Telephone-Based Coaching and Prompting for Physical Activity: Short- and Long-Term Findings of a Randomized Controlled Trial (Movingcall)

 , ,
, ,
Abstract
:1. Introduction
2. Methods
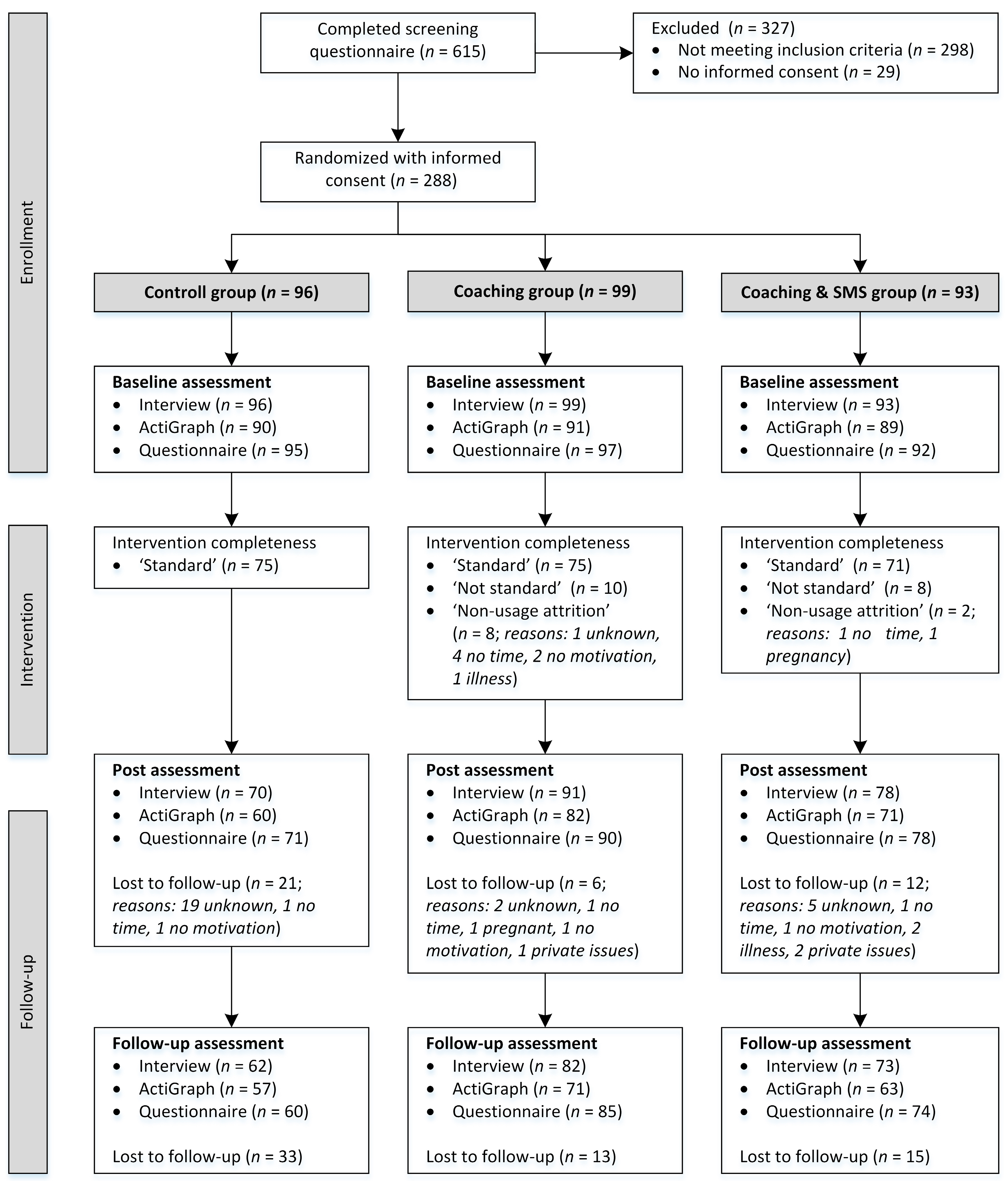
2.1. Study Design and Participants
2.2. Intervention
2.2.1. Coaching Group
2.2.2. Coaching and SMS Group
2.2.3. Control Group (Minimal Intervention)
2.3. Outcome Measures
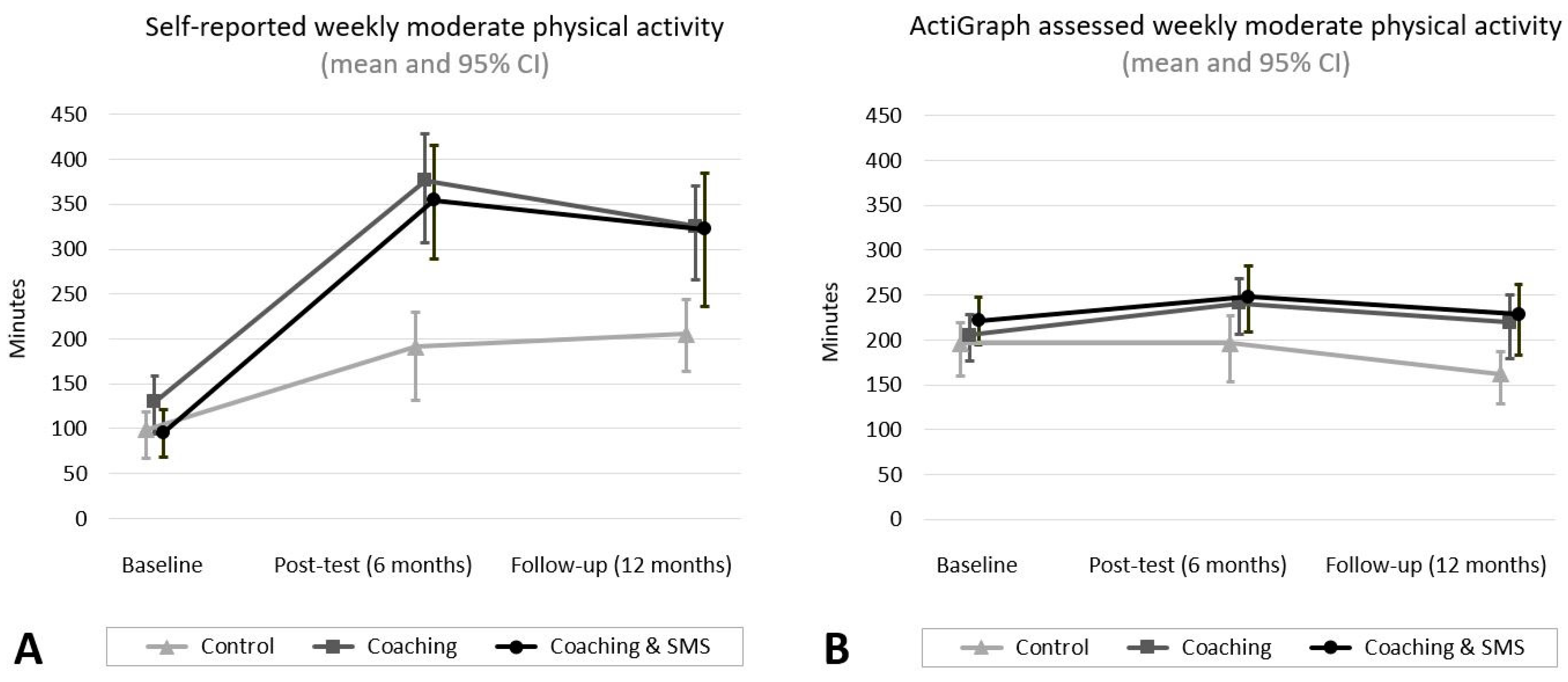
2.3.1. Self-Reported Physical Activity
2.3.2. Objectively Assessed Physical Activity
2.3.3. Perceived Physical Fitness
2.3.4. Intervention Fidelity and Acceptance
2.4. Data Analysis
3. Results
Adherence, Intervention Fidelity, and Acceptance
4. Discussion
4.1. Changes in Physical Activity
4.2. Adherence and Acceptance
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lee, I.M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T. Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef]
- Kohl, H.W., 3rd; Craig, C.L.; Lambert, E.V.; Inoue, S.; Alkandari, J.R.; Leetongin, G.; Kahlmeier, S. The pandemic of physical inactivity: Global action for public health. Lancet 2012, 380, 294–305. [Google Scholar] [CrossRef]
- Stamm, H.P.; Fischer, A.; Wiegand, D.; Lamprecht, M. Indikatorensammlung zum Monitoring-System Ernährung und Bewegung (Moseb); Bundesamt für Gesundheit (BAG): Bern, Switzerland, 2017. [Google Scholar]
- Hallal, P.C.; Andersen, L.B.; Bull, F.C.; Guthold, R.; Haskell, W.; Ekelund, U.; Lancet Physical Activity Series Working Group. Global physical activity levels: Surveillance progress, pitfalls, and prospects. Lancet 2012, 380, 247–257. [Google Scholar] [CrossRef]
- WHO. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Borodulin, K.; Sipila, N.; Rahkonen, O.; Leino-Arjas, P.; Kestila, L.; Jousilahti, P.; Prattala, R. Socio-demographic and behavioral variation in barriers to leisure-time physical activity. Scand. J. Public Health 2016, 44, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Ding, D.; Lawson, K.D.; Kolbe-Alexander, T.L.; Finkelstein, E.A.; Katzmarzyk, P.T.; van Mechelen, W.; Pratt, M.; Lancet Physical Activity Series 2 Executive Committee. The economic burden of physical inactivity: A global analysis of major non-communicable diseases. Lancet 2016, 388, 1311–1324. [Google Scholar] [CrossRef]
