Association between Peptic Ulcer Disease and Osteoporosis: The Population-Based Longitudinal Cohort Study in Korea


Abstract
:1. Strengths and Limitations of this Study
- ►
- This is a prospective study on a large cohort of participants, with a 12-year follow-up examination conducted.
- ►
- This study has considered age, hormone replacement therapy, and menopause in women to minimized confounding factors.
- ►
- This paper lacks information on the major factors of PUD such as H. pylori infection or the use of NSAIDs, which are study limitations.
2. Introduction
3. Methods
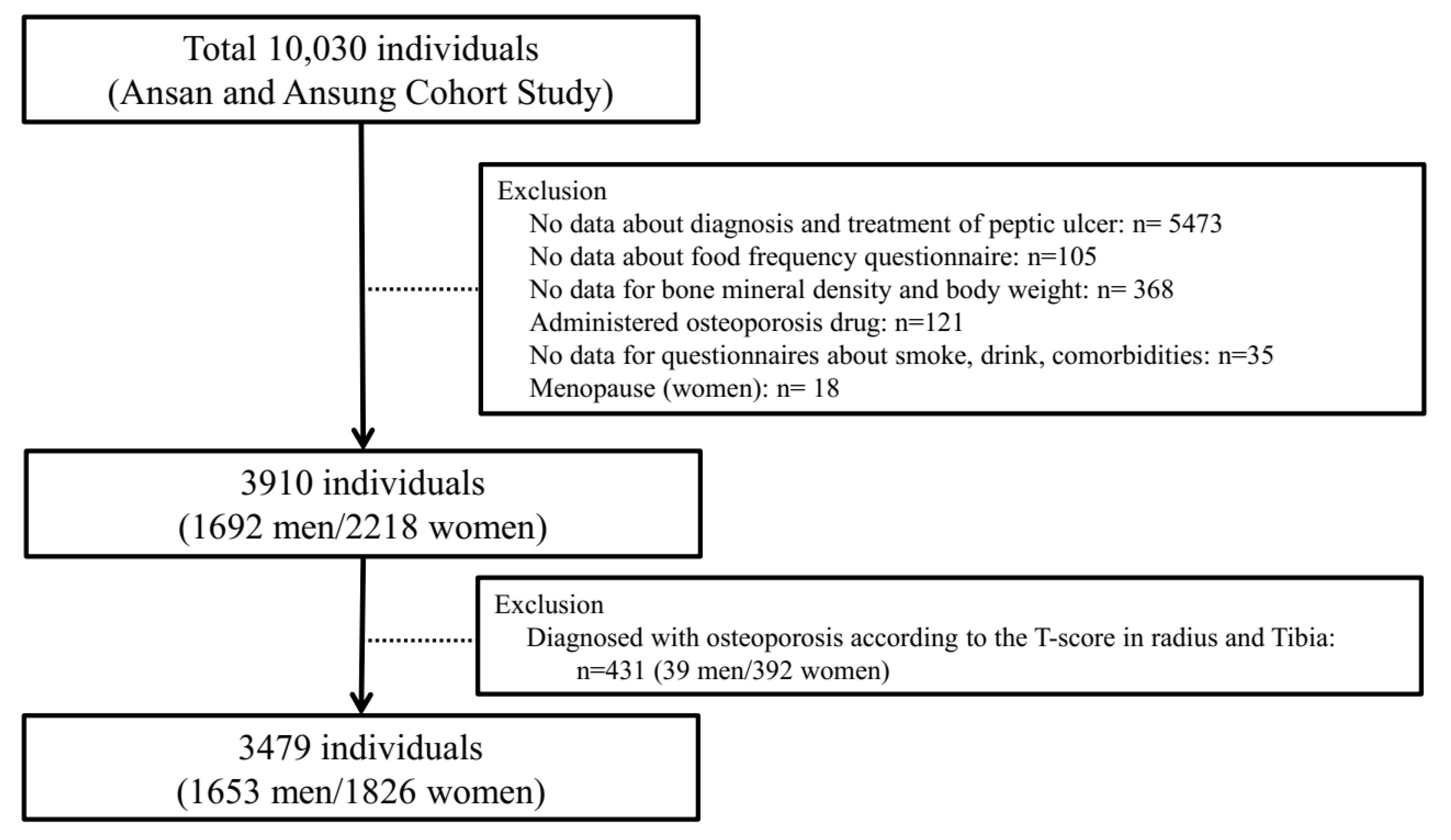
3.1. Study Participants
3.2. Questionnaires
3.3. Anthropometric Parameters and Bone Mass Density
3.4. Statistical Analysis
3.5. Patient and Public Involvement
4. Results
4.1. Baseline Characteristics of the Participants
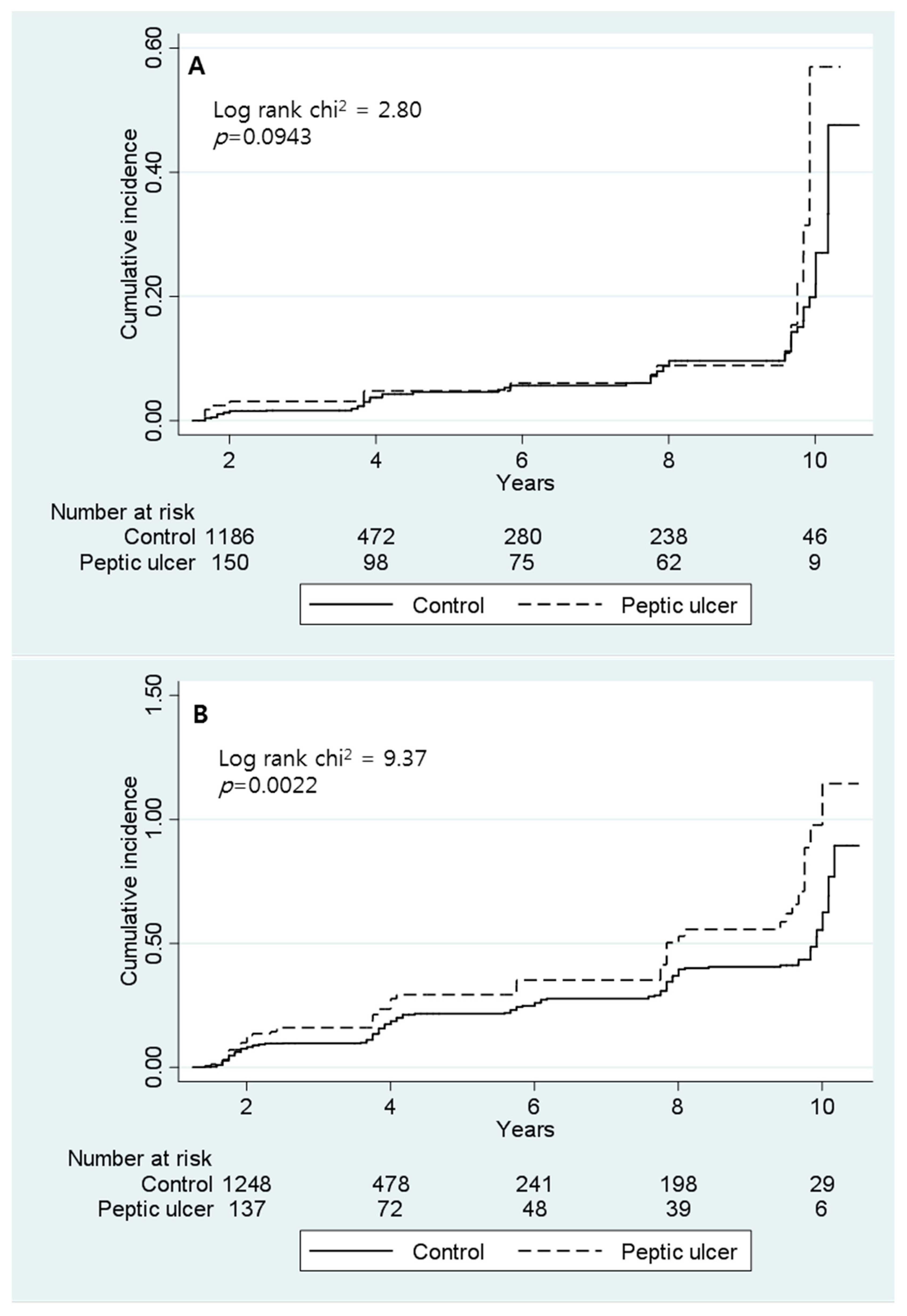
4.2. Incidence and HRs of Osteoporosis
4.3. Risk Factors of Osteoporosis
5. Discussion
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Patient Consent
Ethics Approval
Provenance and Peer Review
Data Sharing Statement Data
Appendix

{kind=link}
{kind=link}
| Variables | Men | p-Value | Women | p-Value | ||
|---|---|---|---|---|---|---|
| Ansung | Ansan | Ansung | Ansan | |||
| Participants, n | 520 | 1133 | 610 | 1216 | ||
| Calcium intake, mg/d | ||||||
| Quartile 1 | 219.1 ± 4.5 | 244.5 ± 3.3 | <0.001 | 200.7 ± 3.5 | 222.4 ± 3.1 | <0.001 |
| Quartile 2 | 376.3 ± 3.3 | 374.3 ± 2.3 | 0.622 | 363.4 ± 3.5 | 357.7 ± 2.2 | 0.158 |
| Quartile3 | 521.1 ± 4.8 | 517.8 ± 2.6 | 0.538 | 510.4 ± 3.8 | 512.3 ± 2.8 | 0.691 |
| Quartile 4 | 881.1 ± 24.2 | 808.2 ± 13.6 | 0.006 | 866.1 ± 26.9 | 791.5 ± 12.1 | 0.004 |
| Age, year | 57.4 ± 0.3 | 49.7 ± 0.2 | <0.001 | 56.2 ± 0.3 | 48.8 ± 0.2 | <0.001 |
| BMI, kg/m2 | 23.9 ± 0.1 | 24.7 ± 0.1 | <0.001 | 25.4 ± 0.1 | 24.8 ± 0.1 | 0.001 |
| Drinking Status, n(%) | <0.001 | 0.004 | ||||
