Dose–Response Relationship of Outdoor Exposure and Myopia Indicators: A Systematic Review and Meta-Analysis of Various Research Methods


Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
2.2. Types of Studies
2.3. Search Strategy
2.4. Assessment of Methodological Quality
2.5. Data Analysis
3. Results
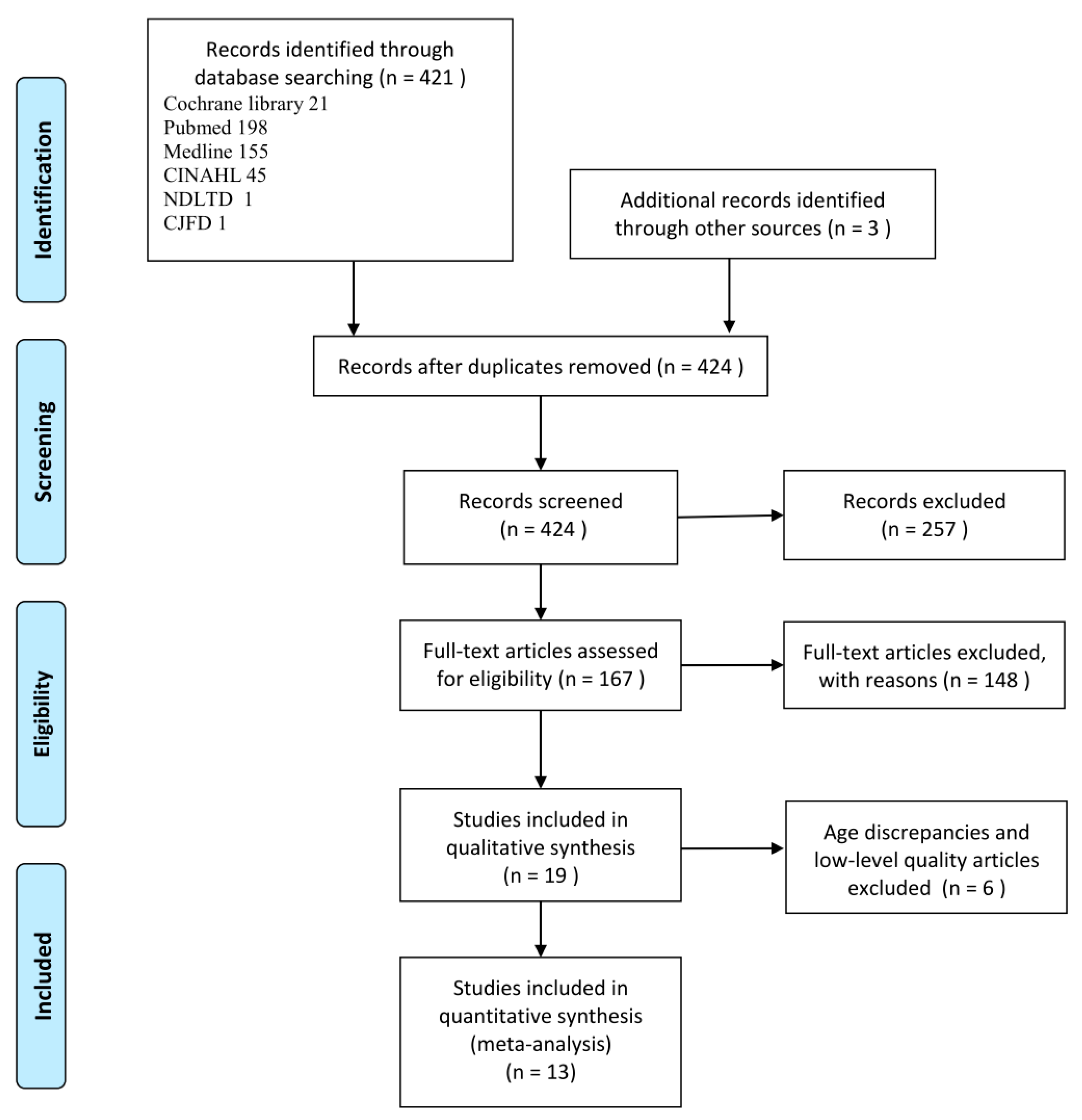
3.1. Search Results and Article Selection
3.2. Description of the Included Articles
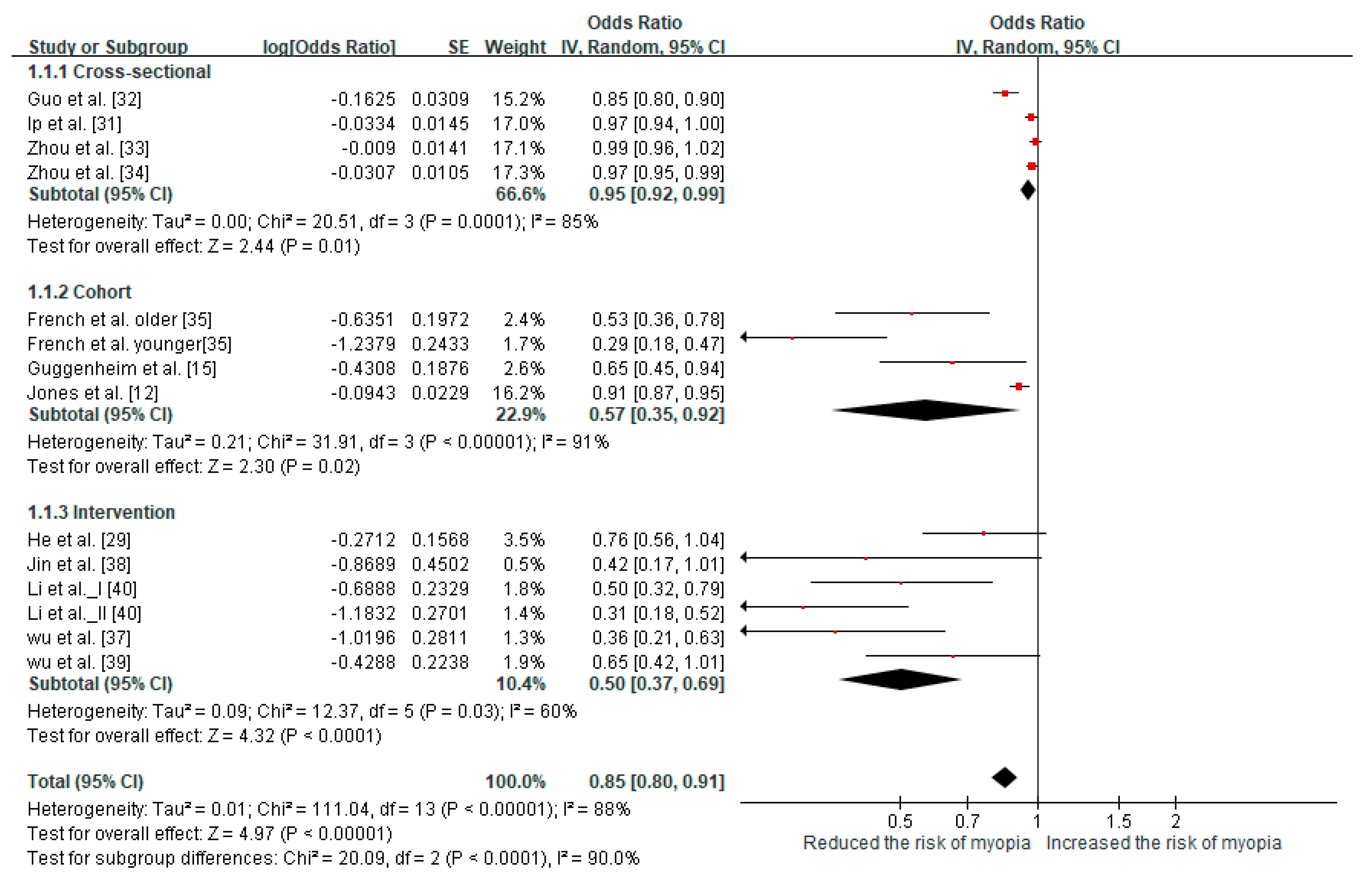
3.3. Association Between Outdoor Time and Risk of Incident/Prevalent Myopia
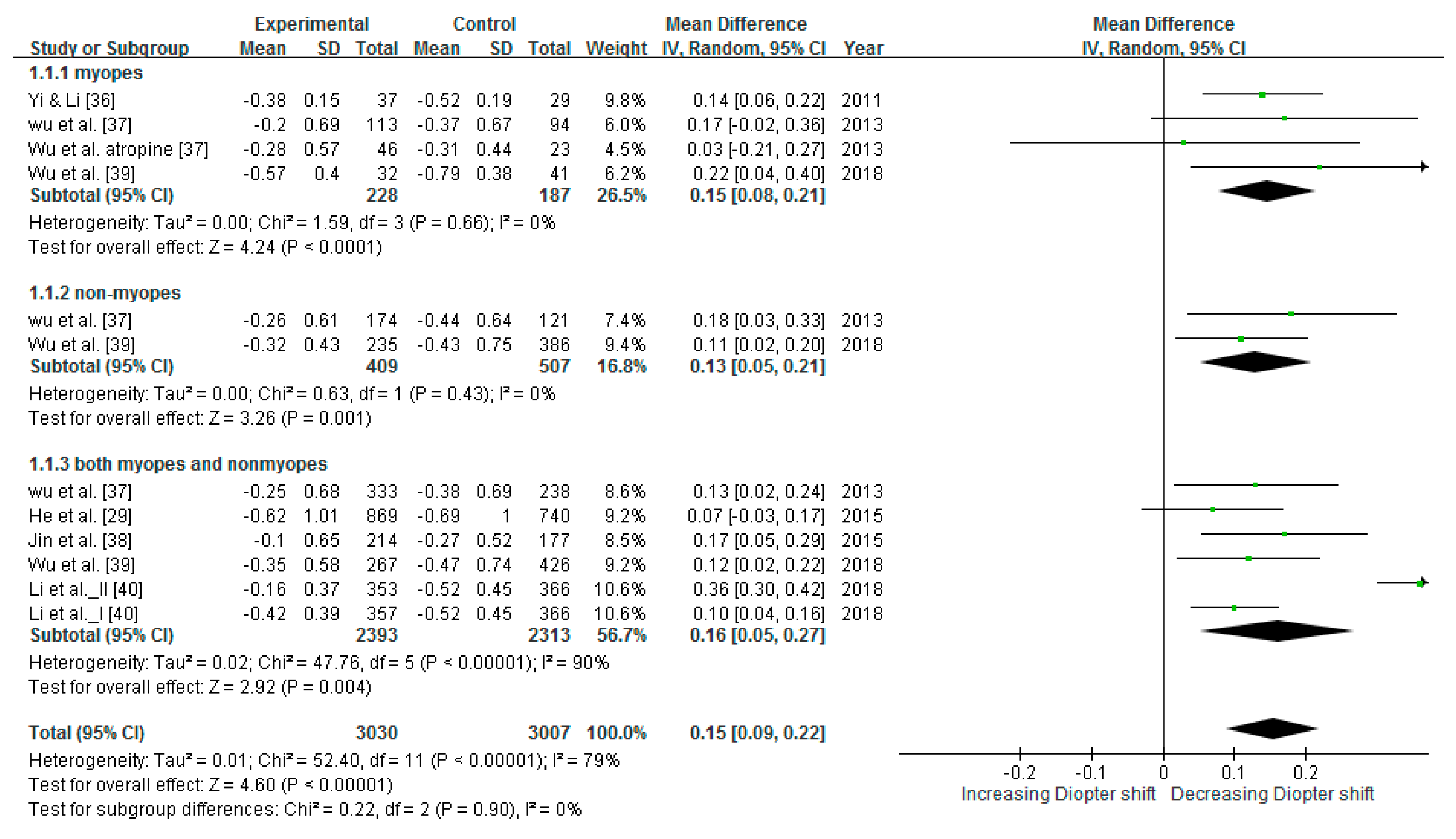
3.4. Reducing SER
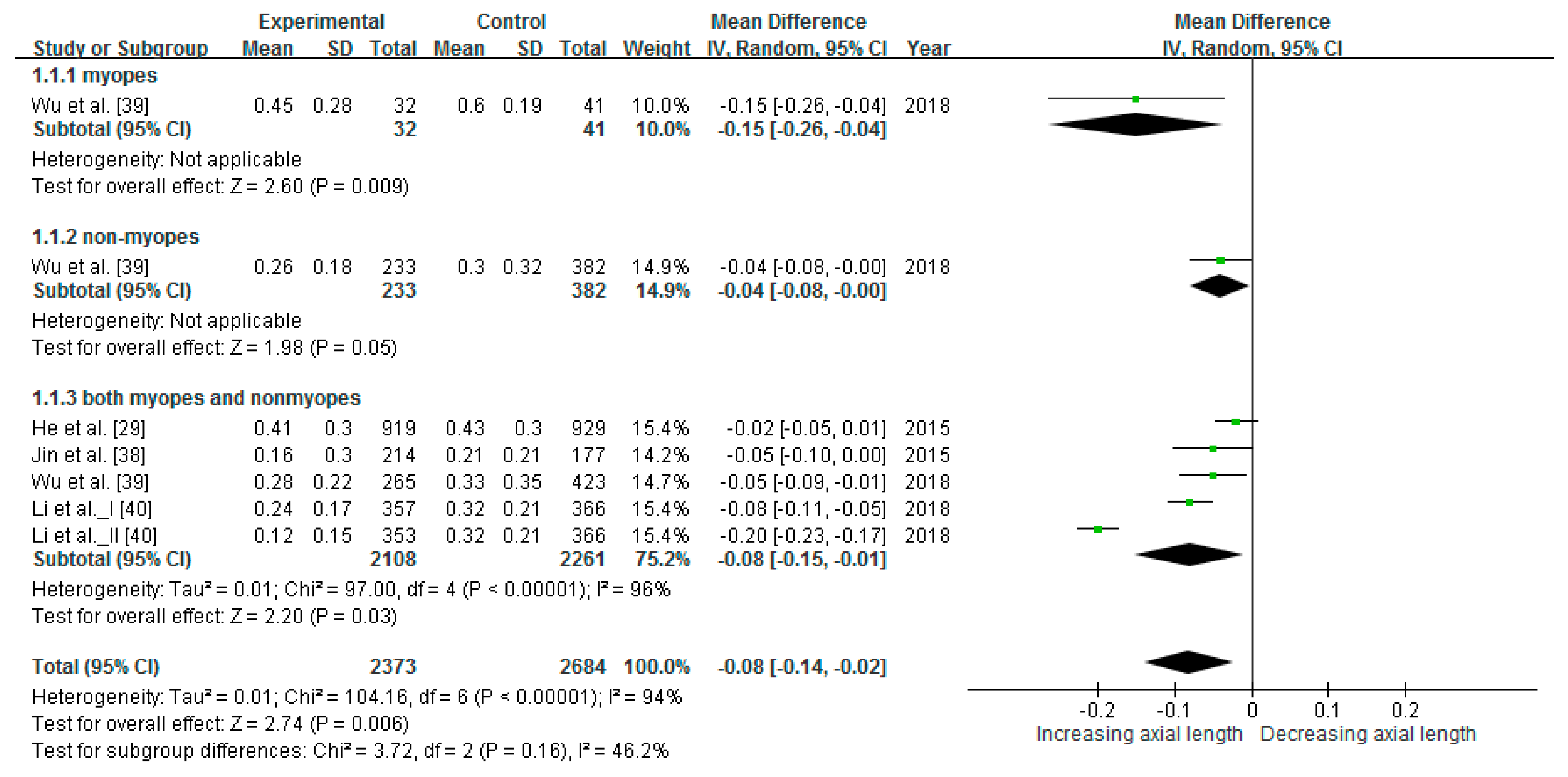
3.5. Slowing Axial Elongation
3.6. Effect of Reducing Myopic Progression in Intervention Studies
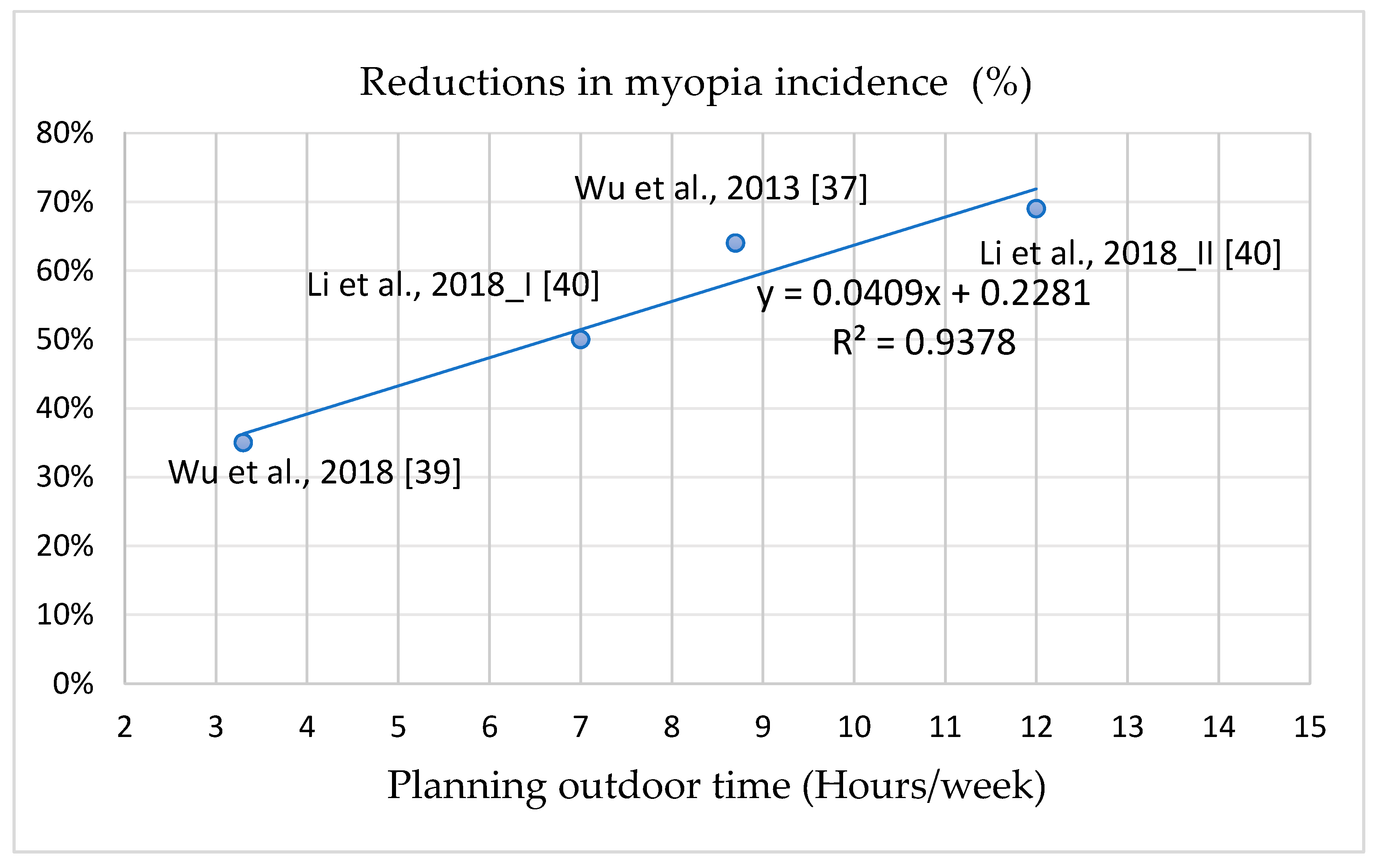
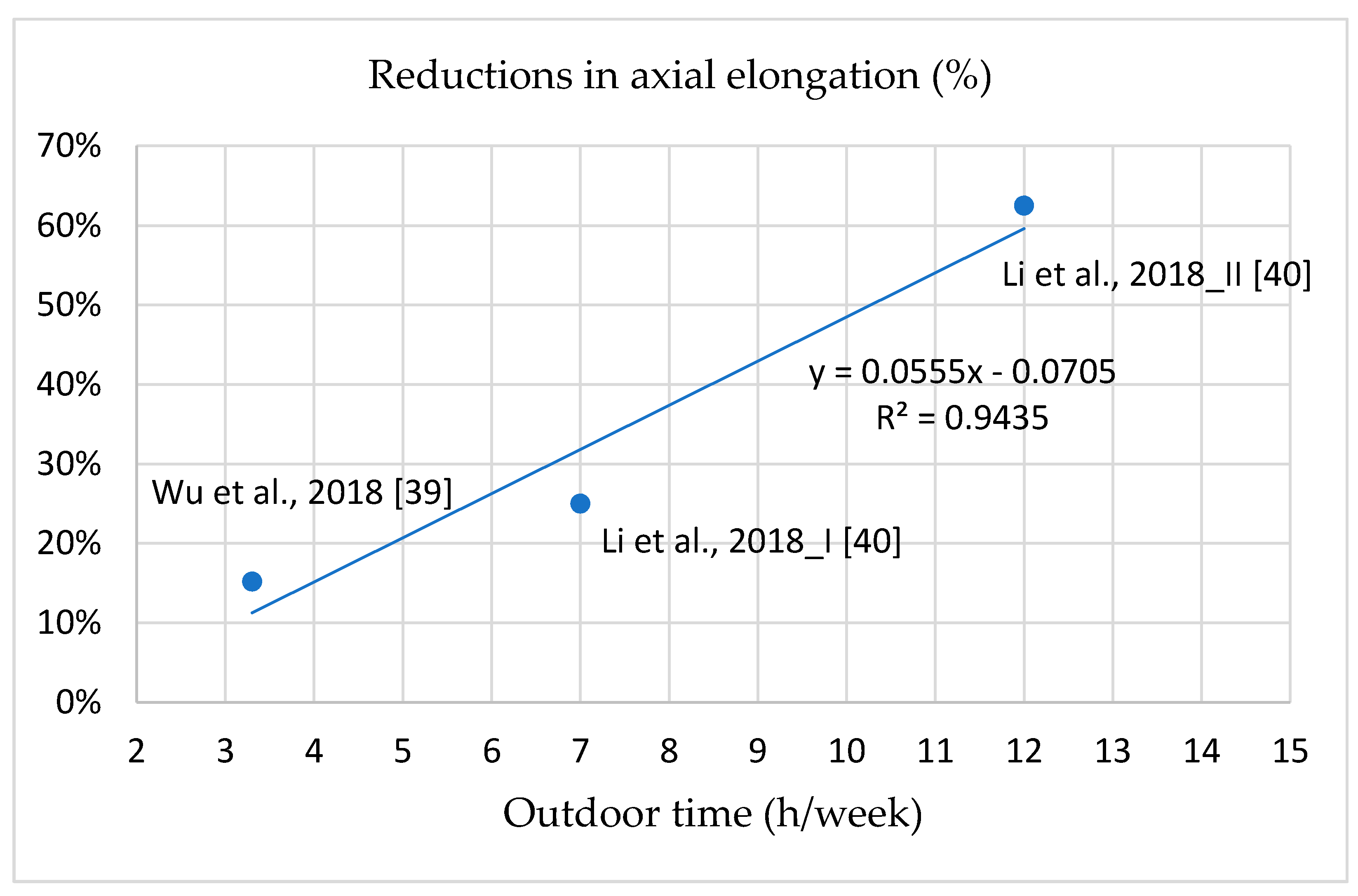
3.7. Dose–Response Effect of Intervention Programs
4. Discussion
4.1. Outdoor Light Exposure Prevented Myopia and Slowed Myopic Progression
4.2. Cross-Methodology Validated the Reduction in Myopia Incidence/Prevalence
4.3. Intervention Programs are Effective in Reducing Myopia Incidence and Progression
4.4. Outdoor Light Exposure Intervention Reduces Myopia Progression in Children with Myopia and Prevents Myopia Development in Children Without Myopia
4.5. Positive Dose–Response Effect of Intervention Programs on Myopia Incidence and Progression
4.6. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Pan, C.W.; Ramamurthy, D.; Saw, S.M. Worldwide prevalence and risk factors for myopia. Ophthalmic Physiol. Opt. J. Br. Coll. Ophthalmic Opt. 2012, 32, 3–16. [Google Scholar] [CrossRef] [PubMed]
- Dolgin, E. The myopia boom. Nature 2015, 519, 276–278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morgan, I.G.; Ohno-Matsui, K.; Saw, S.M. Myopia. Lancet 2012, 379, 1739–1748. [Google Scholar] [CrossRef]
- Holden, B.A.; Fricke, T.R.; Wilson, D.A.; Jong, M.; Naidoo, K.S.; Sankaridurg, P.; Wong, T.Y.; Naduvilath, T.J.; Resnikoff, S. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology 2016, 123, 1036–1042. [Google Scholar] [CrossRef] [PubMed]
- Marcus, M.W.; de Vries, M.M.; Junoy Montolio, F.G.; Jansonius, N.M. Myopia as a risk factor for open-angle glaucoma: A systematic review and meta-analysis. Ophthalmology 2011, 118, 1989–1994. [Google Scholar] [CrossRef] [PubMed]