- Mattli, R.; Wieser, S.; Probst-Hensch, N.; Schmidt-Trucksass, A.; Schwenkglenks, M. Physical inactivity caused economic burden depends on regional cultural differences. Scand. J. Med. Sci. Sports 2019, 29, 95–104. [Google Scholar] [CrossRef]
- Noar, S.M.; Benac, C.N.; Harris, M.S. Does tailoring matter? Meta-analytic review of tailored print health behavior change interventions. Psychol. Bull. 2007, 133, 673–693. [Google Scholar] [CrossRef]
- Foster, C.; Richards, J.; Thorogood, M.; Hillsdon, M. Remote and web 2.0 interventions for promoting physical activity. Cochrane Database Syst. Rev. 2013, 9, CD010395. [Google Scholar]
- Michie, S.; Abraham, C.; Whittington, C.; McAteer, J.; Gupta, S. Effective techniques in healthy eating and physical activity interventions: A meta-regression. Health Psychol. 2009, 28, 690–701. [Google Scholar] [CrossRef]
- Bird, E.L.; Baker, G.; Mutrie, N.; Ogilvie, D.; Sahlqvist, S.; Powell, J. Behavior change techniques used to promote walking and cycling: A systematic review. Health Psychol. 2013, 32, 829–838. [Google Scholar] [CrossRef]
- Samdal, G.B.; Eide, G.E.; Barth, T.; Williams, G.; Meland, E. Effective behaviour change techniques for physical activity and healthy eating in overweight and obese adults; systematic review and meta-regression analyses. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 42. [Google Scholar] [CrossRef] [PubMed]
- Olander, E.K.; Fletcher, H.; Williams, S.; Atkinson, L.; Turner, A.; French, D.P. What are the most effective techniques in changing obese individuals’ physical activity self-efficacy and behaviour: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 29. [Google Scholar] [CrossRef] [PubMed]
