Diabetes Mellitus: An Independent Risk Factor of In-Hospital Mortality in Patients with Infective Endocarditis in a New Era of Clinical Practice

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
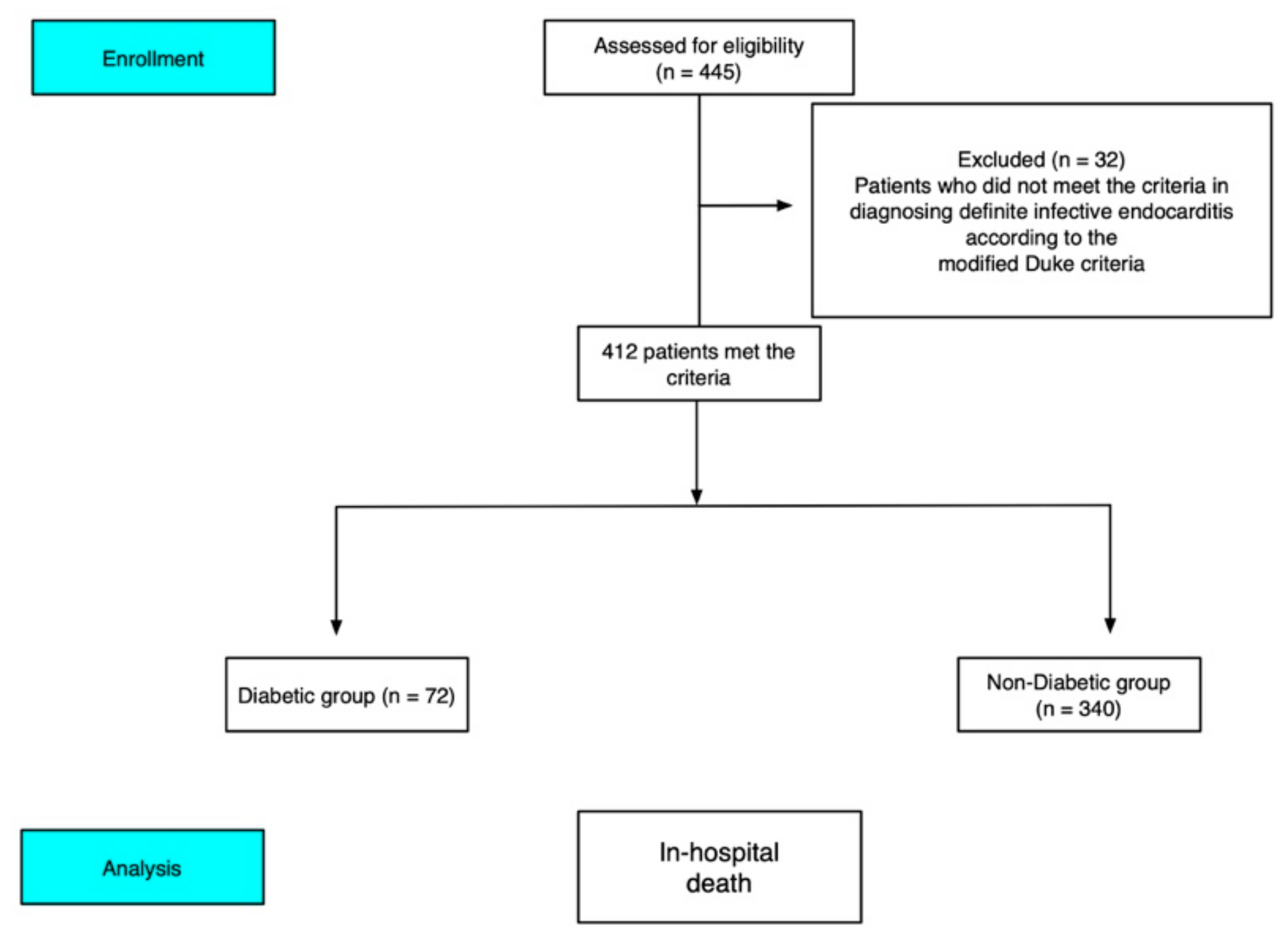
2.1. Patient Selection and Study Population
2.2. Definitions
2.3. End Point and Statistical Analysis
3. Results
3.1. Patient Characteristics and Clinical Data
3.2. Clinical Laboratory Data, Echocardiographic Findings and Complications of Infective Endocarditis (IE)
3.3. Causative Microorganism and Complications of IE
3.4. Predictors for In-Hospital Mortality
4. Discussion
4.1. Main Findings
4.2. The Clinical Presentations and Associated Comorbidities of IE Patients with Diabetes Mellitus (DM)
4.3. The Impact of DM in Predicting In-Hospital Mortality and Probable Mechanisms
4.4. Clinical Implications
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Baddour, L.M.; Wilson, W.R.; Bayer, A.S.; Fowler, V.G., Jr.; Bolger, A.F.; Levison, M.E.; Ferrieri, P.; Gerber, M.A.; Tani, L.Y.; Gewitz, M.H.; et al. Infective endocarditis: Diagnosis, antimicrobial therapy, and management of complications: A statement for healthcare professionals from the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in the Young, and the Councils on Clinical Cardiology, Stroke, and Cardiovascular Surgery and Anesthesia, American Heart Association: Endorsed by the Infectious Diseases Society of America. Circulation 2005, 111, 394–434. [Google Scholar]
- Nishimura, R.A.; Carabello, B.A.; Faxon, D.P.; Freed, M.D.; Lytle, B.W.; O’Gara, P.T.; O’Rourke, R.A.; Shah, P.M.; Bonow, R.O.; Carabello, B.A.; et al. ACC/AHA 2008 guideline update on valvular heart disease: Focused update on infective endocarditis: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines: Endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. Circulation 2008, 118, 887–896. [Google Scholar] [PubMed]
- Shih, C.J.; Chu, H.; Chao, P.W.; Lee, Y.J.; Kuo, S.C.; Li, S.Y.; Tarng, D.C.; Yang, C.Y.; Yang, W.C.; Ou, S.M.; et al. Long-term clinical outcome of major adverse cardiac events in survivors of infective endocarditis: A nationwide population-based study. Circulation 2014, 130, 1684–1691. [Google Scholar] [CrossRef] [PubMed]
- Duval, X.; Delahaye, F.; Alla, F.; Tattevin, P.; Obadia, J.F.; Le Moing, V.; Doco-Lecompte, T.; Celard, M.; Poyart, C.; Strady, C.; et al. Temporal trends in infective endocarditis in the context of prophylaxis guideline modifications: Three successive population-based surveys. J. Am. Coll. Cardiol. 2012, 59, 1968–1976. [Google Scholar] [CrossRef] [PubMed]
- Sy, R.W.; Chawantanpipat, C.; Richmond, D.R.; Kritharides, L. Thrombocytopenia and mortality in infective endocarditis. J. Am. Coll. Cardiol. 2008, 51, 1824–1825. [Google Scholar] [CrossRef]
- De Lastours, V.; Foxman, B. Urinary tract infection in diabetes: Epidemiologic considerations. Curr. Infect. Dis. Rep. 2014, 16, 389. [Google Scholar] [CrossRef]
