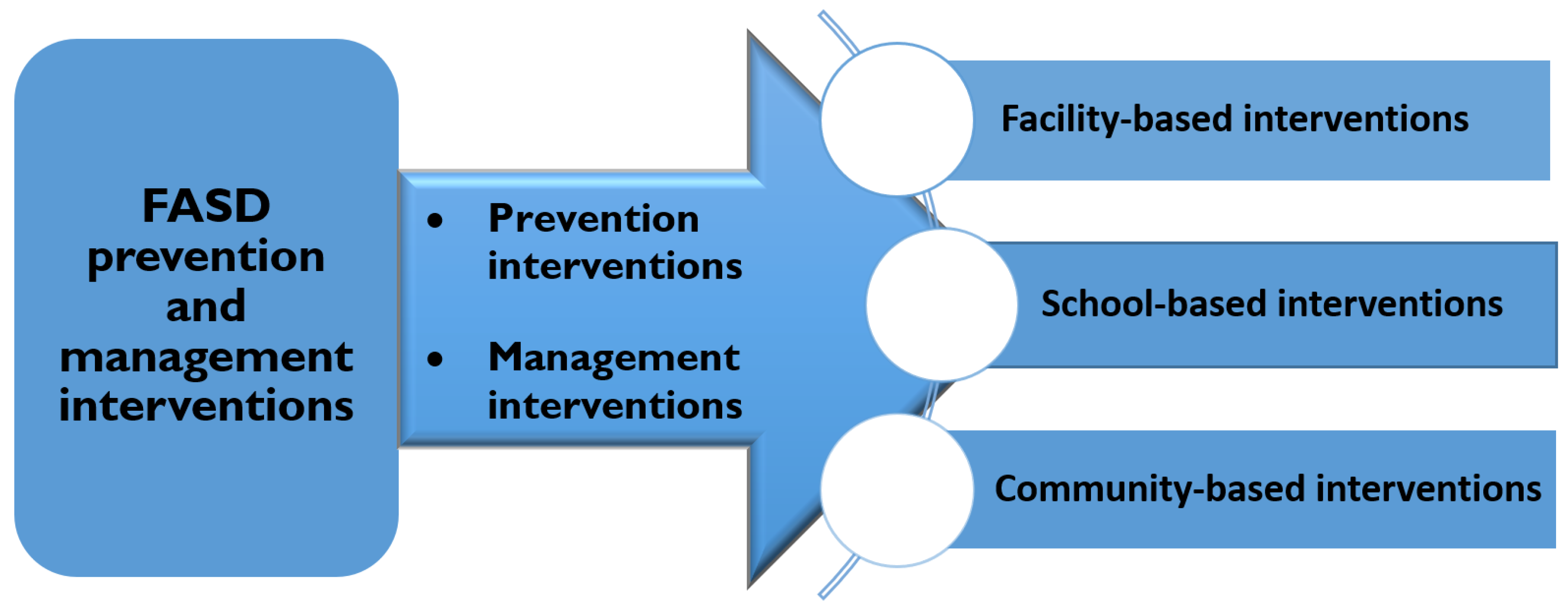
3.2. Prevention Interventions
3.2.1. Facility-Based Prevention Interventions
3.2.2. School-Based/Education-Based Prevention Interventions
3.2.3. Community-Based Prevention Interventions
3.3. Management Interventions
3.4. Facility-Based Management Interventions
3.5. School-Based/Education-Based Management Interventions
3.6. Community-Based Management Interventions
4. Discussion
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Cook, J.L.; Green, C.R.; Lilley, C.M.; Anderson, S.M.; Baldwin, M.E.; Chudley, A.E.; Conry, J.L.; LeBlanc, N.; Loock, C.A.; Lutke, J.; et al. Fetal alcohol spectrum disorder: A guideline for diagnosis across the lifespan. CMAJ 2016, 188, 191–197. [Google Scholar] [CrossRef]
- Chudley, A.E.; Conry, J.; Cook, J.L.; Loock, C.; Rosales, T.; LeBlanc, N. Fetal alcohol spectrum disorder: Canadian guidelines for diagnosis. CAMJ 2005, 172, S1–S21. [Google Scholar] [CrossRef] [Green Version]
- Chudley, A.E. Fetal Alcohol Spectrum Disorder—high rates, high needs, high time for action. JAMA Pediatrics 2017, 171, 940–941. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC). Basics about FASDs | FASD | NCBDDD | CDC. 2018. Available online: https://www.cdc.gov/ncbddd/fasd/facts.html (accessed on 16 July 2018).
- Streissguth, A.P.; Barr, H.M.; Kogan, J.; Bookstein, F.L. Understanding the occurrence of secondary disabilities in clients with Fetal Alcohol Syndrome (FAS) and Fetal Alcohol Effects (FAE); Centers for Disease Control and Prevention: Atlanta, GA, USA, 1996.
- Lange, S.; Probst, C.; Gmel, G.; Rehm, J.; Burd, L.; Popova, S. Global Prevalence of Fetal Alcohol Spectrum Disorder Among Children and Youth. JAMA Pediatr. 2017, 171, 948–956. [Google Scholar] [CrossRef]
- World Health Organization. Management of Substance Abuse Team. In Guidelines for the identification and management of substance use and substance use disorders in pregnancy; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Centers for Disease Control and Prevention (CDC). Fetal Alcohol Spectrum Disorders (FASDs) | NCBDDD | CDC. 2018. Available online: https://www.cdc.gov/ncbddd/fasd/index.html (accessed on 7 May 2018).
