Development and Validation of an Interdisciplinary Worker’s Health Approach Instrument (IWHAI)

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
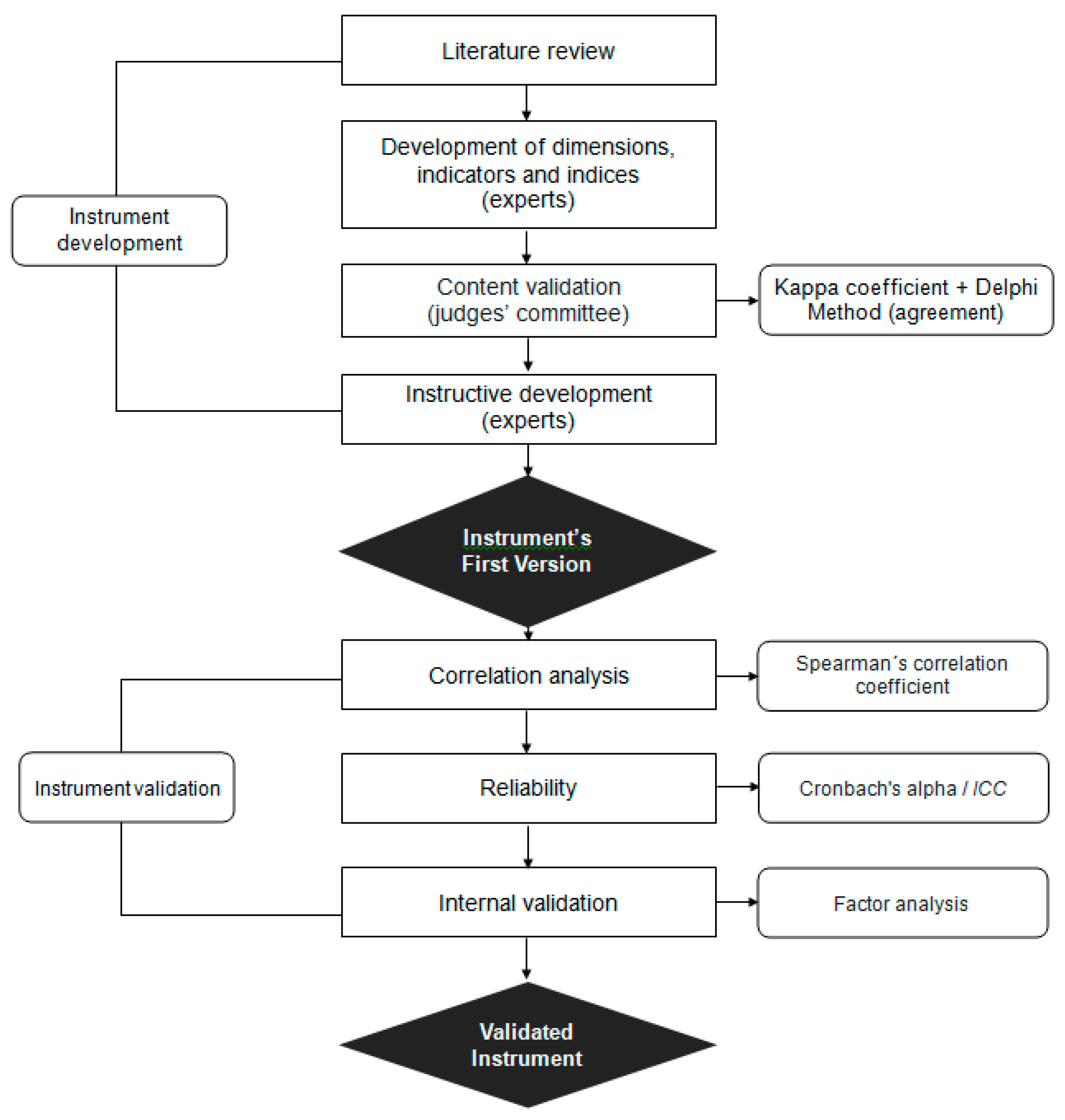
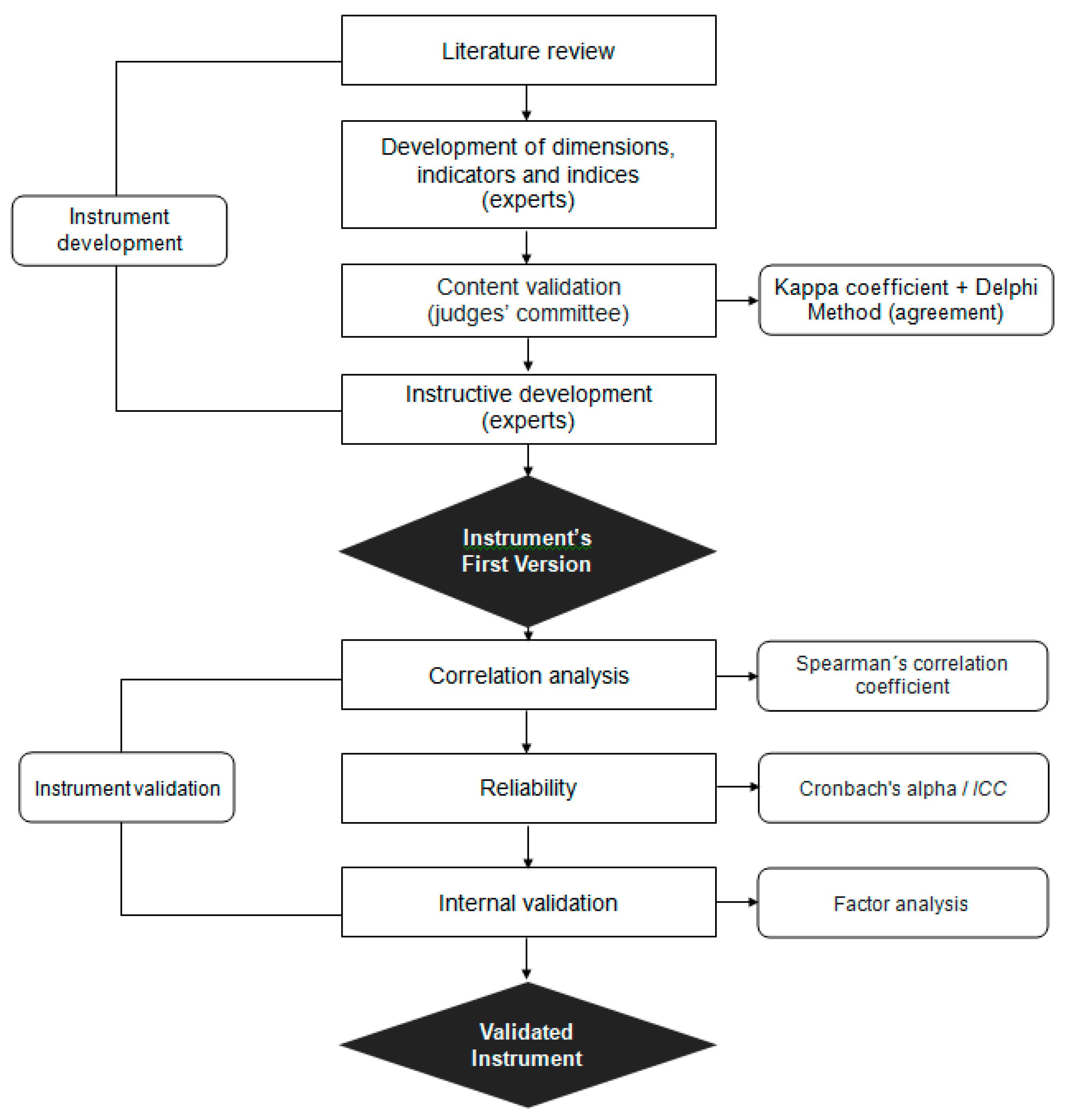
2.1. Study Design
2.2. IWHAI Development
2.3. IWHAI Validation
2.4. Data Analysis
2.5. Ethical Approval
3. Results
4. Discussion
5. Conclusions
5.1. Strengths and Limitations
5.2. Future Applications
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- United Nations Transforming Our World: The 2030 Agenda for Sustainable Development. Resolution adopted by the General Assembly on 25 September 2015, A/RES/70/1. 2015. Available online: http://www.un.org/en/development/desa/population/migration/generalassembly/docs/globalcompact/A_ 549 RES_70_1_E.pdf (accessed on 27 June 2019).
- Leadership Council of the Sustainable Development Solutions Network Indicators and a Monitoring Framework Sustainable Development Goals Launching a Data Revolution for the SDGs. 2015. Available online: http://0-www-jstor-org.brum.beds.ac.uk/stable/resrep15877 (accessed on 28 June 2019).
- United Nations General Assembly Global Indicator Framework for the Sustainable Development Goals and targets of the 2030 Agenda for the Sustainable Development; Official Document System of the United Nations: New York, NY, USA, 2018.
- Eurofound Health and Well-Being at Work—Q2 2014; European Observatory for Working Life: Brussels, Belgium, 2015.
- Eurofound and EU-OHSA Psychosocial Risks in Europe: Prevalence and Strategies for Prevention; Publications Office of the European Union: Brussels, Belgium, 2014.
- Eurofound Developments in Working life in Europe; EurWORK Annual Review 2014; Eurofound: Brussels, Belgium, 2015.