- Howlett, N.; Trivedi, D.; Troop, N.A.; Chater, A.M. Are physical activity interventions for healthy inactive adults effective in promoting behavior change and maintenance, and which behavior change techniques are effective? A systematic review and meta-analysis. Transl. Behav. Med. 2018, 9, 147–157. [Google Scholar] [CrossRef] [PubMed]
- Richards, J.; Hillsdon, M.; Thorogood, M.; Foster, C. Face-to-face interventions for promoting physical activity. Cochrane Database Syst. Rev. 2013, 9, CD010392. [Google Scholar]
- Davies, C.A.; Spence, J.C.; Vandelanotte, C.; Caperchione, C.M.; Mummery, W.K. Meta-analysis of internet-delivered interventions to increase physical activity levels. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 52. [Google Scholar] [CrossRef] [PubMed]
- Garrett, S.; Elley, C.R.; Rose, S.B.; O’Dea, D.; Lawton, B.A.; Dowell, A.C. Are physical activity interventions in primary care and the community cost-effective? A systematic review of the evidence. Br. J. Gen. Pract. 2011, 61, e125–e133. [Google Scholar] [CrossRef] [Green Version]
- Goode, A.D.; Reeves, M.M.; Eakin, E.G. Telephone-delivered interventions for physical activity and dietary behavior change: An updated systematic review. Am. J. Prev. Med. 2012, 42, 81–88. [Google Scholar] [CrossRef]
- Eakin, E.G.; Lawler, S.P.; Vandelanotte, C.; Owen, N. Telephone interventions for physical activity and dietary behavior change: A systematic review. Am. J. Prev. Med. 2007, 32, 419–434. [Google Scholar] [CrossRef]
- Head, K.J.; Noar, S.M.; Iannarino, N.T.; Grant Harrington, N. Efficacy of text messaging-based interventions for health promotion: A meta-analysis. Soc. Sci. Med. 2013, 97, 41–48. [Google Scholar] [CrossRef]
- Joseph, R.P.; Durant, N.H.; Benitez, T.J.; Pekmezi, D.W. Internet-based physical activity interventions. Am. J. Lifestyle Med. 2014, 8, 42–68. [Google Scholar] [CrossRef]
- Vandelanotte, C.; Muller, A.M.; Short, C.E.; Hingle, M.; Nathan, N.; Williams, S.L.; Lopez, M.L.; Parekh, S.; Maher, C.A. Past, present, and future of ehealth and mhealth research to improve physical activity and dietary behaviors. J. Nutr. Educ. Behav. 2016, 48, 219–228. [Google Scholar] [CrossRef] [PubMed]