- Chersich, M.F.; Urban, M.; Olivier, L.; Davies, L.A.; Chetty, C.; Viljoen, D. Universal prevention is associated with lower prevalence of fetal alcohol spectrum disorders in Northern Cape, South Africa: A multicentre before-after study. Alcohol 2012, 47, 67–74. [Google Scholar] [CrossRef]
- O’Connor, M.J.; Whaley, S.E. Brief intervention for alcohol use by pregnant women. Am. J. Public Health 2007, 97, 252–258. [Google Scholar] [CrossRef]
- Hanson, J.D.; Miller, A.L.; Winberg, A.; Elliott, A.J. Prevention of Alcohol-Exposed Pregnancies among nonpregnant American Indian women. Am. J. Health Promot. 2013, 27, S66–S73. [Google Scholar] [CrossRef]
- De Vries, M.; Joubert, B.; Cloete, M.; Roux, S.; Baca, B.; Hasken, J.; Barnard, R.; Buckley, D.; Kalberg, W.; Snell, C.; et al. Indicated prevention of Fetal Alcohol Spectrum Disorders in South Africa: Effectiveness of case management. Int. J. Environ. Res. Public Health 2015, 13, 76. [Google Scholar] [CrossRef]
- Mwansa-Kambafwile, J.; Rendall-Mkosi, K.; Jacobs, R.; Nel, E.; London, L. Evaluation of a service provider short course for prevention of fetal alcohol syndrome. J. Stud. Alcohol Drugs 2011, 72, 530–535. [Google Scholar] [CrossRef]
- Stade, B.C.; Bailey, C.; Dzendoletas, D.; Sgro, M.; Dowswell, T.; Bennett, D. Psychological and/or educational interventions for reducing alcohol consumption in pregnant women and women planning pregnancy. Cochrane Database of Systematic Reviews 2009, 2. [Google Scholar] [CrossRef]
- Gilinsky, A.; Swanson, V.; Power, K. Interventions delivered during antenatal care to reduce alcohol consumption during pregnancy: A systematic review. Addict. Res. Theory 2011, 19, 235–250. [Google Scholar] [CrossRef]
- Poole, N.; Schmidt, R.A.; Green, C.; Hemsing, N. Prevention of fetal alcohol spectrum disorder: Current Canadian efforts and analysis of gaps. Subst. Abuse 2016, 10, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Pei, J.; Baugh, L.; Andrew, G.; Rasmussen, C. Intervention recommendations and subsequent access to services following clinical assessment for fetal alcohol spectrum disorders. Res. Dev. Disabil. 2017, 60, 176–186. [Google Scholar] [CrossRef] [PubMed]
- Jirikowic, T.; Gelo, J.; Astley, S. Children and youth with fetal alcohol spectrum disorders: Summary of intervention recommendations after clinical diagnosis. Intellect. Dev. Disabil. 2010, 48, 330–344. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, J.P.; Latimer, J.; Olson, H.C.; Carter, M.; Oscar, J.; Lucas, B.R.; Doney, R.; Salter, C.; Try, J.; Hawkes, G. Prevalence and profile of neurodevelopment and fetal alcohol spectrum disorder (FASD) amongst Australian Aboriginal children living in remote communities. Res. Dev. Disabil. 2017, 65, 114–126. [Google Scholar] [CrossRef]
- Kodituwakku, P.W.; Kodituwakku, E.L. From research to practice: An integrative framework for the development of interventions for children with Fetal Alcohol Spectrum Disorders. Neuropsychol. Rev. 2011, 21, 204–223. [Google Scholar] [CrossRef] [PubMed]
- Olson, H.C.; Montague, R.A. An innovative look at early intervention for children affected by prenatal Alcohol Exposure. In Prenatal Alcohol Use and FASD: Diagnosis, assessment and new directions in research and multimodal treatment; Bentham Science Publishers: Sharjah, UAE, 2011; Chapter 4; pp. 64–107. [Google Scholar]
- Reid, N.; Dawe, S.; Shelton, D.; Harnett, P.; Warner, J.; Armstrong, E.; LeGros, K.; O’Callaghan, F. Systematic review of fetal alcohol spectrum disorder interventions across the life span. Alcohol Clin. Exp. Res. 2015, 39, 2283–2295. [Google Scholar] [CrossRef]
- Peadon, E.; Rhys-Jones, B.; Bower, C.; Elliott, E.J. Systematic review of interventions for children with Fetal Alcohol Spectrum Disorders. BMC Pediatr. 2009, 9, 35–43. [Google Scholar] [CrossRef]
- Streissguth, A.P.; Bookstein, F.L.; Barr, H.M.; Sampson, P.D.; O’Malley, K.I.E.R.A.N.; Young, J.K. Risk factors for adverse life outcomes in fetal alcohol syndrome and fetal alcohol effects. J. Dev. Behav. Pediatr. 2004, 25, 228–238. [Google Scholar] [CrossRef]
- Paley, B.; O’Connor, M.J. Behavioral interventions for children and adolescents with fetal alcohol spectrum disorders. Alcohol Res. Health 2011, 34, 64–75. [Google Scholar]
- Petrenko, C.L.M. Positive Behavioral Interventions and Family Support for Fetal Alcohol Spectrum Disorders. Curr. Dev. Disord. Reports 2015, 2, 199–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrenko, C.L.M.; Alto, M.E. Interventions in fetal alcohol spectrum disorders: An international perspective. Eur. J. Med. Genet. 2017, 60, 79–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chandrasena, A.N.; Mukherjee, R.A.S.; Turk, J. Fetal Alcohol Spectrum Disorders: An Overview of Interventions for Affected Individuals. Child. Adolesc. Ment. Health 2009, 14, 162–167. [Google Scholar] [CrossRef]
- Bertrand, J. Interventions for children with fetal alcohol spectrum disorders (FASDs): Overview of findings for five innovative research projects. Res. Dev. Disabil. 2009, 30, 986–1006. [Google Scholar] [CrossRef] [PubMed]
- Symons, M.; Pedruzzi, R.A.; Bruce, K.; Milne, E. A systematic review of prevention interventions to reduce prenatal alcohol exposure and fetal alcohol spectrum disorder in indigenous communities. BMC Public Health 2018, 18, 1227. [Google Scholar] [CrossRef] [PubMed]