- Dinis, M.A.P.; Sousa, H.F.P.; Moura, A.D.; Viterbo, L.M.F.; Pinto, R.J. Health behaviors as a mediator of the association between interpersonal relationships and physical health in a workplace context. Int. J. Environ. Res. Public Health 2019, 16, 2392. [Google Scholar] [CrossRef] [PubMed]
- European Comission. Communication from the Commission: Europe 2020. A Strategy for Smart, Sustainable and Inclusive Growth. COM (2010) 2020 final. Brussels, Belgium, 2010. Available online: https://ec.europa.eu/eu2020/pdf/COMPLET%20EN%20BARROSO%20%20%20007%20-%20Europe%202020%20-%20EN%20version.pdf (accessed on 20 June 2019).
- European Comission. Communication from the Commission to the European Parliament, the Council, the European Economic and Social Committee and the Committee of the Regions. Taking Stock of the Europe 2020 Strategy for Smart, Sustainable and Inclusive Growth; Brussels, 19.3.20. European Environment Agency: Brussels, Belgium, 2014. Available online: https://ec.europa.eu/info/publications/taking-stock-europe-2020-strategy-smart-sustainable-and-inclusive-growth_en (accessed on 23 June 2019).
- Lacaz, F.A.D.C. O campo Saúde do. Trabalhador: Resgatando conhecimentos e práticas sobre as relações trabalho-saúde [The workers’ health field: Reclaiming knowledge and practices in the interface between work and health]. Cad. Saúde Pública 2007, 23, 757–766. [Google Scholar] [CrossRef] [PubMed]
- Minayo, C.; Machado, J.M.H.; Pena, P.G.L. Saúde do Trabalhador na Sociedade Brasileira Contemporânea [Worker’s Health at the Contemporary Brazilian Society]; Fiocruz: Rio de Janeiro, Brazil, 2011. [Google Scholar]
- Viterbo, L.M.F.; Costa, A.S.; Dinis, M.A.P. Interdisciplinarity: An articulating movement in the field of worker’s health. In La comunicación ante el ciudadano; Viniegra, L.M., Chávez, S.M., Rodrigo, E.M., Eds.; Editorial GEDISA: Madrid, Spain, 2018; ISBN 9788417690045. [Google Scholar]
- Mendes, R.; Dias, E.C. Da medicina do trabalho à saúde do trabalhador [From work medicine to worker’s health]. Rev. Saúde Pública 1991, 25, 341–349. [Google Scholar] [CrossRef] [PubMed]
- Minayo-Gomez, C.; Maria, S.; Thedim-Costa, F. A construção do campo da saúde do trabalhador: Percurso e dilemas. Cad. Saúde Pública 1997, 13, 21–32. [Google Scholar] [CrossRef] [PubMed]
- Huet Machado, J.M.; de Souza Porto, M.F. Promoção da saúde e intersetorialidade: A experiência da vigilância em saúde do trabalhador na construção de redes [Health promotion and intersectoriality: Experience of occupational health surveillance in the construction of networks]. Epidemiol. e Serviços Saúde 2003, 12, 121–130. [Google Scholar]
- Viterbo, L.M.F.; Dinis, M.A.P.; Vidal, D.G.; Costa, A.S. Implementation of an interdisciplinary approach to promote workers global health status in the oil industry, Brazil (2006–2015). Int. J. Environ. Res. Public Health 2019, 16, 2148. [Google Scholar] [CrossRef]
- Viterbo, L.M.F.; Vidal, D.G.; Costa, A.S.; Dinis, M.A.P. Evaluation of the implementation of the tobacco control program in workers’ health: evidence from an oil industry in Bahia, Brazil. Proc. Int. Congr. Health Well-Being Interv. 2019, in press. [Google Scholar]
- Almeida, G.E.S. De Significados e limites das estratégias de integração disciplinar: Uma reflexão sobre as contribuições da saúde do trabalhador [Meanings and limits concerned to the strategies of disciplinary integration: A reflection about the contributions from the work]. Cien. Saude Colet. 2000, 7, 335–347. [Google Scholar]
- Gelbcke, F.L.; Matos, E.; Sallum, N.C. Desafios para a integração multiprofissional e interdisciplinar [Challenges for multiprofessional and interdisciplinary integration]. Tempus Actas de Saúde Coletiva 2012, 6, 31–39. [Google Scholar]
- Brasil Ministério da Saúde. 3ª Conferência Nacional de Saúde do Trabalhador “Trabalhar, Sim! Adoecer, Não!” [Work, Yes! Get sick, No!]; Brasil Ministério da Saúde: Brasília, Brazil, 2005.
