What is the Role of Internalizing and Externalizing Symptoms in Adolescent Suicide Behaviors?



Abstract
:1. Introduction
Internalizing and Externalizing Symptomatology as a Risk Factor in Adolescents
2. Materials and Methods
2.1. Participants
2.2. Variables and Instruments
2.3. Procedure
2.4. Data Analyses
3. Results
3.1. Preliminary and Descriptive Analyses
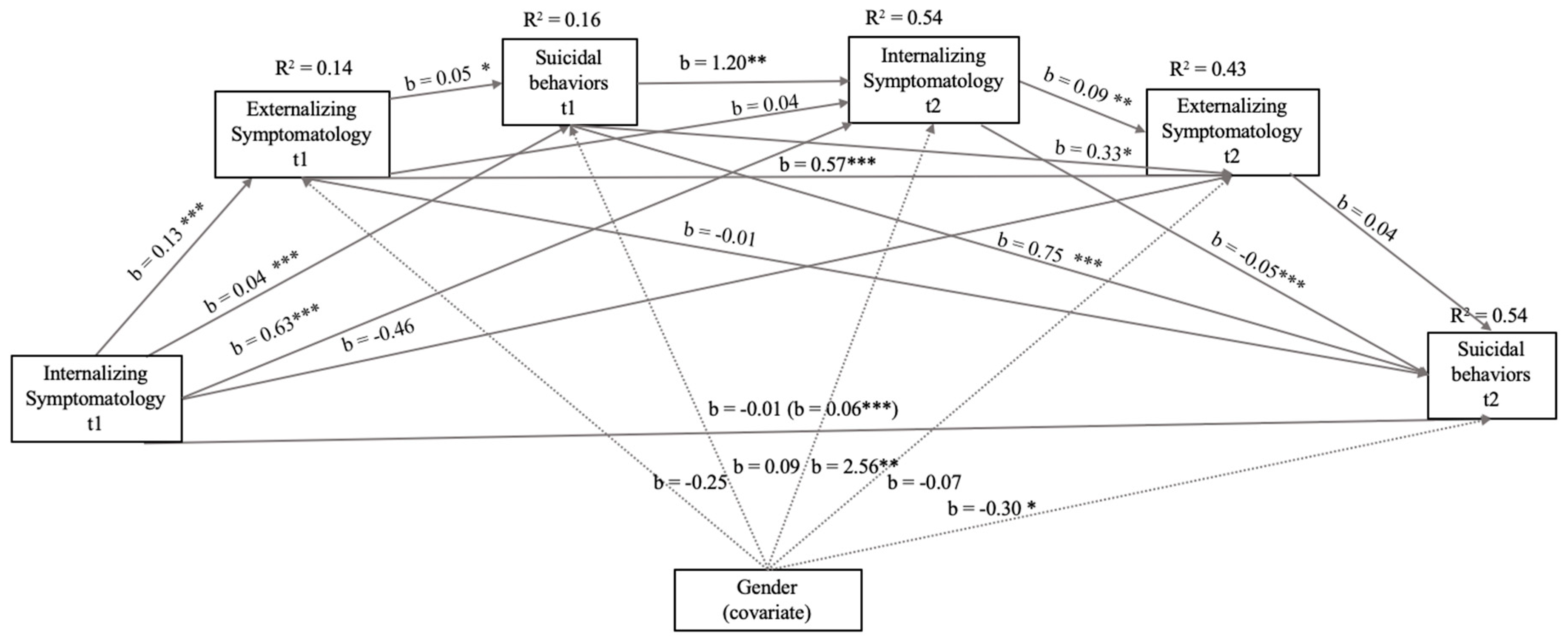
