Scoping Review of Climate Change and Health Research in the Philippines: A Complementary Tool in Research Agenda-Setting


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
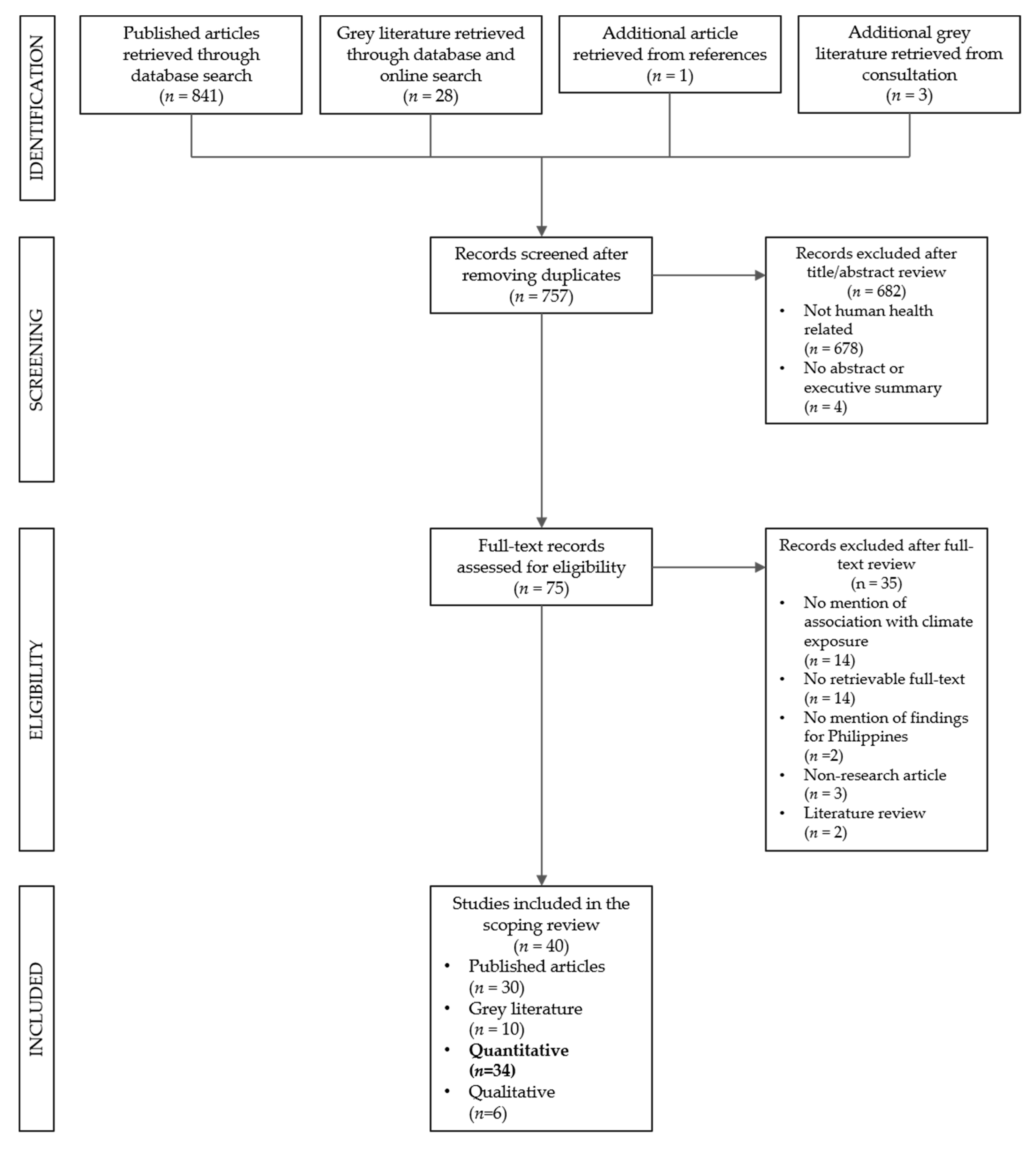
2.3. Screening
2.4. Characterization
2.5. Consultation
2.6. Data Analysis
2.7. Ethical Considerations
3. Results
3.1. General Characteristics
3.2. Methodologies
3.3. Findings
3.4. Challenges and Recommendations
3.5. Research Themes
4. Discussion
4.1. Research Gaps and Priorities
4.2. Limitations
4.3. Research Agenda-Setting
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Cruz, R.V.O.; Aliño, P.M.; Cabrera, O.C.; David, C.P.C.; David, L.T.; Lansigan, F.P.; Lasco, R.D.; Licuanan, W.R.Y.; Lorenzo, F.M.; Mamauag, S.S.; et al. 2017 Philippine Climate Change Assessment: Impacts, Vulnerabilities and Adaptation; The Oscar M. Lopez Center for Climate Change Adaptation and Disaster Risk Management Foundation, Inc. and Climate Change Commission: Quezon City, Philippines, 2017; ISSN 2508–089X. [Google Scholar]
- Cruz, R.V.; Harasawa, H.; Lal, M.; Wu, S.; Anokhin, Y.; Punsalmaa, B.; Honda, Y.; Jafari, M.; Li, C.; Huu Ninh, N. Asia. In Climate Change 2007: Impacts, Adaptation and Vulnerability; Contribution of Working Group II to the Fourth Assessment Report of the Intergovernmental Panel on Climate Change; Parry, M.L., Canziani, O.F., Palutikof, J.P., van der Linden, P.J., Hanson, C.E., Eds.; Cambridge University Press: Cambridge, UK, 2007; pp. 469–506. ISBN 978 0521 88010-7. [Google Scholar]
- David, C.P.; Racoma, B.A.; Gonzales, J.; Clutario, M.V. A manifestation of climate change? A look at Typhoon Yolanda in relation to the historical tropical cyclone archive. Sci. Diliman 2013, 25, 79–86. [Google Scholar]
- Climate Change Commission. Climate expenditures in the GAA by National Climate Change Action Plan Strategic Priority. 2015. Available online: https://data.gov.ph/dataset/climate-expenditures-gaa-national-climate-change-action-plan-strategic-priority (accessed on 29 May 2019).
- Philippine National Research Health System. National Unified Health Research Agenda 2017–2022. Available online: http://www.healthresearch.ph/index.php/nuhra1 (accessed on 29 May 2019).
- Montesanti, S.; Robinson-Vollman, A.; Green, L.A. Designing a framework for primary health care research in Canada: A scoping literature review. BMC Fam. Pract. 2018, 19, 144. [Google Scholar] [CrossRef] [PubMed]
