The Global Prevalence of Anxiety Among Medical Students: A Meta-Analysis

 , , , , and
, , , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Review Protocol and Registration
2.2. Search Strategy
2.3. Inclusion Criteria
2.4. Exclusion Criteria
2.5. Selection of Articles
2.6. Data Extraction and Study Evaluation
2.7. Statistical Analysis
2.8. Subgroup Analyses
3. Results
3.1. Quality of Studies
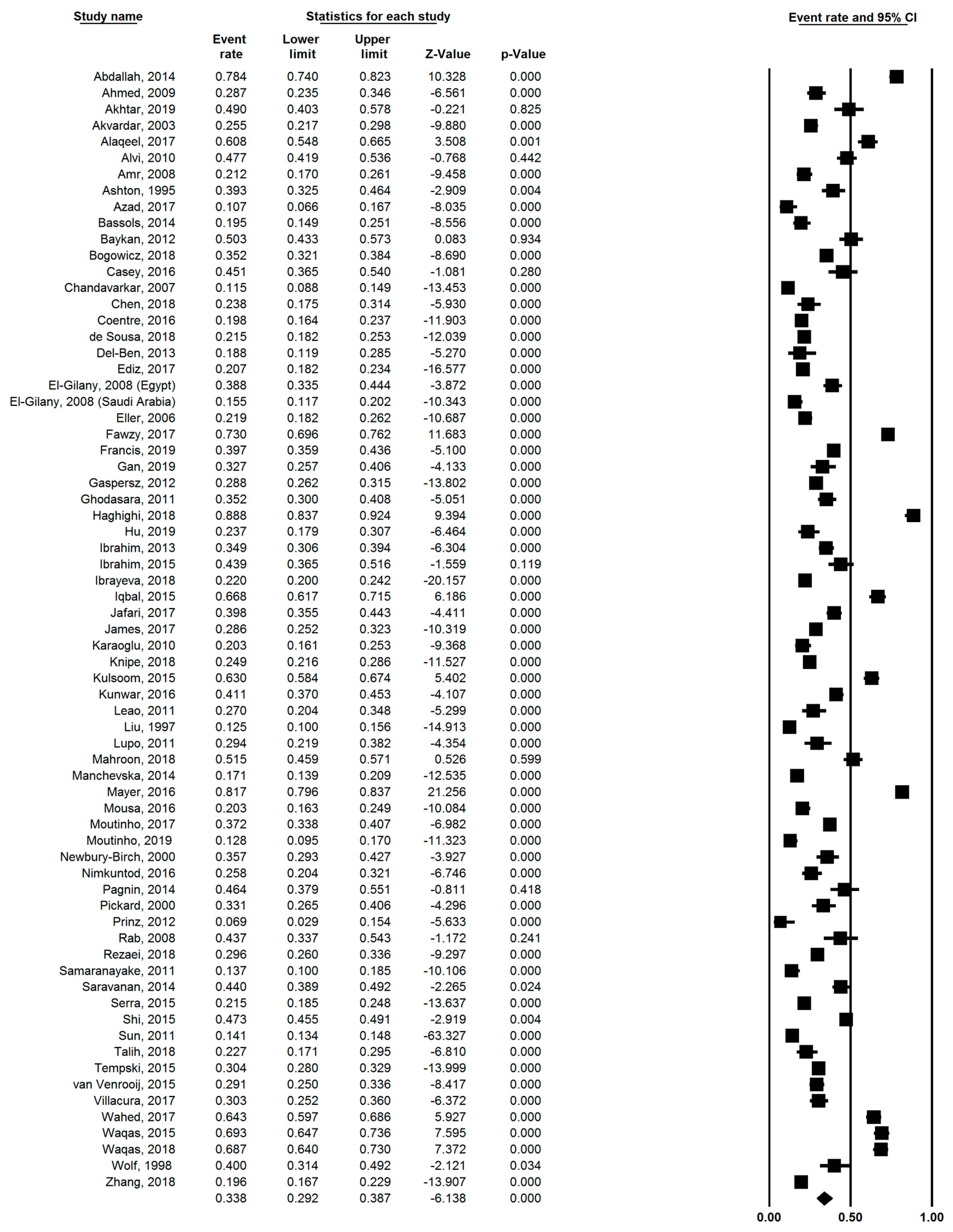
3.2. Pooled Prevalence
3.3. Subgroup Analyses
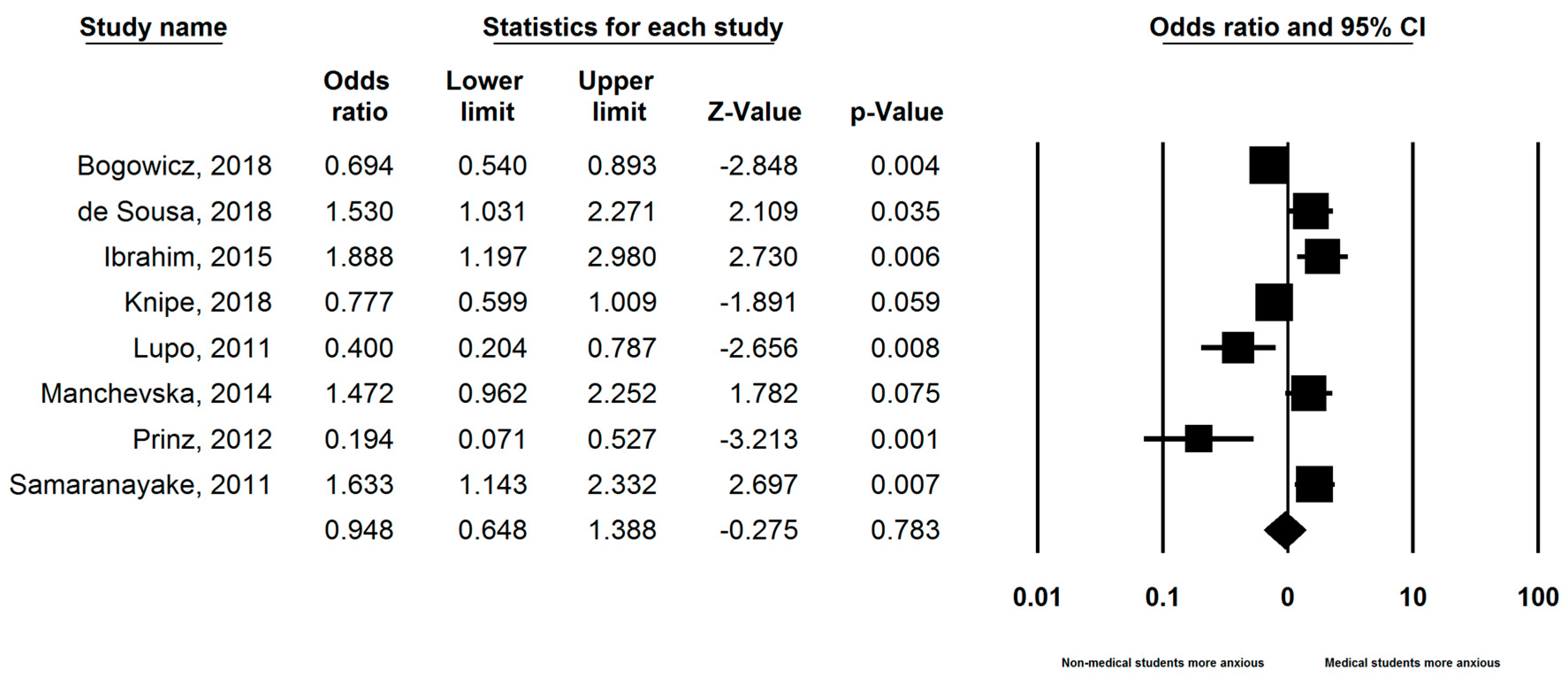
3.4. Comparison with Non-Medical Students
3.5. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Search Strategy
References
- Dyrbye, L.N.; Thomas, M.R.; Shanafelt, T.D. Systematic review of depression, anxiety, and other indicators of psychological distress among U.S. and Canadian medical students. Acad. Med. 2006, 81, 354–373. [Google Scholar] [CrossRef] [PubMed]
- Wolf, T.M. Stress, coping and health: Enhancing well-being during medical school. Med. Educ. 1994, 28, 8–17. [Google Scholar] [CrossRef] [PubMed]
- Mosley, T.H., Jr.; Perrin, S.G.; Neral, S.M.; Dubbert, P.M.; Grothues, C.A.; Pinto, B.M. Stress, coping, and well-being among third-year medical students. Acad. Med. 1994, 69, 765–767. [Google Scholar] [CrossRef] [PubMed]
- Aktekin, M.; Karaman, T.; Senol, Y.Y.; Erdem, S.; Erengin, H.; Akaydin, M. Anxiety, depression and stressful life events among medical students: A prospective study in Antalya, Turkey. Med. Educ. 2001, 35, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Weiller, E.; Bisserbe, J.C.; Maier, W.; Lecrubier, Y. Prevalence and recognition of anxiety syndromes in five European primary care settings. A report from the WHO study on Psychological Problems in General Health Care. Br. J. Psychiatry Suppl. 1998, 34, 18–23. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.; Monahan, P.O.; Lowe, B. Anxiety disorders in primary care: Prevalence, impairment, comorbidity, and detection. Ann. Intern. Med. 2007, 146, 317–325. [Google Scholar] [CrossRef]
- Rynn, M.A.; Brawman-Mintzer, O. Generalized anxiety disorder: Acute and chronic treatment. CNS Spectr 2004, 9, 716–723. [Google Scholar] [CrossRef]
- Testa, A.; Giannuzzi, R.; Sollazzo, F.; Petrongolo, L.; Bernardini, L.; Daini, S. Psychiatric emergencies (part I): Psychiatric disorders causing organic symptoms. Eur. Rev. Med. Pharmacol. Sci. 2013, 17 (Suppl. 1), 55–64. [Google Scholar]
- Eysenck, M.W.; Derakshan, N.; Santos, R.; Calvo, M.G. Anxiety and cognitive performance: Attentional control theory. Emotion 2007, 7, 336–353. [Google Scholar] [CrossRef]
- Moran, T.P. Anxiety and working memory capacity: A meta-analysis and narrative review. Psychol. Bull. 2016, 142, 831–864. [Google Scholar] [CrossRef]
- Runswick, O.R.; Roca, A.; Williams, A.M.; Bezodis, N.E.; North, J.S. The effects of anxiety and situation-specific context on perceptual-motor skill: A multi-level investigation. Psychol. Res. 2018, 82, 708–719. [Google Scholar] [CrossRef] [PubMed]
- Hope, V.; Hendersony, M. Medical student depression, anxiety and distress outside North America: A systematic review. Med. Educ. 2014, 48, 963–979. [Google Scholar] [CrossRef] [PubMed]
- Khuwaja, A.K.; Qureshi, R.; Azam, S.I. Prevalence and factors associated with anxiety and depression among family practitioners in Karachi, Pakistan. J. Pak. Med. Assoc. 2004, 54, 45–49. [Google Scholar] [PubMed]
- Al Saadi, T.; Zaher Addeen, S.; Turk, T.; Abbas, F.; Alkhatib, M. Psychological distress among medical students in conflicts: A cross-sectional study from Syria. BMC Med. Educ. 2017, 17, 173. [Google Scholar] [CrossRef] [PubMed]
- Carter, F.; Bell, C.; Ali, A.; McKenzie, J.; Boden, J.M.; Wilkinson, T.; Bell, C. Predictors of psychological resilience amongst medical students following major earthquakes. N. Z. Med. J. 2016, 129, 17–22. [Google Scholar] [PubMed]
- Loh, L.C.; Ali, A.M.; Ang, T.H.; Chelliah, A. Impact of a spreading epidemic on medical students. Malays 2005, 12, 43–49. [Google Scholar]
- Wong, T.W.; Gao, Y.; Tam, W.W.S. Anxiety among university students during the SARS epidemic in Hong Kong. Stress Health: J. Int. Soc. Investig. Stress 2007, 23, 31–35. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Herzog, R.; Alvarez-Pasquin, M.J.; Diaz, C.; Del Barrio, J.L.; Estrada, J.M.; Gil, A. Are healthcare workers intentions to vaccinate related to their knowledge, beliefs and attitudes? A systematic review. BMC Public Health 2013, 13, 154. [Google Scholar] [CrossRef]