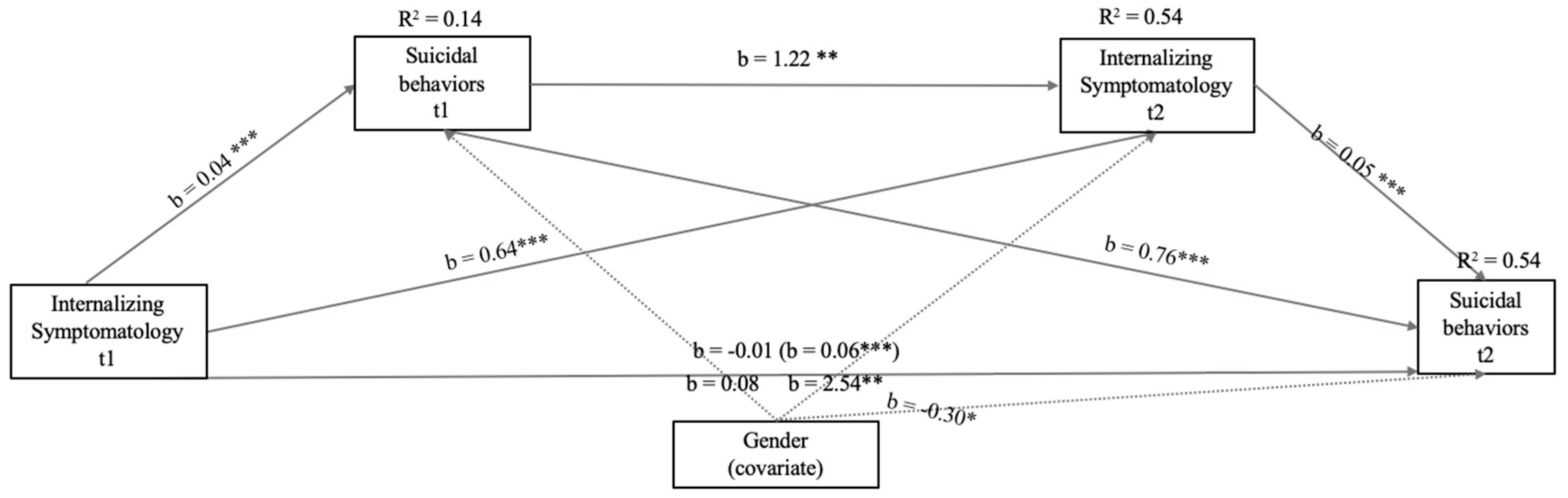
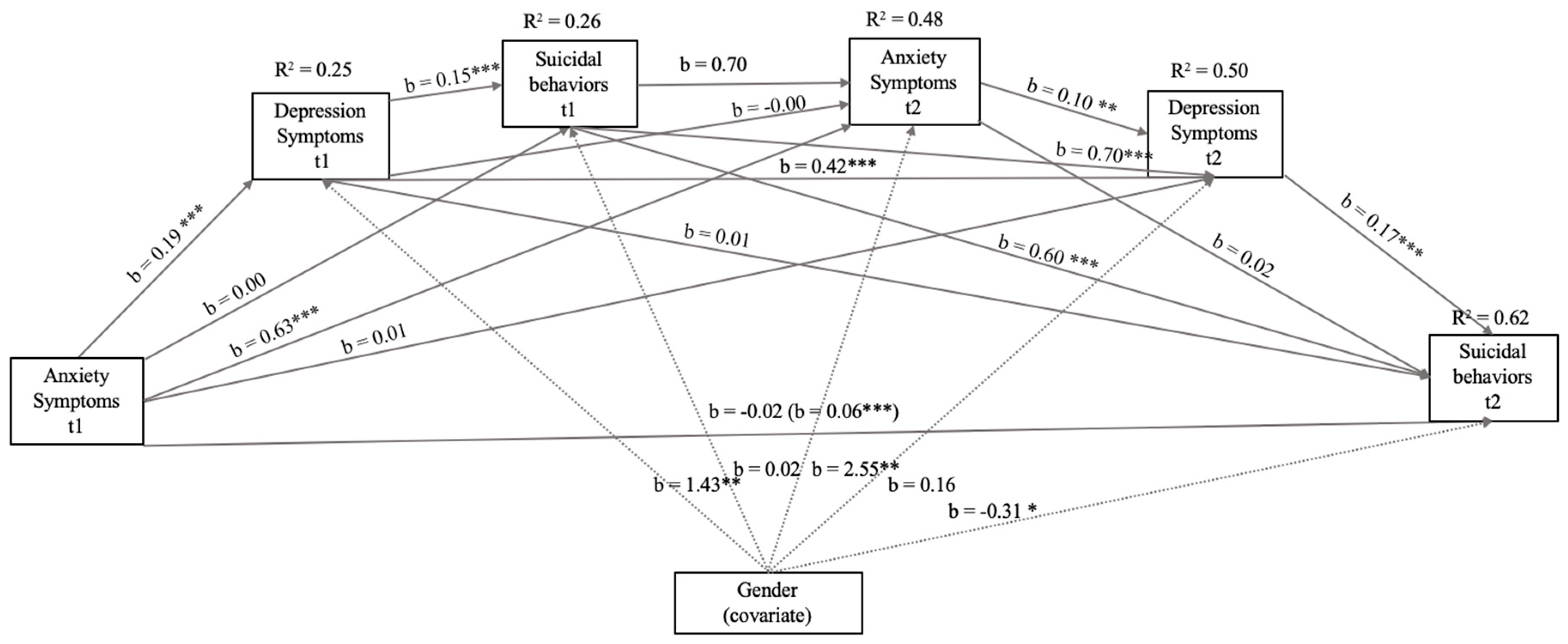
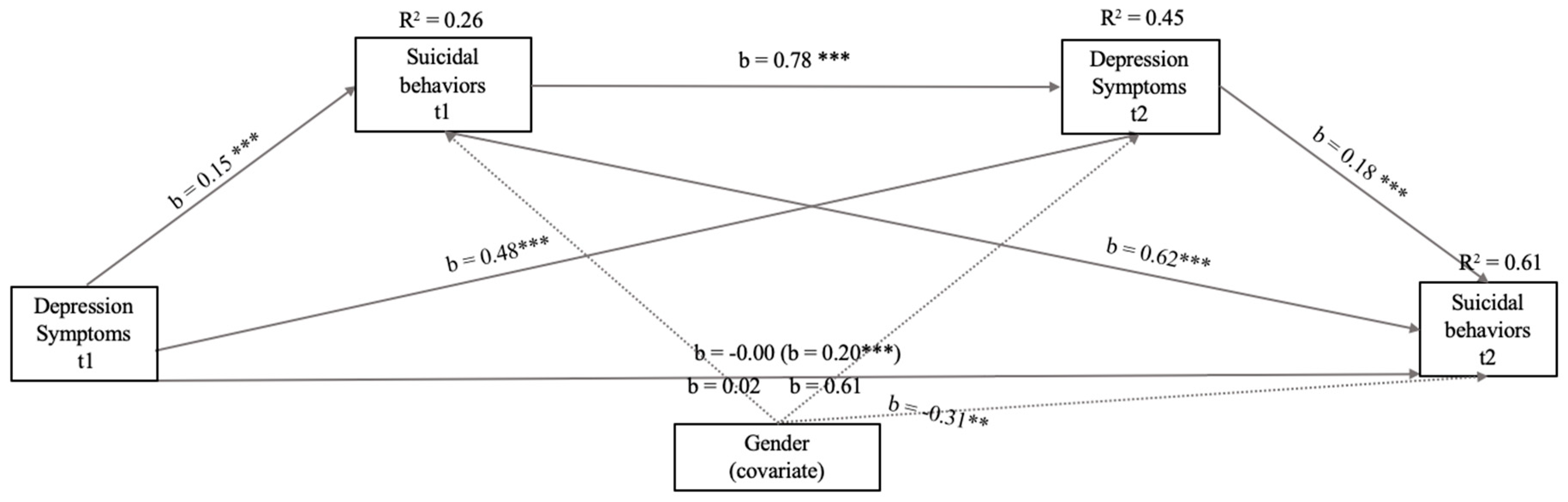
3.2. Internalizing and Externalizing Symptoms at t1 and t2 in the Prediction of Suicidal Behaviors at t2.
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Pitman, A.; Krysinska, K.; Osborn, D.; King, M. Suicide in young men. Lancet 2012, 379, 2383–2392. [Google Scholar] [CrossRef]
- Organización Mundial de la Salud. Prevención del Suicidio: Un Imperativo Global. 2014. Available online: http://apps.who.int/iris/bitstream/10665/131056/1/9789241564779_eng.pd (accessed on 3 February 2019).
- Instituto Nacional de Estadística, INE. Defunción Según la Causa de Muerte. Available online: http://www.ine.es/prensa/edcm_2016.pdf (accessed on 3 February 2019).
