Environmental and Occupational Exposure to Asbestos as a Result of Consumption and Use in Poland


Abstract
:1. Introduction
2. Materials and Methods
3. Results
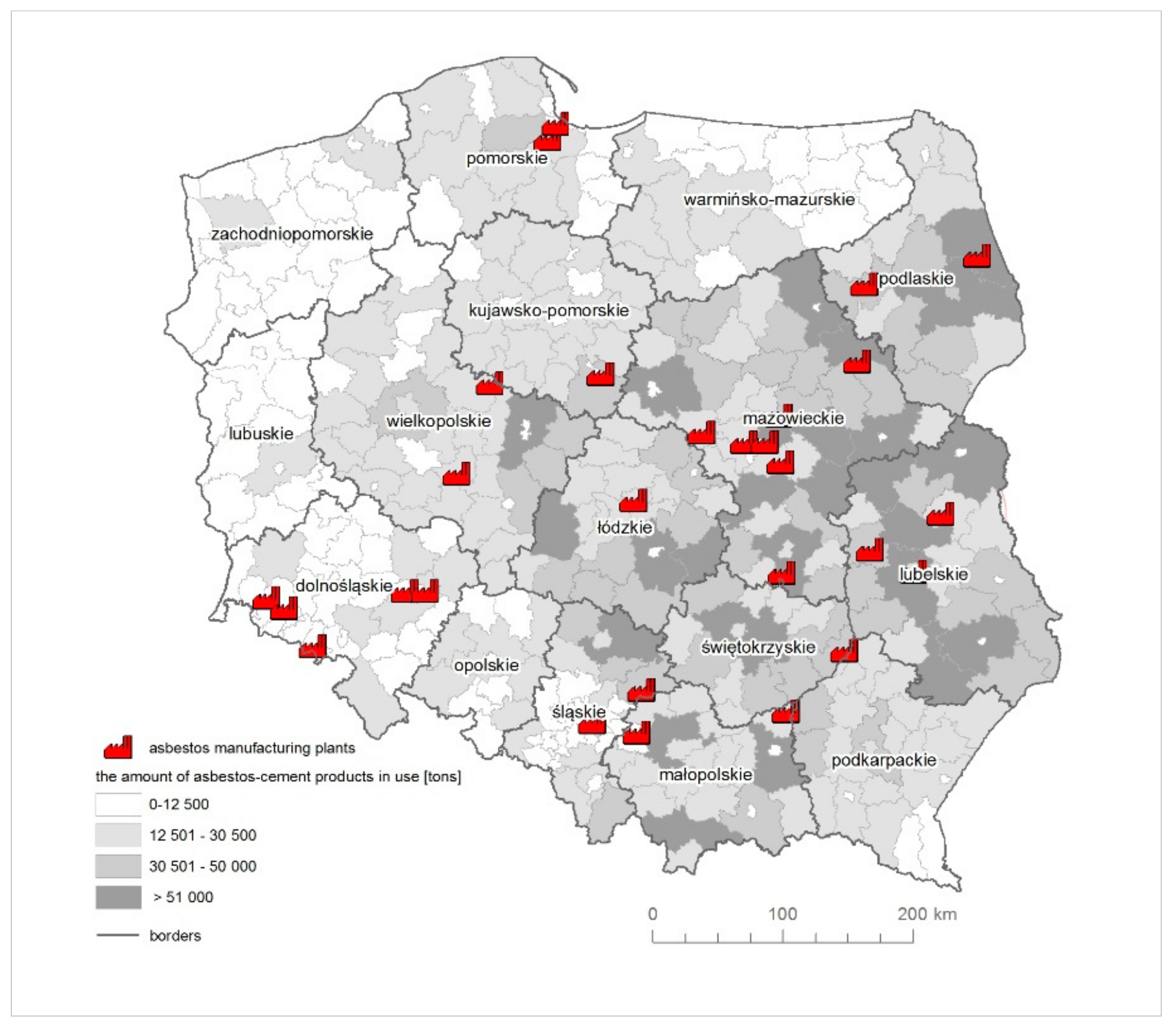
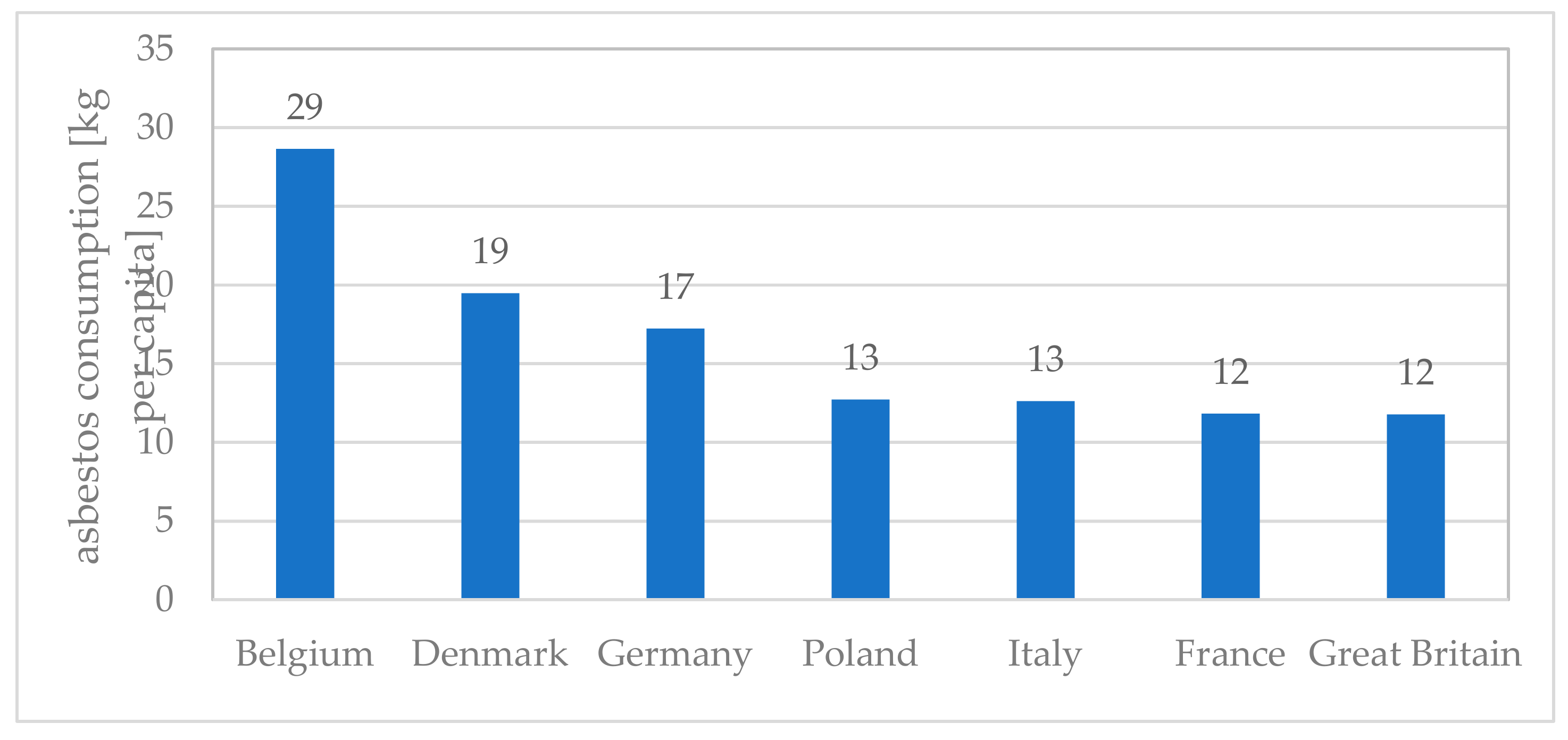
3.1. Asbestos Consumption and Manufacturing
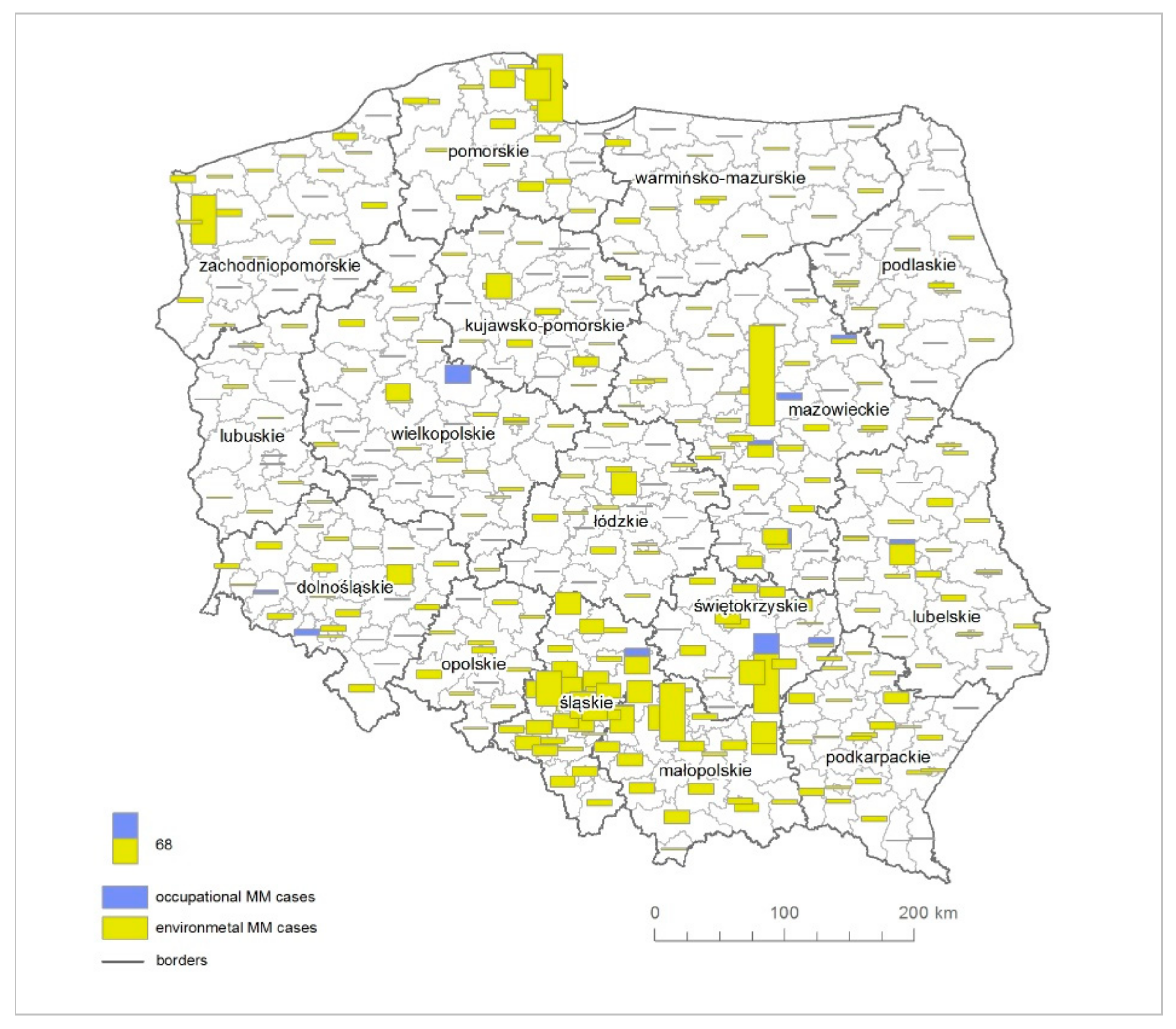
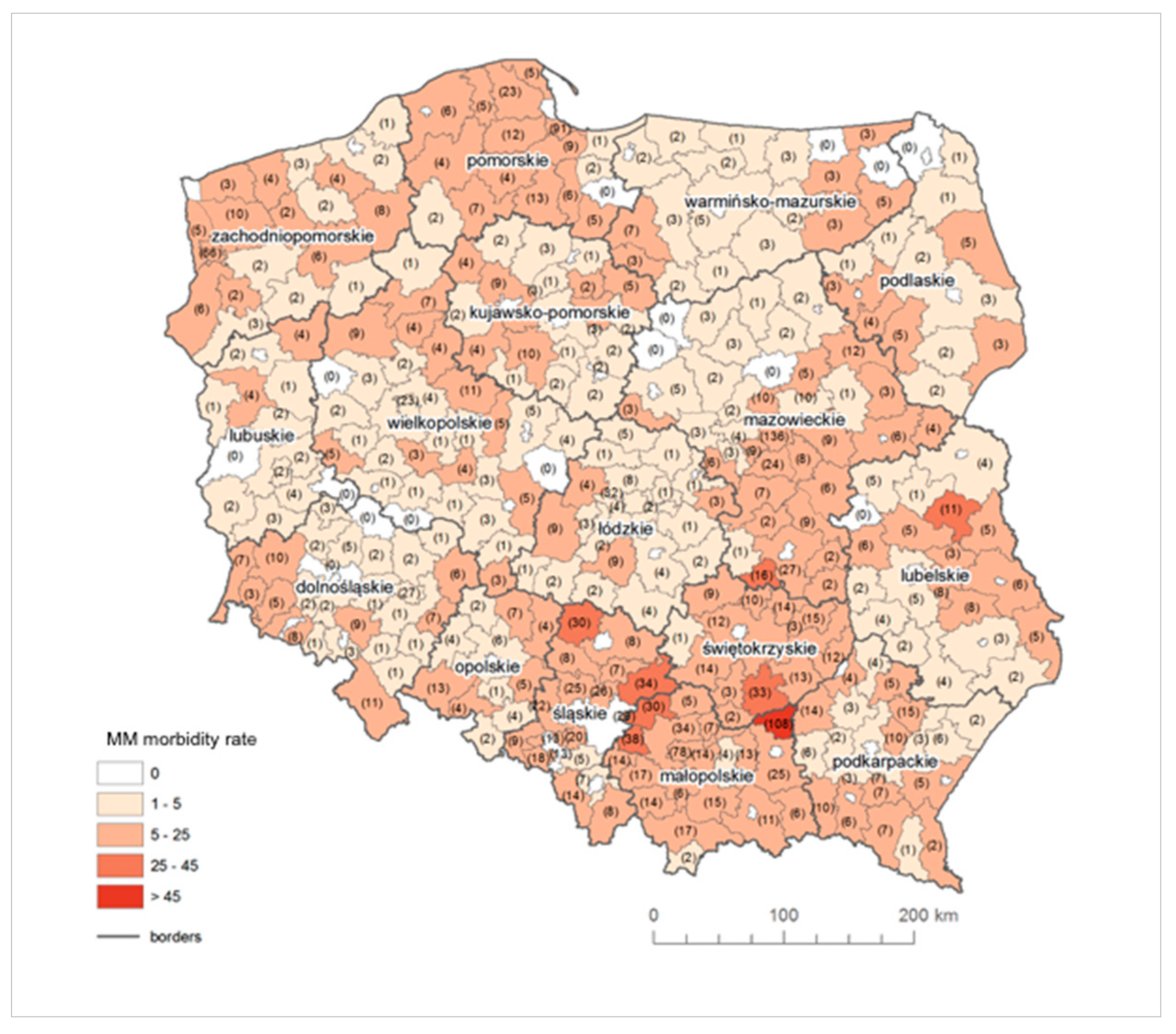
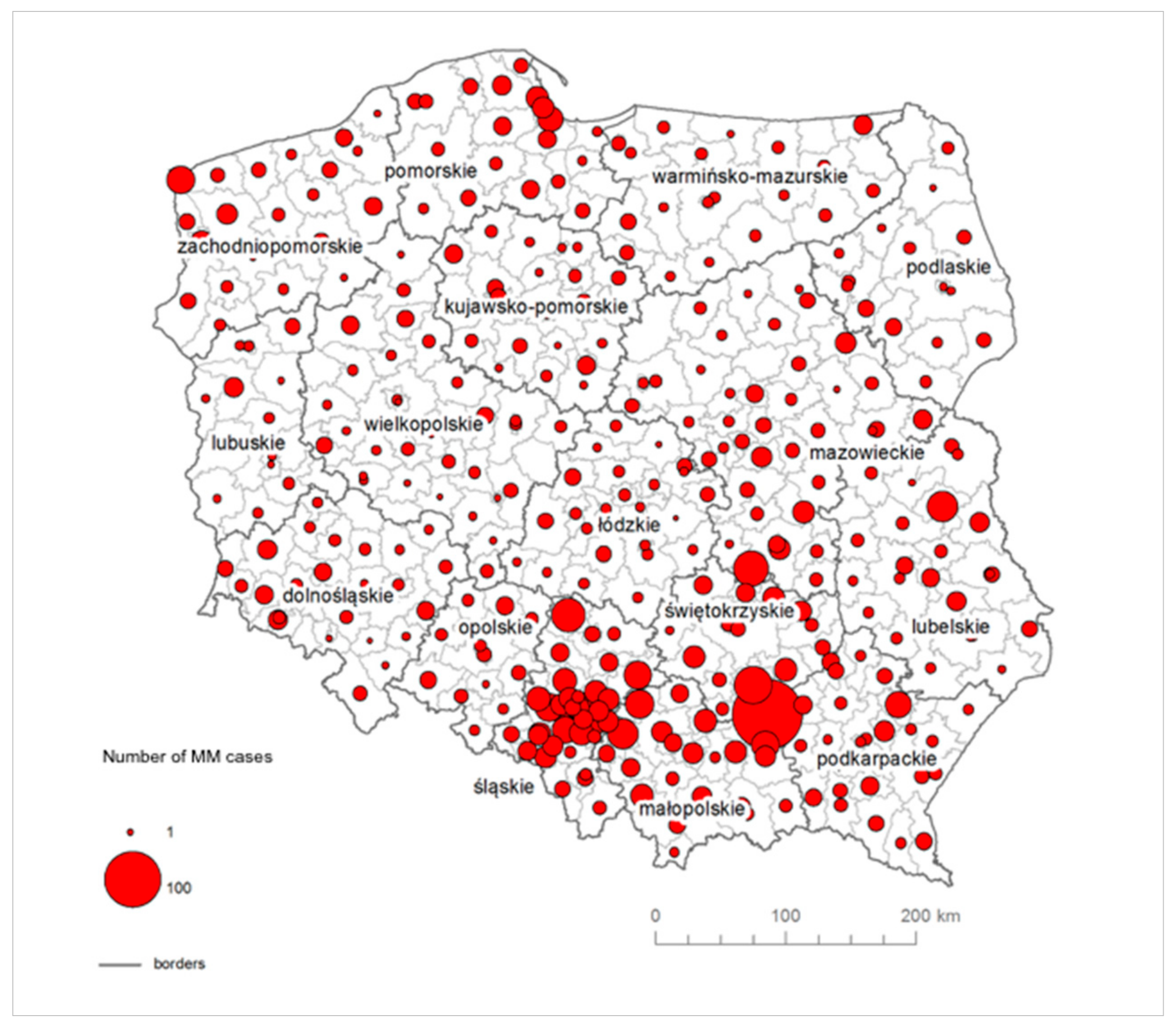
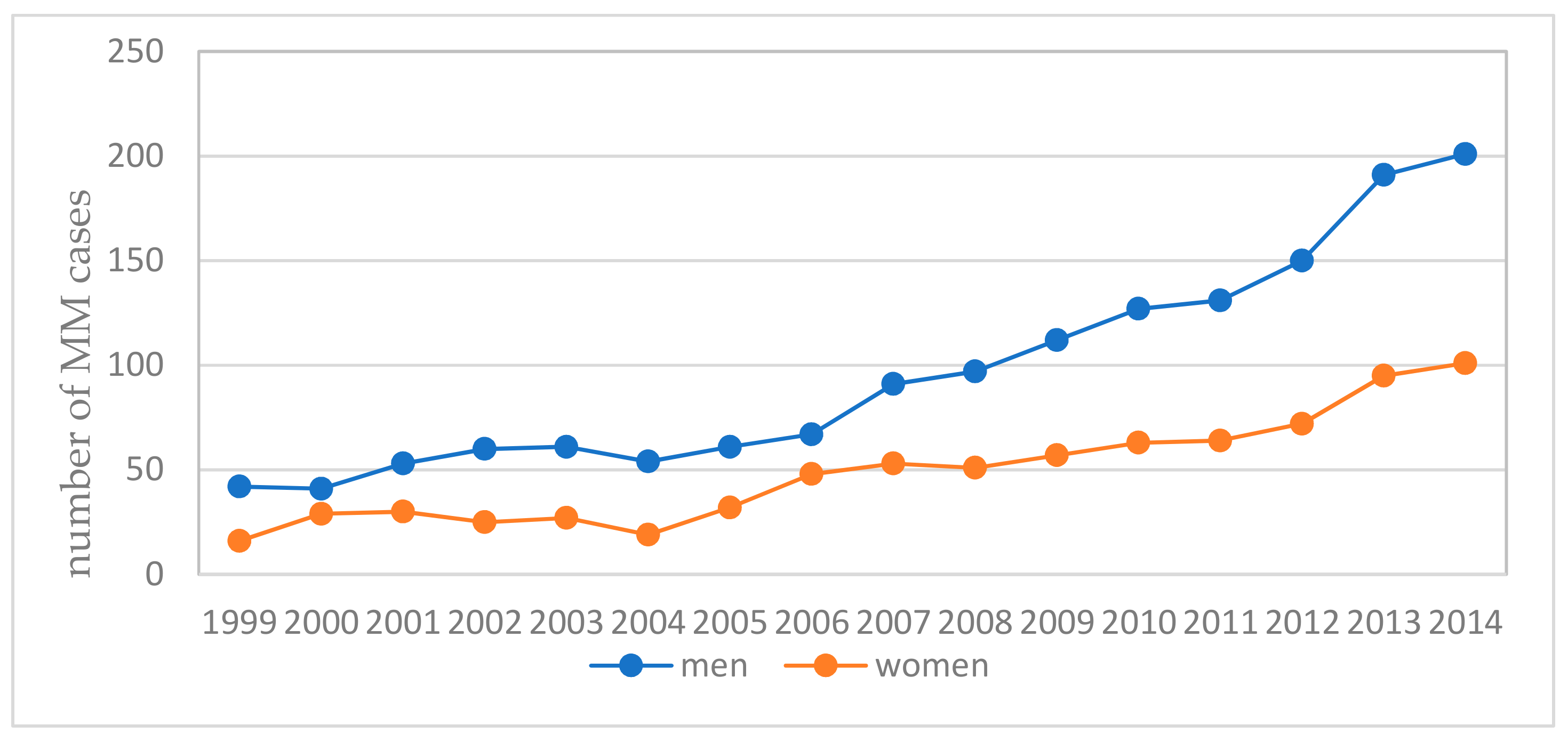