- Hedges, L.V.; Vevea, J.L. Fixed-and random-effects models in meta-analysis. Psychol. Methods 1998, 3, 486. [Google Scholar] [CrossRef]
- Ho, R.C.; Zhang, M.W.; Tsang, T.Y.; Toh, A.H.; Pan, F.; Lu, Y.; Cheng, C.; Yip, P.S.; Lam, L.T.; Lai, C.M.; et al. The association between internet addiction and psychiatric co-morbidity: A meta-analysis. BMC Psychiatry 2014, 14, 183. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- UN Statistics Division. Standard Country or Area Codes for Statistical Use; UN Statistics Division: New York, NY, USA, 2010. [Google Scholar]
- Beck, A.T.; Epstein, N.; Brown, G.; Steer, R.A. An inventory for measuring clinical anxiety: Psychometric properties. J. Consult. Clin. Psychol. 1988, 56, 893. [Google Scholar] [CrossRef] [PubMed]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef]
- Lovibond, S.H.; Lovibond, P.F. Manual for the Depression Anxiety Stress Scales; Psychology Foundation: Sydney, Australia, 1995. [Google Scholar]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [PubMed]
- Abdallah, A.R.; Gabr, H.M. Depression, anxiety and stress among first year medical students in an Egyptian public university. Int. Res. J. Med. Sci. 2014, 2, 11–19. [Google Scholar]
- Ahmed, I.; Banu, H.; Al-Fageer, R.; Al-Suwaidi, R. Cognitive emotions: Depression and anxiety in medical students and staff. J. Crit. Care 2009, 24, e1–e7. [Google Scholar] [CrossRef]
- Akhtar, M.; Herwig, B.K.; Faize, F.A. Depression and Anxiety among International Medical Students in Germany: The Predictive Role of Coping Styles. JPMA J. Pak. Med. Assoc. 2019, 69, 230–234. [Google Scholar]
- Akvardar, Y.; Demiral, Y.; Ergor, G.; Ergor, A.; Bilici, M.; Ozer, O.A. Substance use in a sample of Turkish medical students. Drug Alcohol Depend. 2003, 72, 117–121. [Google Scholar] [CrossRef]
- Alaqeel, M.K.; Alowaimer, N.A.; Alonezan, A.F.; Almegbel, N.Y.; Alaujan, F.Y. Prevalence of Irritable Bowel Syndrome and Its Association with Anxiety among Medical Students at King Saud bin Abdulaziz University for Health Sciences in Riyadh. Pak. J. Med. Sci. 2017, 33, 33–36. [Google Scholar] [CrossRef]
- Alvi, T.; Assad, F.; Ramzan, M.; Khan, F.A. Depression, anxiety and their associated factors among medical students. J. Coll. Physicians Surg. Pak. 2010, 20, 122–126. [Google Scholar]
- Amr, M.; El Gilany, A.H.; El-Hawary, A. Does gender predict medical students’ stress in Mansoura, Egypt? Med. Educ. Online 2008, 13, 12. [Google Scholar] [CrossRef]
- Ashton, C.; Kamali, F. Personality, lifestyles, alcohol and drug consumption in a sample of British medical students. Med. Educ. 1995, 29, 187–192. [Google Scholar] [CrossRef]
- Azad, N.; Shahid, A.; Abbas, N.; Shaheen, A.; Munir, N. Anxiety And Depression in Medical Students of a Private Medical College. J. Ayub Med. Coll. Abbottabad 2017, 29, 123–127. [Google Scholar]
- Bassols, A.M.; Okabayashi, L.S.; Silva, A.B.; Carneiro, B.B.; Feijo, F.; Guimaraes, G.C.; Cortes, G.N.; Rohde, L.A.; Eizirik, C.L. First- and last-year medical students: Is there a difference in the prevalence and intensity of anxiety and depressive symptoms? Braz J. Psychiatry 2014, 36, 233–240. [Google Scholar] [CrossRef]
- Baykan, Z.; Nacar, M.; Cetinkaya, F. Depression, anxiety, and stress among last-year students at Erciyes University Medical School. Acad. Psychiatry 2012, 36, 64–65. [Google Scholar] [CrossRef]
- Bogowicz, P.; Ferguson, J.; Gilvarry, E.; Kamali, F.; Kaner, E.; Newbury-Birch, D. Alcohol and other substance use among medical and law students at a UK university: A cross-sectional questionnaire survey. Postgrad. Med. J. 2018, 94, 131–136. [Google Scholar] [CrossRef]
- Casey, D.; Thomas, S.; Hocking, D.R.; Kemp-Casey, A. Graduate-entry medical students: Older and wiser but not less distressed. Australas. Psychiatry 2016, 24, 88–92. [Google Scholar] [CrossRef]
- Chandavarkar, U.; Azzam, A.; Mathews, C.A. Anxiety symptoms and perceived performance in medical students. Depress. Anxiety 2007, 24, 103–111. [Google Scholar] [CrossRef]
- Chen, C.Y.; Yu, N.W.; Huang, T.H.; Wang, W.S.; Fang, J.T. Harm avoidance and depression, anxiety, insomnia, and migraine in fifth-year medical students in Taiwan. Neuropsychiatr. Dis. Treat. 2018, 14, 1273–1280. [Google Scholar] [CrossRef]