- Viterbo, L.M.F.; Vidal, D.G.; Dinis, M.A.P.; Costa, A.S.; Caridade, S. Mental Health in Oil Workers in Brazil: The relationship with drug abuse. In Proceedings of the 1st International Congress Quality of Life, Citizenship and Mental Health; Projeto Mais Saúde Mental: Viseu, Portugal, 2019. [Google Scholar]
- Lins, G.A.I.; Armendaris, M.K.; Pinho, D.L.M.; Kamada, I.; Jesus, C.A.C.D.; Reis, P.E.D. Teoria de Tornar-se Humano na enfermagem ecológica: Aplicando o método de avaliação de Meleis TT [Theory of human becoming in nursing ecology: Applying Meleis’s evaluation method TT]. Texto Context. Enferm 2013, 22, 1179–1186. [Google Scholar] [CrossRef]
- Bini, C.; Bech, J.; PHEs, Environment and Human Health. Potentially Harmful Elements in the Environment and the Impact on Human Health; Springer: Basel, Switzerland, 2014. [Google Scholar]
- Dinis, M.A.P. Environment and human health. J. Environ. Pollut. Hum. Health 2016, 4, 52–59. [Google Scholar] [CrossRef]
- Barros, C.; Cunha, L.; Baylina, P.; Oliveira, A.; Rocha, Á. Development and validation of a health and work survey based on the rasch model among Portuguese workers. J. Med. Syst. 2017, 41, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Barros, C.; Cunha, L.; Lacomblez, M. Intrumentos de Investigação. INSAT—uma proposta metofológica para análise dos efeitos das condições de trabalho sobre a saúde [Research Instruments. INSAT—a 622 methodological proposal to analyse the effects of working conditions on health]. Laboreal 2007, 3, 54–62. [Google Scholar]
- Niedhammer, I.; Chastang, J.F.; David, S. Importance of psychosocial work factors on general health outcomes in the national French SUMER survey. Occup. Med. 2008, 58, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Coutrot, T.; Wolff, L. L’impact des conditions de travail sur la santé: Une expérience méthodologique [The impact of working conditions on health: Methodological experience]; Center for Employment Studies: Noisy-le-Grand, France, 2005. [Google Scholar]
- Benavides, F.G.; Merino-Salazar, P.; Cornelio, C.; Assunção, A.A.; Agudelo-Suárez, A.A.; Amable, M.; Artazcoz, L.; Astete, J.; Barraza, D.; Berhó, F.; et al. Cuestionario básico y criterios metodológicos para las Encuestas sobre Condiciones de Trabajo, Empleo y Salud en América Latina y el Caribe [Basic questionnaire and methodological criteria for Surveys on 630 Working Conditions, Employment, and Health in Latin America and the Caribbean]. Cad. Saúde Pública 2016, 32, 1–13. [Google Scholar]
- Huang, Y.-H.; Zohar, D.; Robertson, M.M.; Garabet, A.; Murphy, L.A.; Lee, J. Development and validation of safety climate scales for mobile remote workers using utility/electrical workers as exemplar. Accid. Anal. Prev. 2013, 59, 76–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Narocki, C. Encuestas de condiciones de trabajo y salud en España: Comparación de los contenidos del cuestionario del trabajador. Arch. Prev. Riesgos Labor. 2009, 12, 60–68. [Google Scholar]
- Benavides, F.G.; Wesseling, C.; Delclos, G.L.; Felknor, S.; Pinilla, J.; Rodrigo, F. Working conditions and health in Central America: A survey of 12 024 workers in six countries. Occup. Environ. Med. 2014, 71, 459–465. [Google Scholar] [CrossRef]
- Irastorza, X.; Milczarek, M.; Cockburn, W. European Agency for Safety and Health at Work (EU-OSHA) Second European Survey of Enterprises on New and Emerging Risks (ESENER-2)—Overview Report: Managing Safety and Health at Work; European Agency for Safety and Health at Work: Bilbao, Spain, 2016; ISBN1 978-92-9240-897-8. ISBN2 978-92-9240-896-1.
- Eurofound Sixth European Working Conditions Survey—Overview report (2017 update)|European Foundation for the Improvement of Living and Working Conditions; Southern Cross Health Society: Auckland, New Zealand, 2017; ISBN 9789289715973.
- Business, N.Z. Wellness in the Workplace 2017. 2017. Available online: http://www.businessnz.org.nz/__data/assets/pdf_file/0009/128547/Wellness-in-the-Workplace-Survey-2017.pdf (accessed on 29 June 2019).
- Kelly, M.P.; Morgan, A.; Bonnefoy, J.; Butt, J.; Bergman, V.; Mackenbach, W.J.; Exworthy, M.; Popay, J.; Tugwell, P.; Robinson, V.; et al. The Social Determinants of Health: Developing an Evidence Base for Political Action. Final Report to World Health Organization Commission on the Social Determinants of Health. 2007. Available online: https://www.who.int/social_determinants/resources/mekn_report_10oct07.pdf (accessed on 25 June 2019).