- Premji, S.; Benzies, K.; Serrett, K.; Hayden, K.A. Research-based interventions for children and youth with a fetal alcohol spectrum disorder: Revealing the gap. Child. Care Health Dev. 2007, 33, 389–397. [Google Scholar] [CrossRef]
- Adebiyi, B.O.; Mukumbang, F.C.; Cloete, L.G.; Beytell, A.M. Exploring service providers’ perspectives on the prevention and management of fetal alcohol spectrum disorders in South Africa: A qualitative study. BMC Public Health 2018, 18, 1238. [Google Scholar] [CrossRef]
- Adebiyi, B.O.; Mukumbang, F.C.; Cloete, L.G.; Beytell, A.M. Policymakers’ Perspectives Towards Developing a Guideline to Inform Policy on Fetal Alcohol Spectrum Disorder: A Qualitative Study. Int. J. Environ. Res. Public Health 2019, 16, 945. [Google Scholar] [CrossRef]
- Adebiyi, B.O.; Mukumbang, F.C.; Okop, K.J.; Beytell, A.M. A modified Delphi study towards developing a guideline to inform policy on fetal alcohol spectrum disorders in South Africa: A study protocol. BMJ Open 2018, 8, e019907. [Google Scholar] [CrossRef]
- Adebiyi, B.O.; Mukumbang, F.C.; Beytell, A.-M. To what extent is Fetal Alcohol Spectrum Disorder considered in policy-related documents in South Africa? A document review. Health Res. Policy Syst. 2019, 17, 46. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med. Inform. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef] [PubMed]
- Thomas, B.H.; Ciliska, D.; Dobbins, M.; Micucci, S. A process for systematically reviewing the literature: Providing the research evidence for public health nursing interventions. Worldviews Evidence-Based Nurs. 2004, 1, 176–184. [Google Scholar] [CrossRef] [PubMed]
- Jüni, P.; Witschi, A.; Bloch, R.; Egger, M. The hazards of scoring the quality of clinical trials for meta-analysis. JAMA 1999, 282, 1054–1060. [Google Scholar] [CrossRef] [PubMed]
- Rodgers, M.; Sowden, A.; Petticrew, M.; Arai, L.; Roberts, H.; Britten, N.; Popay, J. Testing Methodological Guidance on the Conduct of Narrative Synthesis in Systematic Reviews. Evaluation 2009, 15, 49–73. [Google Scholar] [CrossRef]
- Snilstveit, B.; Oliver, S.; Vojtkova, M. Narrative approaches to systematic review and synthesis of evidence for international development policy and practice. J. Dev. Eff. 2012, 4, 409–429. [Google Scholar] [CrossRef]
- Gale, N.K.; Heath, G.; Cameron, E.; Rashid, S.; Redwood, S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med. Res. Methodol. 2013, 13, 117. [Google Scholar] [CrossRef] [PubMed]
- Joya, X.; Mazarico, E.; Ramis, J.; Pacifici, R.; Salat-Batlle, J.; Mortali, C.; García-Algar, O.; Pichini, S. Segmental hair analysis to assess effectiveness of single-session motivational intervention to stop ethanol use during pregnancy. Drug Alcohol Depend. 2016, 158, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Velasquez, M.M.; von Sternberg, K.; Parrish, D.E. CHOICES: An integrated behavioral intervention to prevent alcohol-exposed pregnancies among high-risk women in community settings. Soc. Work Public Health 2013, 28, 224–233. [Google Scholar] [CrossRef]
- Payne, J.; France, K.; Henley, N.; D’antoine, H.; Bartu, A.; O’leary, C.; Elliott, E.; Bower, C. Changes in health professionals’ knowledge, attitudes and practice following provision of educational resources about prevention of Prenatal Alcohol Exposure and Fetal Alcohol Spectrum Disorder. Paediatr. Perinat. Epidemiol. 2011, 25, 316–327. [Google Scholar] [CrossRef]
- Ondersma, S.J.; Beatty, J.R.; Svikis, D.S.; Strickler, R.C.; Tzilos, G.K.; Chang, G.; Divine, G.W.; Taylor, A.R.; Sokol, R.J. Computer-Delivered Screening and Brief Intervention for Alcohol Use in Pregnancy: A Pilot Randomized Trial. Alcohol Clin. Exp. Res. 2015, 39, 1219–1226. [Google Scholar] [CrossRef] [PubMed]
- Delrahim-Howlett, K.; Chambers, C.D.; Clapp, J.D.; Xu, R.; Duke, K.; Moyer III, R.J.; Van Sickle, D. Web-Based Assessment and Brief Intervention for Alcohol Use in Women of Childbearing Potential: A Report of the Primary Findings. Alcohol Clin. Exp. Res. 2011, 35, 1331–1338. [Google Scholar] [CrossRef] [PubMed]
- Tzilos, G.K.; Sokol, R.J.; Ondersma, S.J. A randomized phase I trial of a brief computer-delivered intervention for alcohol use during pregnancy. J. Womens Health (Larchmt) 2011, 20, 1517–1524. [Google Scholar] [CrossRef] [PubMed]
- Hutton, H.E.; Chander, G.; Green, P.P.; Hutsell, C.A.; Weingarten, K.; Peterson, K.L. A novel integration effort to reduce the risk for alcohol-exposed pregnancy among women attending urban STD clinics. Public Health Rep. 2014, 129 (Suppl 1), 56–62. [Google Scholar] [CrossRef]
- Osterman, R. Feasibility of Using Motivational Interviewing to Decrease Alcohol Consumption During Pregnancy. J. Addict. Nurs. 2011, 22, 93–102. [Google Scholar] [CrossRef]
- Osterman, R.L.; Dyehouse, J. Effects of a Motivational Interviewing Intervention to Decrease Prenatal Alcohol Use. West. J. Nurs. Res. 2012, 34, 434–454. [Google Scholar] [CrossRef] [PubMed]
- LaChausse, R.G. The effectiveness of a multimedia program to prevent Fetal Alcohol Syndrome. Health Promot. Pract. 2008, 9, 289–293. [Google Scholar] [CrossRef]
- Boulter, L. The effectiveness of peer-led FAS/FAE prevention presentations in middle and high schools. J. Alcohol Drug Educ. 2007, 51, 7–26. [Google Scholar]
- Toyama, N.; Sudo, N. Educational effects of a tailored leaflet addressing drinking during pregnancy. Clin. Med. Insights Reprod. Health 2014, 8, 5–14. [Google Scholar] [CrossRef]