- Coentre, R.; Faravelli, C.; Figueira, M.L. Assessment of depression and suicidal behaviour among medical students in Portugal. Int. J. Med. Educ. 2016, 7, 354–363. [Google Scholar] [CrossRef] [Green Version]
- Moreira de Sousa, J.; Moreira, C.A.; Telles-Correia, D. Anxiety, Depression and Academic Performance: A Study Amongst Portuguese Medical Students Versus Non-Medical Students. Acta Med. Port. 2018, 31, 454–462. [Google Scholar] [CrossRef]
- Del-Ben, C.M.; Machado, V.F.; Madisson, M.M.; Resende, T.L.; Valerio, F.P.; De Almeida Troncon, L.E. Relationship between academic performance and affective changes during the first year at medical school. Med. Teach. 2013, 35, 404–410. [Google Scholar] [CrossRef]
- Ediz, B.; Ozcakir, A.; Bilgel, N. Depression and anxiety among medical students: Examining scores of the beck depression and anxiety inventory and the depression anxiety and stress scale with student characteristics. Cogent Psychol. 2017, 4, 1283829. [Google Scholar] [CrossRef]
- El-Gilany, A.H.; Amr, M.; Hammad, S. Perceived stress among male medical students in Egypt and Saudi Arabia: Effect of sociodemographic factors. Ann. Saudi Med. 2008, 28, 442–448. [Google Scholar]
- Eller, T.; Aluoja, A.; Vasar, V.; Veldi, M. Symptoms of anxiety and depression in Estonian medical students with sleep problems. Depress. Anxiety 2006, 23, 250–256. [Google Scholar] [CrossRef]
- Fawzy, M.; Hamed, S.A. Prevalence of psychological stress, depression and anxiety among medical students in Egypt. Psychiatry Res. 2017, 255, 186–194. [Google Scholar] [CrossRef]
- Francis, B.; Gill, J.S.; Yit Han, N.; Petrus, C.F.; Azhar, F.L.; Ahmad Sabki, Z.; Said, M.A.; Ong Hui, K.; Chong Guan, N.; Sulaiman, A.H. Religious Coping, Religiosity, Depression and Anxiety among Medical Students in a Multi-Religious Setting. Int. J. Environ. Res. Public Health 2019, 16, 259. [Google Scholar] [CrossRef]
- Gan, G.G.; Yuen Ling, H. Anxiety, depression and quality of life of medical students in Malaysia. Med. J. Malays. 2019, 74, 57–61. [Google Scholar]
- Garcia, A.; Romero, C.; Arroyave, C.; Giraldo, F.; Sanchez, L.; Sanchez, J. Acute effects of energy drinks in medical students. Eur. J. Nutr. 2017, 56, 2081–2091. [Google Scholar] [CrossRef]
- Ghodasara, S.L.; Davidson, M.A.; Reich, M.S.; Savoie, C.V.; Rodgers, S.M. Assessing student mental health at the Vanderbilt University School of Medicine. Acad. Med. 2011, 86, 116–121. [Google Scholar] [CrossRef]
- Haghighi, M.; Gerber, M. Does mental toughness buffer the relationship between perceived stress, depression, burnout, anxiety, and sleep? Int. J. Stress Manag. 2018. [Google Scholar] [CrossRef]
- Hu, K.S.; Chibnall, J.T.; Slavin, S.J. Maladaptive perfectionism, impostorism, and cognitive distortions: Threats to the mental health of pre-clinical medical students. Acad. Psychiatry 2019, 43, 381–385. [Google Scholar] [CrossRef]
- Ibrahim, N.; Al-Kharboush, D.; El-Khatib, L.; Al-Habib, A.; Asali, D. Prevalence and Predictors of Anxiety and Depression among Female Medical Students in King Abdulaziz University, Jeddah, Saudi Arabia. Iran. J. Public Health 2013, 42, 726–736. [Google Scholar]
- Ibrahim, M.B.; Abdelreheem, M.H. Prevalence of anxiety and depression among medical and pharmaceutical students in Alexandria University. Alex. J. Med. 2015, 51, 167–173. [Google Scholar] [CrossRef]
- Ibrayeva, Z.; Aldyngurov, D.; Myssayev, A.; Meirmanov, S.; Zhanaspayev, M.; Khismetova, Z.; Muzdubayeva, Z.; Smail, E.; Yurkovskaya, O.; Pivina, L.; et al. Depression, Anxiety and Somatic Distress in Domestic and International Undergraduate Medical Students in Kazakhstan. Iran. J. Public Health 2018, 47, 919–921. [Google Scholar]
- Iqbal, S.; Gupta, S.; Venkatarao, E. Stress, anxiety and depression among medical undergraduate students and their socio-demographic correlates. Indian J. Med. Res. 2015, 141, 354–357. [Google Scholar]
- Jafari, P.; Nozari, F.; Ahrari, F.; Bagheri, Z. Measurement invariance of the Depression Anxiety Stress Scales-21 across medical student genders. Int. J. Med. Educ. 2017, 8, 116–122. [Google Scholar] [CrossRef] [Green Version]
- James, B.O.; Thomas, I.F.; Omoaregba, J.O.; Okogbenin, E.O.; Okonoda, K.M.; Ibrahim, A.W.; Salihu, A.S.; Oshodi, Y.O.; Orovwigho, A.; Odinka, P.C.; et al. Psychosocial correlates of perceived stress among undergraduate medical students in Nigeria. Int. J. Med. Educ. 2017, 8, 382–388. [Google Scholar] [CrossRef] [Green Version]