- Commission on Social Determinants of Health Closing the Gap in a Generation: Health Equity through Action on the Social Determinants of Health. 2008. Available online: https://apps.who.int/iris/bitstream/handle/10665/43943/9789241563703_eng.pdf;jsessionid=A41734C2C697 96C98EA28D15E63331DF?sequence=1 (accessed on 26 June 2019).
- Graham, H.; White, P.C.L. Social determinants and lifestyles: Integrating environmental and public health perspectives. Public Health 2016, 141, 270–278. [Google Scholar] [CrossRef]
- Forouzanfar, M.H.; Afshin, A.; Alexander, L.T.; Anderson, H.R.; Bhutta, Z.A.; Biryukov, S.; Brauer, M.; Burnett, R.; Cercy, K.; Charlson, F.J.; et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1659–1724. [Google Scholar] [CrossRef]
- Malta, D.C.; Felisbino-Mendes, M.S.; Machado, Í.E.; Passos, V.M.D.A.; Abreu, D.M.X.D.; Ishitani, L.H.; Velásquez-Meléndez, G.; Carneiro, M.; Mooney, M.; Naghavi, M. Fatores de risco relacionados à carga global de doença do Brasil e Unidades Federadas, 2015 [Risk factors related to the global burden of disease in Brazil and its Federated Units, 2015]. Rev. Bras. Epidemiol. 2017, 20, 217–232. [Google Scholar]
- World Health Organization. Global Health Risks; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Viterbo, L.M.F.; Dinis, M.A.P.; Sá, K.N.; Marques, C.A.S.C.; Navarro, M.V.T.; Leite, H.J.D. Development of a quantitative instrument for sanitary inspection in food and nutrition services, Brazil. Cien. Saúde Colet. Available online: http://www.cienciaesaudecoletiva.com.br/artigos/desenvolvimento-de-um-instrumento-quantitativo-para-inspecao-sanitaria-em-servicos-de-alimentacao-e-nutricao-brasil/16913 (accessed on 2 July 2019).
- Alexandre, N.M.C.; Coluci, M.Z.O. Content validity in the development and adaptation processes of measurement instruments. Cien. Saúde Colet. 2009, 16, 3061–3068. [Google Scholar] [CrossRef]
- Kaizer, U.A.D.O.; Araujo, V.S.D.; Dantas, S.R.P.E. Validation of content of guidelines for people with peripheral neuropathy due to diabetes. ESTIMA Braz. J. Enteros. Ther. 2018, 16, 1–8. [Google Scholar]
- Landis, J.R.; Koch, G.G. The Measurement of Observer Agreement for Categorical Data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed]
- Okoli, C.; Pawlowski, S.D. The Delphi method as a research tool: An example, design considerations and applications. Inf. Manag. 2004, 42, 15–29. [Google Scholar] [CrossRef]
- Santana, P.; Freitas, A.; Costa, C.; Vaz, A. Evaluating population health: The selection of main dimensions and indicators through a participatory approach. Eur. J. Geogr. 2015, 6, 51–63. [Google Scholar]
- Freitas, Â.; Santana, P.; Oliveira, M.D.; Almendra, R.; Bana E Costa, J.C.; Bana E Costa, C.A. Indicators for evaluating European population health: A Delphi selection process. BMC Public Health 2018, 18, 1–20. [Google Scholar] [CrossRef]
- Oliveira, G.M.; Vidal, D.G.; Viterbo, L.M.F.; Maia, R.L. Measuring the Implementation of Sustainable Development Goals at a Local Level: The WeGIx Index. In Universities and Sustainable Communities: Meeting the Goals of the Agenda 2030 World Sustainability Series; Leal Filho, W., Frankenberger, F., Tortato, U., Eds.; Springer International Publishing: Cham, Switzerland, 2020; in press. [Google Scholar]
- IBM Corporation Released IBM SPSS Statistics for Windows, Versão 25; IBM Corp.: Armonk, NY, USA, 2018.
- Ministério da Saúde. Resolução 466 de 12 de dezembro de 2012. Aprova as diretrizes e normas regulamentadoras de pesquisa envolvendo seres humanos. Diário Oficial da União, 12 dez. 2012 [Approves Regulatory Norms of Research Involving Human Beings; National Health Council Resolution No 466 of December 12, 2012]; Diário Oficial da União: Brasilia, Brazil, 2012.