- Castellví, P.; Lucas-Romero, E.; Miranda-Mendizábal, A.; Parés-Badell, O.; Almenara, J.; Alonso, I.; Cebrià, A.; Gabilondo, A.; Gili, M.; Lagares, C.; et al. Longitudinal association between self-injurious thoughts and behaviors and suicidal behavior in adolescents and young adults: A systematic review with meta-analysis. J. Affect. Disord. 2017, 215, 37–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mortier, P.; Auerbach, R.P.; Alonso, J.; Bantjes, J.; Benjet, C.; Cuijpers, P.; Ebert, D.D.; Green, J.G.; Hasking, P.; Nock, M.K.; et al. Suicidal thoughts and behaviors among first-year college students: Results from the WMH-ICS Project. J. Am. Acad. Child Adolesc. Psychiatr. 2018, 57, 263–273. [Google Scholar] [CrossRef] [PubMed]
- Nock, M.K.; Borges, G.; Bromet, E.J.; Cha, C.B.; Kessler, R.C.; Lee, S. Suicide and Suicidal Behavior. Epidemiol. Rev. 2008, 30, 133–154. [Google Scholar] [CrossRef] [PubMed]
- Castellví, P.; Miranda-Mendizábal, A.; Parés-Badell, O.; Almenara, J.; Alonso, I.; Blasco, M.J.; Cebrià, A.; Gabilondo, A.; Gili, M.; Lagares, C.; et al. Exposure to violence, a risk for suicide in youths and young adults. A meta-analysis of longitudinal studies. Acta Psychiatr. Scand. 2017, 135, 195–211. [Google Scholar] [CrossRef] [PubMed]
- Appleby, L.; Shaw, J.; Amos, T.; McDonnell, R.; Harris, C.; McCann, K.; Kiernan, K.; Davies, S.; Bickley, H.; Parsons, R. Suicide within 12 months of contact with mental health services: National clinical survey. BMJ 1999, 318, 1235–1239. [Google Scholar] [CrossRef] [PubMed]
- Brent, D.A.; Perper, J.; Moritz, G.; Baugher, M.; Allman, C. Suicide in adolescents with no apparent psychopathology. J. Am. Acad. Child Adolesc. Psychiatr. 1993, 32, 494–500. [Google Scholar] [CrossRef]
- Brent, D.A.; Mann, J.J. Familial pathways to suicidal behavior: Understanding and preventing suicide among adolescents. N. Engl. J. Med. 2006, 355, 2719–2721. [Google Scholar] [CrossRef]
- Baca–Garcia, E.; Diaz–Sastre, C.; Resa, E.G.; Blasco, H.; Conesa, D.B.; Oquendo, M.A.; Saiz-Ruiz, J.; Leon, J. Suicide attempts and impulsivity. Eur. Arch. Psych. Clin. Neurosci. 2005, 255, 152–156. [Google Scholar] [CrossRef]
- Boergers, J.; Spirito, A.; Donaldson, D. Reasons for adolescent suicide attempts: Associations with psychological functioning. J. Am. Acad. Child Adolesc. Psychiatr. 1998, 37, 1287–1293. [Google Scholar] [CrossRef]
- González, C.; Ramos, L.; Caballero, M.Á.; Wagner, F.A. Correlatos psicosociales de depresión, ideación e intento suicida en adolescentes mexicanos. Psicothema 2003, 15, 524–532. [Google Scholar]
- Wichstrøm, L. Predictors of non-suicidal self-injury versus attempted suicide: Similar or different? Arch. Suicide Res. 2009, 13, 105–122. [Google Scholar] [CrossRef] [PubMed]
- Soto-Sanz, V.; Piqueras, J.A.; Castellví, P.; Rodríguez-Jímenez, T.; Rodríguez-Marín, J.; Miranda-Mendizábal, A.; Parés-Badell, O.; Almenara, J.; Alonso, I.; Blasco, M.J.; et al. Self-esteem and suicidal behaviour in youth: A meta-analysis of longitudinal studies. Psicothema. in press.
