Mental Health of Refugees and Torture Survivors: A Critical Review of Prevalence, Predictors, and Integrated Care


Abstract
:1. Introduction
“any act by which severe pain or suffering, whether physical or mental, is intentionally inflicted on a person for such purposes as obtaining from him or a third person information or a confession, punishing him for an act he or a third person has committed or is suspected of having committed, or intimidating or coercing him or a third person, or for any reason based on discrimination of any kind.”(United Nations Convention against Torture and Other Cruel UNCAT article)
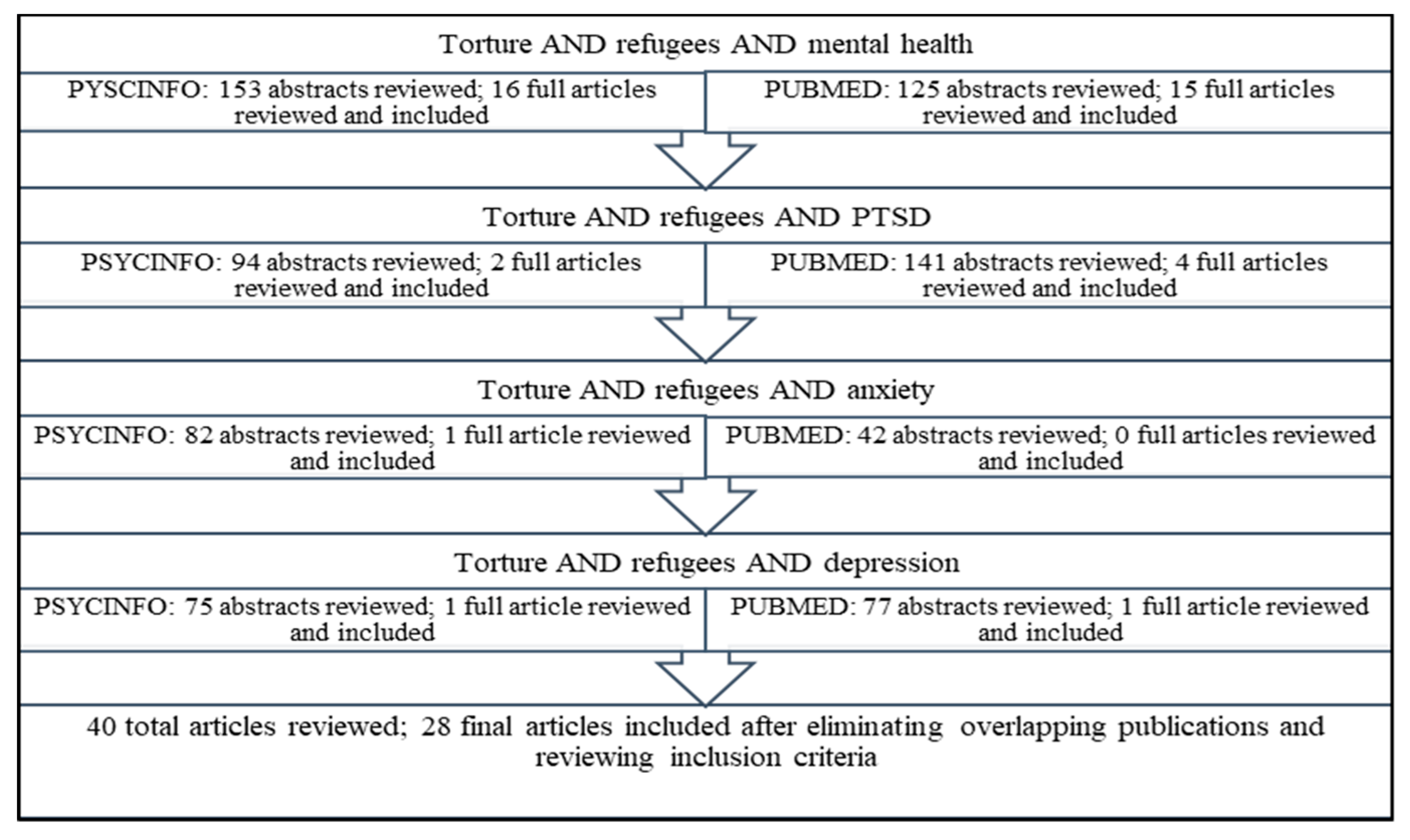
2. Method
3. Results
3.1. Demographics and Characteristics of Survivors of Torture
3.2. Prevalence of Mental Health Conditions in Refugees and Torture Survivors:
3.3. Predictors of Risk and Resilience
3.4. Integrated Care
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Kessler, R.C.; Ustun, T.B. The WHO Mental Health Surveys. Global Perspectives on the Epidemiology of Mental Disorders; Cambridge University Press: Cambridge, UK; New York, NY, USA, 2008. [Google Scholar]
- United Nations Convention Against Torture, Article 1.1. Available online: http://www.unhcr.org/protection/migration/49e479d10/convention-against-torture-other-cruel-inhuman-degrading-treatment-punishment.html (accessed on 21 June 2019).