- Child, D. The Essentials of Factor Analysis, 2nd ed.; Cassel Educational: New York, NY, USA, 1990. [Google Scholar]
- Norusis, M.J. SPSS for Windows; Profession Statistics, Release; SPSS, Ed.; SPSS Inc.: Chicago, IL, USA, 1992. [Google Scholar]
- Kwame, O.-K.J. Critical success factors for Ghanaian contractors. Benchmarking An Int. J. 2016, 23, 843–865. [Google Scholar] [CrossRef]
- Hair, J.F.J.; Babin, B.; Money, A.H.; Samouel, P. Essential of Business Research Methods; John Wiley & Sons: Hoboken, NJ, USA, 2003. [Google Scholar]
- Ruiz Bolívar, C. Confiabilidad [Reliability]. 2002. Available online: http://200.11.208.195/blogRedDocente/alexisduran/wp-content/uploads/2015/11/CONFIABILIDAD.pdf (accessed on 1 July 2019).
- Mahmood, S.S.; Levy, D.; Vasan, R.S.; Wang, T.J. The Framingham Heart Study and the epidemiology of cardiovascular disease: A historical perspective. Lancet 2014, 383, 999–1008. [Google Scholar] [CrossRef]
- Hippisley-Cox, J.; Coupland, C.; Brindle, P. Development and validation of QRISK3 risk prediction algorithms to estimate future risk of cardiovascular disease: Prospective cohort study. BMJ 2017, 357, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Leite, H.J.D.; Navarro, M.V.T. Risco potencial: Um conceito de risco operativo para vigilância sanitária [Potential risk: An operational risk concept for health surveillance]. In Vigilância Sanitária: Temas Para Debate; Costa, E.A., Ed.; EDUFBA: Salvador, Brazil, 2009; ISBN 9788523206529. [Google Scholar]
- Corrêa, C.R. Situações incómodas no trabalho: Confiabilidade de uma escala de medida utilizando o coeficiente alfa ordinal [Uncomfortable situations at work: Reliability of a measurement scale using the ordinal alpha coefficient]. Universidade Federal de Juiz de Fora, 2012. Available online: http://bdtd.ibict.br/vufind/Record/UFJF_6e9d84ff71db1b4b7446a4079b385178/Details#tabnav (accessed on 4 July 2019).
- Bomfim, R.A.; Crosato, E.; Nigro Mazzilli, L.E. Relations between oral health and work ability among administrative workers. Brazilian J. Oral Sci. 2015, 14, 41–45. [Google Scholar] [CrossRef] [Green Version]
- Oral Health Foundation Oral Health and the Workplace. Available online: https://www.dentalhealth.org/in-the-workplace (accessed on 11 July 2019).
- Quintiliani, L.; Poulsen, S.; Sorensen, G. Healthy eating strategies in the workplace. Int. J. Work. Health Manag. 2010, 3, 182–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barreira, E.; Vidal, D.G.; Pontes, M.; Oliveira, G.; Maia, R.L. O Impacto dos Poluentes Atmosféricos no Cancro do Pulmão: Um estudo transversal [The Impact of Atmospheric Pollutants on Lung Cancer: A Cross-sectional Study]. In Proceedings of the 2018 Oncology Spring Meeting; DNA Prime: Évora, Portugal, 2018. [Google Scholar]
- Barreira, E.; Pontes, M.; Maia, R.L.; Oliveira, G.M.; Vidal, D.G. Cancro do Pulmão e Poluição: Um estudo transversal [Lung Cancer and Pollution: A Cross-sectional Study]. Onco. News 2018, 14–19. [Google Scholar]
- WHO Public Health Social and Environmental Determinants of Health Department Burden of disease from ambient air pollution for 2012; World Health Organization (WHO): Geneva, Switzerland, 2014; Available online: http://www.who.int/phe (accessed on 5 July 2019).