- Hanson, J.D.; Nelson, M.E.; Jensen, J.L.; Willman, A.; Jacobs-Knight, J.; Ingersoll, K. Impact of the choices intervention in preventing Alcohol-Exposed Pregnancies in American Indian women. Alcohol Clin. Exp. Res. 2017, 41, 828–835. [Google Scholar] [CrossRef]
- Farrell-Carnahan, L.; Hettema, J.; Jackson, J.; Kamalanathan, S.; Ritterband, L.M.; Ingersoll, K.S. Feasibility and promise of a remote-delivered preconception motivational interviewing intervention to reduce risk for Alcohol-Exposed Pregnancy. Telemed e-Health 2013, 19, 597–604. [Google Scholar] [CrossRef] [PubMed]
- Letourneau, B.; Sobell, L.C.; Sobell, M.B.; Johnson, K.; Heinecke, N.; Robinson, S.M. Preventing Alcohol-Exposed Pregnancies among Hispanic women. J. Ethn. Subst. Abuse 2017, 16, 109–121. [Google Scholar] [CrossRef] [PubMed]
- Tenkku, L.E.; Mengel, M.B.; Nicholson, R.A.; Hile, M.G.; Morris, D.S.; Salas, J. A web-based intervention to reduce Alcohol-Exposed Pregnancies in the community. Health Educ. Behav. 2011, 38, 563–573. [Google Scholar] [CrossRef] [PubMed]
- Montag, A.C.; Brodine, S.K.; Alcaraz, J.E.; Clapp, J.D.; Allison, M.A.; Calac, D.J.; Hull, A.D.; Gorman, J.R.; Jones, K.L.; Chambers, C.D. Preventing Alcohol-Exposed Pregnancy among an American Indian/Alaska native population: Effect of a screening, brief intervention, and referral to treatment intervention. Alcohol Clin. Exp. Res. 2015, 39, 126–135. [Google Scholar] [CrossRef] [PubMed]
- May, P.A.; Marais, A.S.; Gossage, J.P.; Barnard, R.; Joubert, B.; Cloete, M.; Hendricks, N.; Roux, S.; Blom, A.; Steenekamp, J.; et al. Case management reduces drinking during pregnancy among high risk women. Int. J. Alcohol Drug Res. 2013, 2, 61–70. [Google Scholar] [CrossRef] [PubMed]
- France, K.E.; Donovan, R.J.; Bower, C.; Elliott, E.J.; Payne, J.M.; D’Antoine, H.; Bartu, A.E. Messages that increase women’s intentions to abstain from alcohol during pregnancy: Results from quantitative testing of advertising concepts. BMC Public Health 2014, 14, 30. [Google Scholar] [CrossRef]
- Wilton, G.; Moberg, D.P.; Van Stelle, K.R.; Dold, L.L.; Obmascher, K.; Goodrich, J. A randomized trial comparing telephone versus in-person brief intervention to reduce the risk of an Alcohol-Exposed Pregnancy. J. Subst. Abuse Treat. 2013, 45, 389–394. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, C.; Kully-Martens, K.; Denys, K.; Badry, D.; Henneveld, D.; Wyper, K.; Grant, T. The effectiveness of a community-based intervention program for women at-risk for giving birth to a child with Fetal Alcohol Spectrum Disorder (FASD). Community Ment. Health J. 2012, 48, 12–21. [Google Scholar] [CrossRef]
- Floyd, R.L.; Sobell, M.; Velasquez, M.M.; Ingersoll, K.; Nettleman, M.; Sobell, L.; Mullen, P.D.; Ceperich, S.; von Sternberg, K.; Bolton, B. Preventing alcohol-exposed pregnancies: A randomized controlled trial. Am. J. Prev. Med. 2007, 32, 360. [Google Scholar] [CrossRef] [PubMed]
- Dresser, J.; Starling, R.; Woodall, W.G.; Stanghetta, P.; May, P.A. Field trial of alcohol-server training for prevention of Fetal Alcohol Syndrome. J. Stud. Alcohol Drugs 2011, 72, 490–496. [Google Scholar] [CrossRef] [PubMed]
- Hanson, J.D.; Winberg, A.; Elliott, A. Development of a Media Campaign on Fetal Alcohol Spectrum Disorders for Northern Plains American Indian Communities. Health Promot. Pract. 2012, 13, 842–847. [Google Scholar] [CrossRef] [PubMed]
- May, P.A.; Miller, J.H.; Goodhart, K.A.; Maestas, O.R.; Buckley, D.; Trujillo, P.M.; Gossage, J.P. Enhanced Case Management to Prevent Fetal Alcohol Spectrum Disorders in Northern Plains Communities. Matern. Child. Health J. 2008, 12, 747–759. [Google Scholar] [CrossRef] [PubMed]
- Ingersoll, K.S.; Ceperich, S.D.; Hettema, J.E.; Farrell-Carnahan, L.; Penberthy, J.K. Preconceptional motivational interviewing interventions to reduce alcohol-exposed pregnancy risk. J. Subst Abuse Treat. 2013, 44, 407–416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russell, T.T.; Craddock, C.S.; Kodatt, S.A.; Ramirez, D.M. Preventing Fetal Alcohol Spectrum Disorders: An Evidence-Based Prevention Program for Adolescent and Adult Hispanic Females in the South Texas Border Region. Online Submission 2017. [Google Scholar]
- Nguyen, T.T.; Risbud, R.D.; Mattson, S.N.; Chambers, C.D.; Thomas, J.D. Randomized, double-blind, placebo-controlled clinical trial of choline supplementation in school-aged children with fetal alcohol spectrum disorders. Am. J. Clin. Nutr. 2016, 104, 1683–1692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zarnegar, Z.; Hambrick, E.P.; Perry, B.D.; Azen, S.P.; Peterson, C. Clinical improvements in adopted children with Fetal Alcohol Spectrum Disorders through neurodevelopmentally informed clinical intervention: A pilot study. Clin. Child. Psychol. Psychiatry 2016, 21, 551–567. [Google Scholar] [CrossRef] [PubMed]
- Wozniak, J.R.; Fuglestad, A.J.; Eckerle, J.K.; Fink, B.A.; Hoecker, H.L.; Boys, C.J.; Radke, J.P.; Kroupina, M.G.; Miller, N.C.; Brearley, A.M. Choline supplementation in children with Fetal Alcohol Spectrum Disorders: A randomized, double-blind, placebo-controlled trial. Am. J. Clin. Nutr. 2015, 102, 1113–1125. [Google Scholar] [CrossRef]
- Wozniak, J.R.; Fuglestad, A.J.; Eckerle, J.K.; Kroupina, M.G.; Miller, N.C.; Boys, C.J.; Brearley, A.M.; Fink, B.A.; Hoecker, H.L.; Zeisel, S.H. Choline supplementation in children with fetal alcohol spectrum disorders has high feasibility and tolerability. Nutr. Res. 2013, 33, 897–904. [Google Scholar] [CrossRef] [Green Version]