- Ajumobi, O.; Uhomoibhi, P.; Onyiah, P.; Babalola, O.; Sharafadeen, S.; Ughasoro, M.D.; Adamu, A.M.; Odeyinka, O.; Orimogunje, T.; Maikore, I.; et al. Setting a Nigeria national malaria operational research agenda: The process. BMC Health Serv. Res. 2018, 18, 459. [Google Scholar] [CrossRef] [PubMed]
- Woodward, A.; Sondorp, E.; Witter, S.; Martineau, T. Health systems research in fragile and conflict-affected states: A research agenda-setting exercise. Health Res. Policy Syst. 2016, 14, 51. [Google Scholar] [CrossRef] [PubMed]
- Olding, M.; McMillan, S.E.; Reeves, S.; Schmitt, M.H.; Puntillo, K.; Kitto, S. Patient and family involvement in adult critical and intensive care settings: A scoping review. Health Expect. 2016, 19, 1183–1202. [Google Scholar] [CrossRef] [PubMed]
- Hosking, J.; Campbell-Lendrum, D. How well does climate change and human health research match the demands of policymakers? A scoping review. Environ. Health Perspect. 2012, 120, 1076. [Google Scholar] [CrossRef]
- Herlihy, N.; Bar-Hen, A.; Verner, G.; Fischer, H.; Sauerborn, R.; Depoux, A.; Flahault, A.; Schütte, S. Climate change and human health: What are the research trends? A scoping review protocol. BMJ Open 2016, 6, e012022. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Smith, K.R.; Woodward, A.; Campbell-Lendrum, D.; Chadee, D.D.; Honda, Y.; Liu, Q.; Olwoch, J.M.; Revich, B.; Sauerborn, R. Human health: Impacts, adaptation, and co-benefits. In Climate Change 2014: Impacts, Adaptation, and Vulnerability. Part A: Global and Sectoral Aspects, Contribution of Working Group II to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change; Field, C.B., Barros, V.R., Dokken, D.J., Mach, K.J., Mastrandrea, M.D., Bilir, T.E., Chatterjee, M., Ebi, K.L., Estrada, Y.O., Genova, R.C., et al., Eds.; Cambridge University Press: Cambridge, UK; New York, NY, USA, 2014; pp. 709–754. [Google Scholar]
- Seposo, X.T.; Dang, T.N.; Honda, Y. How Does Ambient Air Temperature Affect Diabetes Mortality in Tropical Cities? Int. J. Environ. Res. Public Health 2017, 14, 385. [Google Scholar] [CrossRef]
- Seposo, X.T.; Dang, T.N.; Honda, Y. Effect modification in the temperature extremes by mortality subgroups among the tropical cities of the Philippines. Glob. Health Action 2016, 9, 31500. [Google Scholar] [CrossRef]
- Kamigaki, T.; Chaw, L.; Tan, A.G.; Tamaki, R.; Alday, P.P.; Javier, J.B.; Olveda, R.M.; Oshitani, H.; Tallo, V.L. Seasonality of influenza and respiratory syncytial viruses and the effect of climate factors in subtropical–tropical asia using influenza-like illness surveillance data, 2010–2012. PLoS ONE 2016, 11, e0167712. [Google Scholar] [CrossRef] [PubMed]
