Groundwater Chemistry and Blood Pressure: A Cross-Sectional Study in Bangladesh

 , ,
, ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Participants
2.2. Blood Pressure Measures
2.3. Clinical and Demographic Determinants of Blood Pressure
2.4. Participant Drinking Water Source Data
2.5. Hydro-Geological Data on Groundwater Chemistry
2.6. Selection of Chemicals for Analyses
2.7. Drinking Water Chemical Exposure Assignment
2.8. Statistical Analysis
2.9. Ethical Approval
3. Results
3.1. Characteristics of the Participants
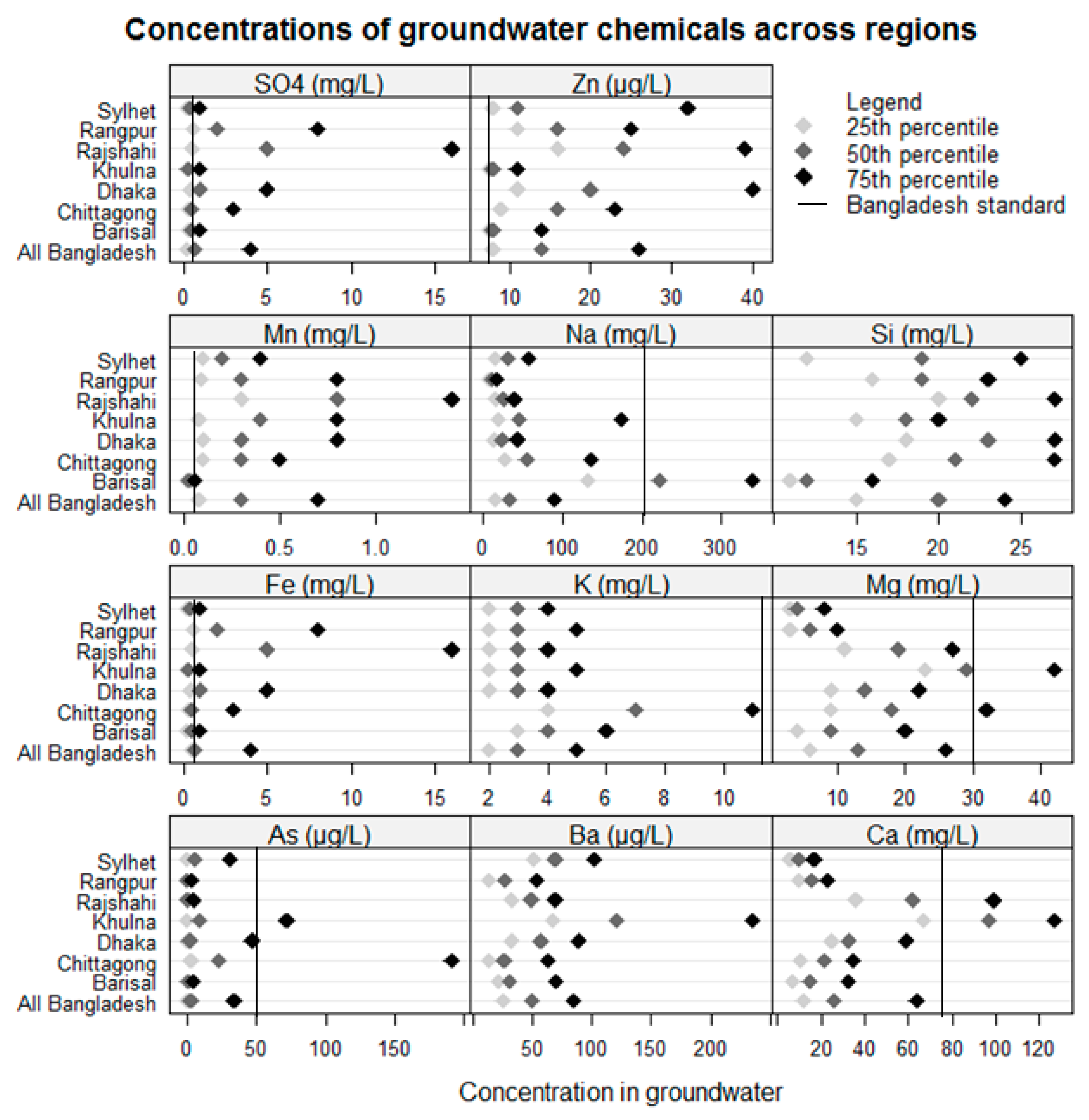
3.2. Distribution of Groundwater Chemicals
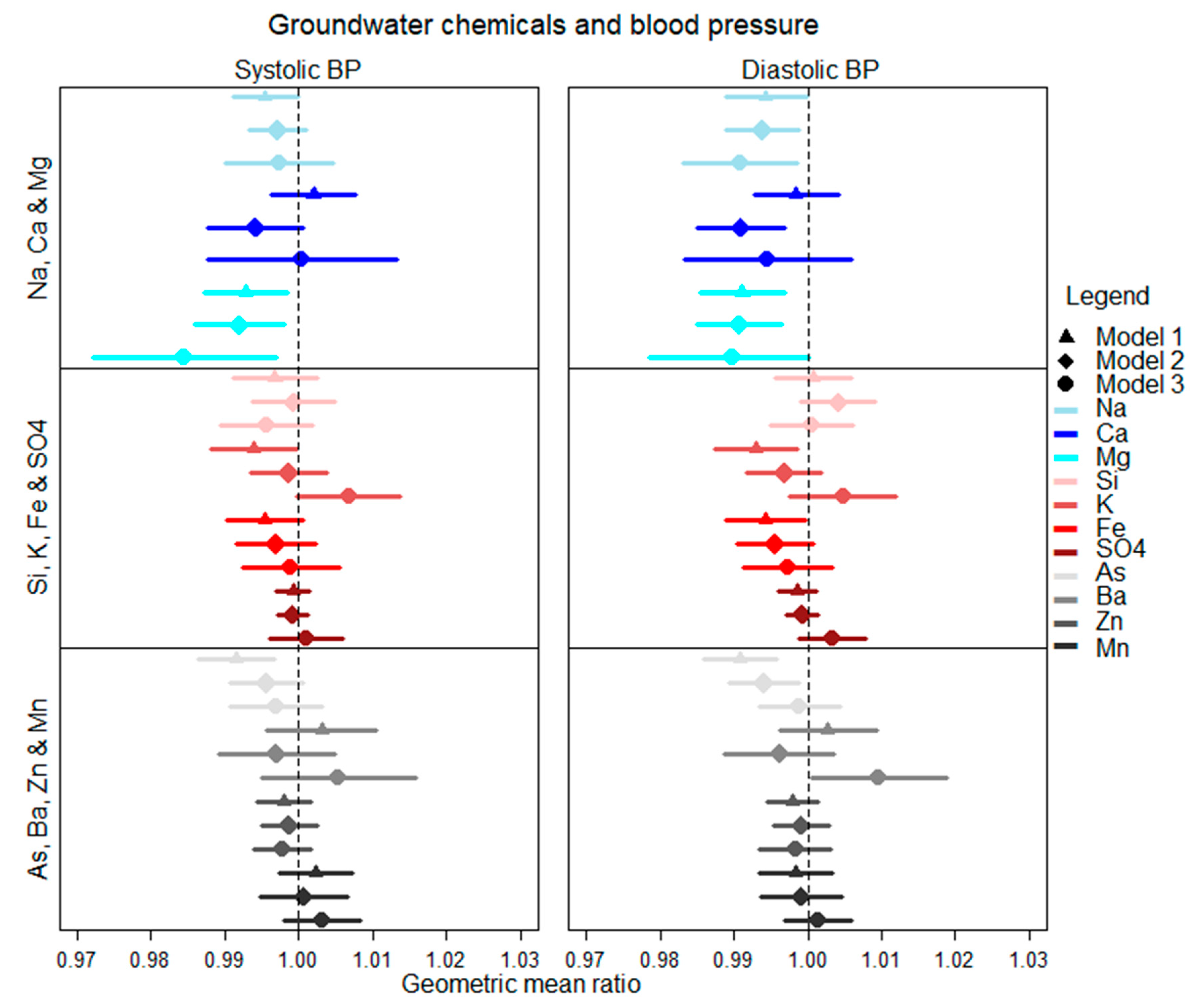
3.3. Association between Groundwater Chemicals and BP
3.4. Interaction between Chemical Pairs to Influence BP
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Marier, J. Geochemistry of Water in Relation to Cardiovascular Diseases: National Research Council; National Academy of Sciences: Washington, DC, USA, 1979. [Google Scholar]
- Lindh, U. Biological functions of the elements. In Essentials of Medical Geology; Springer: Berlin, Germany, 2013; pp. 129–177. [Google Scholar]
- Combs, G.F., Jr. Geological impacts on nutrition. In Essentials of Medical Geology; Springer: Berlin, Germany, 2013; pp. 179–194. [Google Scholar]