3.2. MM Cases in Counties
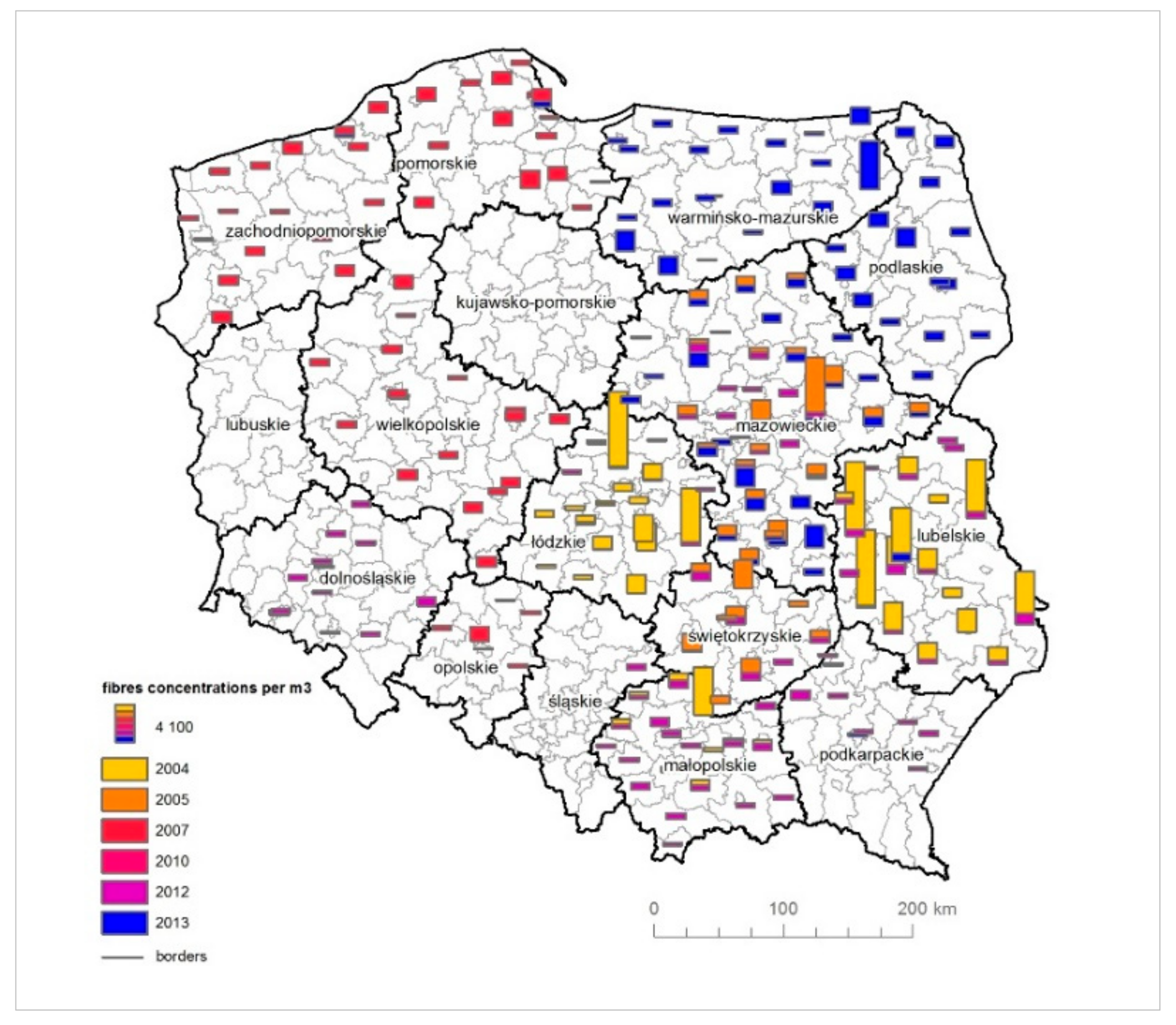
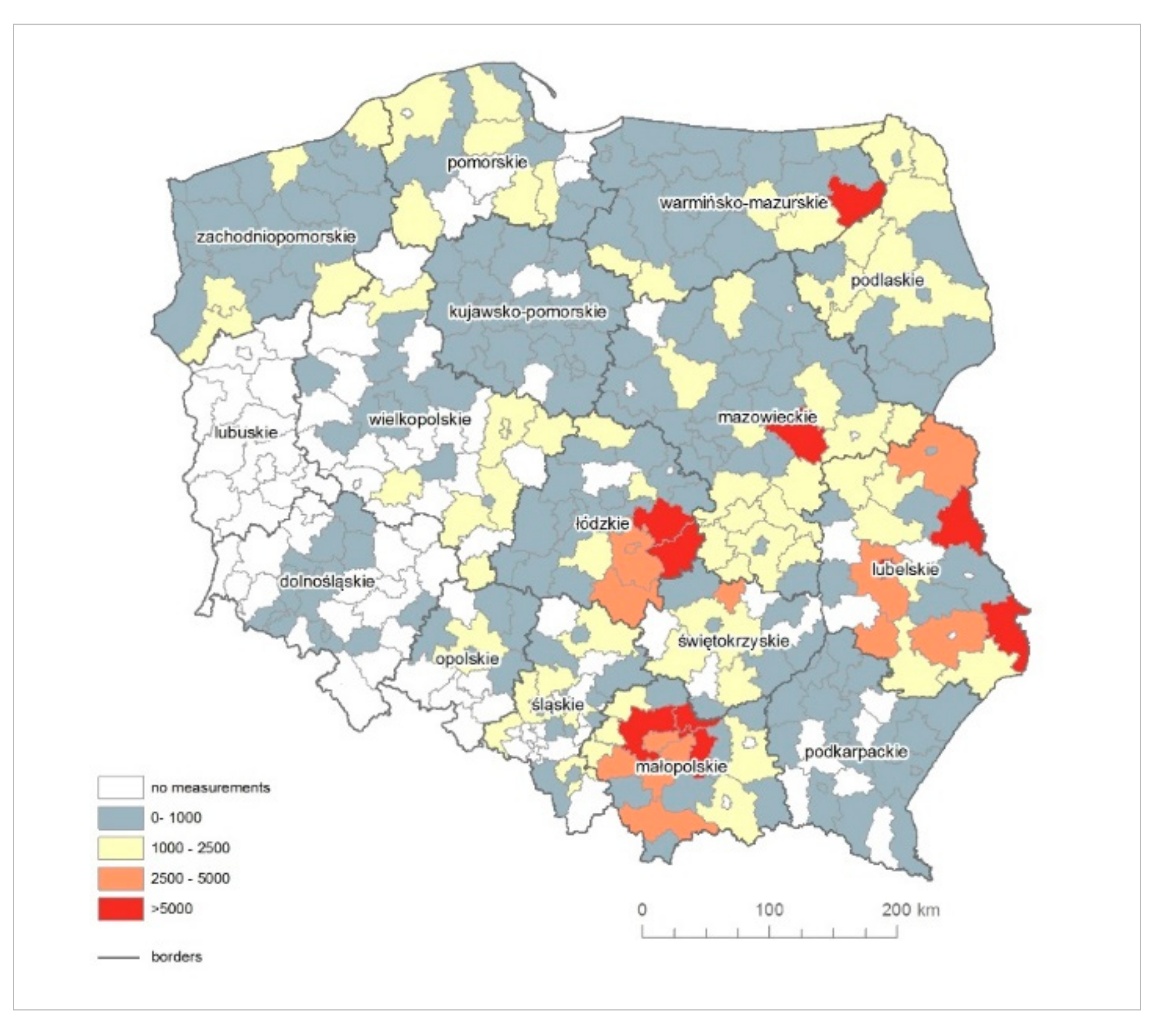
3.3. Asbestos Fibres Concentrations Measurements in Counties
3.4. Correlation of the Amount of Asbestos-Cement Products in Use in Relation to Asbestos Fibres Measurements and the Number of MM Cases
- -
- the average rate of the environmental MM morbidity rate (excluding MM occupational cases);
- -