- Koskela, H.O.; Salonen, P.H.; Romppanen, J.; Niskanen, L. Long-term mortality after community-acquired pneumonia-impacts of diabetes and newly discovered hyperglycaemia: A prospective, observational cohort study. BMJ Open 2014, 4, e005715. [Google Scholar] [CrossRef]
- Korbel, L.; Spencer, J.D. Diabetes mellitus and infection: An evaluation of hospital utilization and management costs in the United States. J. Diabetes Its Complicat. 2015, 29, 192–195. [Google Scholar] [CrossRef]
- UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet 1998, 352, 837–853. [Google Scholar] [CrossRef]
- Adler, A.I.; Stratton, I.M.; Neil, H.A.; Yudkin, J.S.; Matthews, D.R.; Cull, C.A.; Wright, A.D.; Turner, R.C.; Holman, R.R. Association of systolic blood pressure with macrovascular and microvascular complications of type 2 diabetes (UKPDS 36): Prospective observational study. BMJ 2000, 321, 412–419. [Google Scholar] [CrossRef]
- Davis, T.M.; Coleman, R.L.; Holman, R.R.; Group, U. Prognostic significance of silent myocardial infarction in newly diagnosed type 2 diabetes mellitus: United Kingdom Prospective Diabetes Study (UKPDS) 79. Circulation 2013, 127, 980–987. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, M.; Leslie, D.R. Inverse relation between humoral and cellular immunity to glutamic acid decarboxylase in subjects at risk of insulin-dependent diabetes. J. Endocrinol. Investig. 1994, 17, 581–584. [Google Scholar]
- Hawke, S.; Harcourt, G.; Pantic, N.; Beeson, D.; Willcox, N.; Newson-Davis, J. Cellular and humoral immunity in patients with insulin-dependent diabetes. Lancet 1993, 342, 246. [Google Scholar] [PubMed]
- Kaneshige, H.; Endoh, M.; Tomino, Y.; Nomoto, Y.; Sakai, H.; Arimori, S. Impaired granulocyte function in patients with diabetes mellitus. Tokai J. Exp. Clin. Med. 1982, 7, 77–80. [Google Scholar] [PubMed]
- Delamaire, M.; Maugendre, D.; Moreno, M.; Le Goff, M.C.; Allannic, H.; Genetet, B. Impaired leucocyte functions in diabetic patients. Diabet. Med. J. Br. Diabet. Assoc. 1997, 14, 29–34. [Google Scholar] [CrossRef]
- Olmos, C.; Vilacosta, I.; Fernandez, C.; Lopez, J.; Sarria, C.; Ferrera, C.; Revilla, A.; Silva, J.; Vivas, D.; Gonzalez, I.; et al. Contemporary epidemiology and prognosis of septic shock in infective endocarditis. Eur. Heart J. 2013, 34, 1999–2006. [Google Scholar] [CrossRef] [PubMed]
- Di Yacovo, S.; Garcia-Vidal, C.; Viasus, D.; Adamuz, J.; Oriol, I.; Gili, F.; Vilarrasa, N.; Garcia-Somoza, M.D.; Dorca, J.; Carratala, J. Clinical features, etiology, and outcomes of community-acquired pneumonia in patients with diabetes mellitus. Medicine 2013, 92, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Joshi, N.; Caputo, G.M.; Weitekamp, M.R.; Karchmer, A.W. Infections in patients with diabetes mellitus. N. Engl. J. Med. 1999, 341, 1906–1912. [Google Scholar] [CrossRef]