- McCarron, D.A.; Henry, H.J.; Morris, C.D. Human nutrition and blood pressure regulation: an integrated approach. Hypertension 1982, 4, III2. [Google Scholar]
- Kesteloot, H.; Joossens, J.V. Relationship of dietary sodium, potassium, calcium, and magnesium with blood pressure. Belg. Interuniv. Res. Nutr. Health Hypertens. 1988, 12, 594–599. [Google Scholar] [PubMed]
- British Geological Survey. Groundwater Quality: Bangladesh. 2001. Available online: https://www.bgs.ac.uk/downloads/start.cfm?id=1277 (accessed on 5 August 2017).
- France-Lanord, C.; Ananta, G.; Valier, G.; Jérôme, L.; Maarten, L.; Guillaume, M. Sediment Transfer and Deposition throughout the Himalayan Continental and Oceanic Basin: Constraint from Geochemical Composition of River Sediments. EGU General Assembly Conference Abstracts. 2013. Available online: http://meetingorganizer.copernicus.org/EGU2013/EGU2013-11545.pdf (accessed on 6 June 2019).
- Brammer, H. Geography of the Soils of Bangladesh; University Press: Dhaka, Bangladesh, 1996. [Google Scholar]
- BGS and DHPE. Arsenic Contamination of Groundwater in Bangladesh; IKinneburgh, D.G., Smedley, P.L., Eds.; Volume 1: Summary. British Geological Survey Report WC/00/19; British Geological Survey: Keyworth, UK, 2001; ISBN 0 85272 384 9. Available online: http://www.bgs.ac.uk/research/groundwater/health/arsenic/Bangladesh/reports.html (accessed on 20 August 2017).