- Wilczyński, J.; Zawada, K. The impact of sensory integration therapy on gross motor function in children after prenatal exposure to alcohol. Med. Stud. 2015, 1, 10–17. [Google Scholar] [CrossRef]
- Yazdani, P.; Motz, M.; Koren, G. Estimating the neurocognitive effects of an early intervention program for children with Prenatal Alcohol Exposure. Can. J. Clin. Pharmacol. 2009, 16, 453–459. [Google Scholar]
- Kable, J.A.; Coles, C.D.; Keen, C.L.; Uriu-Adams, J.Y.; Jones, K.L.; Yevtushok, L.; Kulikovsky, Y.; Wertelecki, W.; Pedersen, T.L.; Chambers, C.D. The impact of micronutrient supplementation in Alcohol-Exposed Pregnancies on information processing skills in Ukrainian infants. Alcohol 2015, 49, 647–656. [Google Scholar] [CrossRef] [PubMed]
- Connolly, S.C.; Millians, M.; Peterman, R.; Shillingsburg, M.A. The clinical application of applied behavior analysis in a child with partial fetal alcohol syndrome: A case study. Clin. Case Stud. 2016, 15, 225–242. [Google Scholar] [CrossRef]
- Nash, K.; Stevens, S.; Greenbaum, R.; Weiner, J.; Koren, G.; Rovet, J. Improving executive functioning in children with Fetal Alcohol Spectrum Disorders. Child. Neuropsychol. 2015, 21, 191–209. [Google Scholar] [CrossRef] [PubMed]
- Soh, D.W.; Skocic, J.; Nash, K.; Stevens, S.; Turner, G.R.; Rovet, J. Self-regulation therapy increases frontal gray matter in children with fetal alcohol spectrum disorder: Evaluation by voxel-based morphometry. Front. Hum. Neurosci. 2015, 9, 108. [Google Scholar] [CrossRef] [PubMed]
- Keiver, K.; Bertram, C.P.; Orr, A.P.; Clarren, S. Salivary cortisol levels are elevated in the afternoon and at bedtime in children with prenatal alcohol exposure. Alcohol 2015, 49, 79–87. [Google Scholar] [CrossRef] [PubMed]
- Nash, K.; Stevens, S.; Clairman, H.; Rovet, J. Preliminary Findings that a Targeted Intervention Leads to Altered Brain Function in Children with Fetal Alcohol Spectrum Disorder. Brain Sci. 2017, 8, 7. [Google Scholar] [CrossRef]
- Doig, J.; McLennan, J.D.; Gibbard, W.B. Medication Effects on Symptoms of Attention-Deficit/Hyperactivity Disorder in Children with Fetal Alcohol Spectrum Disorder. J. Child. Adolesc. Psychopharmacol. 2008, 18, 365–371. [Google Scholar] [CrossRef] [PubMed]
- Coles, C.D.; Kable, J.A.; Taddeo, E. Math performance and behavior problems in children affected by prenatal alcohol exposure: Intervention and follow-up. J. Dev. Behav. Pediatr. 2009, 30, 7–15. [Google Scholar] [CrossRef]
- Kerns, K.A.; MacSween, J.; Vander Wekken, S.; Gruppuso, V. Investigating the efficacy of an attention training program in children with foetal alcohol spectrum disorder. Dev. Neurorehabil. 2010, 13, 413–422. [Google Scholar] [CrossRef]
- Jirikowic, T.; McCoy, S.W.; Price, R.; Ciol, M.A.; Hsu, L.Y.; Kartin, D. Virtual sensorimotor training for balance. Pediatr. Phys. Ther. 2016, 28, 460–468. [Google Scholar] [CrossRef]
- Adnams, C.M.; Sorour, P.; Kalberg, W.O.; Kodituwakku, P.; Perold, M.D.; Kotze, A.; September, S.; Castle, B.; Gossage, J.; May, P.A. Language and literacy outcomes from a pilot intervention study for children with Fetal Alcohol Spectrum Disorders in South Africa. Alcohol 2007, 41, 403–414. [Google Scholar] [CrossRef] [PubMed]
- Kable, J.A.; Coles, C.D.; Taddeo, E. Socio-cognitive habilitation using the Math interactive learning experience program for alcohol-affected children. Alcohol Clin. Exp. Res. 2007, 31, 1425–1434. [Google Scholar] [CrossRef] [PubMed]
- Kable, J.A.; Taddeo, E.; Strickland, D.; Coles, C.D. Improving FASD children’s self-regulation: Piloting phase 1 of the GoFAR intervention. Child. Fam. Behav. Ther. 2016, 38, 124–141. [Google Scholar] [CrossRef] [PubMed]
- McCoy, S.W.; Jirikowic, T.; Price, R.; Ciol, M.A.; Hsu, L.Y.; Dellon, B.; Kartin, D. Virtual sensorimotor balance training for children with Fetal Alcohol Spectrum Disorders: Feasibility study. Phys. Ther. 2015, 95, 1569–1581. [Google Scholar] [CrossRef] [PubMed]
- Keil, V.; Paley, B.; Frankel, F.; O’Connor, M.J. Impact of a social skills intervention on the hostile attributions of children with Prenatal Alcohol Exposure. Alcohol Clin. Exp. Res. 2010, 34, 231–241. [Google Scholar] [CrossRef] [PubMed]
- Schonfeld, A.M.; Paley, B.; Frankel, F.; O’Connor, M.J. Behavioral Regulation as a Predictor of Response to Children’s Friendship Training in Children with Fetal Alcohol Spectrum Disorders. Clin. Neuropsychol. 2009, 23, 428–445. [Google Scholar] [CrossRef] [PubMed]
- Wells, A.M.; Chasnoff, I.J.; Schmidt, C.A.; Telford, E.; Schwartz, L.D. Neurocognitive Habilitation Therapy for Children with Fetal Alcohol Spectrum Disorders: An Adaptation of the Alert Program(R). Am. J. Occup. Ther. 2012, 66, 24–34. [Google Scholar] [CrossRef]
- O’connor, M.J.; Quattlebaum, J.; Castañeda, M.; Dipple, K.M. Alcohol Intervention for adolescents with Fetal Alcohol Spectrum Disorders: Project step up, a treatment development study. Alcohol Clin. Exp. Res. 2016, 40, 1744–1751. [Google Scholar] [CrossRef]
- Kerns, K.A.; Macoun, S.; MacSween, J.; Pei, J.; Hutchison, M. Attention and working memory training: A feasibility study in children with neurodevelopmental disorders. Appl. Neuropsychol. Child. 2017, 6, 120–137. [Google Scholar] [CrossRef]
- Coles, C.D.; Kable, J.A.; Taddeo, E.; Strickland, D.C. A Metacognitive Strategy for Reducing Disruptive Behavior in Children with Fetal Alcohol Spectrum Disorders: GoFAR Pilot. Alcohol Clin. Exp. Res. 2015, 39, 2224–2233. [Google Scholar] [CrossRef]