- the average amount of asbestos products (in tons);
- -
- average number of asbestos fibres concentrations in the air per m3;
- -
- the average amount of asbestos products in use per person;
- -
- the number of plants that used asbestos in production;
- -
- percentage share of zones classified into class C, in which the specified criteria values have been exceeded for PM2.5 [55];
- -
- percentage share of zones classified to class C, in which the specified criteria values have been exceeded for PM10 [55].
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Hendry, N. The Geology, Occurrences, and Major Uses of Asbestos. Ann. N. Y. Acad. Sci. 1965, 132, 12–21. [Google Scholar] [CrossRef] [PubMed]
- Virta, R. Asbestos: Geology, Mineralogy, Mining, and Uses. Open-File Report 02-149. Available online: https://pubs.usgs.gov/of/2002/of02-149/ (accessed on 10 October 2015).
- Wilk, E.; Krówczyńska, M.; Pabjanek, P.; Mędrzycki, P. Estimation of the amount of asbestos-cement roofing in Poland. Waste Manag. Res. 2017, 35, 491–499. [Google Scholar] [CrossRef] [PubMed]
- Statistical Yearbook of Foreign Trade for 1958; GUS: Warszawa, Poland, 1959.
- Statistical Yearbook of Foreign Trade for 1965; GUS: Warszawa, Poland, 1966.
- Statistical Yearbook of Foreign Trade for 1967; GUS: Warszawa, Poland, 1968.