- Flitcroft, D.I. The complex interactions of retinal, optical and environmental factors in myopia aetiology. Prog. Retin. Eye Res. 2012, 31, 622–660. [Google Scholar] [CrossRef] [PubMed]
- Saw, S.M.; Gazzard, G.; Shih-Yen, E.C.; Chua, W.H. Myopia and associated pathological complications. Ophthalmic Physiol. Opt. J. Br. Coll. Ophthalmic Opt. 2005, 25, 381–391. [Google Scholar] [CrossRef] [PubMed]
- Dudovitz, R.N.; Izadpanah, N.; Chung, P.J.; Slusser, W. Parent, teacher, and student perspectives on how corrective lenses improve child wellbeing and school function. Matern. Child Health J. 2016, 20, 974–983. [Google Scholar] [CrossRef]
- Kumaran, S.E.; Balasubramaniam, S.M.; Kumar, D.S.; Ramani, K.K. Refractive error and vision-related quality of life in South Indian children. Optom. Vis. Sci. Off. Publ. Am. Acad. Optom. 2015, 92, 272–278. [Google Scholar] [CrossRef]
- Holden, B.; Sankaridurg, P.; Smith, E.; Aller, T.; Jong, M.; He, M. Myopia, an underrated global challenge to vision: Where the current data takes us on myopia control. Eye 2014, 28, 142–146. [Google Scholar] [CrossRef]
- Lim, M.C.; Gazzard, G.; Sim, E.L.; Tong, L.; Saw, S.M. Direct costs of myopia in Singapore. Eye 2009, 23, 1086–1089. [Google Scholar] [CrossRef] [PubMed]
- Jones, L.A.; Sinnott, L.T.; Mutti, D.O.; Mitchell, G.L.; Moeschberger, M.L.; Zadnik, K. Parental history of myopia, sports and outdoor activities, and future myopia. Investig. Ophthalmol. Vis. Sci. 2007, 48, 3524–3532. [Google Scholar] [CrossRef] [PubMed]
- Rose, K.A.; Morgan, I.G.; Ip, J.; Kifley, A.; Huynh, S.; Smith, W.; Mitchell, P. Outdoor activity reduces the prevalence of myopia in children. Ophthalmology 2008, 115, 1279–1285. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.C.; Tsai, C.L.; Hu, C.H.; Yang, Y.H. Effects of outdoor activities on myopia among rural school children in Taiwan. Ophthalmic Epidemiol. 2010, 17, 338–342. [Google Scholar] [CrossRef] [PubMed]
- Guggenheim, J.A.; Northstone, K.; McMahon, G.; Ness, A.R.; Deere, K.; Mattocks, C.; Pourcain, B.S.; Williams, C. Time outdoors and physical activity as predictors of incident myopia in childhood: A prospective cohort study. Investig. Ophthalmol. Vis. Sci. 2012, 53, 2856–2865. [Google Scholar] [CrossRef]
- Guo, K.; Yang, D.Y.; Wang, Y.; Yang, X.R.; Jing, X.X.; Guo, Y.Y.; Zhu, D.; You, Q.S.; Tao, Y.; Jonas, J.B. Prevalence of myopia in schoolchildren in Ejina: The Gobi desert children eye study. Investig. Ophthalmol. Vis. Sci. 2015, 56, 1769–1774. [Google Scholar] [CrossRef]