| Never | 88 (16.9) | 237 (20.97) | 455 (74.6) | 851 (70.0) | ||
| Former | 106 (20.4) | 117 (10.33) | 28 (4.6) | 35 (2.9) | ||
| Current | 326 (62.7) | 779 (68.76) | 127 (20.8) | 330 (27.1) | ||
| Smoking status, n(%) | 0.053 | 0.173 | ||||
| Never | 85 (16.3) | 240 (21.2) | 575 (94.3) | 1169 (96.1) | ||
| Former | 187 (36.0) | 404 (35.6) | 8 (1.3) | 9 (0.8) | ||
| Current | 248 (47.7) | 489 (43.2) | 27 (4.4) | 38 (3.1) | ||
| Physical activity, MET-h/week | 30.2 ± 0.7 | 16.7 ± 0.3 | <0.001 | 27.9 ± 0.7 | 16.6 ± 0.3 | |
| Comorbidity, n(%) | ||||||
| Hypertension | 118 (36.1) | 218 (19.2) | <0.001 | 235 (38.5) | 183 (15.0) | <0.001 |
| Diabetes mellitus | 110 (21.1) | 123 (10.9) | <0.001 | 109 (17.9) | 67 (5.5) | <0.001 |
| Chronic kidney disease | 20 (3.8) | 24 (2.12) | 0.043 | 27 (4.4) | 45 (3.7) | 0.452 |
| Chronic pulmonary disease | 10 (1.9) | 8 (0.7) | 0.027 | 8 (1.3) | 4 (0.3) | 0.026 |
| Cerebrovascular disease | 14 (2.7) | 19 (1.7) | 0.171 | 12 (2.0) | 9 (0.7) | 0.020 |
| Coronary artery disease | 16 (3.1) | 13 (1.2) | 0.006 | 12 (2.0) | 7 (0.6) | 0.006 |
| Hepatitis | 41 (7.9) | 59 (5.2) | 0.034 | 26 (4.3) | 38 (3.1) | 0.213 |
| Hormone replacement therapy | 22 (3.6) | 88 (7.2) | 0.002 | |||
| Menopause | 481 (78.9) | 574 (47.2) | 0.001 | |||
References
- Sung, J.J.Y.; Kuipers, E.J.; El-Serag, H.B. Systematic review: The global incidence and prevalence of peptic ulcer disease. Aliment. Pharmacol. Ther. 2009, 29, 938–946. [Google Scholar] [CrossRef] [PubMed]
- Makola, D.; Peura, D.A.; Crowe, S.E. Helicobacter pylori Infection and Related Gastrointestinal Diseases. J. Clin. Gastroenterol. 2007, 41, 548–558. [Google Scholar] [CrossRef] [PubMed]
- Rosenstock, S.; Jørgensen, T.; Bonnevie, O.; Andersen, L. Risk factors for peptic ulcer disease: A population based prospective cohort study comprising 2416 Danish adults. Gut 2003, 52, 186–193. [Google Scholar] [CrossRef] [PubMed]