- Khormi, H.M.; Kumar, L. Future malaria spatial pattern based on the potential global warming impact in South and Southeast Asia. Geospat. Health 2016, 11, 290–298. [Google Scholar] [CrossRef] [PubMed]
- Sumi, A.; Telan, E.F.; Chagan-Yasutan, H.; Piolo, M.B.; Hattori, T.; Kobayashi, N. Effect of temperature, relative humidity and rainfall on dengue fever and leptospirosis infections in Manila, the Philippines. Epidemiol. Infect. 2017, 145, 78–86. [Google Scholar] [CrossRef] [PubMed]
- Edillo, F.E.; Sarcos, J.R.; Sayson, S.L. Natural vertical transmission of dengue viruses in Aedes aegypti in selected sites in Cebu City, Philippines. J. Vector Ecol. 2015, 40, 282–291. [Google Scholar] [CrossRef] [PubMed]
- Van Panhuis, W.G.; Choisy, M.; Xiong, X.; Chok, N.S.; Akarasewi, P.; Iamsirithaworn, S.; Lam, S.K.; Chong, C.K.; Lam, F.C.; Phommasak, B.; et al. Region-wide synchrony and traveling waves of dengue across eight countries in Southeast Asia. Proc. Natl. Acad. Sci. USA 2015, 112, 13069–13074. [Google Scholar] [CrossRef] [Green Version]
- Magalhaes, R.J.S.; Salamat, M.S.; Leonardo, L.; Gray, D.J.; Carabin, H.; Halton, K.; McManus, D.P.; Williams, G.M.; Rivera, P.; Saniel, O.; et al. Mapping the risk of soil-transmitted helminthic infections in the Philippines. PLoS Negl. Trop. Dis. 2015, 9, e0003915. [Google Scholar] [CrossRef]
- Seposo, X.T.; Dang, T.N.; Honda, Y. Evaluating the effects of temperature on mortality in manila city (Philippines) from 2006–2010 using a distributed lag nonlinear model. Int. J. Environ. Res. Public Health 2015, 12, 6842–6857. [Google Scholar] [CrossRef]
- Buczak, A.L.; Baugher, B.; Babin, S.M.; Ramac-Thomas, L.C.; Guven, E.; Elbert, Y.; Koshute, P.T.; Velasco, J.M.S.; Roque, V.G., Jr.; Tayag, E.A.; et al. Prediction of high incidence of dengue in the Philippines. PLoS Negl. Trop. Dis. 2014, 8, e2771. [Google Scholar] [CrossRef]
- Paynter, S.; Yakob, L.; Simoes, E.A.; Lucero, M.G.; Tallo, V.; Nohynek, H.; Ware, R.S.; Weinstein, P.; Williams, G.; Sly, P.D. Using mathematical transmission modelling to investigated rivers of respiratory syncytial virus seasonality in children in the Philippines. PLoS ONE 2014, 9, e90094. [Google Scholar] [CrossRef]
- Paynter, S.; Weinstein, P.; Ware, R.S.; Lucero, M.G.; Tallo, V.; Nohynek, H.; Barnett, A.G.; Skelly, C.; Simoes, E.A.F.; Sly, P.D.; et al. Sunshine, rainfall, humidity and child pneumonia in the tropics: Time-series analyses. Epidemiol. Infect. 2013, 141, 1328–1336. [Google Scholar] [CrossRef]