- Coles, C.D.; Strickland, D.C.; Padgett, L.; Bellmoff, L. Games that “work”: Using computer games to teach alcohol-affected children about fire and street safety. Res. Dev. Disabil. 2007, 28, 518–530. [Google Scholar] [CrossRef] [PubMed]
- Loomes, C.; Rasmussen, C.; Pei, J.; Manji, S.; Andrew, G. The effect of rehearsal training on working memory span of children with fetal alcohol spectrum disorder. Res. Dev. Disabil. 2008, 29, 113–124. [Google Scholar] [CrossRef] [PubMed]
- Clark, E.; George, M.A.; Hardy, C.; Hall, W.A.; MacMillan, P.D.; Wakabayashi, S.; Hughes, K. Exploratory study of the effectiveness of a professional development program on the academic achievement and classroom behavior of students with Fetal Alcohol Spectrum Disorder in British Columbia, Canada. Int. J. Alcohol Drug Res. 2014, 3, 25. [Google Scholar] [CrossRef]
- Leenaars, L.S.; Denys, K.; Henneveld, D.; Rasmussen, C. The impact of Fetal Alcohol Spectrum Disorders on families: Evaluation of a family intervention program. Community Ment. Health J. 2012, 48, 431–435. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, M.J.; Laugeson, E.A.; Mogil, C.; Lowe, E.; Welch-Torres, K.; Keil, V.; Paley, B. Translation of an evidence-based social skills intervention for children with Prenatal Alcohol Exposure in a community mental health setting. Alcohol Clin. Exp. Res. 2012, 36, 141–152. [Google Scholar] [CrossRef] [PubMed]
- Petrenko, C.L.; Pandolfino, M.E.; Quamma, J.; Olson, H.C. Emotional understanding in school-aged children with Fetal Alcohol Spectrum Disorders: A promising target for intervention. J. Popul. Ther. Clin. Pharmacol. 2017, 24, e21–e31. [Google Scholar] [CrossRef] [PubMed]
- Reid, N.; Dawe, S.; Harnett, P.; Shelton, D.; Hutton, L.; O’Callaghan, F. Feasibility study of a family-focused intervention to improve outcomes for children with FASD. Res. Dev. Disabil. 2017, 67, 34–46. [Google Scholar] [CrossRef] [Green Version]
- Petrenko, C.L.M.; Pandolfino, M.E.; Robinson, L.K. Findings from the families on track intervention pilot trial for children with Fetal Alcohol Spectrum Disorders and their families. Alcohol Clin. Exp. Res. 2017, 41, 1340–1351. [Google Scholar] [CrossRef]
- Millians, M.N.; Coles, C.D. Case study: Saturday cognitive habilitation program for children with prenatal alcohol exposure. Psychol. Neurosci. 2014, 7, 163–173. [Google Scholar] [CrossRef]
- Kable, J.A.; Taddeo, E.; Strickland, D.; Coles, C.D. Community translation of the Math interactive learning experience program for children with FASD. Res. Dev. Disabil. 2015, 39, 1–11. [Google Scholar] [CrossRef]
- Pomeroy, E.C.; Parrish, D.E. Online training on Fetal Alcohol Spectrum Disorders for court-appointed special advocates volunteers. Health Soc. Work 2013, 38, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Hanlon-Dearman, A.; Malik, S.; Wellwood, J.; Johnston, K.; Gammon, H.; Andrew, K.N.; Maxwell, B.; Longstaffe, S. A descriptive study of a community-based home-visiting program with preschool children prenatally exposed to alcohol. J. Popul. Ther. Clin. Pharmacol. 2017, 24, e61–e71. [Google Scholar] [CrossRef] [PubMed]
- Kable, J.A.; Coles, C.D.; Strickland, D.; Taddeo, E. Comparing the Effectiveness of On-Line versus In-Person Caregiver Education and Training for Behavioral Regulation in Families of Children with FASD. Int. J. Ment. Health Addict. 2012, 10, 791–803. [Google Scholar] [CrossRef] [PubMed]
- Pelech, W.; Badry, D.; Daoust, G. It takes a team: Improving placement stability among children and youth with Fetal Alcohol Spectrum Disorder in care in Canada. Child. Youth Serv. Rev. 2013, 35, 120–127. [Google Scholar] [CrossRef]
- Denys, K.; Rasmussen, C.; Henneveld, D. The Effectiveness of a Community-Based Intervention for Parents with FASD. Community Ment. Health J. 2011, 47, 209–219. [Google Scholar] [CrossRef] [PubMed]
- Olivier, L.; Curfs, L.M.G.; Viljoen, D.L. Fetal alcohol spectrum disorders: Prevalence rates in South Africa. South. African Med. J. 2016, 106, 103–106. [Google Scholar] [CrossRef] [PubMed]
- Dunn, C.; Deroo, L.; Rivara, F.P. The use of brief interventions adapted from motivational interviewing across behavioral domains: A systematic review. Addiction 2001, 96, 1725–1742. [Google Scholar] [CrossRef] [PubMed]
- Burke, B.L.; Arkowitz, H.; Menchola, M. The efficacy of motivational interviewing: A meta-analysis of controlled clinical trials. J. Consult. Clin. Psychol. 2003, 71, 843–861. [Google Scholar] [CrossRef] [PubMed]
- Martins, R.K.; McNeil, D.W. Review of motivational interviewing in promoting health behaviors. Clin. Psychol. Rev. 2009, 29, 283–293. [Google Scholar] [CrossRef]
- Nolte, E.M.M. Caring for people with chronic conditions. 2008. Available online: http://www.euro.who.int/__data/assets/pdf_file/0006/96468/E91878.pdf (accessed on 17 May 2018).
- Jepson, R.G.; Harris, F.M.; Platt, S.; Tannahill, C. The effectiveness of interventions to change six health behaviors: A review of reviews. BMC Public Health 2010, 10, 538. [Google Scholar] [CrossRef] [PubMed]
- Barati, H.; Tajrishi, P.; Sajedi, F. The effect of social skills training on socialization skills in children with Down syndrome. Iran. Rehabil. J. 2012, 10, 35–38. Available online: https://irj.uswr.ac.ir/article-1-240-en.pdf (accessed on 17 May 2018).