- Lau, J.Y.; Sung, J.; Hill, C.; Henderson, C.; Howden, C.W.; Metz, D.C. Systematic Review of the Epidemiology of Complicated Peptic Ulcer Disease: Incidence, Recurrence, Risk Factors and Mortality. Digestion 2011, 84, 102–113. [Google Scholar] [CrossRef] [PubMed]
- Klibanski, A.; Adams-Campbell, L.; Bassford, T.L.; Blair, S.N.; Boden, S.D.; Dickersin, K.; Gifford, D.R.; Glasse, L.; Goldring, S.R.; Hruska, K. Osteoporosis prevention, diagnosis, and therapy. JAMA 2001, 285, 785–795. [Google Scholar]
- Sozen, T.; Ozisik, L.; Basaran, N.C. An overview and management of osteoporosis. Eur. J. Rheumatol. 2017, 4, 46–56. [Google Scholar] [CrossRef] [PubMed]
- Bernabei, R.; Martone, A.M.; Ortolani, E.; Landi, F.; Marzetti, E. Screening, diagnosis and treatment of osteoporosis: A brief review. Clin. Cases Min. Bone Metab. 2014, 11, 201–207. [Google Scholar] [CrossRef]
- Harris, P.R.; Weber, H.C.; Wilcox, C.M.; Jensen, R.T.; Smith, P.D. Cytokine gene profile in gastric mucosa in Helicobacter pylori infection and Zollinger-Ellison syndrome. Am. J. Gastroenterol. 2002, 97, 312–318. [Google Scholar] [CrossRef] [PubMed]
- Naito, Y.; Yoshikawa, T. Molecular and cellular mechanisms involved in Helicobacter pylori-induced inflammation and oxidative stress. Free Radic. Biol. Med. 2002, 33, 323–336. [Google Scholar] [CrossRef]
- Raisz, L.G. Physiology and pathophysiology of bone remodeling. Clin. Chem. 1999, 45, 1353–1358. [Google Scholar]
- Katz, S.; Weinerman, S. Osteoporosis and gastrointestinal disease. Gastroenterol. Hepatol. 2010, 6, 506–517. [Google Scholar]
- Wu, C.H.; Tung, Y.C.; Chai, C.Y.; Lu, Y.Y.; Su, Y.F.; Tsai, T.H.; Kuo, K.L.; Lin, C.L. Increased Risk of Osteoporosis in Patients with Peptic Ulcer Disease: A Nationwide Population-Based Study. Medicine 2016, 95, e3309. [Google Scholar] [CrossRef] [PubMed]