- Natividad, F.F.; Buerano, C.C.; Lago, C.B.; Mapua, C.A.; de Guzman, B.B.; Seraspe, E.B.; Samentar, L.P.; Endo, T. Prevalence rates of Giardia and Cryptosporidium among diarrheic patients in the Philippines. Southeast Asian J. Trop. Med. Public Health 2008, 39, 991–999. [Google Scholar] [PubMed]
- Sia Su, G.L. Correlation of climatic factors and dengue incidence in Metro Manila, Philippines. AMBIO J. Hum. Environ. 2008, 37, 292–294. [Google Scholar] [CrossRef]
- Abucejo-Ladesma, E.; Simoes, E.A.; Lupisan, S.P.; Sombrero, L.T.; Quiambao, B.P.; Gozum, L.S.; Herva, E.; Ruutu, P.; Arivac Consortium. Serious community-acquired paediatric infections in rural Asia (Bohol Island, Philippines): Bacterial meningitis in children less than 5 years of age. Scand. J. Infect. Dis. 2007, 39, 983–989. [Google Scholar] [CrossRef] [PubMed]
- Limcangco, M.R.; Salole, E.G.; Armour, C.L. Epidemiology of Haemophilus influenzae type b meningitis in Manila, Philippines, 1994 to 1996. Pediatr. Infect. Dis. J. 2000, 19, 7–11. [Google Scholar] [CrossRef] [PubMed]
- San Pedro, M.C.; Walz, S.E. A comprehensive survey of pediatric diarrhea at a private hospital in Metro Manila. Southeast Asian J. Trop. Med. Public Health 1991, 22, 203–210. [Google Scholar] [PubMed]
- Cabrera, B.D. Reinfection and infection rates of ascariasis in relation to seasonal variation in the Philippines. Southeast Asian J. Trop. Med. Public Health 1984, 15, 394–401. [Google Scholar] [PubMed]
- Salvacion, A. Exploring Determinants of Child Malnutrition in Marinduque Island, Philippines. Human Ecol. 2017, 45, 853–863. [Google Scholar] [CrossRef]
- Opena, E.L.; Teves, F.G. Climate and the incidence of dengue fevers in Iligan City, the Philippines. Asia Pac. J. Soc. Sci. 2011, 2, 114–131. [Google Scholar]
- Dulay, A.V.; Bautista, J.R.; Teves, F.G. Climate change and incidence of dengue fever (DF) and dengue hemorrhagic fever (DHF) in Iligan City, Lanao del Norte, Philippines. Int. Res. J. Biol. Sci. 2013, 2, 37–41. [Google Scholar]
- Pasay, J.M.; Awa, A.L.; Ocapan, J.G. Incidence of dengue in Ozamiz City, Philippines. J. Multidiscip. Stud. 2013, 2, 62–85. [Google Scholar] [CrossRef]
- Seposo, X.T.; Dang, T.N.; Honda, Y. Exploring the effects of high temperature on mortality in four cities in the Philippines using various heat wave definitions in different mortality subgroups. Glob. Health Action 2017, 10, 1368969. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dela Cruz, A.C.; Lubrica, J.A.; Punzalan, B.V.; Martin, M.C. Forecasting dengue incidence in the National Capital Region, Philippines: Using time-series analysis with climate variables as predictors. Acta Manil. 2012, 60, 19–26. [Google Scholar]