- Cavanagh, J.T.; Owens, D.G.; Johnstone, E.C. Life events in suicide and undetermined death in south-east Scotland: A case-control study using the method of psychological autopsy. OGY Soc. Psychiatry Psychiatr. Epidemiol. 1999, 34, 645–650. [Google Scholar] [CrossRef]
- Khan, M.M.; Mahmud, S.; Karim, M.S.; Zaman, M.; Prince, M. Case-control study of suicide in Karachi, Pakistan. Br. J. Psychiatr. 2008, 193, 402–405. [Google Scholar] [CrossRef] [PubMed]
- Rueda-Jaimes, G.E.; Rangel-Martínez-Villalba, A.M.; Camacho, P.A. Trastorno bipolar y suicidabilidad en pacientes colombianos. Rev. Colomb. Psiquiatr. 2011, 108S–118S. [Google Scholar] [CrossRef]
- Evans, E.; Hawton, K.; Rodham, K. Factors associated with suicidal phenomena in adolescents: A systematic review of population-based studies. Clin. Psychol. Rev. 2004, 24, 957–979. [Google Scholar] [CrossRef] [PubMed]
- Gili, M.; Castellví, P.; Vives, M.; De La Torre-Luque, A.; Almenara, J.; Blasco, M.J.; Cebrià, A.; Gabilondo, A.; Pérez-Ara, M.A. Mental disorders as risk factors for suicidal behavior in young people: A metaanalysis and systematic review of longitudinal studies. J. Affect. Disord. 2019, 245, 152–162. [Google Scholar] [CrossRef]
- Gabilondo, A.; Alonso, J.; Pinto-Meza, A.; Vilagu, G.; Fernández, A.; Serrano-Blanco, A.; Almansa, J.; Codony, M.; Maria Haro, J. Prevalencia y factores de riesgo de las ideas, planes e intentos de suicidio en la población general española. Resultados del estudio ESEMeD. Med. Clin. 2007, 129, 494–500. [Google Scholar] [CrossRef]
- Langhinrichsen-Rohling, J.; Friend, J.; Powell, A. Adolescent suicide, gender, and culture: A rate and risk factor analysis. Aggress. Violent Behav. 2009, 14, 402–414. [Google Scholar] [CrossRef]
- Parra Uribe, I.; Blasco-Fontecilla, H.; García-Parés, G.; Giró Batalla, M.; Llorens Capdevila, M.; Cebrià Meca, A.; de Leon-Martinez, V.; Pérez-Solà, V.; Palao Vidal, D.J. Attempted and completed suicide: Not what we expected? J. Affect. Disord. 2013, 150, 840–846. [Google Scholar] [CrossRef] [PubMed]
- Achenbach, T.M.; Edelbrock, C.; Howell, C.T. Empirically based assessment of the behavioral/emotional problems of 2- and 3-year-old children. J. Abnorm. Child Psychol. 1987, 15, 629–650. [Google Scholar] [CrossRef] [PubMed]
- Carter, G.L.; Issakidis, C.; Clover, K. Correlates of youth suicide attempters in Australian community and clinical samples. Aust. N. Z. J. Psychiatr. 2003, 37, 286–293. [Google Scholar] [CrossRef] [PubMed]
- Mars, B.; Heron, J.; Crane, C.; Hawton, K.; Kidger, J.; Lewis, G.; Macleod, J.; Tilling, K.; Gunnell, D. Differences in risk factors for self-harm with and without suicidal intent: Findings from the ALSPAC cohort. J. Affect. Disord. 2014, 168, 407–414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norton, P.J.; Temple, S.R.; Pettit, J.W. Suicidal ideation and anxiety disorders: Elevated risk or artifact of comorbid depression? J. Behav. Ther. Exp. Psychiatr. 2008, 39, 515–525. [Google Scholar] [CrossRef] [PubMed]
- Nrugham, L.; Larsson, B.; Sund, A.M. Specific depressive symptoms and disorders as associates and predictors of suicidal acts across adolescence. J. Affect. Disord. 2008, 111, 83–93. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Lee, Y.; Youn, T.; Kim, B.S.; Park, J.I.; Kim, H.; Lee, H.C.; Hong, J.P. Association between level of suicide risk, characteristics of suicide attempts, and mental disorders among suicide attempters. BMC Public Health 2018, 18, 477. [Google Scholar] [CrossRef] [PubMed]
- Roberts, R.E.; Roberts, C.R.; Xing, Y. One-year incidence of suicide attempts and associated risk and protective factors among adolescents. Arch. Suicide Res. Off. J. Arch. Suicide Res. 2010, 14, 66–78. [Google Scholar] [CrossRef] [PubMed]