- Sawicki, A.; Regula, A.; Godwod, K.; Debinski, A. Peptic ulcer disease and calcium intake as risk factors of osteoporosis in women. Osteoporos. Int. 2003, 14, 983–986. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Han, B.G. Cohort Profile: The Korean Genome and Epidemiology Study (KoGES) Consortium. Int. J. Epidemiol. 2017, 46, e20. [Google Scholar] [CrossRef] [PubMed]
- Malfertheiner, P.; Chan, F.K.; McColl, K.E. Peptic ulcer disease. Lancet 2009, 374, 1449–1461. [Google Scholar] [CrossRef]
- Malfertheiner, P.; Leodolter, A.; Peitz, U. Cure of Helicobacter pylori -associated ulcer disease through eradication. Best Pract. Res. Clin. Gastroenterol. 2000, 14, 119–132. [Google Scholar] [CrossRef]
- Rauws, E.; Tytgat, G. Cure of duodenal ulcer associated with eradication of Helicobacter pylori. Lancet 1990, 335, 1233–1235. [Google Scholar] [CrossRef]
- Figura, N.; Gennari, L.; Merlotti, D.; Lenzi, C.; Campagna, S.; Franci, B.; Lucani, B.; Trabalzini, L.; Bianciardi, L.; Gonnelli, C.; et al. Prevalence of Helicobacter pylori Infection in Male Patients with Osteoporosis and Controls. Dig. Dis. Sci. 2005, 50, 847–852. [Google Scholar] [CrossRef]
- Machowska, A.; Brzozowski, T.; Sliwowski, Z.; Pawlik, M.; Konturek, P.C.; Pajdo, R.; Szlachcic, A.; Drozdowicz, D.; Schwarz, M.; Stachura, J.; et al. Gastric secretion, proinflammatory cytokines and epidermal growth factor (EGF) in the delayed healing of lingual and gastric ulcerations by testosterone. Inflammopharmacology 2008, 16, 40–47. [Google Scholar] [CrossRef]
- Ginaldi, L.; Di Benedetto, M.C.; De Martinis, M. Osteoporosis, inflammation and ageing. Immun. Ageing 2005, 2, 14. [Google Scholar] [CrossRef]
- Christiansen, J.; Kirkegaard, P.; Olsen, P.S.; Petersen, B. Interaction of calcium and gastrin on gastric acid secretion in duodenal ulcer patients. Gut 1984, 25, 174–177. [Google Scholar] [CrossRef] [PubMed]
- Ahn, Y.; Kwon, E.; Shim, J.E.; Park, M.K.; Joo, Y.; Kimm, K.; Park, C.; Kim, D.H. Validation and reproducibility of food frequency questionnaire for Korean genome epidemiologic study. Eur. J. Clin. Nutr. 2007, 61, 1435–1441. [Google Scholar] [CrossRef] [PubMed]