- Karaoglu, N.; Seker, M. Anxiety and depression in medical students related to desire for and expectations from a medical career. West Indian Med. J. 2010, 59, 196–202. [Google Scholar]
- Knipe, D.; Maughan, C.; Gilbert, J.; Dymock, D.; Moran, P.; Gunnell, D. Mental health in medical, dentistry and veterinary students: Cross-sectional online survey. BJPsych Open 2018, 4, 441–446. [Google Scholar] [CrossRef]
- Kulsoom, B.; Afsar, N.A. Stress, anxiety, and depression among medical students in a multiethnic setting. Neuropsychiatr. Dis. Treat. 2015, 11, 1713–1722. [Google Scholar] [CrossRef]
- Kunwar, D.; Risal, A.; Koirala, S. Study of Depression, Anxiety and Stress among the Medical Students in two Medical Colleges of Nepal. Kathmandu Univ. Med. J. 2016, 14, 22–26. [Google Scholar]
- Leao, P.B.; Martins, L.A.; Menezes, P.R.; Bellodi, P.L. Well-being and help-seeking: An exploratory study among final-year medical students. Rev. Assoc. Med. Bras. 2011, 57, 379–386. [Google Scholar] [CrossRef]
- Liu, X.; Oda, S.; Peng, X.; Asai, K. Life events and anxiety in Chinese medical students. Soc. Psychiatry Psychiatr. Epidemiol. 1997, 32, 63–67. [Google Scholar] [CrossRef]
- Lupo, M.K.; Strous, R.D. Religiosity, anxiety and depression among Israeli medical students. Isr. Med. Assoc. J. 2011, 13, 613–618. [Google Scholar]
- Mahroon, Z.A.; Borgan, S.M.; Kamel, C.; Maddison, W.; Royston, M.; Donnellan, C. Factors associated with depression and anxiety symptoms among medical students in Bahrain. Acad. Psychiatry 2018, 42, 31–40. [Google Scholar] [CrossRef]
- Manchevska, S.; Pluncevic-Gligoroska, J. The prevalence of high anxiety and substance use in university students in the Republic of Macedonia. Pril (Makedon Akad Nauk Umet Odd Med. Nauki) 2014, 35, 67–74. [Google Scholar] [CrossRef]
- Brenneisen Mayer, F.; Souza Santos, I.; Silveira, P.S.; Itaqui Lopes, M.H.; de Souza, A.R.; Campos, E.P.; de Abreu, B.A.; Hoffman Ii, I.; Magalhaes, C.R.; Lima, M.C.; et al. Factors associated to depression and anxiety in medical students: A multicenter study. BMC Med. Educ. 2016, 16, 282. [Google Scholar] [CrossRef]
- Mousa, O.Y.; Dhamoon, M.S.; Lander, S.; Dhamoon, A.S. The MD Blues: Under-Recognized Depression and Anxiety in Medical Trainees. PLoS ONE 2016, 11, e0156554. [Google Scholar] [CrossRef]
- Moutinho, I.L.; Maddalena, N.C.; Roland, R.K.; Lucchetti, A.L.; Tibirica, S.H.; Ezequiel, O.D.; Lucchetti, G. Depression, stress and anxiety in medical students: A cross-sectional comparison between students from different semesters. Rev. Assoc. Med. Bras. (1992) 2017, 63, 21–28. [Google Scholar] [CrossRef]
- Moutinho, I.L.D.; Lucchetti, A.L.G.; Ezequiel, O.D.S.; Lucchetti, G. Mental health and quality of life of Brazilian medical students: Incidence, prevalence, and associated factors within two years of follow-up. Psychiatry Res. 2019, 274, 306–312. [Google Scholar] [CrossRef]
- Newbury-Birch, D.; White, M.; Kamali, F. Factors influencing alcohol and illicit drug use amongst medical students. Drug Alcohol Depend. 2000, 59, 125–130. [Google Scholar] [CrossRef]
- O’Flynn, J.; Dinan, T.G.; Kelly, J.R. Examining stress: An investigation of stress, mood and exercise in medical students. Ir. J. Psychol. Med. 2018, 35, 63–68. [Google Scholar] [CrossRef]
- Pagnin, D.; de Queiroz, V.; Carvalho, Y.T.M.S.; Dutra, A.S.S.; Amaral, M.B.; Queiroz, T.T. The relation between burnout and sleep disorders in medical students. Acad. Psychiatry 2014, 38, 438–444. [Google Scholar] [CrossRef]
- Pickard, M.; Bates, L.; Dorian, M.; Greig, H.; Saint, D. Alcohol and drug use in second-year medical students at the University of Leeds. Med. Educ. 2000, 34, 148–150. [Google Scholar] [CrossRef]
- Prinz, P.; Hertrich, K.; Hirschfelder, U.; de Zwaan, M. Burnout, depression and depersonalisation--psychological factors and coping strategies in dental and medical students. GMS Z Med. Ausbild 2012, 29, Doc10. [Google Scholar] [CrossRef]
- Rab, F.; Mamdou, R.; Nasir, S. Rates of depression and anxiety among female medical students in Pakistan. East Mediterr Health J. 2008, 14, 126–133. [Google Scholar]
- Rezaei, M.; Khormali, M.; Akbarpour, S.; Sadeghniiat-Hagighi, K.; Shamsipour, M. Sleep quality and its association with psychological distress and sleep hygiene: A cross-sectional study among pre-clinical medical students. Sleep Sci. 2018, 11, 274–280. [Google Scholar] [CrossRef]