- Ahsan, H.; Chen, Y.; Parvez, F.; Argos, M.; Hussain, A.I.; Momotaj, H.; Levy, D.; van Geen, A.; Howe, G.; Graziano, J. Health Effects of Arsenic Longitudinal Study (HEALS): Description of a multidisciplinary epidemiologic investigation. J Expo. Sci. Environ. Epidemiol. 2006, 16, 191–205. [Google Scholar] [CrossRef] [PubMed]
- Jiang, J.; Liu, M.; Parvez, F.; Wang, B.; Wu, F.; Eunus, M.; Bangalore, S.; Newman, J.D.; Ahmed, A.; Islam, T.; et al. Association between arsenic exposure from drinking water and longitudinal change in blood pressure among HEALS cohort participants. Environ. Health Perspect. 2015, 123, 806. [Google Scholar] [CrossRef] [PubMed]
- Scheelbeek, P.F.D.; Chowdhury, M.A.H.; Haines, A.; Alam, A.; Hoque, M.A.; Butler, A.P.; Khan, A.E.; Mojumder, S.K.; Blangiardo, M.A.G.; Elliott, P.; et al. High concentrations of sodium in drinking water and raised blood pressure in coastal deltas affected by episodic seawater inundations. Lancet Glob. Health 2016, 4, S18. [Google Scholar] [CrossRef] [Green Version]
- National Institute of Population Research and Training. Bangladesh Demographic and Health Survey; National Institute of Population Research and Training: Dhaka, Bangladesh, 2011.