- Chow, D.K.; Sung, J.J. Non-NSAID non-H. pylori ulcer disease. Best Pract. Res. Clin. Gastroenterol. 2009, 23, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Nassar, Y.; Richter, S. Proton-pump Inhibitor Use and Fracture Risk: An Updated Systematic Review and Meta-analysis. J. Bone Metab. 2018, 25, 141–151. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.; Siffert, R.; Ryaby, J.; Kaufman, J.; Alves, J.; Lin, D. Ultrasonic assessment of human and bovine trabecular bone: A comparison study. IEEE Trans. Biomed. Eng. 1996, 43, 249–258. [Google Scholar]


| Variables | Men | p-Value | Women | p-Value | ||
|---|---|---|---|---|---|---|
| Control | Peptic Ulcer | Control | Peptic Ulcer | |||
| Participants, n | 1464 | 189 | 1639 | 187 | ||
| Calcium intake, mg/d | ||||||
| Quartile 1 | 236.1 ± 2.9 | 213.9 ± 8.1 | 0.007 | 213.4 ± 2.5 | 205.6 ± 6.9 | 0.269 |
| Quartile 2 | 375.1 ± 2.0 | 373.2 ± 5.5 | 0.742 | 357.6 ± 2.0 | 376.1 ± 5.4 | 0.002 |
| Quartile 3 | 519.6 ± 2.4 | 508.9 ± 6.8 | 0.16 | 511.2 ± 2.3 | 517.4 ± 7.9 | 0.428 |
| Quartile 4 | 825.1 ± 12.6 | 866.1 ± 40.6 | 0.289 | 809.6 ± 11.9 | 827.1 ± 41.5 | 0.658 |
| Age, y | 52.1 ± 0.2 | 52.5 ± 0.6 | 0.556 | 51.2 ± 0.2 | 51.7 ± 0.6 | 0.475 |
| BMI, kg/m2 | 24.6 ± 0.1 | 23.4 ± 0.2 | <0.001 | 25.1 ± 0.1 | 24.1 ± 0.2 | <0.001 |
| Drinking Status, n (%) | 0.007 | 0.006 | ||||
| Never | 295 (20.2) | 30 (15.9) | 1176 (71.8) | 130 (69.5) | ||
| Former | 184 (12.6) | 39 (20.6) | 49 (3.0) | 14 (7.5) | ||
| Current | 985 (67.3) | 120 (63.5) | 414 (25.3) | 43 (23.0) | ||
| Smoking status, n (%) | 0.029 | 0.148 | ||||
| Never | 300 (20.5) | 25 (13.2) | 1570 (95.8) | 174 (93.1) | ||
| Former | 525 (35.9) | 66 (34.9) | 14 (0.9) | 3 (1.6) | ||
| Current | 639 (43.7) | 98 (51.9) | 55 (3.4) | 10 (5.4) | ||