- Bech-Nielsen, G.V.; Hansen, C.H.; Hufeldt, M.R.; Nielsen, D.S.; Aasted, B.; Vogensen, F.K.; Midtvedt, T.; Hansen, A.K. Manipulation of the gut microbiota in C57BL/6 mice changes glucose tolerance without affecting weight development and gut mucosal immunity. Res. Vet. Sci. 2012, 92, 501–508. [Google Scholar] [CrossRef]
- Rapp, U.K.; Kaufmann, S.H. Glucose-regulated stress proteins and antibacterial immunity. Trends Microbiol. 2003, 11, 519–526. [Google Scholar] [CrossRef]
- Giorgino, F.; Leonardini, A.; Laviola, L. Cardiovascular disease and glycemic control in type 2 diabetes: Now that the dust is settling from large clinical trials. Ann. N. Y. Acad. Sci. 2013, 1281, 36–50. [Google Scholar] [CrossRef] [PubMed]
- Duval, X.; Alla, F.; Doco-Lecompte, T.; Le Moing, V.; Delahaye, F.; Mainardi, J.L.; Plesiat, P.; Celard, M.; Hoen, B.; Leport, C.; et al. Diabetes mellitus and infective endocarditis: The insulin factor in patient morbidity and mortality. Eur. Heart J. 2007, 28, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease, C. Prevention, Trends in the prevalence and incidence of self-reported diabetes mellitus—United States, 1980–1994. Mmwr. Morb. Mortal. Wkly. Rep. 1997, 46, 1014–1018. [Google Scholar]
- Chu, V.H.; Cabell, C.H.; Benjamin, D.K., Jr.; Kuniholm, E.F.; Fowler, V.G., Jr.; Engemann, J.; Sexton, D.J.; Corey, G.R.; Wang, A. Early predictors of in-hospital death in infective endocarditis. Circulation 2004, 109, 1745–1749. [Google Scholar] [CrossRef] [PubMed]
- Olmos, C.; Vilacosta, I.; Pozo, E.; Fernandez, C.; Sarria, C.; Lopez, J.; Ferrera, C.; Maroto, L.; Gonzalez, I.; Vivas, D.; et al. Prognostic implications of diabetes in patients with left-sided endocarditis: Findings from a large cohort study. Medicine 2014, 93, 114–119. [Google Scholar] [CrossRef] [PubMed]
- Clinicopathologic Session. (Case 1/00-a 65-year-old woman with heart failure and proteinuria—Instituto do Coracao do Hospital das Clinicas-FMUSP. Arq. Bras. Cardiol. 2000, 74, 159–166. [Google Scholar]
- Horstkotte, D.; Follath, F.; Gutschik, E.; Lengyel, M.; Oto, A.; Pavie, A.; Soler-Soler, J.; Thiene, G.; von Graevenitz, A.; Priori, S.G.; et al. Guidelines on prevention, diagnosis and treatment of infective endocarditis executive summary; the task force on infective endocarditis of the European society of cardiology. Eur. Heart J. 2004, 25, 267–276. [Google Scholar] [CrossRef]
- Mugge, A.; Daniel, W.G.; Frank, G.; Lichtlen, P.R. Echocardiography in infective endocarditis: Reassessment of prognostic implications of vegetation size determined by the transthoracic and the transesophageal approach. J. Am. Coll. Cardiol. 1989, 14, 631–638. [Google Scholar] [CrossRef] [Green Version]
- Rodbard, H.W.; Blonde, L.; Braithwaite, S.S.; Brett, E.M.; Cobin, R.H.; Handelsman, Y.; Hellman, R.; Jellinger, P.S.; Jovanovic, L.G.; Levy, P.; et al. American Association of Clinical Endocrinologists medical guidelines for clinical practice for the management of diabetes mellitus. Endocr. Pract. Off. J. Am. Coll. Endocrinol. Am. Assoc. Clin. Endocrinol. 2007, 13, 1–68. [Google Scholar] [CrossRef]