- Samaranayake, C.B.; Fernando, A.T. Satisfaction with life and depression among medical students in Auckland, New Zealand. N. Z. Med. J. 2011, 124, 12–17. [Google Scholar]
- Saravanan, C.; Wilks, R. Medical students’ experience of and reaction to stress: The role of depression and anxiety. Sci. World J. 2014, 2014, 737382. [Google Scholar] [CrossRef]
- Serra, R.D.; Dinato, S.L.M.E.; Caseiro, M.M. Prevalence of depressive and anxiety symptoms in medical students in the city of Santos. J. Bras. Psiquiatr. 2015, 64, 213–220. [Google Scholar] [CrossRef] [Green Version]
- Shi, M.; Liu, L.; Wang, Z.Y.; Wang, L. The mediating role of resilience in the relationship between big five personality and anxiety among Chinese medical students: A cross-sectional study. PLoS ONE 2015, 10, e0119916. [Google Scholar] [CrossRef]
- Sun, L.; Sun, L.-N.; Sun, Y.-H.; Yang, L.-S.; Wu, H.-Y.; Zhang, D.-D.; Cao, H.-Y.; Sun, Y. Correlations between psychological symptoms and social relationships among medical undergraduates in Anhui Province of China. Int. J. Psychiatry Med. 2011, 42, 29–47. [Google Scholar] [CrossRef]
- Talih, F.; Daher, M.; Daou, D.; Ajaltouni, J. Examining burnout, depression, and attitudes regarding drug use among lebanese medical students during the 4 years of medical school. Acad. Psychiatry 2018. [Google Scholar] [CrossRef]
- Tempski, P.; Santos, I.S.; Mayer, F.B.; Enns, S.C.; Perotta, B.; Paro, H.B.; Gannam, S.; Peleias, M.; Garcia, V.L.; Baldassin, S.; et al. Relationship among Medical Student Resilience, Educational Environment and Quality of Life. PLoS ONE 2015, 10, e0131535. [Google Scholar] [CrossRef]
- van Venrooij, L.T.; Barnhoorn, P.C.; Giltay, E.J.; van Noorden, M.S. Burnout, depression and anxiety in preclinical medical students: A cross-sectional survey. Int. J. Adolesc. Med. Health 2015, 29. [Google Scholar] [CrossRef]
- Villacura, L.; Irarrazabal, N.; Lopez, I. Evaluation of depressive and anxiety symptomatology in medical students at the University of Chile. Ment. Health Prev. 2017, 7, 45–49. [Google Scholar] [CrossRef]
- Wahed, W.Y.A.; Hassan, S.K. Prevalence and associated factors of stress, anxiety and depression among medical Fayoum University students. Alex. J. Med. 2017, 53, 77–84. [Google Scholar] [CrossRef] [Green Version]
- Waqas, A.; Rehman, A.; Malik, A.; Muhammad, U.; Khan, S.; Mahmood, N. Association of Ego Defense Mechanisms with Academic Performance, Anxiety and Depression in Medical Students: A Mixed Methods Study. Cureus 2015, 7, e337. [Google Scholar] [CrossRef] [Green Version]
- Waqas, A.; Naveed, S.; Aedma, K.K.; Tariq, M.; Afzaal, T. Exploring clusters of defense styles, psychiatric symptoms and academic achievements among medical students: A cross-sectional study in Pakistan. BMC Res. Notes 2018, 11, 782. [Google Scholar] [CrossRef] [PubMed]
- Wolf, T.M.; Scurria, P.L.; Webster, M.G. A four-year study of anxiety, depression, loneliness, social support, and perceived mistreatment in medical students. J. Health Psychol. 1998, 3, 125–136. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Xiong, Y.; Dong, J.; Guo, T.; Tang, X.; Zhao, Y. Caffeinated Drinks Intake, Late Chronotype, and Increased Body Mass Index among Medical Students in Chongqing, China: A Multiple Mediation Model. Int. J. Environ. Res. Public Health 2018, 15, 1721. [Google Scholar] [CrossRef]
- Henry, J.D.; Crawford, J.R. The short-form version of the Depression Anxiety Stress Scales (DASS-21): Construct validity and normative data in a large non-clinical sample. Br. J. Clin. Psychol. 2005, 44, 227–239. [Google Scholar] [CrossRef] [Green Version]
- Kader Maideen, S.F.; Mohd Sidik, S.; Rampal, L.; Mukhtar, F. Prevalence, associated factors and predictors of anxiety: A community survey in Selangor, Malaysia. BMC Psychiatry 2015, 15, 262. [Google Scholar] [CrossRef]
- Gillis, M.M.; Haaga, D.A.F.; Ford, G.T. Normative values for the Beck Anxiety Inventory, Fear Questionnaire, Penn State Worry Questionnaire, and Social Phobia and Anxiety Inventory. Psychol. Assess. 1995, 7, 450. [Google Scholar] [CrossRef]
- Lisspers, J.; Nygren, A.; Söderman, E. Hospital Anxiety and Depression Scale (HAD): some psychometric data for a Swedish sample. Acta Psychiatr. Scand. 1997, 96, 281–286. [Google Scholar] [CrossRef]
- Enns, M.W.; Cox, B.J.; Sareen, J.; Freeman, P. Adaptive and maladaptive perfectionism in medical students: A longitudinal investigation. Med. Educ. 2001, 35, 1034–1042. [Google Scholar] [CrossRef]