- Cohen, Y.; Belkin, M.; Yehezkel, O.; Solomon, A.S.; Polat, U. Dependency between light intensity and refractive development under light-dark cycles. Exp. Eye Res. 2011, 92, 40–46. [Google Scholar] [CrossRef]
- Ashby, R.S.; Schaeffel, F. The effect of bright light on lens compensation in chicks. Investig. Ophthalmol. Vis. Sci. 2010, 51, 5247–5253. [Google Scholar] [CrossRef]
- Norton, T.T.; Siegwart, J.T., Jr. Light levels, refractive development, and myopia-a speculative review. Exp. Eye Res. 2013, 114, 48–57. [Google Scholar] [CrossRef]
- Feldkaemper, M.; Schaeffel, F. An updated view on the role of dopamine in myopia. Exp. Eye Res. 2013, 114, 106–119. [Google Scholar] [CrossRef]
- Ashby, R.; Ohlendorf, A.; Schaeffel, F. The effect of ambient illuminance on the development of deprivation myopia in chicks. Investig. Ophthalmol. Vis. Sci. 2009, 50, 5348–5354. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, C.S.; Megaw, P.; Devadas, M.; Morgan, I.G. Dopaminergic agents affect the ability of brief periods of normal vision to prevent form-deprivation myopia. Exp. Eye Res. 2007, 84, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Sherwin, J.C.; Reacher, M.H.; Keogh, R.H.; Khawaja, A.P.; Mackey, D.A.; Foster, P.J. The association between time spent outdoors and myopia in children and adolescents: A systematic review and meta-analysis. Ophthalmology 2012, 119, 2141–2151. [Google Scholar] [CrossRef] [PubMed]
- Xiong, S.; Sankaridurg, P.; Naduvilath, T.; Zang, J.; Zou, H.; Zhu, J.; Lv, M.; He, X.; Xu, X. Time spent in outdoor activities in relation to myopia prevention and control: A meta-analysis and systematic review. Acta Ophthalmol. 2017, 95, 551–566. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; Version 5.1.0; The Cochrane Collaboration: London, UK, 2011. [Google Scholar]
- Ottawa Hospital Research Institute. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp. html (accessed on 12 January 2019).
- Herzog, R.; Álvarez-Pasquin, M.J.; Díaz, C.; Del Barrio, J.L.; Estrada, J.M.; Gil, Á. Are healthcare workers’ intentions to vaccinate related to their knowledge, beliefs and attitudes? A systematic review. BMC Public Health 2013, 13, 154. [Google Scholar] [CrossRef] [PubMed]
- Chinn, S. A simple method for converting an odds ratio to effect size for use in meta-analysis. Stat. Med. 2000, 19, 3127–3131. [Google Scholar] [CrossRef]