- Lubos, L.C. Dengue incidence using climate variables as predictors. Asian J. Health 2015, 5, 1–11. [Google Scholar] [CrossRef]
- Adkins, H.J.; Escamilla, J.; Santiago, L.T.; Ranoa, C.; Echeverria, P.; Cross, J.H. Two-year survey of etiologic agents of diarrheal disease at San Lazaro Hospital, Manila, Republic of the Philippines. J. Clin. Microbiol. 1987, 25, 1143–1147. [Google Scholar] [PubMed]
- Saniel, M.C. Prospective study of diarrhea in infants and young children of a peri-urban Philippine community: Morbidity patterns and etiologies. Trans. Nat. Acad. Sci. Tech. Phil. 1986, 208, 183–187. [Google Scholar]
- Arcenas, A.L. Climate Change, Dengue and the Economy Ascertaining the Link between Dengue and Climatic Conditions. Discussion Paper, School of Economics, University of the Philippines, Quezon City, Philippines, 2016. [Google Scholar]
- Naragdao, M.A. The Association between Local Meteorological Factors and Hospital Admissions of Dengue Hemorrhagic Fever in Iloilo Province, Philippines. Master’s Thesis, Dalhousie University, Halifax, Nova Scotia, Canada, December 2001. [Google Scholar]
- Asian Development Bank. Accounting for Health Impacts of Climate Change; Asian Development Bank: Mandaluyong City, Philippines, 2011; ISBN 978-92-9092-360-2. [Google Scholar]
- Lorenzo, F.M. MDGF 1656: Conduct of Climate Change Vulnerability and Impact Assessment Framework, Development of a Monitoring and Evaluation Framework/System, and Compendium of Good and Innovative Climate Change Adaptation Practices; Institute of Health Policy and Development Studies: Manila, Philippines, 2011. [Google Scholar]
- Alcantara, M.; Caballeros, B.J.; Chuya, A.P.; Regala, A.M.; Sacdalan, D.R.; Santos, K.E. An ecologic study on the presumed impacts of climate change and seasonal patterns on acute respiratory infection and health service utilization in Nueva Ecija from 1999 to 2008. Undergraduate Degree Thesis, Ateneo de Manila University, Quezon City, Philippines, January 2010. [Google Scholar]
- Rarugal, A.; Roxas-Villanueva, R.M.; Tapang, G.A. Impact of climatic factors on acute bloody diarrhea, dengue and influenza-like illness incidences in the Philippines. In Proceedings of the GRASPA 2015 Conference, Bari, Italy, 15–16 June 2015. Abstract no. 3298. [Google Scholar]
- Philippine Atmospheric, Geophysical and Astronomical Services Administration (PAGASA). Documentation and Analysis of Impacts of and Responses to Extreme Climate Events; PAGASA: Quezon City, Philippines, 2001.