- Dahl, S.; Mutapcic, A.; Schei, B. Traumatic events and predictive factors for posttraumatic symptoms in displaced Bosnian women in a war zone. J. Trauma. Stress 1998, 11, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Steel, Z.; Chey, T.; Silove, D.; Marnane, C.; Bryant, R.A.; Van Ommeren, M. Association of torture and other potentially traumatic events with mental health outcomes among populations exposed to mass conflict and displacement: A systematic review and meta-analysis. JAMA 2009, 302, 537–549. [Google Scholar] [CrossRef] [PubMed]
- Campbell, T.A. Psychological assessment, diagnosis, and treatment of torture survivors: A review. Clin. Psychol. Rev. 2007, 27, 628–641. [Google Scholar] [CrossRef] [PubMed]
- Dgani-Ratsaby, A. The Effects of Cultural and Familial Factors on Severity of Trauma and Treatment Outcome among a Multicultural Population of Refugee Survivors of Torture. Ph.D. Thesis, Adelphi University, Garden City, NY, USA, 2011. [Google Scholar]
- Willard, C.L.; Rabin, M.; Lawless, M. The prevalence of torture and associated symptoms in United States Iraqi refugees. J. Immigr. Minor. Health 2014, 16, 1069–1076. [Google Scholar] [CrossRef]
- Breslau, N. Epidemiologic studies of trauma, posttraumatic stress disorder, and other psychiatric disorders. Can. J. Psychiatry 2002, 47, 923–929. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Sonnega, A.; Bromet, E.; Hughes, M.; Nelson, C.B. Posttraumatic stress disorder in the National Comorbidity Survey. Arch. Gen. Psychiatry 1995, 52, 1048–1060. [Google Scholar] [CrossRef] [PubMed]
- Weiss, D.S.; Marmar, C.R.; Schlenger, W.E.; Fairbank, J.A.; Kathleen Jordan, B.; Hough, R.L.; Kulka, R.A. The prevalence of lifetime and partial post-traumatic stress disorder in Vietnam theater veterans. J. Trauma. Stress 1992, 5, 365–376. [Google Scholar] [CrossRef]
- Integrated Care. February 2017. Available online: https://www.nimh.nih.gov/health/topics/integrated-care/index.shtml (accessed on 13 February 2019).