- He, M.; Xiang, F.; Zeng, Y.; Mai, J.; Chen, Q.; Zhang, J.; Smith, W.; Rose, K.; Morgan, I.G. Effect of time spent outdoors at school on the development of myopia among children in China: A randomized clinical trial. Jama 2015, 314, 1142–1148. [Google Scholar] [CrossRef] [PubMed]
- Donovan, L.; Sankaridurg, P.; Ho, A.; Naduvilath, T.; Smith, E.L., 3rd; Holden, B.A. Myopia progression rates in urban children wearing single-vision spectacles. Optom. Vis. Sci. Off. Publ. Am. Acad. Optom. 2012, 89, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Ip, J.M.; Saw, S.M.; Rose, K.A.; Morgan, I.G.; Kifley, A.; Wang, J.J.; Mitchell, P. Role of near work in myopia: Findings in a sample of Australian school children. Investig. Ophthalmol. Vis. Sci. 2008, 49, 2903–2910. [Google Scholar] [CrossRef]
- Guo, Y.; Liu, L.J.; Xu, L.; Lv, Y.Y.; Tang, P.; Feng, Y.; Meng, M.; Jonas, J.B. Outdoor activity and myopia among primary students in rural and urban regions of Beijing. Ophthalmology 2013, 120, 277–283. [Google Scholar] [CrossRef]
- Zhou, R.; Zhang, W.F.; Yang, Y.; Li, Y.T.; Zhang, J.; Wang, W.P. Analysis of myopia prevalence and influencing factors among primary school students in the urban area of Lanzhou city. Int. Eye Sci. 2014, 14, 903–907. [Google Scholar]
- Zhou, Z.; Morgan, I.G.; Chen, Q.; Jin, L.; He, M.; Congdon, N. Disordered sleep and myopia risk among Chinese children. PloS ONE 2015, 10, e0121796. [Google Scholar] [CrossRef] [PubMed]
- French, A.N.; Morgan, I.G.; Mitchell, P.; Rose, K.A. Risk factors for incident myopia in Australian schoolchildren: The Sydney adolescent vascular and eye study. Ophthalmology 2013, 120, 2100–2108. [Google Scholar] [CrossRef] [PubMed]
- Yi, J.H.; Li, R.R. Influence of near-work and outdoor activities on myopia progression in school children. Chin. J. Contemp. Pediatrics 2011, 13, 32–35. [Google Scholar]
- Wu, P.C.; Tsai, C.L.; Wu, H.L.; Yang, Y.H.; Kuo, H.K. Outdoor activity during class recess reduces myopia onset and progression in school children. Ophthalmology 2013, 120, 1080–1085. [Google Scholar] [CrossRef] [PubMed]