- Kawamura, K.Y.; Hunt, S.L.; Frost, R.O.; DiBartolo, P.M. Perfectionism, anxiety, and depression: Are the relationships independent? Cognit. Ther. Res. 2001, 25, 291–301. [Google Scholar] [CrossRef]
- Guthrie, E.A.; Black, D.; Shaw, C.M.; Hamilton, J.; Creed, F.H.; Tomenson, B. Embarking upon a medical career: Psychological morbidity in first year medical students. Med. Educ. 1995, 29, 337–341. [Google Scholar] [CrossRef] [PubMed]
- Wolf, T.M.; Faucett, J.M.; Randall, H.M.; Balson, P.M. Graduating medical students’ ratings of stresses, pleasures, and coping strategies. J. Med. Educ. 1988, 63, 636–642. [Google Scholar] [PubMed]
- Williams, C.M.; Wilson, C.C.; Olsen, C.H. Dying, death, and medical education: Student voices. J. Palliat. Med. 2005, 8, 372–381. [Google Scholar] [CrossRef] [PubMed]
- Richman, J.A.; Flaherty, J.A.; Rospenda, K.M.; Christensen, M.L. Mental health consequences and correlates of reported medical student abuse. JAMA 1992, 267, 692–694. [Google Scholar] [CrossRef] [PubMed]
- Abdullah, T.; Brown, T.L. Mental illness stigma and ethnocultural beliefs, values, and norms: An integrative review. Clin. Psychol. Rev. 2011, 31, 934–948. [Google Scholar] [CrossRef] [PubMed]
- Littlewood, R.; Jadhav, S.; Ryder, A.G. A cross-national study of the stigmatization of severe psychiatric illness: Historical review, methodological considerations and development of the questionnaire. Transcult. Psychiatry 2007, 44, 171–202. [Google Scholar] [CrossRef] [PubMed]
- Rao, D.; Feinglass, J.; Corrigan, P. Racial and ethnic disparities in mental illness stigma. J. Nerv. Ment. Dis. 2007, 195, 1020–1023. [Google Scholar] [CrossRef] [PubMed]
- Baxter, A.; Scott, K.; Vos, T.; Whiteford, H. Global prevalence of anxiety disorders: A systematic review and meta-regression. Psychol. Med. 2013, 43, 897–910. [Google Scholar] [CrossRef] [PubMed]
- Wolf, T.M.; Kissling, G.E.; Burgess, L.A. Lifestyle characteristics during medical school: A four-year cross-sectional study. Psychol. Rep. 1986, 59, 179–189. [Google Scholar] [CrossRef] [PubMed]
- Niemi, P.; Vainiomäki, P. Medical students’ distress–quality, continuity and gender differences during a six-year medical programme. Med. Teach. 2006, 28, 136–141. [Google Scholar] [CrossRef]
- Roberts, L.W.; Warner, T.D.; Lyketsos, C.; Frank, E.; Ganzini, L.; Carter, D. Perceptions of academic vulnerability associated with personal illness: A study of 1027 students at nine medical schools. Collaborative Research Group on Medical Student Health. Compr. Psychiatry 2001, 42, 1–15. [Google Scholar] [CrossRef]
- Chew-Graham, C.A.; Rogers, A.; Yassin, N. I wouldn’t want it on my CV or their records: Medical students’ experiences of help-seeking for mental health problems. Med. Educ. 2003, 37, 873–880. [Google Scholar] [CrossRef] [PubMed]
- Rapaport, M.H.; Clary, C.; Fayyad, R.; Endicott, J. Quality-of-life impairment in depressive and anxiety disorders. Am. J. Psychiatry 2005, 162, 1171–1178. [Google Scholar] [CrossRef] [PubMed]
- Sarnoff, I.; Zimbardo, P.G. Anxiety, fear, and social isolation. J. Abnorm. Soc.Psychol. 1961, 62, 356. [Google Scholar] [CrossRef] [PubMed]
- Sartorius, N.; Üstün, T.B.; Lecrubier, Y.; Wittchen, H.-U. Depression comorbid with anxiety: Results from the WHO study on psychological disorders in primary health care. Br. J. Psychiatry 1996, 168, 38–43. [Google Scholar] [CrossRef]
- Vorspan, F.; Mehtelli, W.; Dupuy, G.; Bloch, V.; Lepine, J.P. Anxiety and substance use disorders: Co-occurrence and clinical issues. Curr. Psychiatry Rep. 2015, 17, 4. [Google Scholar] [CrossRef] [PubMed]
- Krag, N.J.; Norregaard, J.; Larsen, J.K.; Danneskiold-Samsoe, B. A blinded, controlled evaluation of anxiety and depressive symptoms in patients with fibromyalgia, as measured by standardized psychometric interview scales. Acta Psychiatr. Scand. 1994, 89, 370–375. [Google Scholar] [CrossRef] [PubMed]
- Thieme, K.; Turk, D.C.; Flor, H. Comorbid depression and anxiety in fibromyalgia syndrome: Relationship to somatic and psychosocial variables. Psychosom. Med. 2004, 66, 837–844. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.S.; Lewin, A.B.; Murphy, T.K.; Storch, E.A. Misophonia: Incidence, phenomenology, and clinical correlates in an undergraduate student sample. J. Clin. Psychol. 2014, 70, 994–1007. [Google Scholar] [CrossRef]