- Lonergan, S.; Vansickle, T. Relationship between water quality and human health: A case study of the Linggi River Basin in Malaysia. Soc. Sci. Med. 1991, 33, 937–946. [Google Scholar] [CrossRef]
- Windle-Taylor, E. The Relationship Between Water Quality and Human Health: Medical Aspects. R. Soc. Health J. 1978, 98, 121–129. [Google Scholar] [CrossRef]
- Nazri, C.D.; Muhammad Faiz, M.; Siti Nur Anis, H.; Nurlisa, M. Water quality characteristics of dengue vectors breeding containers. Int. J. Mosq. Res. 2016, 3, 25–29. [Google Scholar]

{kind=link}
| Sociodemographic Data | Population n (%) | Sample n (%) | p |
|---|---|---|---|
| Sex | |||
| Male | 1117 (87.6) | 884 (91.6) | > 0.05 |
| Female | 158 (12.4) | 81 (8.4) | |
| Age Group | |||
| ≤29 | 50 (3.9) | 44 (4.6) | |
| 30–39 | 350 (27.5) | 261 (27.0) | |
| 40–49 | 245 (19.2) | 209 (21.7) | |
| 50–59 | 556 (43.6) | 410 (42.5) | |
| ≥60 | 74 (5.8) | 41 (4.2) | |
| Total | 1275 | 965 |
| Dimensions | Indicators |
|---|---|
| Medicine | * Altered blood pressure * Altered glycemia * Arterial hypertension * Diabetes mellitus * Dyslipidemia * Musculoskeletal pathology * Psychiatric pathology * Stress level and symptoms * Tobacco use |
| Nursing | Air quality Drinking water quality * Ergonomic risks—physical aspects Ergonomic risks—organizational aspects * Exposure to environmental risks (physical, chemical and biological Family relationships Pests and vectors * Self-care level Social aspects—leisure Work accident * Work environment health conditions agents) Work-related absenteeism |
| Nutrition | * Alcohol use Altered triglycerides Bodyweight condition Energy balance intake Fibre intake Level of food knowledge * Saturated lipids intake * Simple carbohydrate intake * Sodium mineral intake |
| Dentistry | Bruxism * Caries Oral hygiene quality * Oral lesion on soft or hard tissues * Periodontal condition * Periodontal disease |
| Physical Education | Abdominal strength level Cardiorespiratory fitness * Contemplation stage for physical activity practice * Feeling of pain Flexibility level Manual gripping force Physical activity level |
| Dimension | Indicator | Indices | |
|---|---|---|---|
| Nutrition | Alcohol use | 0 | Frequent heavy drinker (drinks 1 time or more per week and consumes 5 or more doses per occasion, once a week or more) |
| 1 | Frequent drinker (drinks once a week or more and may or may not consume 5 or more doses at least once a week, but more than once a year) | ||
| 2 | Less frequent drinker (drinks 1 to 3 times a month and may or not drink 5 doses or more at least once a year) | ||
| 3 | Non-frequent drinker (drinks less than once a month, but at least once a year and does not drink 5 or more doses at one time) | ||
| 4 | Abstemious (drinks less than once a year or has never drunk in life) | ||
| Dimensions | Rated Items | Applicability | Clarity | Relevance | |||
|---|---|---|---|---|---|---|---|
| n1 (%) | k | n2 (%) | k | n3 (%) | k | ||
| Medicine | 171 | 72 | 0.80 | 90 | 0.76 | 90 | 0.76 |
| Nursing | 285 | 73 | 0.86 | 81 | 0.78 | 79 | 0.78 |
| Nutrition | 171 | 71 | 0.79 | 89 | 0.71 | 90 | 0.71 |
| Dentistry | 114 | 90 | 1.00 | 84 | 0.93 | 90 | 1.00 |
| Physical Education | 133 | 86 | 0.95 | 90 | 0.83 | 90 | 0.83 |
| Mean | 0.88 | 0.80 | 0.82 | ||||
| (%) | 78 | 87 | 88 | ||||
| Indicators | Pests and Vectors | Physical Activity Level | Contemplation Stage for Physical Activity Practice | Saturated Lipids Intake | Level of Food Knowledge | Body Weight Condition | Altered Triglycerides | Altered Blood Pressure | Abdominal Strength Level | Oral Hygiene Quality | Arterial Hypertension |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Air quality | 0.69 ** | ||||||||||
| Contemplation stage for physical activity practice | 0.78 ** | ||||||||||
| Self-care level | 0.40 ** | 0.34 ** | |||||||||
| Sodium mineral intake | 0.23 ** | ||||||||||
| Body weight condition | 0.30 ** | ||||||||||
| Altered triglycerides | 0.31 ** | ||||||||||
| Altered blood pressure | 0.31 ** | 0.33 ** | |||||||||
| Energy balance intake | 0.59 ** | 0.59 ** | 0.37 ** | 0.37 * | |||||||
| Flexibility level | 0.39 ** | ||||||||||
| Periodontal condition | 0.79 ** | ||||||||||
| Arterial hypertension | 0.33 ** | ||||||||||
| Diabetes mellitus | 0.35 ** |