- Fischer, X.; Donath, L.; Zwygart, K.; Gerber, M.; Faude, O.; Zahner, L. Coaching and prompting for remote physical activity promotion: Study protocol of a three-arm randomized controlled trial (movingcall). Int. J. Environ. Res. Public Health 2019, 16, 331. [Google Scholar] [CrossRef] [PubMed]
- Schilling, R.; Scharli, E.; Fischer, X.; Donath, L.; Faude, O.; Brand, S.; Puhse, U.; Zahner, L.; Rosenbaum, S.; Ward, P.B.; et al. The utility of two interview-based physical activity questionnaires in healthy young adults: Comparison with accelerometer data. PLoS ONE 2018, 13, e0203525. [Google Scholar] [CrossRef] [PubMed]
- Thomas, S.; Reading, J.; Shephard, R.J. Revision of the physical activity readiness questionnaire (par-q). Can. J. Sport Sci. 1992, 17, 338–345. [Google Scholar] [PubMed]
- Vickers, A.J.; Altman, D.G. Statistics notes: Analysing controlled trials with baseline and follow up measurements. BMJ 2001, 323, 1123–1124. [Google Scholar] [CrossRef]
- Michie, S.; Richardson, M.; Johnston, M.; Abraham, C.; Francis, J.; Hardeman, W.; Eccles, M.P.; Cane, J.; Wood, C.E. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behavior change interventions. Ann. Behav. Med. 2013, 46, 81–95. [Google Scholar] [CrossRef]
- Michie, S.; Atkins, L.; West, R. The Behaviour Change Wheel: A Guide to Designing Interventions; Silverback Publishing: London, UK, 2014. [Google Scholar]
- Michie, S.; van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef]
- Fuchs, R.; Seelig, H.; Gohner, W.; Burton, N.W.; Brown, W.J. Cognitive mediation of intervention effects on physical exercise: Causal models for the adoption and maintenance stage. Psychol. Health 2012, 27, 1480–1499. [Google Scholar] [CrossRef]
- Vogel, D.; Usov, A.; Fischer, X.; Donath, L.; Zahner, L. Movingcall Activity-Profile. Available online: https://www.movingcall.com (accessed on 17 January 2018).