- Bandeira, M.; Higson-Smith, C.; Bantjes, M.; Polatin, P. The land of milk and honey: A picture of refugee torture survivors presenting for treatment in a South African trauma centre. Torture J. 2010, 20, 92–103. [Google Scholar]
- Berthold, S.M.; Kong, S.; Mollica, R.F.; Kuoch, T.; Scully, M.; Franke, T. Comorbid mental and physical health and health access in Cambodian refugees in the US. J. Community Health 2014, 39, 1045–1052. [Google Scholar] [CrossRef]
- Tamblyn, J.M.; Calderon, A.J.; Combs, S.; O’Brien, M.M. Patients from abroad becoming patients in everyday practice: Torture survivors in primary care. J. Immigr. Minor. Health 2011, 13, 798–801. [Google Scholar] [CrossRef]
- Shannon, P.J.; Vinson, G.A.; Wieling, E.; Cook, T.; Letts, J. Torture, war trauma, and mental health symptoms of newly arrived Karen refugees. J. Loss Trauma 2015, 20, 577–590. [Google Scholar] [CrossRef]
- Odenat, L. ‘Means of Survival’as Moderator of the Relationship between Cumulative Torture Experiences and Posttraumatic Stress Disorder among Refugees. Ph.D. Thesis, Georgia State University, Atlanta, GA, USA, 2012. [Google Scholar]
- Ibrahim, H.; Hassan, C.Q. Post-traumatic stress disorder symptoms resulting from torture and other traumatic events among Syrian Kurdish refugees in Kurdistan Region, Iraq. Front. Psychol. 2017, 8, 241. [Google Scholar] [CrossRef] [PubMed]
- Leaman, S.C.; Gee, C.B. Religious coping and risk factors for psychological distress among African torture survivors. Psychol. Trauma Theory Res. Pract. Policy 2012, 4, 457–465. [Google Scholar] [CrossRef]
- McColl, H.; Higson-Smith, C.; Gjerding, S.; Omar, M.H.; Rahman, B.A.; Hamed, M.; El Dawla, A.S.; Fredericks, M.; Paulsen, N.; Shabalala, G.; et al. Rehabilitation of torture survivors in five countries: Common themes and challenges. Int. J. Ment. Health Syst. 2010, 4, 16. [Google Scholar] [CrossRef] [PubMed]
- Luitel, N.P.; Jordans, M.J.; Sapkota, R.P.; Tol, W.A.; Kohrt, B.A.; Thapa, S.B.; Komproe, I.H.; Sharma, B. Conflict and mental health: A cross-sectional epidemiological study in Nepal. Soc. Psychiatry Psychiatr. Epidemiol. 2013, 48, 183–193. [Google Scholar] [CrossRef] [PubMed]
- Schubert, C.C.; Punamäki, R.L. Mental health among torture survivors: Cultural background, refugee status and gender. Nord. J. Psychiatry 2011, 65, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Le, L.; Morina, N.; Schnyder, U.; Schick, M.; Bryant, R.A.; Nickerson, A. The effects of perceived torture controllability on symptom severity of posttraumatic stress, depression and anger in refugees and asylum seekers: A path analysis. Psychiatry Res. 2018, 264, 143–150. [Google Scholar] [CrossRef]
- Morina, N.; Schnyder, U.; Schick, M.; Nickerson, A.; Bryant, R.A. Attachment style and interpersonal trauma in refugees. Aust. N. Z. J. Psychiatry 2016, 50, 1161–1168. [Google Scholar] [CrossRef]
- Tinghög, P.; Malm, A.; Arwidson, C.; Sigvardsdotter, E.; Lundin, A.; Saboonchi, F. Prevalence of mental ill health, traumas and postmigration stress among refugees from Syria resettled in Sweden after 2011: A population-based survey. BMJ Open 2017, 7, e018899. [Google Scholar] [CrossRef]
- NCTTP (Member Centers of the National Consortium of Torture Treatment Programs). Descriptive, Inferential, Functional Outcome Data on 9,025 Torture Survivors Over Six Years in the United States. Torture 2015, 25, 34–60. [Google Scholar]
