Increased Risk of Carotid Atherosclerosis in Male Patients with Chronic Periodontitis: A Nationwide Population-Based Retrospective Cohort Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Exposure of CP
2.3. CA Event
2.4. Co-Morbidities
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kinane, D.F.; Bartold, P.M. Clinical relevance of the host responses of periodontitis. Periodontol. 2000 2007, 43, 278–293. [Google Scholar] [CrossRef] [PubMed]
- Beck, J.; Garcia, R.; Heiss, G.; Vokonas, P.S.; Offenbacher, S. Periodontal disease and cardiovascular disease. J. Periodontol. 1996, 67, 1123–1137. [Google Scholar] [CrossRef] [PubMed]
- Haraszthy, V.I.; Zambon, J.J.; Tresian, M.; Zeid, M.; Genco, R.J. Identification of periodontal pathogens in atheromatous plaques. J. Periodontol. 2000, 71, 1554–1560. [Google Scholar] [CrossRef] [PubMed]
- Polak, D.; Shapira, L. An update on the evidence for pathogenic mechanisms that may link periodontitis and diabetes. J. Clin. Periodontol. 2018, 45, 150–166. [Google Scholar] [CrossRef] [PubMed]
- Scannapieco, F.A.; Cantos, A. Oral inflammation and infection, and chronic medical diseases: Implications for the elderly. Periodontol. 2000 2016, 72, 153–175. [Google Scholar] [CrossRef] [PubMed]
- International Carotid Stenting Study investigators. Carotid artery stenting compared with endarterectomy in patients with symptomatic carotid stenosis (International Carotid Stenting Study): An interim analysis of a randomized controlled trial. Lancet 2010, 375, 985–997. [Google Scholar] [CrossRef]
- Naylor, A.R.; Bown, M.J. Stroke after cardiac surgery and its association with asymptomatic carotid disease: An updated systematic review and meta-analysis. Eur. J. Vasc. Endovasc. Surg. 2011, 41, 607–624. [Google Scholar] [CrossRef] [PubMed]
- Orlandi, M.; Suvan, J.; Petrie, A.; Donos, N.; Masi, S.; Hingorani, A.; Deanfield, J.; D’Aiuto, F. Association between periodontal disease and its treatment, flow-mediated dilatation and carotid intima-media thickness: A systematic review and meta-analysis. Atherosclerosis 2014, 236, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Zeng, X.T.; Leng, W.D.; Lam, Y.Y.; Yan, B.P.; Wei, X.M.; Weng, H.; Kwong, J.S. Periodontal disease and carotid atherosclerosis: A meta-analysis of 17,330 participants. Int. J. Cardiol. 2016, 203, 1044–1051. [Google Scholar] [CrossRef] [PubMed]
- Kozarov, E.V.; Dorn, B.R.; Shelburne, C.E.; Dunn, W.A., Jr.; Progulske-Fox, A. Human atherosclerotic plaque contains viable invasive Actinobacillus actinomycetemcomitans and Porphyromonas gingivalis. Arteriosclerosis Thromb. Vas. Biol. 2005, 25, 17–18. [Google Scholar] [CrossRef] [PubMed]
- Figuero, E.; Sánchez-Beltrán, M.; Cuesta-Frechoso, S.; Tejerina, J.M.; del Castro, J.A.; Gutiérrez, J.M.; Herrera, D.; Sanz, M. Detection of periodontal bacteria in atheromatous plaque by nested polymerase chain reaction. J. Periodontol. 2011, 82, 469–477. [Google Scholar] [CrossRef] [PubMed]
- Pinho, M.M.; Faria-Almeida, R.; Azevedo, E.; Manso, M.C.; Martins, L. Periodontitis and atherosclerosis: An observational study. J. Periodontal. Res. 2013, 48, 452–457. [Google Scholar] [CrossRef] [PubMed]
- Yakob, M.; Söder, B.; Meurman, J.H.; Jogestrand, T.; Nowak, J.; Söder, P.Ö. Prevotella nigrescens and Porphyromonas gingivalis are associated with signs of carotid atherosclerosis in subjects with and without periodontitis. J. Periodontal. Res. 2011, 6, 749–755. [Google Scholar] [CrossRef] [PubMed]
- National Health Insurance Administration, Ministry of Health and Welfare, Taiwan, R.O.C. National Health Insurance Annual Report 2014–2015. Available online: https://nhird.nhri.org.tw/en/ (accessed on 6 June 2018).