- Madison, J.R.; Spies, C.; Schatz, I.J.; Masaki, K.; Chen, R.; Yano, K.; Curb, J.D. Proteinuria and risk for stroke and coronary heart disease during 27 years of follow-up: the Honolulu Heart Program. Arch. Intern. Med. 2006, 166, 884–889. [Google Scholar] [CrossRef] [PubMed]
- BGS and DHPE. Arsenic Contamination of Groundwater in Bangladesh; IKinneburgh, D.G., Smedley, P.L., Eds.; Volume 2: Final Report. Chapter 1: Introduction. British Geological Survey Report WC/00/19; British Geological Survey: Keyworth, UK, 2001; ISBN 0 85272 384 9. Available online: https://www.bgs.ac.uk/research/groundwater/health/arsenic/Bangladesh/reports.html (accessed on 26 June 2019).
- BGS and DHPE. Arsenic Contamination of Groundwater in Bangladesh; IKinneburgh, D.G., Smedley, P.L., Eds.; Volume 3: Hydrochemical Atlas. Chapter 1: The National Hydrochemical Survey. British Geological Survey Report WC/00/19; British Geological Survey: Keyworth, UK, 2001; ISBN 0 85272 384 9. Available online: https://www.bgs.ac.uk/research/groundwater/health/arsenic/Bangladesh/reports.html (accessed on 26 June 2019).
- BGS and DHPE. Arsenic Contamination of Groundwater in Bangladesh; IKinneburgh, D.G., Smedley, P.L., Eds.; Volume 2: Final Report. Chapter 6: The National Hydrochemical Survey. British Geological Survey Report WC/00/19; British Geological Survey: Keyworth, UK, 2001; ISBN 0 85272 384 9. Available online: https://www.bgs.ac.uk/research/groundwater/health/arsenic/Bangladesh/reports.html (accessed on 26 June 2019).
- Ourshalimian, S.; Naser, A.M.; Rahman, M.; Doza, S.; Stowell, J.; Narayan, K.M.V.; Shamsudduha, M.; Gribble, M.O. Arsenic and Fasting Blood Glucose in the Context of Other Drinking Water Chemicals: A Cross-Sectional Study in Bangladesh. Environ. Res. 2019, 172, 249–257. [Google Scholar]
- Shrivastava, A.; Gupta, V.B. Methods for the determination of limit of detection and limit of quantitation of the analytical methods. Chron. Young Sci. 2011, 2, 21. [Google Scholar] [CrossRef]
- Nickson, R.; McArthur, J.; Burgess, W.; Ahmed, K.M.; Ravenscroft, P.; Rahman, M. Arsenic poisoning of Bangladesh groundwater. Nature 1998, 395, 338. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Stute, M.; van Geen, A.; Gavrieli, I.; Dhar, R.; Simpson, H.J.; Schlosser, P.; Ahmed, K.M. Redox control of arsenic mobilization in Bangladesh groundwater. Appl. Geochem. 2004, 19, 201–214. [Google Scholar] [CrossRef]
- Azur, M.J.; Stuart, E.; Frangakis, C.; Leaf, P. Multiple imputation by chained equations: What is it and how does it work? Int. J. Methods Psychiatr. Res. 2011, 20, 40–49. [Google Scholar] [CrossRef]
- Paisley, K.E.; Beaman, M.; Tooke, J.E.; Mohamed-Ali, V.; Lowe, G.D.; Shore, A.C. Endothelial dysfunction and inflammation in asymptomatic proteinuria. Kidney Int. 2003, 63, 624–633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Guidelines for Drinking-water Quality: Fourth Edition. 2011. [cited 38; 104-8]. Available online: https://www.unicef.org/cholera/Chapter_4_prevention/01_WHO_Guidelines_for_drinking_water_quality.pdf (accessed on 26 June 2019).