- Nissan, H.; Conway, D. From advocacy to action: Projecting the health impacts of climate change. PLoS Med. 2018, 15, e1002624. [Google Scholar] [CrossRef]
- Gao, J.; Kovats, S.; Vardoulakis, S.; Wilkinson, P.; Woodward, A.; Li, J.; Gu, S.; Liu, X.; Wu, H.; Wang, J.; et al. Public health co-benefits of greenhouse gas emissions reduction: A systematic review. Sci. Total Environ. 2018, 627, 388–402. [Google Scholar] [CrossRef]
- Banwell, N.; Rutherford, S.; Mackey, B.; Street, R.; Chu, C. Commonalities between disaster and climate change risks for health: A theoretical framework. Int. J. Environ. Res. Public Health 2018, 15, 538. [Google Scholar] [CrossRef]


{kind=link}
| Category | Keywords |
|---|---|
| Climate factors and health | (“climate” OR “climate change” OR “extreme weather” OR “global warming” OR “climate variability” OR “greenhouse gas” OR “rising temperature” OR “sea-level rising” OR “CO2”) AND (“health” OR “disease” OR “epidemiology” OR “air pollution” OR “water” OR “food” OR “nutrition” OR “vector”) |
| Location/study site | “Philippines” |
| Timeframe | “1980” to “2017” |
| Theme | Criteria |
|---|---|
| Vulnerability to Disease and Injury Due to Climate Variability and Climate Change | Studies that had findings on health vulnerabilities, such as socioeconomic status, age, and gender in relation to the effect of climate change. |
| Direct Impacts of Climate and Weather on Health | Studies with the aim of and results on associating the direct effects of climate change with health outcomes like mortality and diseases unmediated by the ecosystem. |
| Ecosystem-Mediated Impacts of Climate Change on Health Outcomes | Studies with the aim of and results on associating climate change with vector-borne, food- and water-borne, as well as air quality-related health outcomes. |
| Health Impacts Heavily Mediated through Human Institutions | Studies with the aim of and results on associating climate change with nutrition, occupational health, mental health, and violence and conflict. |
| Adaptation to Protect Health | Studies with the aim of and results on improving basic public health and health care services, as well as the formulation of adaptation policies and measures (including early warning systems) based on associated health impacts of climate change. |
| Co-benefits | Studies with the aim of and results related to mitigation measures and their benefits to health outcomes. |
| Characteristics | Number (n = 34) | References |
|---|---|---|
| Publication year | ||
| 2011–2017 | 23 | [14,15,16,17,18,19,20,21,22,23,24,25,32,33,34,35,36,37,38,41,43,44,46] |
| 2000–2010 | 7 | [26,27,28,29,42,45,47] |
| 1985–1999 | 4 | [30,31,39,40] |
| Type of paper | ||
| Research article | 27 | [14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40] |
| Technical report | 3 | [43,44,47] |
| Master’s thesis | 1 | [42] |
| Undergraduate thesis | 1 | [45] |
| Conference paper | 1 | [46] |
| Discussion paper | 1 | [41] |
| Health topic | ||
| Mosquito-borne diseases | 18 | [17,18,19,20,23,27,33,34,35,37,38,41,42,43,44,46,47] |
| Water-related diseases | 9 | [18,21,26,30,31,39,40,46,47] |
| Respiratory diseases | 8 | [15,16,22,24,25,36,45,46] |
| Other communicable diseases | 3 | [28,29,47] |
| Non-communicable diseases | 4 | [14,15,22,36] |
| Malnutrition | 1 | [32] |
| Study sites | ||
