A Qualitative Study of Parents’ Conceptualizations on Fever in Children Aged 0 to 12 Years


Abstract
:1. Introduction
2. Methods
2.1. Sample and Data Collection
2.2. Data Analysis
2.3. Validity
2.4. Ethical Considerations
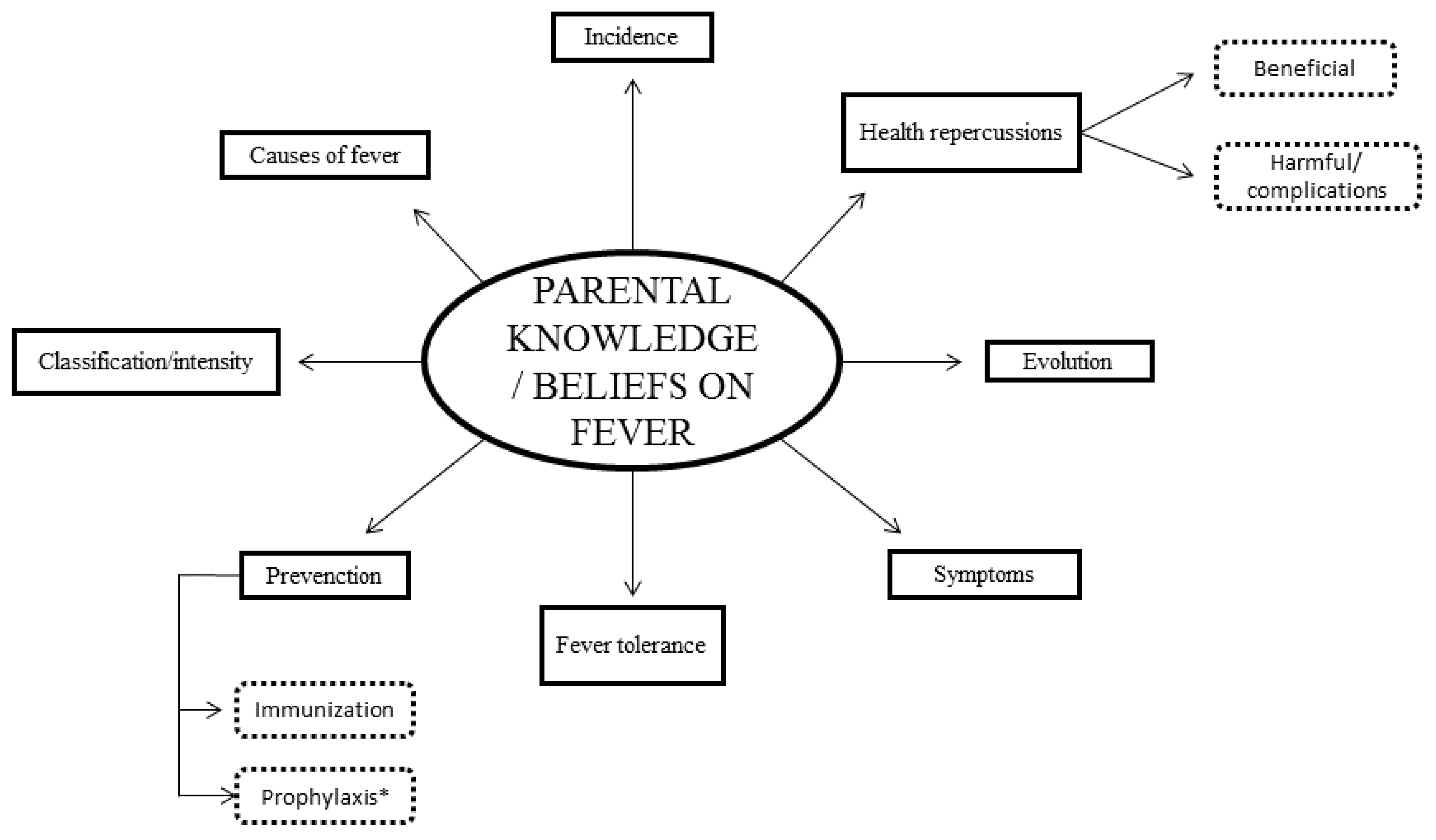
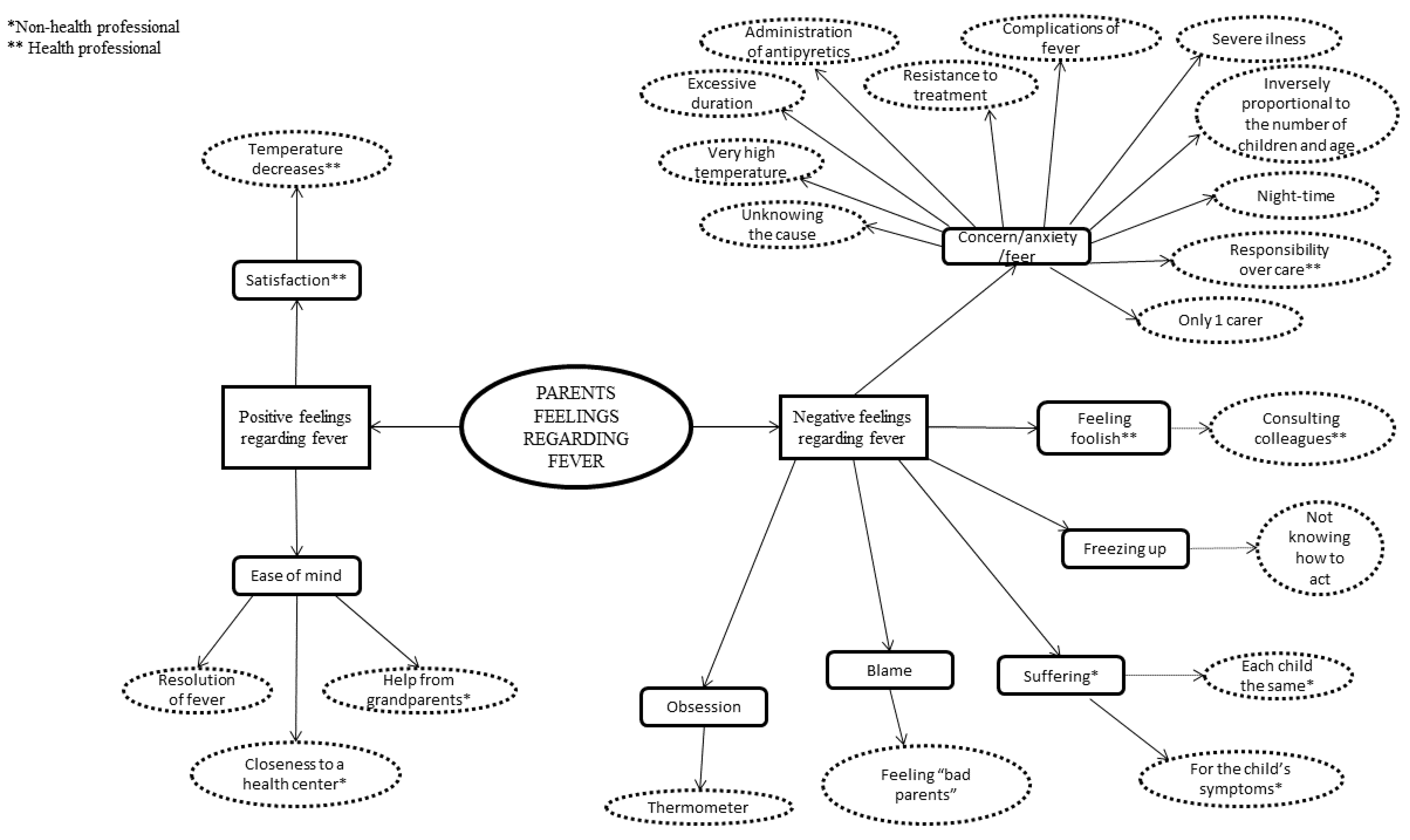
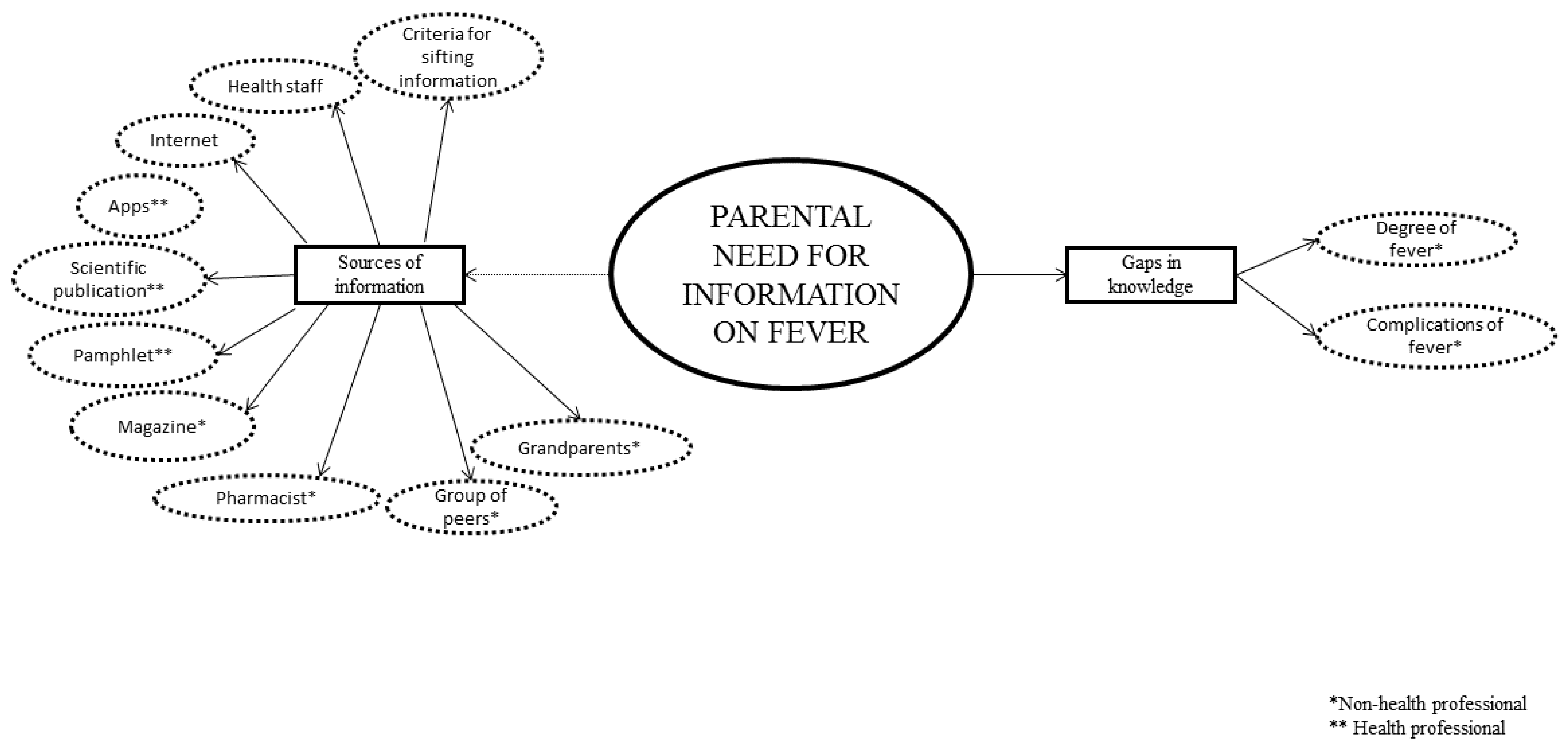
3. Results
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ertmann, R.K.; Reventlow, S.; Söderström, M. Is my child sick? Parent’s management of signs of illness and experiences of the medical encounter: Parents of recurrently sick children urge for more cooperation. Scand. J. Prim. Health 2011, 29, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Stagnara, J.; Vermont, J.; Dürr, F.; Ferradji, K.; Mege, L.; Duquesne, A.; Ferley, J.P.; Kassaï, B. Parents’ attitudes towards childhood fever. A cross-sectional survey in the Lyon metropolitan area (202 cases). Presse Med. 2005, 34, 1129–1136. [Google Scholar] [CrossRef]
- García, J.M.; Callejas, J.E.; Castillo, L.; Hernández, D.; Garrido, F.J.; Jiménez, T.; Ortega, E.; Santos, J.L.; Expósito, M.; Pérez, S.; et al. Knowledge and management of fever by parents. Rev. Pediatr. Aten. Prim. 2011, 13, 367–379. [Google Scholar]