- Jin, J.X.; Hua, W.J.; Jiang, X.; Wu, X.Y.; Yang, J.W.; Gao, G.P.; Fang, Y.; Pei, C.L.; Wang, S.; Zhang, J.Z.; et al. Effect of outdoor activity on myopia onset and progression in school-aged children in northeast China: The Sujiatun eye care study. BMC Ophthalmol. 2015, 15, 73. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.C.; Chen, C.T.; Lin, K.K.; Sun, C.C.; Kuo, C.N.; Huang, H.M.; Poon, Y.C.; Yang, M.L.; Chen, C.Y.; Huang, J.C.; et al. Myopia prevention and outdoor light intensity in a school-based cluster randomized trial. Ophthalmology 2018, 125, 1239–1250. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Liu, F.; Zhou, X.W.; Li, C.G.; Huang, H.H. Effect of outdoor exposure on myopia prevention among school-aged children. Chin. J. Sch. Health 2018, 39, 1227–1229. [Google Scholar]
- Dirani, M.; Tong, L.; Gazzard, G.; Zhang, X.; Chia, A.; Young, T.L.; Rose, K.A.; Mitchell, P.; Saw, S.M. Outdoor activity and myopia in Singapore teenage children. Br. J. Ophthalmol. 2009, 93, 997–1000. [Google Scholar] [CrossRef]
- Liao, C.C.; Chen, L.J.; Yu, J.H.; Lin, J.C. Refractive error change and its association with ocular and general parameters in junior high school students in Taiwan. Jpn. J. Ophthalmol. 2014, 58, 375–380. [Google Scholar] [CrossRef]
- Gwiazda, J.; Hyman, L.; Hussein, M.; Everett, D.; Norton, T.T.; Kurtz, D.; Leske, M.C.; Manny, R.; Marsh-Tootle, W.; Scheiman, M. A randomized clinical trial of progressive addition lenses versus single vision lenses on the progression of myopia in children. Investig. Ophthalmol. Vis. Sci. 2003, 44, 1492–1500. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Participants | Outcome: Myopia Incidence, Myopia Prevalence, SER, and Axial Length |
|---|---|---|
| Cross-sectional studies | ||
| Zhou et al., 2014 [33] | 823 children aged 6–12; Lanzhou City, Gansu Province, China. | Prevalence: OR = 0.937 (0.775–1.134) (h/day) transforms into OR = 0.991 (0.964–1.018) (h/week). |
| Zhou et al., 2015 [34] | 1902 urban primary school children; mean age: 9.8 years; Guangzhou, China. | Prevalence: OR = 0.97 (0.95–0.99), h/week. |
| Guo et al., 2013 [32] | 681 primary school students aged 8–13 years, mean age: 9.4 years; Beijing, China. | Prevalence: OR = 0.32 (0.21–0.48) (h/day) transforms into OR = 0.85 (0.8–0.902) (h/week). |
| Ip et al., 2008 [31] | 2339 school children; mean age: 12 y; Sydney, Australia. | Prevalence: OR = 0.97 (0.94–0.995), h/week. |
| Cohort studies | ||