- Yu, H.C.; Chen, T.P.; Wei, C.Y.; Chang, Y.C. Association between Peptic Ulcer Disease and Periodontitis: A Nationwide Population-Based Case-Control Study in Taiwan. Int. J. Environ. Res. Public Health 2018, 15, 912. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.K.; Huang, J.Y.; Wu, Y.T.; Chang, Y.C. Dental Scaling Decreases the Risk of Parkinson’s Disease: A Nationwide Population-Based Nested Case-Control Study. Int. J. Environ. Res. Public Health 2018, 15, 1587. [Google Scholar] [CrossRef] [PubMed]
- Desvarieux, M.; Schwahn, C.; Völzke, H.; Demmer, R.T.; Lüdemann, J.; Kessler, C.; Jacobs, D.R., Jr.; John, U.; Kocher, T. Gender differences in the relationship between periodontal disease, tooth loss, and atherosclerosis. Stroke 2004, 35, 2029–2035. [Google Scholar] [CrossRef] [PubMed]
- Bengtsson, V.W.; Persson, G.R.; Berglund, J.; Renvert, S. A cross-sectional study of the associations between periodontitis and carotid arterial calcifications in an elderly population. Acta Odontol. Scand. 2016, 74, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Carallo, C.; Fortunato, L.; de Franceschi, M.S.; Irace, C.; Tripolino, C.; Cristofaro, M.G.; Giudice, M.; Gnasso, A. Periodontal disease and carotid atherosclerosis: Are hemodynamic forces a link? Atherosclerosis 2010, 213, 263–267. [Google Scholar] [CrossRef] [PubMed]
- Carallo, C.; De Franceschi, M.S.; Tripolino, C.; Figliuzzi, M.; Irace, C.; Fortunato, L.; Gnasso, A. Common carotid and brachial artery hemodynamic alterations in periodontal disease. J. Clin. Periodontol. 2013, 40, 431–436. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Chronic Periodontitis (N = 72,630) | Control (N = 72,630) | p-Value | |||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Age | 0.290 | ||||
| <40 | 30,585 | 42.1 | 30,597 | 42.1 | |
| 40–64 | 35,039 | 48.2 | 35,198 | 48.5 | |
| ≥65 | 7006 | 9.6 | 6835 | 9.4 | |
| Mean ± SD | 44.02 ± 14.63 | 44.15 ± 14.41 | 0.107 | ||
| Gender | 0.258 | ||||
| Female | 38,252 | 52.7 | 38,467 | 53.0 | |
| Male | 34,378 | 47.3 | 34,163 | 47.0 | |
| Monthly income | 0.177 | ||||
| <NTD $20,000 | 31,190 | 42.9 | 30,876 | 42.5 | |
| NTD $20,000–NTD $40,000 | 22,390 | 30.8 | 22,679 | 31.2 | |