- Schmitt, B.D. Fever in childhood. Pediatrics 1984, 74, 929–936. [Google Scholar] [PubMed]
- Maguire, S.; Ranmal, R.; Komulainen, S.; Pearse, S.; Maconochie, I.; Lakhanpaul, M.; Davies, F.; Kai, J.; Stephenson, T. Which urgent care services do febrile children use and why? Arch. Dis. Child. 2011, 96, 810–816. [Google Scholar] [CrossRef] [PubMed]
- Monsma, J. Empowering parents for evidence-based fever management: An integrative review. J. Am. Assoc. Nurse Pract. 2015, 27, 222–229. [Google Scholar] [CrossRef]
- Rodríguez-Martín, B.; Castillo, C.A. Carbohydrates and sports practice: A Twitter virtual ethnography. Nutr. Hosp. 2017, 34, 144–153. [Google Scholar] [CrossRef]
- Karwowska, A.; Nijssen-Jordan, C.; Johnson, D.; Davies, H. Parental and health care pro-vider understanding of childhood fever: A Canadian perspective. CJEM 2002, 4, 394–400. [Google Scholar] [CrossRef]
- Impicciatore, P.; Pandolfini, C.; Casella, N.; Bonati, M. Reliability of health information for the public on the World Wide Web: Systematic survey of advice on managing fever in children at home. BMJ 1997, 314, 1875. [Google Scholar] [CrossRef]
- Hay, A.; Heron, J.; Ness, A. The prevalence of symptoms and consultations in pre-school children in the Avon Longitudinal Study of Parents and Children (ALSPAC): A prospective cohort study. Fam. Pract. 2005, 22, 367–374. [Google Scholar] [CrossRef]