- Olsson, N.C.; Flygare, O.; Coco, C.; Görling, A.; Råde, A.; Chen, Q.; Lindstedt, K.; Berggren, S.; Serlachius, E.; Jonsson, U. Social skills training for children and adolescents with Autism Spectrum Disorder: A randomized controlled trial. J. Am. Acad. Child. Adolesc. Psychiatry 2017, 56, 585–592. [Google Scholar] [CrossRef] [PubMed]
- Rus-Calafell, M.; Gutiérrez-Maldonado, J.; Ribas-Sabaté, J.; Lemos-Giráldez, S. Social skills training for people with schizophrenia: What do we train? Behav. Psychol./Psicol. Conduct. 2014, 22, 461–477. [Google Scholar]
- DuPaul, G.J.; Weyandt, L.L.; Janusis, G.M. ADHD in the classroom: Effective intervention strategies. Theory Pract. 2011, 50, 35–42. [Google Scholar] [CrossRef]
- Johnson, M.H.; George, P.; Armstrong, M.I.; Lyman, D.R.; Dougherty, R.H.; Daniels, A.S.; Ghose, S.S.; Delphin-Rittmon, M.E. Behavioral management for children and adolescents: Assessing the evidence. Psychiatr. Serv. 2014, 65, 580–590. [Google Scholar] [CrossRef] [PubMed]
- Salmon, A.; Clarren, S.K. Developing effective, culturally appropriate avenues to FASD diagnosis and prevention in northern Canada. Int. J. Circumpolar Health 2011, 70, 428–433. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Criteria |
|---|---|
| Population | Individuals with FASD, young people, adult, women, and children |
| Intervention | Any strategy aimed at preventing or managing FASD |
| Comparison | Individuals who do not receive interventions |
| Outcome | Effective in preventing or managing FASD |
| Components | Strong | Moderate | Weak |
|---|---|---|---|
| Selection bias | Very likely to be representative of the target population and >80% participation rate | Somewhat likely to be representative of the target population and 60% to 79% participation rate | Not likely to be representative (i.e., self-referred), <60% participation rate or not stated |
| Design | Randomized controlled trial and controlled clinical trial | Cohort analytic, case-control, cohort, or an interrupted time series | All other designs or designs not stated |
| Cofounders | Controlled for at least 80% of confounders | Controlled for 60% to 79% of confounders | Confounders not controlled for, or not stated |
| Blinding | Blinding of outcome assessor and study participants to intervention status and/or research question | Blinding of either outcome assessor or study participants or blinding is not described | Outcome assessor and study participants are aware of intervention status and/or research question |
| Data collection methods | Tools are valid and reliable | Tools are valid but have not been shown to be reliable | No evidence of validity or reliability |
| Withdrawals and dropouts | Follow-up rate of >80% of participants | Follow-up rate of 60% to 79% of participants | Follow-up rate of <60% of participants or withdrawals and dropouts not described |
| Characteristics | Number of Studies |
|---|---|
| Research approach | |
| Quantitative | 72 |
| Mixed method | 1 |
| Study design | |
| Mixed method | 1 |
| Descriptive longitudinal study | 1 |
| Prospective | 3 |
| Survey | 2 |
| Dichotomized control trial | 2 |
| Retrospective case analysis | 4 |
| Pre-post-test | 13 |
| Non-randomized control trial | 2 |
| Randomized control trial | 40 |
| Quasi-experimental | 2 |
| Case study | 2 |
| Cohort analytic | 1 |
| Type of intervention | |
| Prevention | 32 |
| Management | 41 |
| Study setting (continent) | |
| North America | 61 |
| Africa | 5 |
| Europe | 3 |
| Australia | 3 |
| Asia | 1 |
| Prevention Interventions | |||
|---|---|---|---|
| Nature of Interventions | Numbers of Studies and Citation | Interventions | Outcomes of Interventions |
| Facility-based | Joya et al. [43] | Single-session motivational interview for pregnant women | Decreased alcohol consumption during pregnancy |
| Velasquez et al. [44] | Dual-focused approach (motivation interviewing on alcohol and contraception) | Reduced the risk for alcohol-exposed pregnancy (AEP) by increasing the effective use of contraception and decreasing alcohol use | |
| Payne et al. [45] | Educational resources on FASD for Health professionals | Increased practitioners’ knowledge of FASD | |
| Mwansa-Kambafwile et al. [13] | Training course on FASD capacity building for service providers | Built service providers’ capacity to prevent and manage women at risk for AEP | |
| Ondersma et al. [46] | Computer-Delivered Screening and Brief Intervention for pregnant women | Demonstrated efficacy for favorable birth outcome | |
| Delrahim-Howlett et al. [47] | Web-based alcohol assessment and personalized feedback for women of reproductive age | Reduced number of risky alcohol consumption | |
| Tzilos et al. [48] | Brief Computer-Delivered Intervention for pregnant women | Significantly decreased alcohol use | |
| Hutton et al. [49] | Project CHOICES intervention for women | Decreased the AEP risk in the through effective use of contraception and decrease alcohol use | |
| Osterman et al. [50] | Single-session of motivational interviewing (MI) for women | MI was not found effective in decreasing alcohol use | |
| Osterman and Dyehouse [51] | Motivational interview intervention for pregnant women | MI was not found effective in decreasing alcohol use | |
| School-based/education-based | LaChausse [52] | Multimedia presentation on FASD for high school students | Increased the students’ knowledge of FASD |
| Boulter [53] | Peer-delivered educational presentation on FASD for youth | Increased youths’ knowledge about FASD | |
| Toyama and Sudo [54] | Tailored leaflet educational intervention | Improved knowledge of pregnant women re FASD | |
| Community-based | Hanson et al. [55] | Preconception prevention program (motivational interview techniques) for at-risk women | Reduced the risk for AEP by increasing contraception use |
| Farrell-Carnahan et al. [56] | One-session motivational interview for non–treatment-seeking community women | Decreased the AEP risk in the community by increasing contraception use and decreasing alcohol use | |
| Hanson et al. [11] | Motivational interview-based intervention for women | Modified self-reported drinking and contraception behavior positively | |
| O’Connor and Whaley [10] | Brief intervention (10–15 min counseling sessions) for pregnant women | Promoted abstinence from alcohol by increasing motivation to change unhealthy behavior | |
| Letourneau et al. [57] | Mail-based prevention program for at-risk women | Reduced the risk for AEP by increasing the effective use of contraception | |
| Tenkku et al. [58] | Web-based intervention using tailored motivational messaging for women | Reduced the risk of an AEP by increasing the effective use of contraception and decreasing alcohol use | |
| De Vries et al. [12] | Case management intervention for heavy drinking pregnant women | Helped women to stop drinking and reduced the risk of FASD | |
| Montag et al. [59] | Targeted Screening, Brief Intervention, and Referral to Treatment (SBIRT) intervention for women | Decreased risky drinking behavior and vulnerability to AEP | |
| May et al. [60] | Case management intervention for heavy drinking pregnant women | Reduced maternal alcohol drinking at critical times | |
| France et al. [61] | Threat-based and self-efficacy based message on alcohol for women | Promoted women’s intentions to abstain from alcohol | |
| Wilton et al. [62] | Telephone-based brief intervention (counseling sessions) | Reduced the risk of an AEP by increasing contraception use and decreasing alcohol use | |
| Rasmussen et al. [63] | Mentorship program for at-risk women | Reduced the risk of an AEP by increasing contraception use | |
| Floyd et al. [64] | Brief motivational intervention for women | Reduced the risk of an AEP by increasing contraception use and decreasing alcohol use | |