- Jee, S.H.; Miller, E.R., 3rd; Guallar, E.; Singh, V.K.; Appel, L.J.; Klag, M.J. The effect of magnesium supplementation on blood pressure: a meta-analysis of randomized clinical trials. Am. J. Hypertens. 2002, 15, 691–696. [Google Scholar] [CrossRef] [Green Version]
- van Leer, E.M.; Seidell, J.C.; Kromhout, D. Dietary calcium, potassium, magnesium and blood pressure in the Netherlands. Int. J. Epidemiol. 1995, 24, 1117–1123. [Google Scholar] [CrossRef] [PubMed]
- Catling, L.A.; Abubakar, I.; Lake, I.R.; Swift, L.; Hunter, P.R. A systematic review of analytical observational studies investigating the association between cardiovascular disease and drinking water hardness. J. Water Health 2008, 6, 433–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shlezinger, M.; Amitai, Y.; Goldenberg, I.; Shechter, M. Desalinated seawater supply and all-cause mortality in hospitalized acute myocardial infarction patients from the Acute Coronary Syndrome Israeli Survey 2002–2013. Int. J. Cardiol. 2016, 220, 544–550. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Factor-Litvak, P.; Howe, G.R.; Parvez, F.; Ahsan, H. Nutritional influence on risk of high blood pressure in Bangladesh: A population-based cross-sectional study. Am. J. Clin. Nutr. 2006, 84, 1224–1232. [Google Scholar] [CrossRef] [PubMed]
- Hoque, M.A.; Butler, A.P. Medical hydrogeology of Asian deltas: status of groundwater toxicants and nutrients, and implications for human health. Int. J. Environ. Res. Public Health 2015, 13, 81. [Google Scholar] [CrossRef] [PubMed]
- Naser, A.M.; Rahman, M.; Unicomb, L.; Doza, S.; Gazi, M.S.; Alam, G.R.; Karim, M.R.; Uddin, M.N.; Khan, G.K.; Ahmed, K.M. Drinking water salinity, urinary macro-mineral excretions, and blood pressure in the southwest coastal population of Bangladesh. J. Am. Heart Assoc. 2019, 8, e012007. [Google Scholar] [CrossRef]
- World Health Organization. Calcium and Magnesium in Drinking-Water: Public Health Significance; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Dhar, R.K.; Zheng, Y.; Stute, M.; van Geen, A.; Cheng, Z.; Shanewaz, M.; Shamsudduha, M.; Hoque, M.A.; Rahman, M.W.; Ahmed, K.M. Temporal variability of groundwater chemistry in shallow and deep aquifers of Araihazar, Bangladesh. J. Contam. Hydrol. 2008, 99, 97–111. [Google Scholar] [CrossRef] [Green Version]
- Deng, Y.; Li, H.; Wang, Y.; Duan, Y.; Gan, Y. Temporal variability of groundwater chemistry and relationship with water-table fluctuation in the Jianghan Plain, central China. Procedia Earth Planet. Sci. 2014, 10, 100–103. [Google Scholar] [CrossRef]