- Quek, T.C.; Ho, C.S.; Choo, C.C.; Nguyen, L.H.; Tran, B.X.; Ho, R.C. Misophonia in Singaporean Psychiatric Patients: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2018, 15, 1410. [Google Scholar] [CrossRef]
- Lydiard, R.B. Irritable bowel syndrome, anxiety, and depression: What are the links? J. Clin. Psychiatry 2001, 62 (Suppl. 8), 38–45. discussion 46–37. [Google Scholar]
- Fond, G.; Loundou, A.; Hamdani, N.; Boukouaci, W.; Dargel, A.; Oliveira, J.; Roger, M.; Tamouza, R.; Leboyer, M.; Boyer, L. Anxiety and depression comorbidities in irritable bowel syndrome (IBS): A systematic review and meta-analysis. Eur. Arch. Psychiatry Clin. Neurosci. 2014, 264, 651–660. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, R.; Brazeau, C.M.; Zackin, F.; Rovi, S.; Dickey, J.; Johnson, M.S.; Keller, S.E. Do state medical board applications violate the americans with disabilities act? Acad. Med. 2009, 84, 776–781. [Google Scholar] [CrossRef] [PubMed]
- Givens, J.L.; Tjia, J. Depressed medical students’ use of mental health services and barriers to use. Acad. Med. 2002, 77, 918–921. [Google Scholar] [CrossRef] [PubMed]
- Aaronson, A.L.; Backes, K.; Agarwal, G.; Goldstein, J.L.; Anzia, J. Mental Health During Residency Training: Assessing the Barriers to Seeking Care. Acad. Psychiatry 2018, 42, 469–472. [Google Scholar] [CrossRef] [PubMed]
- Puthran, R.; Zhang, M.W.; Tam, W.W.; Ho, R.C. Prevalence of depression amongst medical students: A meta-analysis. Med. Educ. 2016, 50, 456–468. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Chu, F.; Wang, H.; Wang, X.P. Efficacy of Williams LifeSkills training for improving psychological health: A pilot comparison study of Chinese medical students. Asia Pac. Psychiatry 2014, 6, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Warnecke, E.; Quinn, S.; Ogden, K.; Towle, N.; Nelson, M.R. A randomised controlled trial of the effects of mindfulness practice on medical student stress levels. Med. Educ. 2011, 45, 381–388. [Google Scholar] [CrossRef]
- Vonnegut, M. A Doctor Shares His Story about Overcoming Mental Illness. 2015. Available online: KevinMD.com (accessed on 15 June 2019).




{kind=link}
{kind=link}
{kind=link}
| First Author, Year [ref] | Country | Continent | Sample Size | Number of Medical Students with Anxiety | Prevalence of Anxiety, % | Instrument Used a |
|---|---|---|---|---|---|---|
| Abdallah, 2014 [28] | Egypt | Middle East | 379 | 297 | 78.4 | DASS-21-A |
| Ahmed, 2009 [29] | UAE | Middle East | 254 | 73 | 28.7 | BAI-21 |
| Akhtar, 2019 [30] | Germany | Europe | 122 | 60 | 49.0 | BAI-21 |
| Akvardar, 2003 [31] | Turkey | Middle East | 447 | 114 | 25.5 | HADS-A |
| Alaqeel, 2017 [32] | Saudi Arabia | Middle East | 268 | 163 | 60.8 | DASS-21-A |
| Alvi, 2010 [33] | Pakistan | Asia | 279 | 133 | 47.7 | BAI-21 |
| Amr, 2008 [34] | Egypt | Middle East | 311 | 66 | 21.2 | HADS-A |
| Ashton, 1995 [35] | UK | Europe | 186 | 73 | 39.3 | HADS-A |
| Azad, 2017 [36] | Pakistan | Asia | 150 | 16 | 10.7 | BAI-21 |
| Bassols, 2014 [37] | Brazil | South America | 232 | 45 | 19.5 | BAI-21 |
| Baykan, 2012 [38] | Turkey | Middle East | 193 | 97 | 50.3 | DASS-21-A |
| Bogowicz, 2018 [39] | UK | Europe | 889 | 313 | 35.2 | HADS-A |
| Casey, 2016 [40] | Australia | Oceania | 122 | 55 | 45.1 | DASS-21 |
| Chandavarkar, 2007 [41] | USA | North America | 427 | 49 | 11.5 | STAI-Trait |
| Chen, 2018 [42] | Taiwan | Asia | 143 | 34 | 23.8 | BAI-21 |
| Coentre, 2016 [43] | Portugal | Europe | 456 | 90 | 19.8 | ZSAS |
| de Sousa, 2018 [44] | Portugal | Europe | 512 | 121 | 23.6 | HADS-A |
| Del-Ben, 2013 [45] | Brazil | South America | 85 | 16 | 18.8 | BAI-21 |
| Ediz, 2017 [46] | Turkey | Middle East | 928 | 192 | 20.7 | BAI-21 |
| El-Gilany,2008 [47] (Egypt) | Egypt | Middle East | 304 | 118 | 38.8 | BAI-21 |
| El-Gilany, 2008 [47] (Saudi Arabia) | Saudi Arabia | Middle East | 284 | 44 | 15.5 | BAI-21 |
| Eller, 2006 [48] | Estonia | Europe | 413 | 90 | 21.9 | EST-Q |
| Fawzy, 2017 [49] | Egypt | Middle East | 700 | 511 | 73.0 | DASS-21-A |
| Francis, 2019 [50] | Malaysia | Asia | 622 | 247 | 39.7 | HADS-A |
| Gan, 2019 [51] | Malaysia | Asia | 149 | 49 | 32.7 | HADS-A |
| Gaspersz, 2012 [52] | Netherlands | Europe | 1130 | 325 | 28.8 | BSI-ANG |
| Ghodasara, 2011 [53] | USA | North America | 301 | 106 | 35.2 | STAI-State |
| Haghighi, 2018 [54] | Iran | Middle East | 207 | 184 | 88.8 | STAI-Trait |