- Saghaei, M. An overview of randomization and minimization programs for randomized clinical trials. J. Med. Signals Sens. 2011, 1, 55–61. [Google Scholar] [Green Version]
- Olsen, J.M. Health coaching: A concept analysis. Nurs. Forum 2014, 49, 18–29. [Google Scholar] [CrossRef]
- Trost, S.G.; McIver, K.L.; Pate, R.R. Conducting accelerometer-based activity assessments in field-based research. Med. Sci. Sports Exerc. 2005, 37, S531–S543. [Google Scholar] [CrossRef] [PubMed]
- McMinn, D.; Acharya, R.; Rowe, D.A.; Gray, S.R.; Allan, J.L. Measuring activity energy expenditure: Accuracy of the gt3x+ and actiheart monitors. Int. J. Exerc. Sci. 2013, 6, 217–229. [Google Scholar]
- Kamada, M.; Shiroma, E.J.; Harris, T.B.; Lee, I.M. Comparison of physical activity assessed using hip- and wrist-worn accelerometers. Gait Posture 2016, 44, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Pedisic, Z.; Bauman, A. Accelerometer-based measures in physical activity surveillance: Current practices and issues. Br. J. Sports Med. 2015, 49, 219–223. [Google Scholar] [CrossRef]
- Cole, R.J.; Kripke, D.F.; Gruen, W.; Mullaney, D.J.; Gillin, J.C. Automatic sleep/wake identification from wrist activity. Sleep 1992, 15, 461–469. [Google Scholar] [CrossRef] [PubMed]
- Troiano, R.P. Large-scale applications of accelerometers: New frontiers and new questions. Med. Sci. Sports Exerc. 2007, 39, 1501. [Google Scholar] [CrossRef]
- Ainsworth, B.E.; Haskell, W.L.; Herrmann, S.D.; Meckes, N.; Bassett, D.R., Jr.; Tudor-Locke, C.; Greer, J.L.; Vezina, J.; Whitt-Glover, M.C.; Leon, A.S. 2011 compendium of physical activities: A second update of codes and met values. Med. Sci. Sports Exerc. 2011, 43, 1575–1581. [Google Scholar] [CrossRef]
- Plante, T.; Lantis, A.; Checa, G. The influence of perceived versus aerobic fitness on psychological health and physiological stress responsivity. Int. J. Stress Manag. 1998, 5, 141–156. [Google Scholar] [CrossRef]
- Wen, C.P.; Wai, J.P.; Tsai, M.K.; Yang, Y.C.; Cheng, T.Y.; Lee, M.C.; Chan, H.T.; Tsao, C.K.; Tsai, S.P.; Wu, X. Minimum amount of physical activity for reduced mortality and extended life expectancy: A prospective cohort study. Lancet 2011, 378, 1244–1253. [Google Scholar] [CrossRef]
- Murray, J.M.; Brennan, S.F.; French, D.P.; Patterson, C.C.; Kee, F.; Hunter, R.F. Effectiveness of physical activity interventions in achieving behaviour change maintenance in young and middle aged adults: A systematic review and meta-analysis. Soc. Sci. Med. 2017, 192, 125–133. [Google Scholar] [CrossRef] [Green Version]
- Fjeldsoe, B.; Neuhaus, M.; Winkler, E.; Eakin, E. Systematic review of maintenance of behavior change following physical activity and dietary interventions. Health Psychol. 2011, 30, 99–109. [Google Scholar] [CrossRef] [PubMed]
- Dejonghe, L.A.L.; Becker, J.; Froboese, I.; Schaller, A. Long-term effectiveness of health coaching in rehabilitation and prevention: A systematic review. Patient Educ. Couns. 2017, 100, 1643–1653. [Google Scholar] [CrossRef] [PubMed]