- Basu, A.M.; Stephenson, R. Low levels of maternal education and the proximate determinants of childhood mortality: A little learning is not a dangerous thing. Soc. Sci. Med. 2005, 60, 2011–2023. [Google Scholar] [CrossRef] [PubMed]
- Peetoom, K.K.; Smits, J.J.; Ploum, L.J.; Verbakel, J.Y.; Dinant, G.J.; Cals, J.W. Does well-child care education improve consultations and medication management for childhood fever and common infections? A systematic review. Arch. Dis. Child. 2017, 102, 261–267. [Google Scholar] [CrossRef]
- Pan, C.C.; Huang, H.L.; Chen, M.C.; Kung, C.Y.; Kung, P.T.; Chou, W.Y.; Tsai, W.C. Lower risk of end stage renal disease in diabetic nurse. BioMedicine 2017, 7, 29–37. [Google Scholar] [CrossRef]
- Salgado, A.C. Quality investigation, designs, evaluation of the methodological strictness and challenges. Liber. 2007, 13, 71–78. [Google Scholar]
- Glaser, B.G.; Strauss, A.L. The Discovery of Grounded Theory: Strategies for Qualitative Research; Aldine: Chicago, IL, USA.
- Boeije, H. A purposeful approach to the constant comparative method in the analysis of qualitative interviews. Qual. Quant. 2002, 36, 391–409. [Google Scholar] [CrossRef]