- Burgess, W.G.; Hoque, M.A.; Michael, H.A.; Voss, C.I.; Breit, G.N.; Ahmed, K.M. Vulnerability of deep groundwater in the Bengal Aquifer System to contamination by arsenic. Nat. Geosci. 2010, 3, 83. [Google Scholar] [CrossRef]
- van Geen, A.; Zheng, Y.; Versteeg, R.; Stute, M.; Horneman, A.; Dhar, R.; Steckler, M.; Gelman, A.; Small, C.; Ahsan, H.; et al. Spatial variability of arsenic in 6000 tube wells in a 25 km2 area of Bangladesh. Water Resour. Res. 2003, 39. [Google Scholar] [CrossRef]
- Merrill, R.D.; Labrique, A.B.; Shamim, A.A.; Schulze, K.; Christian, P.; Merrill, R.K.; West, K.P., Jr. Elevated and variable groundwater iron in rural northwestern Bangladesh. J. Water Health 2010, 8, 818–825. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naser, A.M.; Higgins, E.M.; Arman, S.; Ercumen, A.; Ashraf, S.; Das, K.K.; Rahman, M.; Luby, S.P.; Unicomb, L. Effect of Groundwater Iron on Residual Chlorine in Water Treated with Sodium Dichloroisocyanurate Tablets in Rural Bangladesh. Am. J. Trop. Med. Hyg. 2018, 98, 977–983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wood, M.E.; Chrysanthopoulou, S.; Nordeng, H.M.E.; Lapane, K.L. The Impact of Nondifferential Exposure Misclassification on the Performance of Propensity Scores for Continuous and Binary Outcomes. Med. Care 2018, 56, e46–e53. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participants’ Characteristics | All Participants with Blood Pressure Measurement (N = 7887) | Groundwater Drinkers with Blood Pressure Measurement (N = 6875) | Participants Eligible for Blood Pressure Measurement (N = 7992) |
|---|---|---|---|
| Age, mean (95% Confidence Interval) | 51.4 (51.1, 51.7) | 51.7 (51.4, 52.1) | 51.5 (51.1, 51.8) |
| BMI (kg/m2), mean (95% CI) | 20.9 (20.7, 21.0) | 20.6 (20.4, 20.7) | 20.9 (20.7, 21.0) |
| BMI categories, % | |||
| Underweight (<18.5 kg/m2) | 29.1 (27.7, 30.6) | 31.1 (29.6, 32.6) | 29.1 (27.7, 30.6) |
| Normal weight (≥18.5 to <25 kg/m2) | 57.4 (56.0, 58.8) | 57.3 (55.9, 58.9) | 57.4 (56.0, 58.8) |
| Overweight (≥25 to <30 kg/m2) | 11.3 (10.5, 12.3) | 9.9 (9.0, 10.9) | 11.4 (10.5, 12.3) |
| Obese (≥30 kg/m2) | 2.1 (1.8, 2.5) | 1.7 (13.7, 2.1) | 2.1 (1.8, 2.5) |
| Years of education, mean (95% CI) | 3.3 (3.3, 3.5) | 3.1 (2.9, 3.2) | 3.4 (3.2, 3.6) |
| Education categories, % (95% CI) | |||
| No institutional education | 49.6 (47.7, 51.4) | 52.0 (50.0, 53.9) | 49.6 (47.7, 51.4) |
| Primary level (≤5 years) | 25.8 (24.4, 27.1) | 25.9 (24.5, 27.3) | 25.8 (24.4, 27.1) |
| Secondary level (6 to ≤10 years) | 17.5 (16.3, 18.7) | 16.7 (15.5, 17.9) | 17.5 (16.3, 18.7) |