- Silfee, V.J.; Haughton, C.F.; Jake-Schoffman, D.E.; Lopez-Cepero, A.; May, C.N.; Sreedhara, M.; Rosal, M.C.; Lemon, S.C. Objective measurement of physical activity outcomes in lifestyle interventions among adults: A systematic review. Prev. Med. Rep. 2018, 11, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Van Hoecke, A.S.; Delecluse, C.; Bogaerts, A.; Boen, F. The long-term effectiveness of need-supportive physical activity counseling compared with a standard referral in sedentary older adults. J. Aging Phys. Act. 2014, 22, 186–198. [Google Scholar] [CrossRef] [PubMed]
- Clemes, S.A.; Parker, R.A. Increasing our understanding of reactivity to pedometers in adults. Med. Sci. Sports Exerc. 2009, 41, 674–680. [Google Scholar] [CrossRef] [PubMed]
- Wickstrom, G.; Bendix, T. The “hawthorne effect”—What did the original hawthorne studies actually show? Scand. J. Work Environ. Health 2000, 26, 363–367. [Google Scholar] [PubMed]
- Hall, A.K.; Cole-Lewis, H.; Bernhardt, J.M. Mobile text messaging for health: A systematic review of reviews. Annu. Rev. Public Health 2015, 36, 393–415. [Google Scholar] [CrossRef]
- Muller, A.M.; Khoo, S.; Morris, T. Text messaging for exercise promotion in older adults from an upper-middle-income country: Randomized controlled trial. J. Med. Internet Res. 2016, 18, e5. [Google Scholar] [CrossRef] [PubMed]
- Patrick, K.; Raab, F.; Adams, M.A.; Dillon, L.; Zabinski, M.; Rock, C.L.; Griswold, W.G.; Norman, G.J. A text message-based intervention for weight loss: Randomized controlled trial. J. Med. Internet Res. 2009, 11, e1. [Google Scholar] [CrossRef]
- Orrow, G.; Kinmonth, A.L.; Sanderson, S.; Sutton, S. Republished research: Effectiveness of physical activity promotion based in primary care: Systematic review and meta-analysis of randomised controlled trials. Br. J. Sports Med. 2013, 47, 27. [Google Scholar] [CrossRef]
- Prince, S.A.; Adamo, K.B.; Hamel, M.E.; Hardt, J.; Connor Gorber, S.; Tremblay, M. A comparison of direct versus self-report measures for assessing physical activity in adults: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2008, 5, 56. [Google Scholar] [CrossRef] [PubMed]
- Hildebrand, M.; Van Hees, V.T.; Hansen, B.H.; Ekelund, U. Age group comparability of raw accelerometer output from wrist- and hip-worn monitors. Med. Sci. Sports Exerc. 2014, 46, 1816–1824. [Google Scholar] [CrossRef] [PubMed]
- Troiano, R.P.; McClain, J.J.; Brychta, R.J.; Chen, K.Y. Evolution of accelerometer methods for physical activity research. Br. J. Sports Med. 2014, 48, 1019–1023. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dieu, O.; Mikulovic, J.; Fardy, P.S.; Bui-Xuan, G.; Beghin, L.; Vanhelst, J. Physical activity using wrist-worn accelerometers: Comparison of dominant and non-dominant wrist. Clin. Physiol. Funct. Imaging 2016, 37, 525–529. [Google Scholar] [CrossRef] [PubMed]