- Song, S.J.; Subica, A.; Kaplan, C.; Tol, W.; De Jong, J. Predicting the mental health and functioning of torture survivors. J. Nerv. Ment. Dis. 2018, 206, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Robertson, C.L.; Savik, K.; Mathiason-Moore, M.; Mohamed, A.; Hoffman, S. Modeling psychological functioning in refugees. J. Am. Psychiatr. Nurses Assoc. 2016, 22, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Asgary, R.; Charpentier, B.; Burnett, D.C. Socio-medical challenges of asylum seekers prior and after coming to the US. J. Immigr. Minor. Health 2013, 15, 961–968. [Google Scholar] [CrossRef] [PubMed]
- Chu, T.; Keller, A.S.; Rasmussen, A. Effects of post-migration factors on PTSD outcomes among immigrant survivors of political violence. J. Immigr. Minor. Health 2013, 15, 890–897. [Google Scholar] [CrossRef] [PubMed]
- Raghavan, S.; Rasmussen, A.; Rosenfeld, B.; Keller, A.S. Correlates of symptom reduction in treatment-seeking survivors of torture. Psychol. Trauma Theory Res. Pract. Policy 2013, 5, 377. [Google Scholar] [CrossRef]
- Hoffman, S.J.; Robertson, C.L.; Shannon, P.J.; Cook, T.L.; Letts, J.; Mathiason, M.A. Physical correlates of torture exposure in Karen refugees. J. Loss Trauma 2017, 22, 135–149. [Google Scholar] [CrossRef]
- Carlsson, J.M.; Olsen, D.R.; Kastrup, M.; Mortensen, E.L. Late mental health changes in tortured refugees in multidisciplinary treatment. J. Nerv. Ment. Dis. 2010, 198, 824–828. [Google Scholar] [CrossRef] [PubMed]
- Hooberman, J.; Rosenfeld, B.; Rasmussen, A.; Keller, A. Resilience in trauma-exposed refugees: The moderating effect of coping style on resilience variables. Am. J. Orthopsychiatry 2010, 80, 557–563. [Google Scholar] [CrossRef]
- Kroo, A.; Nagy, H. Posttraumatic growth among traumatized Somali refugees in Hungary. J. Loss Trauma 2011, 16, 440–458. [Google Scholar] [CrossRef]
- Keatley, E.; D’Alfonso, A.; Abeare, C.; Keller, A.; Bertelsen, N.S. Health outcomes of traumatic brain injury among refugee survivors of torture. J. Head Trauma Rehabil. 2015, 30, E1–E8. [Google Scholar] [CrossRef]
- Tufan, A.E.; Alkin, M.; Bosgelmez, S. Post-traumatic stress disorder among asylum seekers and refugees in Istanbul may be predicted by torture and loss due to violence. Nord. J. Psychiatry 2013, 67, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Song, S.J.; Kaplan, C.; Tol, W.A.; Subica, A.; De Jong, J. Psychological distress in torture survivors: Pre-and post-migration risk factors in a US sample. Soc. Psychiatry Psychiatr. Epidemiol. 2015, 50, 549–560. [Google Scholar] [CrossRef] [PubMed]
- Nickerson, A.; Schick, M.; Schnyder, U.; Bryant, R.A.; Morina, N. Comorbidity of Posttraumatic Stress Disorder and Depression in Tortured, Treatment-Seeking Refugees. J. Trauma. Stress 2017, 30, 409–415. [Google Scholar] [CrossRef] [PubMed]
- Esala, J.J.; Vukovich, M.M.; Hanbury, A.; Kashyap, S.; Joscelyne, A. Collaborative care for refugees and torture survivors: Key findings from the literature. Traumatology 2018, 24, 168–185. [Google Scholar] [CrossRef]
- Carlsson, J.M.; Mortensen, E.L.; Kastrup, M. Predictors of mental health and quality of life in male tortured refugees. Nord. J. Psychiatry 2006, 60, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Foa, E.B.; Rothbaum, B.O.; Molnar, C. Cognitive-behavioral therapy of PTSD. In Neurobiological and Clinical Consequences of Stress: From Normal Adaptation to PTSD; Lippincott Williams & Wilkins Publishers: Philadelphia, PA, USA, 1995; pp. 483–494. [Google Scholar]
- Greenberg, P.E.; Leong, S.A.; Birnbaum, H.G.; Robinson, R.L. The economic burden of depression with painful symptoms. J. Clin. Psychiatry 2003, 64, 17–23. [Google Scholar] [PubMed]
- CDC—Medical Examination—Immigrant and Refugee Health. 29 March 2012. Available online: https://www.cdc.gov/immigrantrefugeehealth/exams/medical-examination.html (accessed on 13 February 2019).