| >NTD $40,000 | 19,050 | 26.2 | 19,075 | 26.3 | |
| Urbanization | 0.803 | ||||
| Urban | 49,325 | 67.9 | 49,367 | 68.0 | |
| Suburban | 19,208 | 26.4 | 19,224 | 26.5 | |
| Rural | 4097 | 5.6 | 4039 | 5.6 | |
| Hypertension | 8973 | 12.4 | 8985 | 12.4 | 0.924 |
| Hyperlipidemia | 4390 | 6.0 | 4263 | 5.9 | 0.159 |
| Diabetes | 4002 | 5.5 | 3957 | 5.4 | 0.604 |
| COPD | 3022 | 4.2 | 2973 | 4.1 | 0.518 |
| Heart failure | 347 | 0.5 | 287 | 0.4 | 0.017 |
| Stroke | 1235 | 1.7 | 1132 | 1.6 | 0.033 |
| Thyroid disease | 1325 | 1.8 | 1328 | 1.8 | 0.953 |
| Carotid ultrasound | 5702 | 7.9 | 5505 | 7.6 | 0.053 |
| Statin | 13,206 | 18.2 | 13,270 | 18.3 | 0.664 |
| Aspirin | 10,852 | 14.9 | 10,915 | 15.0 | 0.643 |
| No. of Event | Observed Person-Years | ID | Crude HR | 95% CI | Adjusted HR | 95% CI | |
|---|---|---|---|---|---|---|---|
| Chronic periodontitis | |||||||
| No | 284 | 624,078 | 0.5 | 1 | 1 | ||
| Yes | 305 | 628,342 | 0.5 | 1.06 | 0.91–1.25 | 1.02 | 0.86–1.19 |
| Age | |||||||
| <40 | 21 | 543,733 | 0.04 | 1 | 1 | ||
| 40–64 | 307 | 596,995 | 0.5 | 13.50 | 8.68–21.00 | 8.72 | 5.56–13.68 |
| ≥65 | 261 | 111,691 | 2.3 | 62.41 | 40.01–97.36 | 17.10 | 10.63–27.53 |
| Gender | |||||||
| Female | 237 | 663,089 | 0.4 | 1 | 1 | ||
| Male | 352 | 589,331 | 0.6 | 1.67 | 1.42–1.97 | 1.37 | 1.15–1.62 |
| Monthly income | |||||||
| <NTD $20,000 | 325 | 536,670 | 0.6 | 1 | 1 | ||
| NTD $20,000–NTD $40,000 | 167 | 384,515 | 0.4 | 0.72 | 0.60–0.87 | 1.03 | 0.84–1.25 |
| >NTD $40,000 | 97 | 331,236 | 0.3 | 0.48 | 0.39–0.61 | 0.85 | 0.66–1.09 |
| Urbanization | |||||||
| Urban | 383 | 850,525 | 0.5 | 1 | 1 | ||
| Suburban | 170 | 332,359 | 0.5 | 1.14 | 0.95–1.36 | 1.15 | 0.96–1.38 |
| Rural | 36 | 69,536 | 0.5 | 1.15 | 0.82–1.62 | 0.87 | 0.61–1.24 |
| Hypertension | 266 | 141,725 | 1.9 | 6.68 | 5.67–7.85 | 1.72 | 1.42–2.08 |
| Hyperlipidemia | 98 | 64,594 | 1.5 | 3.87 | 3.11–4.81 | 1.38 | 1.09–1.76 |
| Diabetes | 111 | 61,758 | 1.8 | 4.64 | 3.77–5.70 | 1.47 | 1.17–1.83 |
| COPD | 86 | 51,674 | 1.7 | 3.97 | 3.16–4.99 | 1.50 | 1.18–1.90 |
| Heart failure | 11 | 4737 | 2.3 | 5.25 | 2.89–9.53 | 1.06 | 0.58–1.93 |