- Fusch, P.I.; Lawrence, R.N. Are we there yet? Data saturation in qualitative research. Qual. Rep. 2015, 20, 1408–1416. [Google Scholar]
- Kitzinger, J. Introducing focus groups. BMJ 1995, 311, 299–302. [Google Scholar] [CrossRef] [PubMed]
- Barbour, R.S. Using focus groups in general practice research. Fam. Pract. 1995, 12, 328–334. [Google Scholar] [CrossRef] [PubMed]
- Walker, D.; Florence, M. Grounded theory: An exploration of process and procedure. Qual. Health Res. 2006, 16, 547–559. [Google Scholar] [CrossRef]
- Yun-Hee, J. The application of grounded theory and symbolic interactionism. Scand. J. Caring Sci. 2004, 18, 249–256. [Google Scholar]
- Strauss, A.L.; Corbin, J.M. Basic of Qualitative Research. Techniques and Procedures for Developing Grounded Theory; SAGE Publications: London, UK, 1998. [Google Scholar]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32- ítem checklist for interviews and focus group. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef]
- Spanish Personal Data Protection Law. Organic law 15/1999, of December 13. Official Bulletin of the State, nº 298 (14 December 1999). Available online: https://www.boe.es/buscar/pdf/1999/BOE-A-1999-23750-consolidado.pdf (accessed on 15 June 2019).