- McKee, P.A.; Castelli, W.P.; McNamara, P.M.; Kannel, W.B. The natural history of congestive heart failure: The Framingham study. N. Engl. J. Med. 1971, 285, 1441–1446. [Google Scholar] [CrossRef]
- Saji, M.; Katz, M.R.; Ailawadi, G.; Fowler, D.E.; Ragosta, M.; Lim, D.S. Predictive Value of Age-Adjusted Charlson Co-Morbidity Index for 1-, 3- and 5-Year Mortality in Patients Requiring Transcatheter Mitral Valve Repair. Am. J. Cardiol. 2017, 120, 309–314. [Google Scholar] [CrossRef] [PubMed]
- Lu, K.J.; Kearney, L.G.; Ord, M.; Jones, E.; Burrell, L.M.; Srivastava, P.M. Age adjusted Charlson Co-morbidity Index is an independent predictor of mortality over long-term follow-up in infective endocarditis. Int. J. Cardiol. 2013, 168, 5243–5248. [Google Scholar] [CrossRef] [PubMed]
- Bartko, P.E.; Arfsten, H.; Heitzinger, G.; Pavo, N.; Toma, A.; Strunk, G.; Hengstenberg, C.; Hulsmann, M.; Goliasch, G. A Unifying Concept for the Quantitative Assessment of Secondary Mitral Regurgitation. J. Am. Coll. Cardiol. 2019, 73, 2506–2517. [Google Scholar] [CrossRef] [PubMed]
- Bland, J.M.; Altman, D.G. Statistics Notes: Bootstrap resampling methods. BMJ 2015, 350, h2622. [Google Scholar] [CrossRef] [PubMed]
- Dwivedi, A.K.; Mallawaarachchi, I.; Alvarado, L.A. Analysis of small sample size studies using nonparametric bootstrap test with pooled resampling method. Stat. Med. 2017, 36, 2187–2205. [Google Scholar] [CrossRef]
- Mylonakis, E.; Calderwood, S.B. Infective endocarditis in adults. N. Engl. J. Med. 2001, 345, 1318–1330. [Google Scholar] [CrossRef] [PubMed]
- Murdoch, D.R.; Corey, G.R.; Hoen, B.; Miro, J.M.; Fowler, V.G., Jr.; Bayer, A.S.; Karchmer, A.W.; Olaison, L.; Pappas, P.A.; Moreillon, P.; et al. International Collaboration on Endocarditis-Prospective Cohort Study, I., Clinical presentation, etiology, and outcome of infective endocarditis in the 21st century: The International Collaboration on Endocarditis-Prospective Cohort Study. Arch. Intern. Med. 2009, 169, 463–473. [Google Scholar] [CrossRef]
- Kourany, W.M.; Miro, J.M.; Moreno, A.; Corey, G.R.; Pappas, P.A.; Abrutyn, E.; Hoen, B.; Habib, G.; Fowler, V.G., Jr.; Sexton, D.J.; et al. Influence of diabetes mellitus on the clinical manifestations and prognosis of infective endocarditis: A report from the International Collaboration on Endocarditis-Merged Database. Scand. J. Infect. Dis. 2006, 38, 613–619. [Google Scholar] [CrossRef]
- Suzuki, K.; Yoshioka, D.; Toda, K.; Yokoyama, J.Y.; Samura, T.; Miyagawa, S.; Yoshikawa, Y.; Hata, H.; Takano, H.; Matsumiya, G.; et al. Results of surgical management of infective endocarditis associated with Staphylococcus aureus. Eur. J. Cardiothorac. Thorac. Surg. 2019, 56, 30–37. [Google Scholar] [CrossRef]
- Rieg, S.; von Cube, M.; Kaasch, A.; Bonaventura, B.; Bothe, W.; Wolkewitz, M.; Peyerl-Hoffmann, G.; Deppe, A.C.; Wahlers, T.; Beyersdorf, F.; et al. Investigating the impact of early valve surgery on survival in Staphylococcus aureus infective endocarditis using a marginal structural model approach-results of a large prospectively evaluated cohort. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2018. [Google Scholar] [CrossRef]