| Component: % | Factor load | C * | (α) ** | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| I | II | III | IV | V | VI | VII | VIII | IX | X | XI | XII | XIII | XIV | |||
| Food Behaviour: 7.2 | ||||||||||||||||
| Energy balance intake | 0.82 | 0.76 | 0.57 | |||||||||||||
| Level of food knowledge | 0.58 | 0.58 | 0.59 | |||||||||||||
| Bodyweight condition | 0.73 | 0.67 | 0.59 | |||||||||||||
| Altered triglycerides | 0.47 | 0.52 | 0.58 | |||||||||||||
| Altered blood pressure | 0.53 | 0.47 | 0.59 | |||||||||||||
| Altered glycemia | 0.64 | 0.55 | 0.61 | |||||||||||||
| Environmental Factors: 6.0 | ||||||||||||||||
| Pests and vectors | 0.77 | 0.62 | 0.62 | |||||||||||||
| Air quality | 0.91 | 0.85 | 0.61 | |||||||||||||
| Drinking water quality | 0.55 | 0.57 | 0.62 | |||||||||||||
| Oral Health:5.4 | ||||||||||||||||
| Oral hygiene quality | 0.86 | 0.82 | 0.58 | |||||||||||||
| Periodontal condition | 0.90 | 0.85 | 0.59 | |||||||||||||
| Periodontal disease | 0.50 | 0.60 | 0.60 | |||||||||||||
| Bruxism | 0.80 | 0.61 | 0.58 | |||||||||||||
| Personal Factors: 5.0 | ||||||||||||||||
| Diabetes mellitus | 0.68 | 0.59 | 0.60 | |||||||||||||
| Arterial hypertension | 0.67 | 0.58 | 0.59 | |||||||||||||
| Physical Activity: 4.9 | ||||||||||||||||
| Physical activity level | 0.85 | 0.77 | 0.59 | |||||||||||||
| Contemplation stage for physical activity practice | 0.86 | 0.77 | 0.60 | |||||||||||||
| Physical aptitude: 4.8 | ||||||||||||||||
| Cardiorespiratory fitness | 0.48 | 0.57 | 0.60 | |||||||||||||
| Abdominal strength level | 0.73 | 0.61 | 0.61 | |||||||||||||
| Flexibility level | 0.67 | 0.59 | 0.61 | |||||||||||||
| Manual gripping force | 0.59 | 0.62 | 0.61 | |||||||||||||
| Musculoskeletal Factors: 4.6 | ||||||||||||||||
| Feeling of pain | 0.82 | 0.71 | 0.61 | |||||||||||||
| Musculoskeletal pathology | 0.82 | 0.71 | 0.61 | |||||||||||||
| Behavioural Factors: 4.5 | ||||||||||||||||
| Simple carbohydrate intake | 0.75 | 0.63 | 0.60 | |||||||||||||
| Fibre intake | 0.67 | 0.61 | 0.61 | |||||||||||||
| Self-care level | 0.48 | 0.62 | 0.59 | |||||||||||||
| Mental Disorder and Working Conditions: 4.0 | ||||||||||||||||
| Psychiatric pathology | 0.46 | 0.53 | 0.61 | |||||||||||||
| Work environment health conditions | 0.55 | 0.46 | 0.62 | |||||||||||||
| Stress level and symptoms | 0.66 | 0.64 | 0.62 | |||||||||||||
| Consumption: 3.9 | ||||||||||||||||
| Alcohol use | 0.67 | 0.59 | 0.60 | |||||||||||||
| Dyslipidemia | 0.40 | 0.59 | 0.61 | |||||||||||||
| Intake Levels: 3.8 | ||||||||||||||||
| Saturated lipids intake | 0.57 | 0.62 | 0.61 | |||||||||||||
| Sodium mineral intake | 0.59 | 0.57 | 0.61 | |||||||||||||
| Organizational and Social Factors: 3.6 | ||||||||||||||||
| Ergonomic risks—organizational aspects | 0.47 | 0.69 | 0.61 | |||||||||||||
| Social aspects—leisure | 0.68 | 0.73 | 0.61 | |||||||||||||
| Work accident | 0.53 | 0.60 | 0.61 | |||||||||||||
| Family relationships | 0.80 | 0.68 | 0.61 | |||||||||||||
| Work-related absenteeism | 0.82 | 0.72 | 0.61 | |||||||||||||
| Occupational Risks: 2.5 | ||||||||||||||||
| Exposure to environmental risks (physical, chemical and biological agents) | 0.61 | 0.48 | 0.61 | |||||||||||||
| Ergonomic risks—physical aspects | 0.46 | 0.59 | 0.62 | |||||||||||||
| Drugs and Injuries: 2.4 | ||||||||||||||||
| Tobacco use | 0.77 | 0.66 | 0.61 | |||||||||||||
| Oral lesion on soft or hard tissues | 0.32 | 0.58 | 0.61 | |||||||||||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Viterbo, L.M.F.; Dinis, M.A.P.; Costa, A.S.; Vidal, D.G. Development and Validation of an Interdisciplinary Worker’s Health Approach Instrument (IWHAI). Int. J. Environ. Res. Public Health 2019, 16, 2803. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16152803
Viterbo LMF, Dinis MAP, Costa AS, Vidal DG. Development and Validation of an Interdisciplinary Worker’s Health Approach Instrument (IWHAI). International Journal of Environmental Research and Public Health. 2019; 16(15):2803. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16152803
Chicago/Turabian StyleViterbo, Lilian Monteiro Ferrari, Maria Alzira Pimenta Dinis, André Santana Costa, and Diogo Guedes Vidal. 2019. "Development and Validation of an Interdisciplinary Worker’s Health Approach Instrument (IWHAI)" International Journal of Environmental Research and Public Health 16, no. 15: 2803. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16152803