- Kai, J. What worries parents when their preschool children are acutely ill, and why: A qualitative study. BMJ 1996, 313, 983–986. [Google Scholar] [CrossRef]
- Lagerløv, P.; Helseth, S.; Holager, T. Childhood illnesses and the use of paracetamol (acetaminophen): A qualitative study of parents’ management of common childhood illnesses. Fam. Pract. 2003, 20, 717–723. [Google Scholar] [CrossRef] [PubMed]
- Langer, T.; Pfeifer, M.; Soenmez, A.; Kalitzkus, V.; Wilm, S.; Schnepp, W. Activation of the maternal caregiving system by childhood fever–a qualitative study of the experiences made by mothers with a German or a Turkish background in the care of their children. Fam. Pract. 2013, 14, 35. [Google Scholar] [CrossRef]
- Walsh, A.; Edwards, H.; Fraser, J. Influences on parents´ fever management: Beliefs, experiences and information sources. J. Clin. Nurs. 2007, 16, 2331–2340. [Google Scholar] [CrossRef] [PubMed]
- de Bont, E.G.; Peetoom, K.K.; Moser, A.; Francis, N.A.; Dinant, G.J.; Cals, J.W. Childhood fever: A qualitative study on GPs’ experiences during out-of- hours care. Fam. Pract. 2015, 32, 701–702. [Google Scholar] [CrossRef] [PubMed]
- Westin, E.; Levander, M.S. Parent’s experiences of their children suffering febrile seizures. J. Pediatr. Nurs. 2018, 38, 68–73. [Google Scholar] [CrossRef]
- Ravanipour, M.; Akaberian, S.; Hatami, G. Mothers’ perceptions of fever in children. J. Educ. Health Promot. 2014, 3, 97. [Google Scholar] [PubMed]
- NICE Guidance. Fever in under 5s: Assessment and Initial Management. Available online: https://www.nice.org.uk/guidance/cg160 (accessed on 11 August 2019).
- Sahm, L.J.; Kelly, M.; McCarthy, S.; O’Sullivan, R.; Shiely, F.; Rømsing, J. Knowledge, attitudes and beliefs of parents regarding fever in children: A Danish interview study. Acta. Paediatr. 2016, 105, 69–73. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Sex | Men | Women | ||
|---|---|---|---|---|
| Age | <30 years old | 0 | 4 | |
| 30–40 years old | 15 | 14 | ||
| >40 years old | 12 | 12 | ||
| Number of children | 1 | 7 | 12 | |
| 2 | 11 | 13 | ||
| 3–4 | 7 | 5 | ||
| >4 | 2 | 0 | ||
| Place of residence (environment) | Rural environment | 13 | 16 | |
| Urban environment | 14 | 14 | ||
| Level of studies | No studies | 0 | 0 | |
| Primary studies | 4 | 2 | ||
| Secondary studies | 6 | 9 | ||
| University studies: diploma, Bachelors degree | 16 | 18 | ||
| Master/PhD | 1 | 1 | ||
| Profession | Non-health professional | 14 | 15 | |
| Health professional | Medical degree | 7 | 7 | |
| Nursing diploma or degree | 4 | 8 | ||
| Nurse aide/Health technician | 2 | 0 | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Villarejo-Rodríguez, M.G.; Rodríguez-Martín, B. A Qualitative Study of Parents’ Conceptualizations on Fever in Children Aged 0 to 12 Years. Int. J. Environ. Res. Public Health 2019, 16, 2959. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16162959
Villarejo-Rodríguez MG, Rodríguez-Martín B. A Qualitative Study of Parents’ Conceptualizations on Fever in Children Aged 0 to 12 Years. International Journal of Environmental Research and Public Health. 2019; 16(16):2959. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16162959
Chicago/Turabian StyleVillarejo-Rodríguez, María Gloria, and Beatriz Rodríguez-Martín. 2019. "A Qualitative Study of Parents’ Conceptualizations on Fever in Children Aged 0 to 12 Years" International Journal of Environmental Research and Public Health 16, no. 16: 2959. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16162959