- Heriot, G.S.; Cheng, A.C.; Tong, S.Y.C.; Liew, D. Clinical predictors and prediction rules to estimate initial patient risk for infective endocarditis in Staphylococcus aureus bacteraemia: Attention must be paid to the reference standard. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2018, 24, 314–316. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.Y.; Chang, T.M.; Lin, C.J.; Huang, Y.C. Infective endocarditis caused by community-associated methicillin-resistant Staphylococcus aureus in a previously healthy preschool child. J. Microbiol. Immunol. Infect. 2014, 47, 257–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, S.M.; Sorabella, R.A.; Vasan, S.; Grbic, M.; Lambert, D.; Prasad, R.; Wang, C.; Kurlansky, P.; Borger, M.A.; Gordon, R.; et al. Influence of Staphylococcus aureus on Outcomes after Valvular Surgery for Infective Endocarditis. J. Cardiothorac. Surg. 2017, 12, 57. [Google Scholar] [CrossRef] [PubMed]
- Bai, A.D.; Agarwal, A.; Steinberg, M.; Showler, A.; Burry, L.; Tomlinson, G.A.; Bell, C.M.; Morris, A.M. Clinical predictors and clinical prediction rules to estimate initial patient risk for infective endocarditis in Staphylococcus aureus bacteraemia: A systematic review and meta-analysis. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2017, 23, 900–906. [Google Scholar] [CrossRef] [PubMed]
- Ohara, T.; Nakatani, S.; Kokubo, Y.; Yamamoto, H.; Mitsutake, K.; Hanai, S.; Investigators, C. Clinical predictors of in-hospital death and early surgery for infective endocarditis: Results of CArdiac Disease REgistration (CADRE), a nation-wide survey in Japan. Int. J. Cardiol. 2013, 167, 2688–2694. [Google Scholar] [CrossRef] [PubMed]
- Geerlings, S.E.; Hoepelman, A.I. Immune dysfunction in patients with diabetes mellitus (DM). Fems. Immunol. Med. Microbiol. 1999, 26, 259–265. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, M.; Uzuka, T.; Sato, H.; Kondo, M.; Sakata, J.; Kodama, F.; Murai, D.; Komatsu, H.; Makino, T.; Kohya, T. Early surgery with aggressive surgical approach to improve 6-month outcomes in patients with active infective endocarditis: Contribution of cerebral preoperative magnetic resonance imaging. Gen. Thorac. Cardiovasc. Surg. 2019, 67, 427–435. [Google Scholar] [CrossRef] [PubMed]
- Varela Barca, L.; Lopez-Menendez, J.; Navas Elorza, E.; Moya Mur, J.L.; Centella Hernendez, T.; Redondo Palacios, A.; Fajardo, E.R.; Miguelena Hycka, J.; Martin Garcia, M.; Munoz Perez, R.; et al. Long-term prognosis after surgery for infective endocarditis: Distinction between predictors of early and late survival. Enferm. Infecc. Microbiol. Clin. 2018. [Google Scholar] [CrossRef]


{kind=link}
| Baseline Characteristics | DM (72) | Without DM (340) | p |
|---|---|---|---|
| Age | 55.9 ± 11.7 | 44.2 ± 17.1 | 0.001 |