- Statistical Yearbook of Foreign Trade for 1970; GUS: Warszawa, Poland, 1971.
- Statistical Yearbook of Foreign Trade for 1971; GUS: Warszawa, Poland, 1972.
- Statistical Yearbook of Foreign Trade for 1976; GUS: Warszawa, Poland, 1977.
- Statistical Yearbook of Foreign Trade for 1978; GUS: Warszawa, Poland, 1979.
- Statistical Yearbook of Foreign Trade for 1980; GUS: Warszawa, Poland, 1981.
- Statistical Yearbook of Foreign Trade for 1981; GUS: Warszawa, Poland, 1982.
- Statistical Yearbook of Foreign Trade for 1985; GUS: Warszawa, Poland, 1988.
- Statistical Yearbook of Foreign Trade for 1987; GUS: Warszawa, Poland, 1989.
- Statistical Yearbook of Foreign Trade for 1989; GUS: Warszawa, Poland, 1990.
- Statistical Yearbook of Foreign Trade for 1990; GUS: Warszawa, Poland, 1991.
- Statistical Yearbook of Foreign Trade for 1991; GUS: Warszawa, Poland, 1992.
- Statistical Yearbook of Foreign Trade for 1992; GUS: Warszawa, Poland, 1993.
- Wilk, E.; Krówczyńska, M.; Zagajewski, B. Asbestos manufacturing plants in Poland. Misc. Geogr. 2014, 18, 53–58. [Google Scholar] [CrossRef] [Green Version]
- Krówczyńska, M.; Wilk, E.; Zagajewski, B. The Electronic Spatial Information System—Tools for the monitoring of asbestos in Poland. Misc. Geogr. 2014, 18, 59–64. [Google Scholar] [CrossRef]
- Murray, R. Asbestos: A chronology of its origins and health effects. Br. J. Ind. Med. 1990, 47, 361–365. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. World Health Organization website: www.who.int. Available online: http://www.who.int/news-room/fact-sheets/detail/asbestos-elimination-of-asbestos-related-diseases (accessed on 10 October 2016).
- Matsuzaki, H.; Maeda, M.; Lee, S.; Nishimura, Y.; Kumagai-Takei, N.; Hayashi, H.; Yamamoto, S.; Hatayama, T.; Kojima, Y.; Tabata, R.; et al. Asbestos-induced cellular and molecular alteration of immunocompetent cells and their relationship with chronic inflammation and carcinogenesis. J. Biomed. Biotechnol. 2012, 2012. [Google Scholar] [CrossRef] [PubMed]
- Carbone, M.; Yang, H. Molecular Pathways: Targeting Mechanisms of Asbestos and Erionite Carcinogenesis in Mesothelioma. Clin. Cancer Res. 2012, 18. [Google Scholar] [CrossRef]
- Hodgson, J.T.; Darnton, A. The quantitative risks of mesothelioma and lung cancer in relation to asbestos exposure. Ann. Occup. Hyg. 2000, 44, 565–601. [Google Scholar] [CrossRef]
- Berman, D.W.; Crump, K.S. A meta-analysis of asbestos-related cancer risk that addresses fiber size and mineral type. Crit. Rev. Toxicol. 2008, 38, 49–73. [Google Scholar] [CrossRef]
- Selikoff, I.J.; Hammond, E.C.; Seidman, H. Latency of asbestos disease among insulation workers in the United States and Canada. Cancer 1980, 46, 2340–2736. [Google Scholar] [CrossRef]
- Yates, D.H.; Corrin, B.; Stidolph, P.N.; Browne, K. Malignant mesothelioma in South East England: Clinicopathological experience of 272 cases. Thorax 1997, 52, 507–512. [Google Scholar] [CrossRef] [PubMed]
- Lanphear, B.P.; Buncher, C.R. Latent period for malignant mesothelioma of occupational origin. J. Occup. Med. 1992, 34, 718–721. [Google Scholar] [PubMed]
- Camus, M.; Siemiatycki, J.; Meek, B. Nonoccupational exposure to chrysotile asbestos and the risk of lung cancer. N. Eng. J. Med. 1998, 338, 1565–1571. [Google Scholar] [CrossRef] [PubMed]
- McDonald, A.D.; Case, B.W.; Churg, A.; Dufresne, A.; Gibbs, G.W.; Sébastien, P.; McDonald, J.C. Mesothelioma in Quebec chrysotile miners and millers: Epidemiology and aetiology. Ann. Occup. Hyg. 1997, 41, 707–719. [Google Scholar] [CrossRef]
- Nicholson, W.J.; Perkel, G.; Selikoff, I.J. Occupational exposure to asbestos: Population at risk and projected mortality-1980–2030. Am. J. Ind. Med. 1982, 3, 259–311. [Google Scholar] [CrossRef] [PubMed]
- Ferrante, D.; Mirabelli, D.; Tunesi, S.; Terracini, B.; Magnani, C. Pleural mesothelioma and occupational and non-occupational asbestos exposure: A case-control study with quantitative risk assessment. Occup. Environ. Med. 2016, 73, 147–153. [Google Scholar] [CrossRef]
- Mensi, C.; De Matteis, S.; Dallari, B.; Riboldi, L.; Bertazzi, P.A.; Consonni, D. Incidence of mesothelioma in Lombardy, Italy: Exposure to asbestos, time patterns and future projections. Occup. Environ. Med. 2016, 73, 607–613. [Google Scholar] [CrossRef]
- Hillerdal, G. Mesothelioma: Cases associated with non-occupational and low dose exposures. Occup. Environ. Med. 1999, 56, 505–513. [Google Scholar] [CrossRef]
- Regulation of the Minister of Economy of December 13, 2010 on the requirements for the use of asbestos-containing products and the use and treatment of installations or equipment in which asbestos-containing products have been or are used. J. Law 2011, 8, 31. Available online: http://isap.sejm.gov.pl/isap.nsf/DocDetails.xsp?id=WDU20110080031 (accessed on 26 February 2018).
- Krówczyńska, M.; Wilk, E.; Pabjanek, P.; Zagajewski, B.; Meuleman, K. Mapping asbestos-cement roofing with the use of APEX hyperspectral airborne imagery: Karpacz area, Poland—A case study. Misc. Geogr. 2016, 20, 41–46. [Google Scholar] [CrossRef]
- Fiumi, L.; Tocci, S.; Meoni, C. Remote sensing and GIS for land use planning: An application for mapping asbestos cement roofing in Tiburtina, Rome, Italy. Int. J. Remote Sens. Geosci. (IJRSG) 2014, 3, 1–9. Available online: http://ijrsg.com/Files/ae004674-aae0-4eee-9bff-f390797fd2b6_IJRSG_13_01.pdf (accessed on 20 October 2018).