- Shaffer, D.; Gould, M.S.; Fisher, P.; Trautman, P.; Moreau, D.; Kleinman, M.; Flory, M. Psychiatric diagnosis in child and adolescent suicide. Arch. Gen. Psychiatr. 1966, 53, 339–348. [Google Scholar] [CrossRef]
- Brausch, A.M.; Gutierrez, P.M. Differences in non-suicidal self-injury and suicide attempts in adolescents. J. Youth Adolesc. 2010, 39, 233–242. [Google Scholar] [CrossRef]
- Goldston, D.B.; Daniel, S.S.; Erkanli, A.; Reboussin, B.A.; Mayfield, A.; Frazier, P.H.; Treadway, S.L. Psychiatric diagnoses as contemporaneous risk factors for suicide attempts among adolescents and young adults: Developmental changes. J. Consult. Clin. Psychol. 2009, 77, 281–290. [Google Scholar] [CrossRef] [PubMed]
- Soto-Sanz, V.; Castellví, P.; Piqueras, J.A.; Rodríguez-Marín, J.; Rodríguez-Jiménez, T.; Miranda-Mendizábal, A.; Parés-Badell, O.; Almenara, J.; Alonso, I.; Blasco, M.J. Internalizing and externalizing symptoms and suicidal behavior in young people: A systematic review and meta-analysis of longitudinal studies. Acta Psychiatr. Scand. 2019. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Petukhova, M.; Sampson, N.A.; Zaslavsky, A.M.; Wittchen, H.-U. Twelve-month and lifetime prevalence and lifetime morbid risk of anxiety and mood disorders in the United States. Int. J. Methods Psychiatr. Res. 2012, 21, 169–184. [Google Scholar] [CrossRef] [PubMed]
- Campos, R.C.; Holden, R.R.; Laranjeira, P.; Troister, T.; Oliveira, A.R.; Costa, F.; Abreu, M.; Fresca, N. Self-report depressive symptoms do not directly predict suicidality in nonclinical individuals: Contributions toward a more psychosocial approach to suicide risk. Death Stud. 2016, 40, 335–349. [Google Scholar] [CrossRef] [PubMed]
- Piqueras, J.A.; Garcia-Olcina, M.; Rivera-Riquelme, M.; Rodriguez-Jimenez, T.; Martinez-Gonzalez, A.E.; Cuijpers, P. DetectaWeb Project: Study protocol of a web-based detection of mental health of children and adolescents. BMJ Open 2017, 7, e017218. [Google Scholar] [CrossRef] [PubMed]
- Instituto Nacional de Estadística, INE. Enseñanzas No Universitarias Alumnado Matriculado. Curso 2017–2018. Available online: http://www.educacionyfp.gob.es/servicios-al-ciudadano/estadisticas/no-universitaria/alumnado/matriculado/2017-2018-rd.html (accessed on 9 July 2019).
- Currie, C.E.; Elton, R.A.; Todd, J.; Platt, S. Indicators of socioeconomic status for adolescents: The WHO Health Behaviour in School-aged Children Survey. Health Educ. Res. 1997, 12, 385–397. [Google Scholar] [CrossRef] [PubMed]
- Boyce, W.; Torsheim, T.; Currie, C.; Zambon, A. The family affluence scale as a measure of national wealth: Validation of an adolescent self-report measure. Soc. Indic. Res. 2006, 78, 473–487. [Google Scholar] [CrossRef]
- García-Olcina, M.; Rivera-Riquelme, M.; Cantó-Diez, T.; Tomás-Berenguer, M.R.; Bustamante, R.; Piqueras, J.A. Detección Online de la Salud Mental en población clínica de niños y adolescentes: Escala DetectaWeb-Malestar. Rev. Psicol. Clínica Niños Adolesc. 2017, 4, 1–21. [Google Scholar]
- García-Olcina, M.; Piqueras, J.A.; Martínez-González, A.E. Datos preliminares de la validación del Cuestionario de Detección vía Web para los trastornos emocionales (DETECTA-WEB) en adolescentes españoles [Preliminary data of the Web-based Screening Questionnaire for emotional mental disorders (DETECTA-WEB) in Spanish adolescents]. Rev. Psicol. Clínica Niños Adolesc. 2014, 1, 69–77. [Google Scholar]
- Goodman, R. The Strengths and Difficulties Questionnaire: A research note. J. Child Psychol. Psychiatry 1997, 38, 581–586. [Google Scholar] [CrossRef]
- Goodman, A.; Lamping, D.L.; Ploubidis, G.B. When to use broader internalising and externalising subscales instead of the hypothesised five subscales on the Strengths and Difficulties Questionnaire (SDQ): Data from British parents, teachers and children. J. Abnorm. Child Psychol. 2010, 38, 1179–1191. [Google Scholar] [CrossRef] [PubMed]