| City-level | 16 | [14,15,16,18,19,22,29,30,31,33,34,35,36,38,39,40] |
| Province-level | 7 | [24,25,28,32,42,44,45] |
| Region-level | 5 | [16,27,37,44,47] |
| Country-level | 8 | [17,20,21,23,26,41,43,46] |
| First author affiliation | ||
| Philippines | 20 | [19,26,27,28,29,30,31,32,33,34,35,37,38,40,41,43,44,47] |
| Japan | 6 | [14,15,16,18,22,36] |
| USA | 3 | [20,23,39] |
| Australia | 3 | [21,24,25] |
| Canada | 1 | [42] |
| Saudi Arabia | 1 | [17] |
| Funding source | ||
| Foreign-based | 18 | [14,15,16,18,20,21,22,23,24,25,26,28,30,31,36,39,42,44] |
| Philippine-based | 2 | [19,39] |
| No statement of funding | 15 | [17,27,29,32,33,34,35,37,38,40,41,43,45,46,47] |
| Characteristics | Number (n = 34) | References |
|---|---|---|
| Study design | ||
| Time-series analysis | 27 | [14,15,16,18,19,20,22,25,27,28,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47] |
| Cross-sectional | 3 | [26,29,30] |
| Process-based modeling | 2 | [17,24] |
| Bayesian modeling | 1 | [21] |
| Fuzzy association rule mining | 1 | [23] |
| Case-crossover | 1 | [25] |
| Exposure variables | ||
| Meteorological parameters | 27 | [16,17,18,19,20,21,23,24,25,27,28,31,32,33,34,35,37,38,39,40,41,42,43,44,45,46,47] |
| Extreme weather events | 5 | [14,15,22,23,36] |
| Atmosphere-ocean interactions | 3 | [20,23,41] |
| Wet/dry seasons | 3 | [26,29,30] |
| Outcome variables | ||
| Surveillance data | 15 | [16,17,18,19,20,23,27,37,38,41,43,44,45,46,47] |
| Hospital admissions | 9 | [24,25,28,29,33,34,35,39,42] |
| Vital statistics data | 4 | [14,15,22,36] |
| National surveys | 3 | [21,26,32] |
| Community-based | 2 | [19,40] |
| School-based | 1 | [31] |
| Outpatient-based | 1 | [30] |
| Themes | Number (n = 34) | References |
|---|---|---|
| Ecosystem-Mediated Impacts of Climate Change on Health Outcomes | 23 | [17,18,19,20,21,23,26,27,30,31,33,34,35,37,38,39,40,41,42,43,44,46,47] |
| Direct Impacts of Climate and Weather on Health | 11 | [14,15,16,24,25,28,29,36,45,46,47] |
| Vulnerability to Disease and Injury Due to Climate Variability and Climate Change | 4 | [15,22,36,42] |
| Adaptation to Protect Health | 4 | [23,31,37,44] |
| Health Impacts Heavily Mediated through Human Institutions | 1 | [32] |
| Co-Benefits | 0 | - |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chua, P.L.; Dorotan, M.M.; Sigua, J.A.; Estanislao, R.D.; Hashizume, M.; Salazar, M.A. Scoping Review of Climate Change and Health Research in the Philippines: A Complementary Tool in Research Agenda-Setting. Int. J. Environ. Res. Public Health 2019, 16, 2624. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16142624
Chua PL, Dorotan MM, Sigua JA, Estanislao RD, Hashizume M, Salazar MA. Scoping Review of Climate Change and Health Research in the Philippines: A Complementary Tool in Research Agenda-Setting. International Journal of Environmental Research and Public Health. 2019; 16(14):2624. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16142624
Chicago/Turabian StyleChua, Paul Lester, Miguel Manuel Dorotan, Jemar Anne Sigua, Rafael Deo Estanislao, Masahiro Hashizume, and Miguel Antonio Salazar. 2019. "Scoping Review of Climate Change and Health Research in the Philippines: A Complementary Tool in Research Agenda-Setting" International Journal of Environmental Research and Public Health 16, no. 14: 2624. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16142624