| Stroke | 68 | 18,367 | 3.7 | 9.05 | 7.03–11.65 | 1.57 | 1.20–2.05 |
| Thyroid disease | 16 | 22,481 | 0.7 | 1.53 | 0.93–2.52 | 1.28 | 0.77–2.11 |
| Carotid ultrasound | 310 | 103,674 | 3.0 | 12.08 | 10.27–14.2 | 4.72 | 3.91–5.69 |
| Statin | 206 | 238,841 | 0.9 | 2.25 | 1.90–2.66 | 0.63 | 0.52–0.76 |
| Aspirin | 319 | 199,526 | 1.6 | 6.11 | 5.20–7.19 | 1.25 | 1.02–1.53 |
| Chronic Periodontitis | Control | HR | 95% CI | |||
|---|---|---|---|---|---|---|
| N | No. of Event | N | No. of Event | |||
| Age † | ||||||
| <40 | 30,585 | 11 | 30,597 | 10 | 1.06 | 0.45–2.50 |
| 40–64 | 35,039 | 156 | 35,198 | 151 | 1.02 | 0.82–1.28 |
| ≥65 | 7006 | 138 | 6835 | 123 | 1.02 | 0.80–1.30 |
| p for interaction = 0.985 | ||||||
| Gender ‡ | ||||||
| Female | 38,252 | 109 | 38,467 | 128 | 0.81 | 0.63–1.05 |
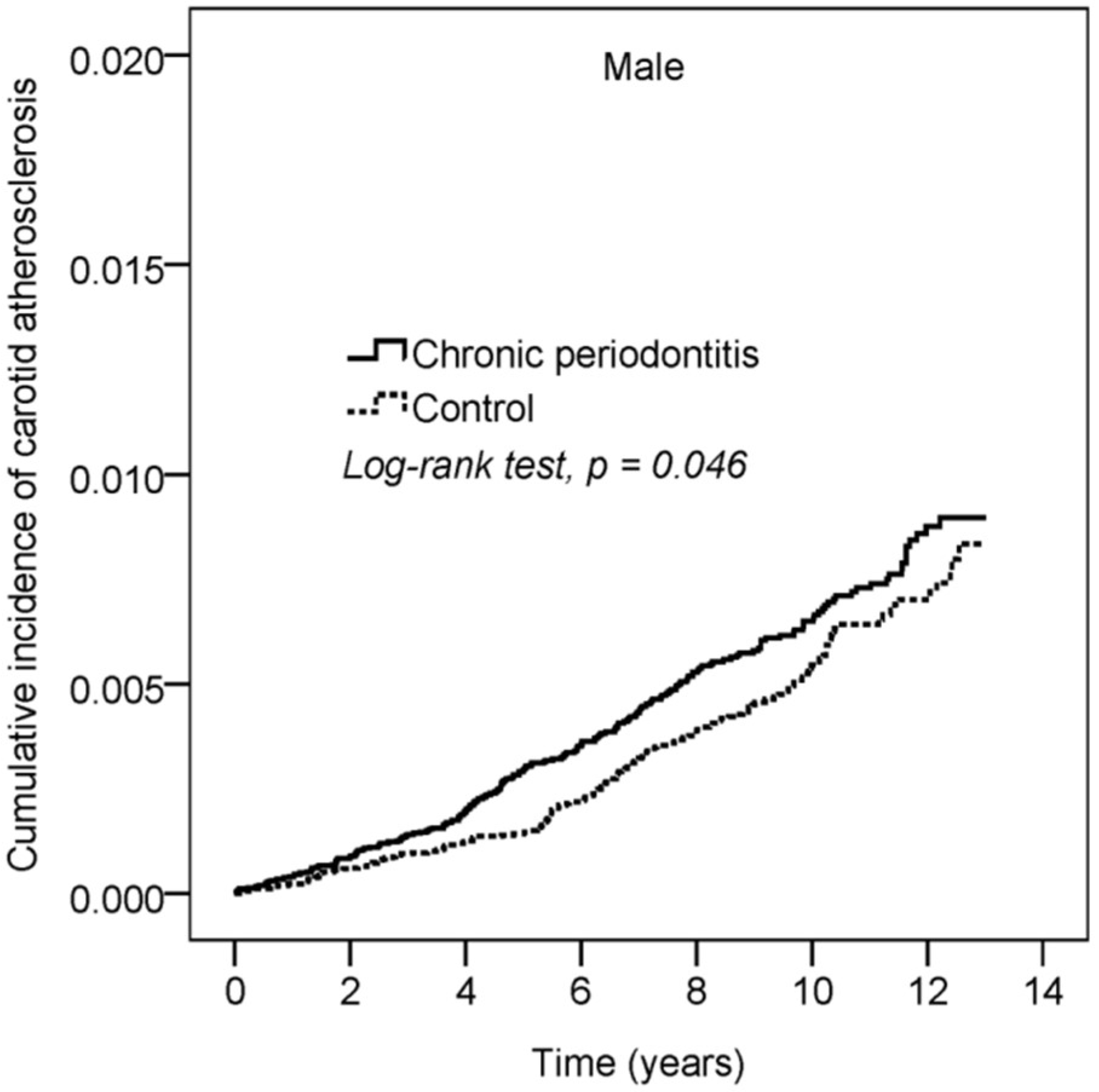
| Male | 34,378 | 196 | 34,163 | 156 | 1.16 | 0.94–1.43 |
| p for interaction = 0.042 | ||||||
| Chronic Periodontitis (N = 72,630) | Control (N = 72,630) | p-Value | |
|---|---|---|---|
| Follow-up duration (years) | 8.65 ± 3.06 | 8.59 ± 3.08 | <0.001 |
| Time to event (years), N = 589 | 5.69 ± 3.24 | 6.07 ± 3.14 | 0.149 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tong, C.; Wang, Y.-H.; Chang, Y.-C. Increased Risk of Carotid Atherosclerosis in Male Patients with Chronic Periodontitis: A Nationwide Population-Based Retrospective Cohort Study. Int. J. Environ. Res. Public Health 2019, 16, 2635. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16152635
Tong C, Wang Y-H, Chang Y-C. Increased Risk of Carotid Atherosclerosis in Male Patients with Chronic Periodontitis: A Nationwide Population-Based Retrospective Cohort Study. International Journal of Environmental Research and Public Health. 2019; 16(15):2635. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16152635
Chicago/Turabian StyleTong, Ching, Yu-Hsun Wang, and Yu-Chao Chang. 2019. "Increased Risk of Carotid Atherosclerosis in Male Patients with Chronic Periodontitis: A Nationwide Population-Based Retrospective Cohort Study" International Journal of Environmental Research and Public Health 16, no. 15: 2635. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16152635