- Carlin, D.J.; Larson, T.C.; Pfau, J.C.; Gavett, S.H.; Shukla, A.; Miller, A.; Hines, R. Current Research and Opportunities to Address Environmental Exposures. Environ. Health Perspect. 2015, 123, 194–197. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, K.; Takahashi, K.; Karjalainen, A.; Wen, C.; Furuya, S.; Hoshuyama, T.; Todoroki, M.; Kiyomoto, Y.; Wilson, D.; Higashi, T.; et al. Recent Mortality from Pleural Mesothelioma, Historical Patterns of Asbestos Use, and Adoption of Bans: A Global Assessment. Environ. Health Perspect. 2008, 116, 1675–1680. [Google Scholar] [CrossRef] [PubMed]
- Krówczyńska, M.; Wilk, E. Asbestos Exposure and the Mesothelioma Incidence in Poland. Int. J. Environ. Res. Public Health 2018, 15, 1741. [Google Scholar] [CrossRef] [PubMed]
- Flanagan, D.M. Mineral Commodity Summaries. Asbestos; U.S. Geological Survey: Reston, VA, USA, 2016. Available online: https://minerals.usgs.gov/minerals/pubs/commodity/asbestos/myb1-2015-asbes.pdf (accessed on 19 June 2017).
- Flanagan, D.M. 2015 Minerals Yearbook. Asbestos; U.S. Geological Survey: Reston, VA, USA, 2016.
- Wojciechowska, U.; Didkowska, J. Zachorowania i Zgony na Nowotwory Złośliwe w Polsce. Krajowy Rejestr Nowotworów, Centrum Onkologii—Instytut im. Marii Skłodowskiej—Curie. Available online: http://onkologia.org.pl/raporty/ (accessed on 20 March 2019).
- Bilans Gospodarki Surowcami Mineralnymi w Polsce na tle Gospodarki Światowej (The Balance of Mineral Resources Management in POLAND and the Background of the Global Economy); Ministerstwo Ochrony Środowiska, Zasobów Naturalnych i Leśnictwa, Centrum Podstawowych problemów Gospodarki Surowcami Mineralnymi i Energią PAN: Kraków, Poland, 1992; pp. 14–19.
- Bilans Gospodarki Surowcami Mineralnymi w Polsce na tle Gospodarki Światowej (The Balance of Mineral Resources Management in POLAND and the Background of the Global Economy); Ministerstwo Ochrony Środowiska, Zasobów Naturalnych i Leśnictwa, Centrum Podstawowych problemów Gospodarki Surowcami Mineralnymi i Energią PAN: Kraków, Poland, 1994; pp. 14–19.
- Bilans Gospodarki Surowcami Mineralnymi w Polsce na tle Gospodarki Światowej (The Balance of Mineral Resources Management in POLAND and the Background of the Global Economy); Ministerstwo Ochrony Środowiska, Zasobów Naturalnych i Leśnictwa, Centrum Podstawowych problemów Gospodarki Surowcami Mineralnymi i Energią PAN: Kraków, Poland, 1995; pp. 14–19.
- Bilans Gospodarki Surowcami Mineralnymi w Polsce na tle Gospodarki Światowej (The Balance of Mineral Resources Management in POLAND and the Background of the Global Economy); Ministerstwo Ochrony Środowiska, Zasobów Naturalnych i Leśnictwa, Centrum Podstawowych problemów Gospodarki Surowcami Mineralnymi i Energią PAN: Kraków, Poland, 2002; pp. 14–19.
- Bilans Gospodarki Surowcami Mineralnymi w Polsce na tle Gospodarki Światowej (The Balance of Mineral Resources Management in POLAND and the Background of the Global Economy); Ministerstwo Ochrony Środowiska, Zasobów Naturalnych i Leśnictwa, Centrum Podstawowych problemów Gospodarki Surowcami Mineralnymi i Energią PAN: Kraków, Poland, 2003; pp. 14–19.
- Bilans Gospodarki Surowcami Mineralnymi w Polsce na tle Gospodarki Światowej (The Balance of Mineral Resources Management in POLAND and the Background of the Global Economy); Ministerstwo Ochrony Środowiska, Zasobów Naturalnych i Leśnictwa, Centrum Podstawowych problemów Gospodarki Surowcami Mineralnymi i Energią PAN: Kraków, Poland, 2004; pp. 14–19.
- Dyczek, J. Surface of Asbestos-cement (AC) Roof Sheets and Assessment of the Risk of Asbestos Release. In Proceedings of the International Seminar Held in AGH on Asbestos Risk Reduction and Measurement of Asbestos Fibre Concentration, Cracow, Poland, 28–29 September 2006; pp. 57–63. [Google Scholar]
- Świątkowska, B.; Szeszenia-Dąbrowska, N.; Wilczyńska, U. Medical monitoring of asbestos-exposed workers: Experience from Poland. Bull. World Health Organ. 2016, 94, 599–604. [Google Scholar] [CrossRef] [PubMed]
- Szeszenia-Dąbrowska, N.; Sobala, W.; Swiątkowska, B.; Stroszejn-Mrowca, G.; Wilczyńska, U. Environmental asbestos pollution—Situation in Poland. Int. J. Occup. Med. Environ. Health 2012, 25, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Krówczyńska, M.; Wilk, E. Spatial analysis of the exposure to asbestos and health care in Poland in 2004–2013. Geospat. Health 2018, 13. [Google Scholar] [CrossRef] [PubMed]
- Kobus, D.; Kostrzewa, J.; Iwanek, J.; Mitosek, G.; Parvi, R. Wyniki Pięcioletniej Oceny Jakości Powietrza w strefach w Polsce. Państwowy Monitoring Środowiska—Inspekcja Ochrony Środowiska. Available online: http://powietrze.gios.gov.pl/pjp/content/show/1000357 (accessed on 20 October 2018).