| Chersich et al. [9] | Universal intervention (highlighting FASD using local media and health promotion talks at health facilities) | Reduced the prevalence of FASD by increasing knowledge of harms of maternal drinking | |
| Dresser et al. [65] | Training program on FASD for alcohol-server | Reduced serving of alcohol to pregnant women | |
| Hanson et al. [66] | Media campaign on FASD for women | Increased knowledge of FASD and decreased actual drinking | |
| May et al. [67] | Case management intervention for women | Helped women to stop drinking and reduced the risk of FASD | |
| Ingersoll et al. [68] | Pre-conceptional motivational interviewing interventions for women | Decreased DDD (drinks per drinking day), ineffective contraception rate and AEP risk | |
| Russell et al. [69] | Project CHOICES intervention for youth and adult | Demonstrated increased effectiveness of birth control use and decreased use and abuse of alcohol | |
| Management Interventions | |||
|---|---|---|---|
| Nature of Interventions | Numbers of Studies and Citation | Interventions | Outcomes of Interventions |
| Facility-based | Nguyen et al. [70] | Use of choline supplement for children | Did not improve cognitive performance |
| Zarnegar et al. [71] | Use of neuro-developmentally informed intervention for children | Improved developmental deficit in several domains | |
| Wozniak et al. [72] | Use of choline supplement for children | Improved neurocognitive functioning | |
| Wozniak et al. [73] | Use of choline supplement for children | Has potential to improve neurocognitive functioning | |
| Wilczynski et al. [74] | Use of sensory integration (SI) therapy for children | Improved gross motor function | |
| Yazdani et al. [75] | An early intervention program for mother and young children | Mitigated cognitive deficit | |
| Kable et al. [76] | Use of choline supplement with multivitamin/mineral for children | Impacted brain development positively | |
| Connolly et al. [77] | Applied behavior analysis (ABA)-based verbal behavior treatment program for children | Showed rapid skill acquisition in communication adaptive emotional/behavioral functioning | |
| Nash et al. [78] | Individual designated therapy room for children | Ameliorated executive functioning deficits | |
| Soh et al. [79] | Sensory integration and cognitive behavioral training | Improved self-regulation skills and brain development | |
| Keiver et al. [80] | Physical activity program for children with FASD | Showed differences in cortisol levels in children with FASD compared to Controls | |
| Nash et al. [81] | Alert® Program for Self-Regulation for behavioral regulation for children | Improved functional integrity in the neural circuitry for behavioral regulation | |
| Doig et al. [82] | Attention-deficit/hyperactivity disorder (ADHD) treatment for children | Inattention may be less responsive to ADHD medication | |
| School-based/education-based | Coles et al. [83] | Educational intervention for specific learning and behavior need for children | Improved both mathematical skill and behavior |
| Kerns et al. [84] | Use of computerized attention training for children | Improved cognitive performance | |
| Jirikowic et al. [85] | Intervention to increase compliance with motor function in children | Improved sensory adaptation, balance and motor performance | |
| Adnams et al. [86] | Classroom language and literacy intervention for children | Improved cognitive in targeted brain areas | |
| Kable et al. [87] | The educational intervention focused on behavior mathematical functions for children | Remediated mathematical deficits | |
| Kable et al. [88] | Computerized instruction for children | Improved self-regulation | |
| McCoy et al. [89] | Sensorimotor Training for children | Increased postural sway velocity | |
| Keil et al. [90] | Social skills intervention | Improved deficits in social information-processing | |
| Schonfeld et al. [91] | Social-skills and play-therapy | Improved social skills and reduced problem behaviors | |
| Wells et al. [92] | Group therapy intervention for foster and adoptive caregivers and children | Improved the executive functioning and emotional problem-solving | |
| O’Connor et al. [93] | Alcohol reduction intervention for adolescents with FASD | Reduced and prevented alcohol use and some secondary disabilities | |
| Kerns et al. [94] | Game-based process specific intervention for children | Improved cognitive development | |
| Coles et al. [95] | Computer game for a metacognitive control strategy for children | Reduced disruptive behaviors | |
| Coles et al. [96] | Virtual reality game of fire safety and street safety for children | Showed significantly better knowledge of the game to which they were exposed | |
| Loomes et al. [97] | Rehearsal training on working memory span of children | Showed improvement in digit span in children receiving rehearsal training | |
| Clark et al. [98] | Professional development program for teachers | Provided support for the effectiveness of the professional development program for teachers | |
| Community-based | Leenaars et al. [99] | Families intervention program | Assisted families to cope with stress |
| O’Connor et al. [100] | Social-skills and play-therapy for children and parents | Improved knowledge of appropriate social skills, and parent-reported social skills | |
| Petrenko et al. [101] | Tailored intervention for children and caregivers | Improved child self-regulation and caregiver behavior | |
| Reid et al. [102] | Home-based program for high-risk, vulnerable families | Improved self-regulatory skills | |
| Petrenko et al. [103] | Program targeting key risk and protective factors for children and families | Showed promising result for the prevention of secondary conditions and improves the family adaptation | |
| Millians and Coles [104] | A program developed to address neurocognitive mathematical impairments for children | Remediated learning problems | |
| Kable et al. [105] | Mathematical skills intervention for children | Improved mathematical skill | |
| Pomeroy and Parrish [106] | Online training on FASD for Court Appointed Special Advocates | Improved FASD knowledge | |
| Hanlon-Dearman et al. [107] | Use of community home-based attachment intervention for caregivers | Improved communication of needs | |
| Kable et al. [108] | Caregiver Education and Training for Behavioral Regulation for children | Improved caregivers’ knowledge of FASD | |
| Pelech et al. [109] | Intervention to enhance practice at child welfare and improve placement stability | Significant decline in number of placement changes | |
| Denys et al. [110] | Step by Step mentor program for parents | Significant reduction in client’s needs and significant increase in client’s goals | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adebiyi, B.O.; Mukumbang, F.C.; Erasmus, C. The Distribution of Available Prevention and Management Interventions for Fetal Alcohol Spectrum Disorder (2007 to 2017): Implications for Collaborative Actions. Int. J. Environ. Res. Public Health 2019, 16, 2244. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16122244
Adebiyi BO, Mukumbang FC, Erasmus C. The Distribution of Available Prevention and Management Interventions for Fetal Alcohol Spectrum Disorder (2007 to 2017): Implications for Collaborative Actions. International Journal of Environmental Research and Public Health. 2019; 16(12):2244. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16122244
Chicago/Turabian StyleAdebiyi, Babatope O., Ferdinand C. Mukumbang, and Charlene Erasmus. 2019. "The Distribution of Available Prevention and Management Interventions for Fetal Alcohol Spectrum Disorder (2007 to 2017): Implications for Collaborative Actions" International Journal of Environmental Research and Public Health 16, no. 12: 2244. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16122244