- Javanbakht, A.; Amirsadri, A.; Suhaiban, H.A.; Alsaud, M.I.; Alobaidi, Z.; Rawi, Z.; Arfken, C.L. Prevalence of possible mental disorders in syrian refugees resettling in the united states screened at primary care. J. Immigr. Minor. Health 2018, 21, 664–667. [Google Scholar] [CrossRef] [PubMed]
- Javanbakht, A.; Rosenberg, D.; Haddad, L.; Arfken, C.L. Mental health in Syrian refugee children resettling in the United States: War trauma, migration, and the role of parental stress. J. Am. Acad. Child Adolesc. Psychiatry 2018, 57, 209–211. [Google Scholar] [CrossRef] [PubMed]
- Shannon, P.J.; Wieling, E.; McCleary, J.S.; Becher, E. Exploring the mental health effects of political trauma with newly arrived refugees. Qual. Health Res. 2015, 25, 443–457. [Google Scholar] [CrossRef] [PubMed]
- Marshall, G.N.; Schell, T.L.; Miles, J.N. Ethnic differences in posttraumatic distress: Hispanics’ symptoms differ in kind and degree. J. Consult. Clin. Psychol. 2009, 77, 1169–1178. [Google Scholar] [CrossRef] [PubMed]
- Bisson, J.I.; Roberts, N.P.; Andrew, M.; Cooper, R.; Lewis, C. Psychological therapies for chronic post-traumatic stress disorder (PTSD) in adults. Cochrane Database Syst. Rev. 2013, 12, CD003388. [Google Scholar] [CrossRef] [PubMed]
- Monson, C.M.; Macdonald, A.; Vorstenbosch, V.; Shnaider, P.; Goldstein, E.S.; Ferrier-Auerbach, A.G.; Mocciola, K.E. Changes in social adjustment with cognitive processing therapy: Effects of treatment and association with PTSD symptom change. J. Trauma. Stress 2012, 25, 519–526. [Google Scholar] [CrossRef] [PubMed]
- Grasser, L.R.; Javanbakht, A. Treatments of Posttraumatic Stress Disorder in Civilian Populations. Curr. Psychiatry Rep. 2019, 21, 11. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study | Sample | Age (Mean) | Gender (Male) | Status (Married) | Education | Religion |
|---|---|---|---|---|---|---|
| Shannon et al. (2016) [16] | 179 Karen refugees | 35.27 | 51.4% | 62.6% | 35.8% completed primary school | - |
| Odenat (2012) [17] | 326 adult refugee torture survivors | 38.55 | 57% | 65% | 40% completed primary school | - |
| Ibrahim and Hassan (2017) [18] | 91 Syrian Kurdish refugees | 29.91 | 55% | 60.4% | 5.5% had no formal education | - |
| Leaman and Gee (2012) [19] | 131 African torture survivors | 34.12 | 42% | 47.3% | 77.1% completed at least high school | Christians 92.4% Muslims 4.6% |
| McColl et al. (2010) [20] | 306 torture survivors from Gaza, Egypt, Mexico, Honduras, South Africa | 37.7 | 56% | 42% | 30% completed secondary education. | Christians 55% Muslims 38% |
| Luitel et al. (2013) [21] | 720 torture survivors | 29.2% ≥ 45 years | 51.0% | 74.9% | 79.2% literate | - |
| Schubert and Punamäki (2011) [22] | 78 torture survivors from Middle East (ME), Central Africa (CA), South Asia (SA), Southeast Europe (SE) | 37.60 | 62.8% | ME: 58.1% CA: 47.8% SA: 69.2% SE: 81.8% | Majority completed secondary school | ME: 58.1% Muslims CA: 91.3% Christians SA: 76.9% Muslims SE: 100% Muslims |
| Le et al. (2018) [23] | 108 refugees in Switzerland | 43.2 | 78.7% | 62.1% | 41.6% completed secondary | - |
| Morina et al. (2016) [24] | 134 refugees in Switzerland | 42 | 78.4% | 58.2% | 36.6% completed ≥12 years of education | - |
| Tinghög et al. (2017) [25] | 1215 Syrian refugees resettled in Sweden | 32.9% between 30 and 39 years | 62.8% | 63.5% | 40.2% completed 0–9 years | - |
| NCTTP (2015) [26] | 9025 torture survivors | 40.18 | 53% | 53% | Mean: 11.8 years of education | Christians 48.0% Muslims 38.5% Buddhist 7.5% |
| Song et al. (2018) [27] | 278 torture survivors mainly from Iraq, Iran, Eritrea | 40.31 | 45.3% | - | 36.5% completed ≥13 years | Christians 37.4% Muslims 36% Buddhist 8.6% |
| Willard et al. (2014) [8] | 497 Iraqi refugees in the United States | 57.95% between 19 and 64 years | 55.5% | - | - | - |