- Ortuño-Sierra, J.; Fonseca-Pedrero, E.; Paino, M.; i Riba, S.S.; Muñiz, J. Screening mental health problems during adolescence: Psychometric properties of the Spanish version of the Strengths and Difficulties Questionnaire. J. Adolesc. 2015, 38, 49–56. [Google Scholar] [CrossRef] [PubMed]
- SPSS: IBM Corp. IBM SPSS Statistics for Macintosh; Version 24.0; IBM Corporations: Armonk, NY, USA, 2016. [Google Scholar]
- McDonald, R.P. Test Theory: A Unified Approach; Erlbaum: Mahwah, NJ, USA, 1999. [Google Scholar]
- Dunn, T.J.; Baguley, T.; Brunsden, V. From alpha to omega: A practical solution to the pervasive problem of internal consistency estimation. Br. J. Psychol. 2014, 105, 399–412. [Google Scholar] [CrossRef]
- Campo-Arias, A.; Oviedo, H.C. PROPIEDADES PSICOMÉTRICAS DE UNA ESCALA: LA CONSISTENCIA INTERNA. Rev. Salud Pública 2008, 10, 831–839. [Google Scholar] [CrossRef] [PubMed]
- Katz, M.H. Multivariate Analysis, 2nd ed.; Cambridge University Press: Cambridge, UK, 2006. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Hayes, A.F.; Preacher, K.J. Processes. In Structural Equation Modeling: A Second Course, 2nd ed.; Hancock, G.R., Mueller, R.O., Eds.; Information Age Publishing: Charlotte, NC, USA, 2013. [Google Scholar]
- Preacher, K.J.; Hayes, A.F. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav. Res. Methods 2018, 40, 879–891. [Google Scholar] [CrossRef]
- Yoder, K.A.; Longley, S.L.; Whitbeck, L.B.; Hoyt, D.R. A dimensional model of psychopathology among homeless adolescents: Suicidality, internalizing, and externalizing disorders. J. Abnorm. Child Psychol. 2008, 36, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Esposito, C.L.; Clum, G.A. The relative contribution of diagnostic and psychosocial factors in the prediction of adolescent suicidal ideation. J. Clin. Child. Adolesc. Psychol. 2013, 32, 386–395. [Google Scholar] [CrossRef]
- Choo, C.; Chew, P.; Ho, R. Suicide precipitants differ across the lifespan but are not significant in predicting medically severe attempts. Int. J. Environ. Res. Public Health 2018, 15, 691. [Google Scholar] [CrossRef]
- Vander Stoep, A.; Adrian, M.; McCauley, E.; Crowell, S.E.; Stone, A.; Flynn, C. Risk for suicidal ideation and suicide attempts associated with co-occurring depression and conduct problems in early adolescence. Suicide Life-Threat. Behav. 2011, 41, 316–329. [Google Scholar] [CrossRef]
- Windfuhr, K.; While, D.; Hunt, I.; Turnbull, P.; Lowe, R.; Burns, J.; Swinson, N.; Shaw, J.; Appleby, L.; Kapur, N. Suicide in juveniles and adolescents in the United Kingdom. J. Child Psychol. Psychiatry 2008, 49, 1155–1165. [Google Scholar] [CrossRef]
- Epkins, C.C.; Heckler, D.R. Integrating etiological models of social anxiety and depression in youth: Evidence for a cumulative interpersonal risk model. Clin. Child Fam. Psychol. Rev. 2011, 14, 329–376. [Google Scholar] [CrossRef] [PubMed]
- Kingery, J.N.; Erdley, C.A.; Marshall, K.C.; Whitaker, K.G.; Reuter, T.R. Peer experiences of anxious and socially withdrawn youth: An integrative review of the developmental and clinical literature. Clin. Child Fam. Psychol. Rev. 2010, 13, 91–128. [Google Scholar] [CrossRef] [PubMed]
- Gariépy, G.; Honkaniemi, H.; Quesnel-Vallée, A. Social support and protection from depression: Systematic review of current findings in Western countries. Br. J. Psychiatr. 2016, 209, 284–293. [Google Scholar] [CrossRef] [PubMed]
- Hawton, K.; Casañas, I.; Comabella, C.; Haw, C.; Saunders, K. Risk factors for suicide in individuals with depression: A systematic review. J. Affect. Disord. 2013, 147, 17–28. [Google Scholar] [CrossRef] [PubMed]
- Miranda-Mendizabal, A.; Castellví, P.; Parés-Badell, O.; Alayo, I.; Almenara, J.; Alonso, I.; Blasco, M.J.; Cebrià, A.; Gabilondo, A. Gender differences in suicidal behavior in adolescents and young adults: Systematic review and meta-analysis of longitudinal studies. Int. J. Public Health 2019, 64, 265–283. [Google Scholar] [CrossRef] [PubMed]