| French et al. 2013 [35] | 2103 students; 6 and 12 years at baseline; 5–6-year follow-up period; Australia. | Incident myopia of younger cohort (6 years old): High 8.2% (n = 22) versus low 23.3% (n = 64), OR = 0.29 (0.18–0.5), h/week. Incident myopia of older cohort (12 years old): High 15.5% (n = 52) versus low 25.8% (n = 77), OR = 0.53 (0.36–0.78), h/week. Outdoor time per week is as follows: Younger cohort, low-level (<16 h/week) and high-level (>23 h/week); older cohort, low-level (<13.5 h/week) and high-level (>22.5 h/week). |
| Guggenheim et al., 2012 [15] | 2005 children aged ≥7 years who attended follow-up for an average of 4 years; United Kingdom. | Prediction of incident myopia: Time outdoors (high versus low), OR = 0.65 (0.45–0.96), h/week. Amount of outdoor time per week was considered high-level if the response was “3 or more h/day”; otherwise it was considered low-level. |
| Jones et al., 2007 [12] | 514 children aged 8 or 9 years; 5-year follow-up period; United States. | The nonmyopia group spent on average 11.65 ± 6.97 h/week (high-level) in sports and outdoor light exposure, whereas the future myopia group spent an average of 7.98 ± 6.54 h/week (low-level) outdoors. Outdoor time (nonmyopia versus myopia), OR = 0.91 (0.87–0.94), h/week. |
| Intervention studies | ||
| Yi & Li, 2011 [36] | 80 children with myopia aged 7–11 years; 2-year follow-up period; China. | An intervention group (n = 41) and a control group (n = 39). Myopia group: Intervention: −0.38 ± 0.15 D/year, n = 37; control: −0.52 ± 0.19 D/year, n = 29. |
| Wu et al., 2013 [37] | 571 children aged 7–11 years; 1-year follow-up period; Kaohsiung, Taiwan. | New cases of myopia onset, intervention group vs. control group: 8.41% (28/174) vs. 17.65% (42/121); p < 0.001. Nonmyopia group, intervention: −0.26 ± 0.61 D/year, n = 174; control, −0.44 ± 0.64 D/year, n = 121. Myopia group without atropine treatment: Intervention, −0.20 ± 0.69 D/year, n = 113; control, −0.37 ± 0.67 D/year, n = 94. Myopia group with atropine treatment: Intervention, −0.28 ± 0.57 D/year, n = 46; control, −0.31 ± 0.44 D/year, n = 23. Both myopia and nonmyopia group: Intervention, −0.25 ± 0.68 D/year, n = 333; control, −0.38 ± 0.69 D/year, n = 238. |
| Jin et al.,2015 [38] | 391 children; grades 1, 3, 5, and 7; urban and rural; 1-year follow-up; Northeast China. | Incidence of new myopia onset, the intervention group vs. the control group: 3.70% (8/214) vs. 8.50% (15/177), p = 0.048. Both myopia and nonmyopia group: Intervention, −0.10 ± 0.65 D/year, 0.16 ± 0.30 mm/year, n = 214; control, −0.27 ± 0.52 D/year, 0.21 ± 0.21 mm/year, n = 177. |