| Male | 75% (54) | 79.4% (270) | 0.407 |
| Comorbidity | |||
| CHD | 6.9% (5) | 15.3% (52) | 0.06 |
| CKD | 26.4% (19) | 8.8% (30) | 0.001 |
| HTN | 51.4% (37) | 23.3 (79) | 0.001 |
| LC | 10.4% (5) | 4% (10) | 0.099 |
| Malignancy | 4.2% (3) | 2.4% (8) | 0.386 |
| Rheumatic heart disease | 11.1% (8) | 17.9% (61) | 0.159 |
| Prosthetic valve | 4.2% (3) | 13% (44) | 0.033 |
| Previous endocarditis | 11.1% (8) | 5.9% (20) | 0.109 |
| ACCI score | 3.24 | 2.13 | 0.002 |
| IV drug user | 8.3% (6) | 28.5% (97) | 0.001 |
| Diabetic status | |||
| Oral DM | 84.7% (61) | 0% | 0.001 |
| Insulin DM | 15.3% (11) | 0% | 0.001 |
| Dyspnea | 18% (13) | 16.2% (55) | 0.696 |
| Neurological symptoms | 16.7% (12) | 13.5% (46) | 0.687 |
| Constitutional symptoms | 18.1% (13) | 7.6% (26) | 0.006 |
| Time from admission to the diagnosis of IE (hours) | 89 (64–127) | 56 (32–89) | 0.032 |
| DM (72) | Without DM (340) | p | |
|---|---|---|---|
| Laboratory findings | |||
| WBC counts (×103/mL) | 13.6 ± 6.1 | 13.9 ± 6.7 | 0.707 |
| Hemoglobin level (g/dL) | 11.1 ± 2.75 | 10.9 ± 2.33 | 0.950 |
| Platelet cell count (×103/mL) | 185.3 ± 97.8 | 205.9 ± 112.5 | 0.235 |
| Serum creatinine level (mg/dL) | 2.26 ±2.63 | 1.52 ± 2.04 | 0.029 |
| eGFR | 41.2 ± 6.5 | 57.9± 5.4 | <0.01 |
| Location of IE | |||
| Aortic valve | 44.4% (32) | 44.1% (142) | 0.676 |
| Mitral valve | 40.7% (28) | 41.5% (129) | 0.880 |
| Tricuspid valve | 6.9% (6) | 9.4% (32) | 0.403 |
| Aortic + mitral valve | 2.7% (2) | 2.1% (7) | 0.705 |
| Echocardiography | |||
| Abscess | 2.8% (2) | 2.9% (10) | 0.940 |
| Valve perforation | 5.6% (4) | 6.5% (22) | 0.772 |
| Pericardial effusion | 9.7% (7) | 5.3% (18) | 0.153 |
| Vegetation * | 31.9% (23) | 25.3% (86) | 0.245 |
| Complication of IE | |||
| Neurological complications | 25.1% (18) | 22.6% (77) | 0.667 |
| Pulmonary septic embolisms | 6.9% (5) | 13.2 (25) | 0.775 |
| Peripheral embolic complications | 4.1% (3) | 6.7% (23) | 0.410 |
| Advanced congestive heart failure | 34.7% (25) | 27.9% (95) | 0.250 |
| Surgical intervention | 12.5% (9) | 24.4% (83) | 0.04 |
| In-hospital mortality | 41.7% (30) | 16.5% (56) | <0.001 |
| Microorganisms | DM (72) | Without DM (340) | p |
|---|---|---|---|
| Staphylococcus aureus | 41.7% (30) | 27.9% (95) | 0.021 |
| Coagulase-negative Staphylococci | 8.3% (6) | 4.1% (14) | 0.131 |
| Staphylococcus epidermis | 1.4% (2) | 4.7% (16) | 0.467 |
| Viridans streptococci | 27.8% (20) | 36.2% (123) | 0.174 |
| Other Streptococci spp. | 8.3% (6) | 7.4% (25) | 0.775 |
| Enterococcus spp. | 2.8% (2) | 6.2% (21) | 0.254 |
| Gram-negative bacteria | 0% (0) | 1.2% (4) | 0.355 |
| Fungus | 0% (0) | 0.3% (1) | 0.645 |
| Other microorganisms | 1.4% (1) | 1.5% (5) | 0.958 |
| No microorganism identified | 6.9% (5) | 10.6% (36) | 0.348 |
| Variables | OR | 95% CI | p Value |
|---|---|---|---|
| ACCI score > 3 | 4.42 | 2.11–6.73 | 0.002 |
| Ages (per years) | 1.09 | 1.04–1.14 | 0.011 |
| Male gender | 1.08 | 0.34–1.81 | 0.781 |