- Kumar, C.S.; Mohan, R.; Ranjith, G.; Chandrasekaran, R. Gender differences in medically serious suicide attempts: A study from South India. Psychiatry Res. 2006, 144, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Canetto, S.S.; Lester, D. Gender, culture, and suicidal behavior. Transcult. Psychiatry 1998, 35, 163–190. [Google Scholar] [CrossRef]
- Fennig, S.; Geva, K.; Zalzman, G.; Weitzman, A.; Fennig, S.; Apter, A. Effect of gender on suicide attempters versus nonattempters in an adolescent inpatient unit. Compr. Psychiatry 2005, 46, 90–97. [Google Scholar] [CrossRef] [PubMed]
- Keng, S.L.; Lee, Y.; Drabu, S.; Hong, R.Y.; Chee, C.Y.; Ho, C.S.; Ho, R.C. Construct validity of the mclean screening instrument for borderline personality disorder in two singaporean samples. J. Pers. Disord. 2018, 1–20. [Google Scholar] [CrossRef]
- Ramos, V.; Canta, G.; de Castro, F.; Leal, I. The relation between attachment, personality, internalizing, and externalizing dimensions in adolescents with borderline personality disorder. Bull. Menn. Clin. 2016, 80, 213–233. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | M Boys (N = 152) | SD | M Girls (N = 86) | SD | t | d |
|---|---|---|---|---|---|---|
| Suicide Behaviors, t1 | 0.29 | 0.77 | 0.65 | 1.29 | −2.41 ** | 0.33 |
| Suicide Behaviors, t2 | 0.42 | 1.23 | 0.68 | 1.37 | −1.59 | 0.20 |
| Internalizing Symptomatology, t1 | 15.8 | 7.37 | 22.63 | 8.99 | −6.29 *** | 0.83 |
| Internalizing Symptomatology, t2 | 13.83 | 8.48 | 21.16 | 7.99 | −6.65 *** | 0.88 |
| Externalizing symptomatology, t1 | 5.57 | 3.07 | 6.20 | 2.53 | −1.63 | 0.22 |
| Externalizing symptomatology, t2 | 5.84 | 3.15 | 6.61 | 2.67 | −1.90 | 0.26 |
| Variables | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|
| (1) Suicide Behaviors, t1 | - | |||||
| (2) Suicide Behaviors, t2 | 0.68 *** | - | ||||
| (3) Internalizing Symptomatology, t1 | 0.38 *** | 0.35 *** | - | |||
| (4) Internalizing Symptomatology, t2 | 0.39 *** | 0.48 *** | 0.71 *** | - | ||
| (5) Externalizing Symptomatology, t1 | 0.25 *** | 0.22 *** | 0.37 *** | 0.29 *** | - | |
| (6) Externalizing Symptomatology, t2 | 0.31 *** | 0.33 *** | 0.30 *** | 0.37 *** | 0.61 *** | - |
| Ideaction t1 N (%) | Ideation t2 N (%) | Plan t1 N (%) | Plan t2 N (%) | Attempt t1 N (%) | Attempt t2 N (%) | |
|---|---|---|---|---|---|---|
| Never (score 0) | 204 (85.7) | 201 (84.5) | 199 (83.6) | 197 (82.8) | 226 (95.0) | 221 (92.9) |
| Sometimes (score 1) | 29 (12.2) | 28 (11.8) | 31 (13.0) | 29 (12.2) | 12 (5.0) | 14 (5.9) |
| Many times (score 2) | 4 (1.7) | 8 (3.4) | 8 (3.4) | 10 (4.2) | - | 2 (0.8) |
| Always (score 3) | 1 (0.4) | 1 (0.4) | - | 2 (0.8) | - | 1 (0.4) |
| Total (score 1–3) | 34 (14.3) | 37 (15.5) | 39 (16.4) | 41 (17.2) | 12 (5.0) | 17 (7.1) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piqueras, J.A.; Soto-Sanz, V.; Rodríguez-Marín, J.; García-Oliva, C. What is the Role of Internalizing and Externalizing Symptoms in Adolescent Suicide Behaviors? Int. J. Environ. Res. Public Health 2019, 16, 2511. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16142511
Piqueras JA, Soto-Sanz V, Rodríguez-Marín J, García-Oliva C. What is the Role of Internalizing and Externalizing Symptoms in Adolescent Suicide Behaviors? International Journal of Environmental Research and Public Health. 2019; 16(14):2511. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16142511
Chicago/Turabian StylePiqueras, José Antonio, Victoria Soto-Sanz, Jesús Rodríguez-Marín, and Carlos García-Oliva. 2019. "What is the Role of Internalizing and Externalizing Symptoms in Adolescent Suicide Behaviors?" International Journal of Environmental Research and Public Health 16, no. 14: 2511. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16142511