| He et al., 2015 [29] | 1903 children; mean age: 6.6 years; 3-year follow-up; Guangzhou, China. | Cumulative incidence rate, intervention group vs. control group: 30.4% (259/853) vs. 39.5% (287/726)/3 years transforms into 10.1% (86/853) vs. 13.2% (96/ 726)/year. Both myopia and nonmyopia group: Intervention: −1.42 (−1.58 to −1.27)/3 years transforms into −0.62 ± 1.01 D/year, n = 869; 0.95 (0.91 to 1.00) mm/3 years transforms into 0.41 ± 0.30 mm/year, n = 919. Control: −1.59 (−1.76 to −1.43)/3 years transforms into −0.69 ± 1.00 D, n = 740; 0.98 mm (0.94 to 1.03)/3 years transforms into 0.43 ± 0.30 mm/year, n = 929. |
| Wu et al., 2018 [39] | 693 children aged 6–7 years; 1-year follow-up; northern, central, southern, and western Taiwan. | Incidence of new myopia onset in the intervention group was less than that in the control group (14.47% vs. 17.40%), and risk of myopia was 35% lower (OR = 0.65; 95% CI: 0.42–1.01; p = 0.054). Nonmyopia group: Intervention: −0.32 ± 0.43 D/year, 0.26 ± 0.18 mm/year, n = 235; control: −0.43 ± 0.75 D/year, 0.3 ± 0.32 mm/year, n = 386. Myopia group: Intervention: −0.57 ± 0.4 D/year, 0.45 ± 0.28 mm/year, n = 32; control: −0.79 ± 0.38 D/year, 0.6 ± 0.19 mm/year, n = 41. Both myopia and nonmyopia group: Intervention: −0.35 ± 0.58 D/year, n = 267; 0.28 ± 0.22 mm/year, n = 265; control: −0.47 ± 0.74 D/year, n = 426; 0.33 ± 0.35 mm/year, n = 423. |
| Li et al., 2018 [40] | 1076 children aged 6–8 years; 1-year follow-up; Wenzhou area, China. 366 participants in the control group, 357 participants in test Group I, and 353 participants in test Group II. | Cases of newly onset myopia, intervention groups vs. control group: 32 (32/357) (Group I), 20 (20/353) (Group II), 60 (60/366). Refractive error changes, axial changes Both myopia and nonmyopia, Group I: Intervention: −0.42 ± 0.39 D/year, 0.24 ± 0.17 mm/year, n = 357; control: −0.52 ± 0.45 D/year, 0.32 ± 0.21 mm/year, n = 366. Both myopia and nonmyopia group, Group II: Intervention: −0.16 ± 0.37 D/year, 0.12 ± 0.15 mm/year, n = 353; control: −0.52 ± 0.45 D/year, 0.32 ± 0.21 mm/year, n = 366. |
| Intervention Types | Outdoor Light Exposure Time at School (h/week) | The Reduction in Myopia Incidence (%) | The Reduction in SER (%) | The Reduction in Axial Elongation (%) | |