| Robertson et al. (2016) [28] | 449 Somali and Oromo refugee trauma survivors | 37.1 | 52% | 32% | 50% completed secondary school | - |
| Asgary et al. (2013) [29] | 30 asylee in the United States | 31.2 | 70% | 68% | 40 % had at least college education | - |
| Chu et al. (2013) [30] | 875 survivors of political violence | 34.37 | 64% | 63% | 59% completed high school or more | Muslims 38% Christians 31% Buddhist 28% |
| Raghavan et al. (2013) [31] | 172 refugees in the United States | 36.9 | 66.9% | 64.5% | - | Muslims 37.2% Christians 33.1% Buddhist 24.4% |
| Hoffman et al. (2017) [32] | 111 Karen refugees | 33.7 | 52% | 57% | - | - |
| Carlsson et al. (2010) [33] | 45 (66% Iraqi) refugees | 39.2 | 66.7% | 82.2% | - | - |
| Hooberman et al. (2010) [34] | 75 torture survivors in the United States | - | 58.7% | 54.7% | 30.6% completed less than high school | Muslims 42.7% Christians 23.9% Buddhist 14.7% |
| Kroo and Nagy (2011) [35] | 53 Somali refugees | 83.0% between 18 and 29 years | 83.0% | 35.8% | 45.3% completed 1–4 elementary educations | - |
| Berthold et al. (2014) [14] | 136 Cambodian refugees | 56.5 | 39% | 58.8% | 47.8% completed 1–5 years of education | - |
| Keatley et al. (2015) [36] | 85 torture survivors with Traumatic Brain Injury (TBI) | 34.18 | 69.4% | - | 49.41% completed post-secondary education | Christians 41.17% Muslims 36.47% Buddhist 15.29% |
| Study | Sample | Trauma (%) | Primary Torture (%) | Secondary Torture (%) | Torture Methods (%) | Demographics |
|---|---|---|---|---|---|---|
| Shannon et al. (2016) [16] | 179 Karen refugees | - | 27.4 | 51.4 | - | - |
| Odenat (2012) [17] | 326 adult refugee torture survivors | - | - | - | Witnessing (59.5); physical (56.4); sexual (36.5); loss of control of basic life routine (45.4); aggressive environmental control (31.6); formal accusation (30.4) | - |
| Ibrahim and Hassan (2017) [18] | 91 Syrian Kurdish refugees | Three or more events during or after migration (79); forced to flee home country (86.8); witnessed destruction (64.8); confinement due to violence (61.5); exposure to elements (72.6); food/water deprivation (27.5) | - | - | - | - |
| Leaman and Gee (2012) [19] | 131 African torture survivors | - | - | - | Sexual (45); beatings (89); threats to family (48); threats of death (44); verbal abuse (58); food/water deprivation (61) | 64% of those who experienced sexual torture were women |
| McColl et al. (2010) [20] | 306 torture survivors from Gaza, Egypt, Mexico, Honduras, South Africa | Ten or more events (10) | 76 | - | Higher exposure to trauma in men than women | |
| Luitel et al. (2013) [21] | 720 torture survivors | Witnessed murders (73); witnessed injury (70); witnessed harassment (68); witnessed destruction of property (60) | - | - | - | - |
| Schubert and Punamäki (2011) [22] | 78 torture survivors from Middle East (ME), Central Africa (CA), South Asia (SA), Southeast Europe (SE) | - | - | - | Death threats and terrorization; witnessing injury/killings; sexual molestations | Sexual torture more common in women; detainment more common in men |
| Le et al. (2018) [23] | 108 refugees in Switzerland | - | - | - | Physical (97.2); forced stress positions (94.4); psychological manipulation (93.5); humiliating treatment (93.5); deprivation of basic needs (91.7); exposure to sensory discomfort (86.1); sexual torture (82.4) | - |
| Morina et al. (2016) [24] | 134 refugees in Switzerland | - | 85 | Isolation (76.9); imprisonment (76.9); physical assault (75.4); combat (75.4); murder of friend or family member (64.9) forced separation from family (60.4); brainwashing (47.8); disappearing or kidnapping (47) | - | |