| College level or higher (≥11 years) | 6.9 (6.0, 7.9) | 5.5 (4.7, 6.3) | 7.2 (6.2, 8.3) |
| Male sex, % (95% CI) | 49.4 (48.6, 50.2) | 49.4 (48.5, 50.3) | 49.5 (48.7, 50.2) |
| Female sex, % (95% CI) | 50.6 (49.8, 51.3) | 50.6 (49.7, 51.5) | 50.5 (49.7, 51.3) |
| Current Smoker, % (95% CI) | 13.6 (12.2, 15.1) | 13.8 (12.3, 15.3) | 13.6 (12.2, 15.1) |
| Household characteristics | |||
| Urban residence, % (95% CI) | 23.3 (22.2, 24.4) | 16.5 (15.0, 18.1) | 23.8 (22.8, 25.0) |
| Wealth index, (95% CI) | |||
| Quintile 1 | 19.4 (17.7, 21.3) | 20.8 (18.9, 22.8) | 19.3 (17.5, 21.1) |
| Quintile 2 | 19.2 (17.8, 20.7) | 21.1 (19.6, 22.8) | 19.1 (17.7, 20.6) |
| Quintile 3 | 19.8 (18.3, 12.4) | 21.5 (19.9, 23.2) | 19.8 (18.2, 21.3) |
| Quintile 4 | 20.7 (19.1, 22.3) | 21.4 (19.8, 23.2) | 20.6 (19.0, 22.2) |
| Quintile 5 | 20.9 (19.2, 22.7) | 15.1 (13.5, 16.9) | 21.3 (19.6, 23.2) |
| Cluster characteristics | % (n/N) | ||
| Distance of nearest well in kilometers, mean (95% CI) | 3.2 (2.8, 3.7) | 3.3 (2.9, 3.8) | 3.2 (2.8, 3.7) |
| Divisional distribution, % (95% CI) | |||
| Dhaka | 32.1 (30.9, 33.3) | 29.0 (27.3, 30.7) | 32.3 (31.1, 33.6) |
| Barisal | 5.9 (5.5, 6.4) | 6.3 (5.8, 6.9) | 5.9 (5.5, 6.4) |
| Chittagong | 17.0 (16.1, 17.9) | 17.6 (16.6, 18.6) | 16.9 (16.0, 17.8) |
| Khulna | 13.0 (12.3, 13.8) | 12.9 (11.9, 14.0) | 12.9 (12.2, 13.7) |
| Rajshahi | 14.5 (13.6, 15.4) | 15.5 (14.5, 16.6) | 14.6 (13.7, 15.5) |
| Rangpur | 11.7 (11.1, 12.4) | 12.9 (12.2, 13.7) | 11.7 (11.1, 12.3) |
| Sylhet | 5.7 (5.3, 6.1) | 5.8 (5.3, 6.3) | 5.8 (5.4, 6.2) |
| Chemicals | 25th Percentile | 75th Percentile | Predicted Change in BP | |
|---|---|---|---|---|
| SBP (95% CI) | DBP (95% CI) | |||
| Na (mg/L) | 15 | 91 | −0.15 (−0.06, −0.25) | −0.34 (−0.25, −0.43) |
| Ca (mg/L) | 13 | 71 | 0.06 (0.01, 0.11) | −0.56 (−0.66, −0.45) |
| Mg (mg/L) | 7 | 27 | −1.96 (−1.68, −2.25) | −0.84 (−1.01, −0.67) |
| K (mg/L) | 2 | 5 | 0.47 (0.47, 0.48) | 0.22 (0.22, 0.23) |
| Fe (mg/L) | 0.12 | 4.28 | −0.14 (−0.06, −0.21) | −0.22 (−0.12, −0.32) |
| Si (mg/L) | 15 | 24 | −0.77 (−0.97, −0.77) | 0.06 (−0.09, 0.22) |
| S04 (mg/L) | 0.2 | 3.7 | 0.01 (0.00, 0.02) | 0.02 (0.02, 0.02) |
| As (μg/L) | 0.5 | 39 | −0.13 (−0.12, −0.15) | −0.03 (−0.04, −0.02) |
| Ba (μg/L) | 26 | 88 | 0.38 (0.37, 0.39) | 0.45 (0.45, 0.45) |
| Zn (μg/L) | 8 | 25 | −0.03 (−0.04, −0.03) | −0.02 (−0.02, −0.010 |
| Mn (μg/L) | 76 | 735 | 0.29 (0.26, 0.31) | 0.09 (0.07, 0.10) |
| Chemical Pairs | p Values | Chemical Pairs | p Values | ||
|---|---|---|---|---|---|