| WBC (increased per 103/mL) | 1.00 | 0.99–1.001 | 0.418 |
| Serum creatinine level Platelet cell count (increased per 103/mL) | 1.06 0.993 | 0.79–1.32 0.99–0.997 | 0.5 0.0001 |
| RHD | 2.32 | 0.46–4.18 | 0.559 |
| Drug abuse | 0.96 | 0.32–1.59 | 0.417 |
| Previous IE | 4.05 | 0.62–7.47 | 0.221 |
| Advanced heart failure Liver cirrhosis Diabetes mellitus Chronic renal failure Viridans streptococci | 8.43 1.26 3.29 1.91 0.36 | 1.37–15.49 0.57–8.55 1.47–5.11 0.38–3.44 0.16–0.56 | 0.030 0.261 0.003 0.82 0.02 |
| Staphylococcus aureus | 3.13 | 1.15–5.10 | 0.011 |
| Enterococci spp. Neurological complications Surgical intervention | 2.73 4.36 0.27 | 0.79–9.83 2.14–9.17 0.11–0.43 | 0.12 0.00009 0.004 |
| Variables | Logistic Regression | Bootstrap-Adjusted | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p Value | OR | 95% CI | p Value | |
| Age | 1.08 | 1.05–1.11 | 0.001 | 1.05 | 1.04–1.06 | 0.012 |
| ACCI score > 3 | 3.56 | 1.89–5.23 | 0.0032 | 3.78 | 1.97–5.59 | 0.0093 |
| Advanced heart failure | 8.76 | 1.24–16.28 | 0.041 | 6.32 | 2.13–10.51 | 0.032 |
| Diabetes mellitus | 2.36 | 1.31–3.41 | 0.012 | 3.02 | 1.56–4.48 | 0.021 |
| Viridans streptococci | 0.34 | 0.11–0.57 | 0.032 | 0.32 | 0.13–0.51 | 0.028 |
| Neurological complications | 4.17 | 2.06–6.28 | 0.0012 | 4.52 | 2.16–6.88 | 0.0017 |
| Surgical interventions | 0.32 | 0.09–0.55 | 0.0024 | 0.29 | 0.11–0.47 | 0.0019 |
| Univariable | Multivariable | |||||||
|---|---|---|---|---|---|---|---|---|
| Period | Variable | OR | 95% CI | p Value | Variable | OR | 95% CI | p Value |
| 1988–2002 | DM vs. without DM | 2.43 | 1.31–3.55 | 0.0012 | DM vs. without DM | 2.67 | 1.28–4.06 | 0.032 |
| 2003–2007 | DM vs. without DM | 4.32 | 1.91–6.73 | 0.0047 | DM vs. without DM | 3.44 | 1.79–5.09 | 0.028 |
| 2008–2012 | DM vs. without DM | 3.42 | 1.56–5.28 | 0.0058 | DM vs. without DM | 2.34 | 1.45–3.23 | 0.014 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, C.-J.; Chua, S.; Chung, S.-Y.; Hang, C.-L.; Tsai, T.-H. Diabetes Mellitus: An Independent Risk Factor of In-Hospital Mortality in Patients with Infective Endocarditis in a New Era of Clinical Practice. Int. J. Environ. Res. Public Health 2019, 16, 2248. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16122248
Lin C-J, Chua S, Chung S-Y, Hang C-L, Tsai T-H. Diabetes Mellitus: An Independent Risk Factor of In-Hospital Mortality in Patients with Infective Endocarditis in a New Era of Clinical Practice. International Journal of Environmental Research and Public Health. 2019; 16(12):2248. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16122248
Chicago/Turabian StyleLin, Cheng-Jei, Sarah Chua, Sheng-Ying Chung, Chi-Ling Hang, and Tzu-Hsien Tsai. 2019. "Diabetes Mellitus: An Independent Risk Factor of In-Hospital Mortality in Patients with Infective Endocarditis in a New Era of Clinical Practice" International Journal of Environmental Research and Public Health 16, no. 12: 2248. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16122248