| Tinghög et al. (2017) [25] | 1215 Syrian refugees resettled in Sweden | Forced separation from friends or family (67.9); loss of significant other (64); witnessed violence or assault (63); sexual violence (7) | 31 | - | - | |
| NCTTP (2015) [26] | 9025 torture survivors | - | - | - | Beating (67.3); threats (67.2); rape (31.1—females; 8.1—male) | Women exposed to rape more than men; age at first torture was 25–44 years |
| Song et al. (2018) [27] | 278 torture survivors mainly from Iraq, Iran, Eritrea | - | - | - | Beating (45.6); wound/maim (8.4); rape/sexual (8.8); forced posture—stretched or hung (11.7); deprivation (17.9); sensory stress (12.4); threats and psychological (56); witnessing (30.8) | Political beliefs (36.3%), family background (38.2%), religious beliefs (30.9%), ethnicity/race (12.3%), and group membership (17.6%) were reasons for torture |
| Willard et al. (2014) [8] | 497 Iraqi refugees in the United States | - | 56 | Beatings, kidnapping and interrogation, electric shock, rape, witness torture of family member | 57.6% of adults; 52.9% of children | |
| Robertson et al. (2016) [28] | 449 Somali and Oromo refugee trauma survivors | - | - | - | Physical (71); witness (74); sexual (21) | - |
| Asgary et al. (2013) [29] | 30 asylee in the United States | - | - | - | Blunt force trauma (93) | Political beliefs (63%) and group membership were reasons for torture |
| Study | Sample | Measures | PTSD | Depression | Anxiety |
|---|---|---|---|---|---|
| Ibrahim and Hassan (2017) [18] | 91 Syrian Kurdish refugees | HTQ 1 (cut-off 2.5) | 35.16% (16 items) 38.46% (45 items) | - | - |
| Song et al. (2018) [27] | 278 torture survivors mainly from Iraq, Iran, Eritrea | PCL 2 (45–50 points) HSCL-25 3 (cut-off 1.75) | 56.9% | 83.8% | 81.3% |
| Odenat (2012) [17] | 326 adult refugee torture survivors | Clinician Administered PTSD Scale | 23% | - | - |
| Leaman and Gee (2012) [19] | 131 African torture survivors | Part 4 HTQ (cut-off 2.5) HSCL-25 (cut-off 1.75) | 57.3% | 94.7% | - |
| Asgary et al. (2013) [29] | 30 asylee in the United States | DSM IV-TR | 69% | 69% | - |
| Luitel et al. (2013) [21] | 720 torture survivors | PCL-C (more than 50 score) BDI 4 (more than 20) BAI 5 (more than 17) | 9.6% | 27.5% | 22.9% |
| Hooberman et al. (2010) [34] | 75 torture survivors in the United States | HTQ (cut-off 2.5) | 40.0% | - | - |
| Tufan et al. (2013) [37] | 57 refugees | DSM-IV-TR | 55.2% | 55.2% | - |
| Bandeira et al. (2010) [13] | 55 refugees torture survivors | HTQ (cut-off 2.5) HADS 6 (more than 11) | 69% | 74% | 91% |
| Schubert and Punamäki (2011) [22] | 78 torture survivors | IES-R 7 HSCL-25 | 88.3% | 78.2% | 78.2% |
| Tinghög et al. (2017) [25] | 1215 Syrian refugees resettled in Sweden | HTQ (mean item score of 2.06) HSCL-25 (1.80 depression, 1.75 anxiety) | 29.9% | 40.2% | 31.8% |
| Tamblyn et al. (2011) [15] | 61 torture survivors | DSM-IV TR | 48% | 45% | 31% |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abu Suhaiban, H.; Grasser, L.R.; Javanbakht, A. Mental Health of Refugees and Torture Survivors: A Critical Review of Prevalence, Predictors, and Integrated Care. Int. J. Environ. Res. Public Health 2019, 16, 2309. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16132309
Abu Suhaiban H, Grasser LR, Javanbakht A. Mental Health of Refugees and Torture Survivors: A Critical Review of Prevalence, Predictors, and Integrated Care. International Journal of Environmental Research and Public Health. 2019; 16(13):2309. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16132309
Chicago/Turabian StyleAbu Suhaiban, Hiba, Lana Ruvolo Grasser, and Arash Javanbakht. 2019. "Mental Health of Refugees and Torture Survivors: A Critical Review of Prevalence, Predictors, and Integrated Care" International Journal of Environmental Research and Public Health 16, no. 13: 2309. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16132309