- Sallis, J.F.; Saelens, B.E. Assessment of physical activity by self-report: Status, limitations, and future directions. Res. Q. Exerc. Sport 2000, 71 (Suppl. 2), 1–14. [Google Scholar] [CrossRef] [PubMed]
- Van Sluijs, E.M.; Griffin, S.J.; van Poppel, M.N. A cross-sectional study of awareness of physical activity: Associations with personal, behavioral and psychosocial factors. Int. J. Behav. Nutr. Phys. Act. 2007, 4, 53. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Control (n = 96) | Coaching (n = 99) | Coaching and SMS (n = 93) | Total (n = 288) |
|---|---|---|---|---|
| Age in years, mean (SD) | 42.20 (11.39) | 41.93 (11.12) | 42.54 (11.78) | 42.22 (11.39) |
| Age category, n (%) | ||||
| 20–31 years | 19 (19.8) | 22 (22.2) | 21 (22.6) | 62 (21.5) |
| 32–42 years | 31 (32.3) | 23 (23.2) | 24 (25.8) | 78 (27.1) |
| 43–53 years | 27 (28.2) | 39 (39.4) | 32 (34.4) | 98 (34.0) |
| 54–65 years | 19 (19.8) | 15 (15.2) | 16 (17.2) | 50 (17.4) |
| Gender, n (%) | ||||
| Female | 64 (66.7) | 69 (69.7) | 64 (68.8) | 197 (68.4) |
| Male | 32 (33.3) | 30 (30.3) | 29 (31.2) | 91 (31.6) |
| BMI in kg/m2, mean (SD) | 26.43 (5.33) | 25.26 (4.28) | 26.24 (4.99) | 25.97 (4.89) |
| BMI Category, n (%) | ||||
| Underweight (<18.50) | 2 (2.1) | 2 (2.0) | 1 (1.1) | 5 (1.7) |
| Normal weight (18.50–24.99) | 44 (45.8) | 54 (54.6) | 43 (46.2) | 141 (49.0) |
| Overweight (25.00–29.99) | 28 (29.2) | 27 (27.3) | 32 (34.4) | 87 (30.2) |
| Obese (≥30.00) | 22 (22.9) | 16 (16.2) | 17 (18.3) | 55 (19.1) |
| Occupation, n (%) | ||||
| Employed | 83 (86.5) | 84 (84.9) | 76 (81.7) | 243 (84.4) |
| Student | 4 (4.2) | 8 (8.1) | 8 (8.6) | 20 (6.9) |
| House wife/husband | 4 (4.2) | 2 (2.0) | 5 (5.4) | 11 (3.8) |
| Pensioner | 2 (2.1) | 3 (3.0) | 1 (1.1) | 6 (2.1) |
| Unemployed | 1 (1.0) | - | 3 (3.2) | 4 (1.4) |
| No response | 2 (2.1) | 2 (2.0) | - | 4 (1.4) |
| Highest education level, n (%) | ||||
| Compulsory education | 1 (1.0) | 1 (1.0) | 2 (2.2) | 4 (1.4) |
| Apprenticeship | 28 (29.2) | 30 (30.3) | 27 (29.0) | 85 (29.5) |
| High school | 21 (21.9) | 21 (21.2) | 22 (23.7) | 64 (22.2) |
| University | 39 (40.6) | 39 (39.4) | 37 (39.8) | 115 (39.9) |
| Doctorate | 5 (5.2) | 7 (7.1) | 5 (5.4) | 17 (5.9) |
| No response | 2 (2.1) | 1 (1.0) | - | 3 (1.0) |
| Yearly household income, n (%) | ||||
| <50,000 CHF | 13 (13.5) | 19 (19.2) | 11 (11.8) | 43 (14.9) |
| 50,000–100,000 CHF | 40 (41.7) | 42 (42.4) | 47 (50.5) | 129 (44.8) |
| >100,000 CHF | 41 (42.7) | 35 (35.4) | 32 (34.4) | 108 (37.5) |
| No response | 2 (2.1) | 3 (3.0) | 3 (3.23) | 8 (2.8) |
| Family status: Number of children bellow 18 years, n (%) | ||||
| No children | 69 (71.9) | 63 (63.6) | 63 (67.7) | 195 (67.7) |
| 1 child | 9 (9.4) | 8 (8.1) | 9 (9.7) | 26 (9.0) |
| 2 children | 10 (10.4) | 19 (19.2) | 12 (12.9) | 41 (14.2) |
| 3–4 children | 3 (3.1) | 3 (3.0) | 1 (1.1) | 7 (2.4) |