|---|---|---|---|---|---|
| Meta-Analysis | 50% | 32.9% | 24.9% | ||
| Li et al., 2018_II [40] | Intervention Group II had 7 h/week of exposure and an extra 5 h/week after school. | 12 | 69% | 69.2% | 62.5% |
| Wu et al., 2013 [37] | Total daily recess time was 80 min; total weekly recess time was 6.7 h. The control group did not have any special program during recess. Schools had 2 h of outdoor physical education per week. | 8.7 | 64% | 34.2% | |
| Li et al., 2018_I [40] | Intervention Group I had 7 h/week of exposure, including recess and physical education. | 7 | 50% | 23.1% | 25% |
| Wu et al., 2018 [39] | If children went outside the classroom during every recess, they would accumulate 200 min of outdoor time per 5-day school week. | 3.3 | 35% | 25.5% | 15.2% |
| He et al., 2015 [29] | An additional 40-min outdoor light exposure class was scheduled at the end of each school day. The study did not explain class recess time. | Unclear | 24% | 10.1% | 4.7% |
| Jin et al., 2015 [38] | The interventions were two additional 20-min recesses programs for outdoor light exposure. The study did not explain class recess time. | Unclear | 58% | 63% | 23.8% |
| Yi & Li, 2011 [36] | The children in the intervention group had near and middle vision exposure of >30 h/week and more outdoor light exposure than 14–15 h/week. The study did not explain class recess time. | Unclear | 26.9% |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ho, C.-L.; Wu, W.-F.; Liou, Y.M. Dose–Response Relationship of Outdoor Exposure and Myopia Indicators: A Systematic Review and Meta-Analysis of Various Research Methods. Int. J. Environ. Res. Public Health 2019, 16, 2595. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16142595
Ho C-L, Wu W-F, Liou YM. Dose–Response Relationship of Outdoor Exposure and Myopia Indicators: A Systematic Review and Meta-Analysis of Various Research Methods. International Journal of Environmental Research and Public Health. 2019; 16(14):2595. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16142595
Chicago/Turabian StyleHo, Ciao-Lin, Wei-Fong Wu, and Yiing Mei Liou. 2019. "Dose–Response Relationship of Outdoor Exposure and Myopia Indicators: A Systematic Review and Meta-Analysis of Various Research Methods" International Journal of Environmental Research and Public Health 16, no. 14: 2595. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16142595