| Systolic BP | Diastolic BP | Systolic BP | Diastolic BP | ||
| Mg & Ca | 0.318 | 0.185 | Na & Si | 0.307 | 0.900 |
| Mg & Na | 0.854 | 0.307 | Na & Mn | 0.217 | 0.827 |
| Mg & K | 0.811 | 0.386 | Na & Zn | 0.772 | 0.566 |
| Mg & As | 0.593 | 0.421 | Na & Fe | 0.089 | 0.045 |
| Mg & Si | 0.308 | 0.796 | Na & SO4 | 0.012 | 0.591 |
| Mg & Ba | 0.668 | 0.102 | Na & Ba | 0.393 | 0.024 |
| Mg & Zn | 0.684 | 0.583 | Na & Ca | 0.503 | 0.254 |
| Mg & Fe | 0.820 | 0.109 | Na & Mg | 0.938 | 0.958 |
| Mg & SO4 | 0.231 | 0.034 | Na & K | 0.814 | 0.811 |
| Mg & Mn | 0.755 | 0.782 | Na & As | 0.188 | 0.014 |
| Ca & Si | 0.250 | 0.750 | K & Si | 0.440 | 0.529 |
| Ca & Mn | 0.537 | 0.368 | K & Mn | 0.254 | 0.340 |
| Ca & Zn | 0.198 | 0.225 | K & Zn | 0.899 | 0.423 |
| Ca & Fe | 0.678 | 0.058 | K & Fe | 0.499 | 0.304 |
| Ca & SO4 | 0.279 | 0.073 | K & SO4 | 0.849 | 0.277 |
| Ca & Ba | 0.121 | 0.003 | K & Ba | 0.750 | 0.083 |
| Ca & Mg | 0.013 | 0.026 | K & Ca | 0.258 | 0.007 |
| Ca & Na | 0.604 | 0.670 | K & Mg | 0.452 | 0.582 |
| Ca & K | 0.641 | 0.417 | Na & K | 0.295 | 0.987 |
| Ca & As | 0.819 | 0.917 | K & As | 0.819 | 0.953 |
| As & Si | 0.012 | 0.184 | As & Ba | 0.991 | 0.430 |
| As & Mn | 0.672 | 0.285 | As & Ca | 0.710 | 0.294 |
| As & Zn | 0.568 | 0.890 | As & Mg | 0.361 | 0.801 |
| As & Fe | 0.387 | 0.911 | As & K | 0.564 | 0.266 |
| As & SO4 | 0.763 | 0.348 | AS & Na | 0.113 | 0.199 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Naser, A.M.; Clasen, T.F.; Luby, S.P.; Rahman, M.; Unicomb, L.; Ahmed, K.M.; Doza, S.; Ourshalimian, S.; Chang, H.H.; Stowell, J.D.; et al. Groundwater Chemistry and Blood Pressure: A Cross-Sectional Study in Bangladesh. Int. J. Environ. Res. Public Health 2019, 16, 2289. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16132289
Naser AM, Clasen TF, Luby SP, Rahman M, Unicomb L, Ahmed KM, Doza S, Ourshalimian S, Chang HH, Stowell JD, et al. Groundwater Chemistry and Blood Pressure: A Cross-Sectional Study in Bangladesh. International Journal of Environmental Research and Public Health. 2019; 16(13):2289. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16132289
Chicago/Turabian StyleNaser, Abu Mohd, Thomas F. Clasen, Stephen P. Luby, Mahbubur Rahman, Leanne Unicomb, Kazi M. Ahmed, Solaiman Doza, Shadassa Ourshalimian, Howard H. Chang, Jennifer D. Stowell, and et al. 2019. "Groundwater Chemistry and Blood Pressure: A Cross-Sectional Study in Bangladesh" International Journal of Environmental Research and Public Health 16, no. 13: 2289. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16132289