| Missing response | 5 (5.2) | 6 (6.1) | 8 (8.6) | 19 (6.6) |
| M | Adjusted Mean Change from Baseline in min/week (95% CI) | Pairwise Comparison: Differences among Groups in Change from Baseline (95% CI) | ||||
|---|---|---|---|---|---|---|
| Control | Coaching | Coaching and SMS | Coaching versus Control | Coaching and SMS versus Control | Coaching and SMS versus Coaching | |
| 6 | 86.9 (28.1 to 145.7) | 259.9 (208.1 to 311.7) | 252.3 (196.5 to 308.1) | 173.0 (94.5 to 251.5) | 165.4 (84.4 to 246.3) | −7.6 (−83.9 to 68.7) |
| 12 | 98.9 (36.8 to 161.1) | 211.4 (157.0 to 265.7) | 212.1 (154.6 to 269.6) | 112.4 (29.7 to 195.2) | 113.2 (28.6 to 197.8) | 40.9 (−37.2 to 119.0) |
| M | Adjusted Mean Change from Baseline in min/week (95% CI) | Pairwise Comparison: Differences among Groups in Change from Baseline (95% CI) | ||||
|---|---|---|---|---|---|---|
| Control | Coaching | Coaching and SMS | Coaching vs. Control | Coaching and SMS vs. Control | Coaching and SMS vs. Coaching | |
| 6 | −5.1 (−28.7 to 18.6) | 26.5 (5.8 to 47.1) | 28.5 (7.0 to 50.0) | 31.5 (0.1 to 62.9) | 33.5 (1.6 to 65.5) | 2.0 (−27.8 to 31.8) |
| 12 | −26.1 (−50.1 to −2.1) | 6.9 (−14.7 to 28.5) | 15.6 (−6.8 to 38.0) | 33.0 (0.7 to 65.2) | 41.7 (8.9 to 74.5) | 8.7 (−22.4 to 39.8) |
| Behavior Change Technique | Mean | SD |
|---|---|---|
| Action planning | 7.2 | 3.2 |
| Feedback on behavior | 7 | 3 |
| Self-monitoring of behavior | 6.3 | 3.1 |
| Problem solving | 5.2 | 2.4 |
| Goal setting (behavior) | 4.7 | 2.6 |
| Review of behavioral goal (s) | 4.5 | 2.8 |
| Instruction on how to perform the behavior | 3 | 2.4 |
| Social support | 2.9 | 2.4 |
| Habit formation | 2.9 | 2.6 |
| Information about health consequences | 2.1 | 1.6 |
| Goal setting (outcome) | 1.6 | 2 |
| Behavior practice/rehearsal | 1.3 | 1.5 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fischer, X.; Kreppke, J.-N.; Zahner, L.; Gerber, M.; Faude, O.; Donath, L. Telephone-Based Coaching and Prompting for Physical Activity: Short- and Long-Term Findings of a Randomized Controlled Trial (Movingcall). Int. J. Environ. Res. Public Health 2019, 16, 2626. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16142626
Fischer X, Kreppke J-N, Zahner L, Gerber M, Faude O, Donath L. Telephone-Based Coaching and Prompting for Physical Activity: Short- and Long-Term Findings of a Randomized Controlled Trial (Movingcall). International Journal of Environmental Research and Public Health. 2019; 16(14):2626. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16142626
Chicago/Turabian StyleFischer, Xenia, Jan-Niklas Kreppke, Lukas Zahner, Markus Gerber, Oliver Faude, and Lars Donath. 2019. "Telephone-Based Coaching and Prompting for Physical Activity: Short- and Long-Term Findings of a Randomized Controlled Trial (Movingcall)" International Journal of Environmental Research and Public Health 16, no. 14: 2626. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16142626