- Liu, B.; van Gerwen, M.; Bonassi, S.; Taioli, E. Epidemiology of Environmental Exposure and Malignant Mesothelioma. J. Thorac. Oncol. 2017, 12, 1031–1045. [Google Scholar] [CrossRef] [Green Version]
- Magnani, C.; Agudo, A.; Gonzalez, C.A.; Andrion, A.; Calleja, A.; Chelini, E.; Dalmasso, P.; Escolar, A.; Hernandez, S.; Ivaldi, C.; et al. Multicentric study on malignant pleural mesothelioma and non-occupational exposure to asbestos. Brit. J. Cancer 2000, 83, 104–111. [Google Scholar] [CrossRef] [Green Version]
- McDonald, C. Health Implications of Environmental Exposure to Asbestos. Environ. Health Perspect. 1985, 62, 319–328. [Google Scholar] [CrossRef]
- Lacourt, A.; Gramond, C.; Rolland, P.; Ducamp, S.; Audignon, S.; Astoul, P.; Chamming, S.; Gilg Soit Ilg, A.; Rinaldo, M.; Raherison, C.; et al. Occupational and non-occupational attributable risk of asbestos exposure for malignant pleural mesothelioma. Thorax 2014, 69, 532–539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noonan, C.W. Environmental asbestos exposure and risk of mesothelioma. Ann. Transl. Med. 2017, 5, 234. [Google Scholar] [CrossRef] [PubMed]
- Peto, J.; Decarli, A.; La Vecchia, C.; Levi, F.; Negri, E. The European mesothelioma epidemic. Brit. J. Cancer 1999, 79, 666–672. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magnani, C.; Terracini, B.; Ivaldi, C.; Botta, M.; Mancini, A.; Andrion, A. Pleural malignant mesothelioma and non-occupational exposure to asbestos in Casale Monferrato, Italy. Occup. Environ. Med. 1995, 52, 362–367. [Google Scholar] [CrossRef] [PubMed]
- Marsili, D.; Angelini, A.; Bruno, C.; Corfiati, M.; Marinaccio, A.; Silvestri, A.; Zona, A.; Comba, P. Asbestos Ban in Italy: A Major Milestone, Not the Final Cut. Int. J. Environ. Res. Public Health 2017, 14, 1379. [Google Scholar] [CrossRef] [PubMed]
- Baur, X. Asbestos-Related Disorders in Germany: Background, Politics, Incidence, Diagnostics and Compensation. Int. J. Environ. Res. Public Health 2017, 15, 143. [Google Scholar] [CrossRef] [PubMed]
- European Cancer Information System. Available online: https://ecis.jrc.ec.europa.eu/ (accessed on 28 May 2019).
- Kotela, I.; Bednarenko, M.; Wilk-Frańczuk, M.; Kotela, P.; Wołowiec, B.; Laskowicz, K. The effects of environmental exposition to asbestos dust on health. Przegląd Lek. 2010, 67, 107–109. [Google Scholar]
- Krzakowski, M.; Jassem, J.; Dziadziuszko, R.; Kowalski, D.M.; Olszewski, W.; Orłowski, T.; Rzyman, W.; Smoraczewska, M. Nowotwory złośliwe płuca i opłucnej [in:] Zalecenia postępowania diagnostyczno—Terapeutycznego w nowotworach złośliwych. Med. Gdańsk 2011, 1, 69–96. [Google Scholar]
- Rosario, C.M.; Lin, X.; Kamp, D.W. Mesothelioma—Update on Diagnostic Strategies. Clin. Pulm. Med. 2012, 19, 282–288. [Google Scholar] [CrossRef]
- Mensi, C.; Riboldi, L.; De Matteis, S.; Bertazzi, P.A.; Consonni, D. Impact of an asbestos cement factory on mesothelioma incidence: Global assessment of effects of occupational, familial, and environmental exposure. Environ. Int. 2015, 74, 191–199. [Google Scholar] [CrossRef]
- Pira, E.; Pelucchi, C.; Buffoni, L.; Palmas, A.; Turbiglio, M.; Negri, E.; Piolatto, P.G.; La Vecchia, C. Cancer mortality in a cohort of asbestos textile workers. Br. J. Cancer 2005, 92, 580–586. [Google Scholar] [CrossRef] [PubMed] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Province | MM Morbidity Rate | Average Quantity of Asbestos-Cement Products (tons) [3] | Average Value of the Asbestos Fibres Concentrations in the Air (per m3) | Asbestos-Cement Products per Person | Number of Asbestos Manufacturing Plants | % Zone C PM2.5 | % Zone C PM10 |
|---|---|---|---|---|---|---|---|
| Dolnośląskie | 4.71 | 9244 | 507.25 | 95 | 5 | 25% | 25% |
| Kujawsko-Pomorskie | 4.88 | 18,125 | 556.70 | 199 | 1 | 25% | 0% |
| Lubelskie | 6.38 | 39,842 | 2710.18 | 445 | 3 | 50% | 0% |
| Lubuskie | 3.43 | 7851 | n.m. | 108 | 0 | 0% | 0% |
| Łódzkie | 4.19 | 32,621 | 1643.60 | 313 | 1 | 100% | 0% |
| Małopolskie | 19.09 | 25,770 | 2240.56 | 168 | 2 | 50% | 50% |
| Mazowieckie | 6.63 | 36,272 | 1111.97 | 286 | 7 | 67% | 67% |
| Opolskie | 5.56 | 14,395 | 397.02 | 173 | 0 | 50% | 0% |
| Podkarpackie | 7.00 | 20,129 | 587.24 | 236 | 0 | 0% | 0% |
| Podlaskie | 4.05 | 31,707 | 1048.21 | 452 | 2 | 50% | 0% |
| Pomorskie | 8.27 | 13,633 | 904.44 | 118 | 2 | 0% | 0% |
| Śląskie | 14.11 | 12,968 | 1033.90 | 102 | 2 | 80% | 50% |
| Świętokrzyskie | 12.06 | 37,137 | 1176.83 | 412 | 1 | 0% | 60% |
| Warmińsko-Mazurskie | 4.45 | 10,304 | 1135.77 | 150 | 0 | 0% | 0% |
| Wielkopolskie | 3.71 | 19,963 | 816.98 | 201 | 2 | 67% | 0% |
| Zachodniopomorskie | 7.35 | 8679 | 777.09 | 106 | 0 | 0% | 0% |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krówczyńska, M.; Wilk, E. Environmental and Occupational Exposure to Asbestos as a Result of Consumption and Use in Poland. Int. J. Environ. Res. Public Health 2019, 16, 2611. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16142611
Krówczyńska M, Wilk E. Environmental and Occupational Exposure to Asbestos as a Result of Consumption and Use in Poland. International Journal of Environmental Research and Public Health. 2019; 16(14):2611. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16142611
Chicago/Turabian StyleKrówczyńska, Małgorzata, and Ewa Wilk. 2019. "Environmental and Occupational Exposure to Asbestos as a Result of Consumption and Use in Poland" International Journal of Environmental Research and Public Health 16, no. 14: 2611. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16142611