| Physical activity, MET-h/week | 20.4 ± 0.4 | 25.7 ± 1.2 | <0.001 | 19.9 ± 0.3 | 24.8 ± 1.2 | <0.001 |
| Comorbidity, n (%) | ||||||
| Hypertension | 370 (25.3) | 36 (19.1) | 0.061 | 392 (23.9) | 26 (13.9) | 0.002 |
| Diabetes mellitus | 221 (15.1) | 12 (6.4) | 0.001 | 170 (10.4) | 6 (3.2) | 0.002 |
| Chronic kidney disease | 41 (2.8) | 3 (1.6) | 0.471 | 62 (3.8) | 10 (5.4) | 0.298 |
| Chronic pulmonary disease | 15 (1.0) | 3 (1.6) | 0.451 | 12 (0.7) | - | 0.625 |
| Cerebrovascular disease | 28 (1.9) | 5 (2.7) | 0.498 | 20 (1.2) | 1 (0.5) | 0.716 |
| Coronary artery disease | 27 (1.8) | 2 (1.1) | 0.766 | 16 (1.0) | 3 (1.6) | 0.434 |
| Hepatitis | 85 (5.8) | 15 (7.9) | 0.248 | 54 (3.3) | 10 (5.4) | 0.148 |
| Hormone replacement therapy | - | - | - | 103 (6.3) | 7 (3.7) | 0.166 |
| Menopause | - | - | - | 941 (57.4) | 114 (61.0) | 0.352 |
| Gender | Group | Osteoporosis | PY 1 | Rate 2 | IRR 3 (95% CI 4) | Adjusted HR 5,* (95% CI) |
|---|---|---|---|---|---|---|
| Men | Control (n = 1464) | 70 | 6224.0 | 11.2 | 1.82 (1.06–3.00) | 1.72 (1.02–2.92) |
| Peptic ulcer (n = 189) | 21 | 1024.6 | 20.5 | |||
| Women | Control (n = 1639) | 271 | 6402.7 | 42.3 | 1.52 (1.19–2.16) | 1.62 (1.20–2.18) |
| Peptic ulcer (n = 187) | 56 | 817.4 | 68.5 |
| Variables | Men | Women | ||
|---|---|---|---|---|
| HR * | 95% CI | HR 1,* | 95% CI 2 | |
| Calcium intake, mg/d | ||||
| Quartile 1 | 1.00 | |||
| Quartile 2 | 0.74 | 0.42–1.29 | 1.02 | 0.75–1.38 |
| Quartile 3 | 0.55 | 0.29–1.03 | 1.06 | 0.79–1.43 |
| Quartile 4 | 0.78 | 0.44–1.38 | 0.87 | 0.62–1.20 |
| Age, year | ||||
| <50 | 1.00 | |||
| ≥50 | 1.82 | 1.07–3.09 | 4.43 | 1.85–10.60 |
| BMI, kg/m2 | ||||
| 18.5–24.9 | 1.00 | |||
| 25.0–29.9 | 1.48 | 0.95–2.31 | 1.37 | 1.08–1.74 |
| 30–34.9 | 3.21 | 1.13–9.12 | 1.47 | 1.00–2.17 |
| >35 | - | 2.70 | 0.99–7.41 | |
| <18.5 | 0.94 | 0.22–3.95 | 0.97 | 0.35–2.67 |
| Drinking Status | ||||
| Never | 1.00 | |||