| Hu, 2019 [55] | USA | North America | 169 | 40 | 23.7 | STAI-State |
| Ibrahim, 2013 [56] | Saudi Arabia | Middle East | 450 | 157 | 34.9 | HADS-A |
| Ibrahim, 2015 [57] | Egypt | Middle East | 164 | 72 | 43.9 | BAI-21 |
| Ibrayeva, 2018 [58] | Kazakhstan | Asia | 1478 | 325 | 22.0 | GAD-7 |
| Iqbal, 2015 [59] | India | Asia | 353 | 236 | 66.8 | DASS-42-A |
| Jafari, 2017 [60] | Iran | Middle East | 477 | 190 | 39.8 | DASS-21-A |
| James, 2017 [61] | Nigeria | Africa | 623 | 178 | 28.6 | HADS-A |
| Karaoglu, 2010 [62] | Turkey | Middle East | 290 | 59 | 20.3 | BAI-21 |
| Knipe, 2018 [63] | UK | Europe | 583 | 145 | 24.9 | GAD-7 |
| Kulsoom, 2015 [64] | Saudi Arabia | Middle East | 442 | 283 | 64.0 | DASS-21-A |
| Kunwar, 2016 [65] | Nepal | Asia | 538 | 221 | 41.1 | DASS-21-A |
| Leao, 2011 [66] | Brazil | South America | 144 | 39 | 27.0 | BAI-21 |
| Liu, 1997 [67] | China | Asia | 537 | 67 | 12.5 | ZSAS |
| Lupo, 2011 [68] | Israel | Middle East | 119 | 35 | 29.4 | BAI-21 |
| Mahroon, 2018 [69] | Bahrain | Middle East | 307 | 158 | 51.5 | BAI-21 |
| Manchevska, 2014 [70] | Macedonia | Europe | 445 | 76 | 17.1 | BAI-21 |
| Mayer, 2016 [71] | Brazil | South America | 1350 | 1103 | 81.7 | STAI-State |
| Mousa, 2016 [72] | USA | North America | 336 | 68 | 20.3 | GAD-7 |
| Moutinho, 2017 [73] | Brazil | South America | 761 | 283 | 37.2 | DASS-21-A |
| Moutinho, 2019 [74] | Brazil | South America | 312 | 40 | 12.8 | DASS-21-A |
| Newbury-Birch, 2000 [75] | UK | Europe | 194 | 69 | 35.7 | HADS-A |
| Nimkuntod, 2016 [76] | Thailand | Asia | 213 | 55 | 25.8 | DASS-21-A |
| Pagnin, 2014 [77] | Brazil | South America | 127 | 59 | 46.4 | BAI-21 |
| Pickard, 2000 [78] | UK | Europe | 169 | 56 | 33.1 | HADS-A |
| Prinz, 2012 [79] | Germany | Europe | 73 | 5 | 6.8 | HADS-A |
| Rab, 2008 [80] | Pakistan | Asia | 87 | 38 | 43.7 | BAI-21 |
| Rezaei, 2018 [81] | Iran | Middle East | 553 | 164 | 29.6 | DASS-21-A |
| Samaranayake, 2011 [82] | New Zealand | Oceania | 255 | 35 | 13.7 | GAD-7 |
| Saravanan, 2014 [83] | Malaysia | Asia | 358 | 158 | 44.0 | DASS-21-A |
| Serra, 2015 [84] | Brazil | South America | 657 | 141 | 21.5 | BAI-21 |
| Shi, 2015 [85] | China | Asia | 2925 | 1384 | 47.3 | ZSAS |
| Sun, 2011 [86] | China | Asia | 10,140 | 1430 | 14.1 | BAI-21 |
| Talih, 2018 [87] | Lebanon | Middle East | 176 | 40 | 22.7 | GAD-7 |
| Tempski, 2015 [88] | Brazil | South America | 1350 | 410 | 30.4 | STAI-State |
| van Venrooij, 2015 [89] | Netherlands | Europe | 433 | 126 | 29.1 | SQ-48-A |
| Villacura, 2017 [90] | Chile | South America | 277 | 84 | 30.3 | BAI-21 |
| Wahed, 2017 [91] | Egypt | Middle East | 442 | 284 | 64.3 | DASS-21-A |
| Waqas, 2015 [92] | Pakistan | Asia | 409 | 283 | 69.3 | HADS-A |
| Waqas, 2018 [93] | Pakistan | Asia | 409 | 281 | 68.7 | HADS-A |
| Wolf, 1998 [94] | Hong Kong | Asia | 114 | 46 | 40.0 | BAI-21 |
| Zhang, 2018 [95] | China | Asia | 616 | 121 | 19.6 | DASS-21-A |
| Subgroups Comparison | Number of Studies, n | Pooled Prevalence, % | 95% Confidence Interval, % | p-Value |
|---|---|---|---|---|
| Continent | 0.04 * | |||
| Asia | 18 | 35.2 | 26.3–45.3 | |
| Middle East | 21 | 42.4 | 33.3–52.1 | |
| Rest of the World | 30 | 27.5 | 21.5–34.5 | |
| Gender | 0.16 | |||
| Female | 22 | 38.0 | 27.6–49.5 | |
| Male | 23 | 27.6 | 19.3–37.8 | |
| Year of study | 0.96 | |||
| Pre-clinical | 21 | 26.2 | 21.2–31.9 | |
| Clinical | 16 | 26.4 | 20.6–33.1 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tian-Ci Quek, T.; Wai-San Tam, W.; X. Tran, B.; Zhang, M.; Zhang, Z.; Su-Hui Ho, C.; Chun-Man Ho, R. The Global Prevalence of Anxiety Among Medical Students: A Meta-Analysis. Int. J. Environ. Res. Public Health 2019, 16, 2735. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16152735
Tian-Ci Quek T, Wai-San Tam W, X. Tran B, Zhang M, Zhang Z, Su-Hui Ho C, Chun-Man Ho R. The Global Prevalence of Anxiety Among Medical Students: A Meta-Analysis. International Journal of Environmental Research and Public Health. 2019; 16(15):2735. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16152735
Chicago/Turabian StyleTian-Ci Quek, Travis, Wilson Wai-San Tam, Bach X. Tran, Min Zhang, Zhisong Zhang, Cyrus Su-Hui Ho, and Roger Chun-Man Ho. 2019. "The Global Prevalence of Anxiety Among Medical Students: A Meta-Analysis" International Journal of Environmental Research and Public Health 16, no. 15: 2735. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16152735