| Former | 0.75 | 0.39–1.44 | 0.88 | 0.48–1.62 |
| Current | 0.69 | 0.41–1.17 | 0.90 | 0.68–1.19 |
| Smoking status | ||||
| Never | 1.000 | |||
| Former | 0.95 | 0.52–1.72 | 2.32 | 0.93–5.78 |
| Current | 1.09 | 0.61–1.95 | 0.90 | 0.49–1.67 |
| Physical activity, MET-h/week | ||||
| Low | 1.00 | |||
| Mid | 0.77 | 0.39–1.49 | 1.02 | 0.75–1.38 |
| High | 1.16 | 0.68–1.95 | 1.31 | 1.00–1.71 |
| Comorbidity | ||||
| Hypertension | 1.10 | 0.69–1.75 | 1.01 | 0.79–1.29 |
| Diabetes mellitus | 1.15 | 0.67–1.98 | 1.06 | 0.77–1.45 |
| Chronic kidney disease | 1.58 | 0.62–4.00 | 0.67 | 0.36–1.26 |
| Chronic pulmonary disease | 0.52 | 0.07–3.85 | 3.10 | 1.41–6.83 |
| Cerebrovascular disease | - | 1.37 | 0.62–2.99 | |
| Coronary artery disease | 1.66 | 0.58–4.77 | 2.83 | 1.36–5.90 |
| Hepatitis | 2.06 | 1.03–4.13 | 0.57 | 0.27–1.16 |
| Menopause | 2.14 | 1.40–3.29 | ||
| Hormone replacement therapy | 0.72 | 0.43–1.19 | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoon, P.H.; An, S.J.; Jeong, S.-H.; Yang, Y.-J.; Hong, Y.-p. Association between Peptic Ulcer Disease and Osteoporosis: The Population-Based Longitudinal Cohort Study in Korea. Int. J. Environ. Res. Public Health 2019, 16, 2777. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16152777
Yoon PH, An SJ, Jeong S-H, Yang Y-J, Hong Y-p. Association between Peptic Ulcer Disease and Osteoporosis: The Population-Based Longitudinal Cohort Study in Korea. International Journal of Environmental Research and Public Health. 2019; 16(15):2777. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16152777
Chicago/Turabian StyleYoon, Phill Hoon, Sang Joon An, Seok-Hoo Jeong, Yun-Jung Yang, and Yeon-pyo Hong. 2019. "Association between Peptic Ulcer Disease and Osteoporosis: The Population-Based Longitudinal Cohort Study in Korea" International Journal of Environmental Research and Public Health 16, no. 15: 2777. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16152777