Can Replacing Sitting Time with Standing Time Improve Adolescents’ Cardiometabolic Health?

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Participants
2.2. Physical Activity and Body Position Measures
2.3. Anthropometric, Demographic, and Blood Pressure Measures
2.4. Cardiometabolic Biomarkers Measurement
2.5. Statistical Analysis
3. Results
3.1. Descriptive Characteristics
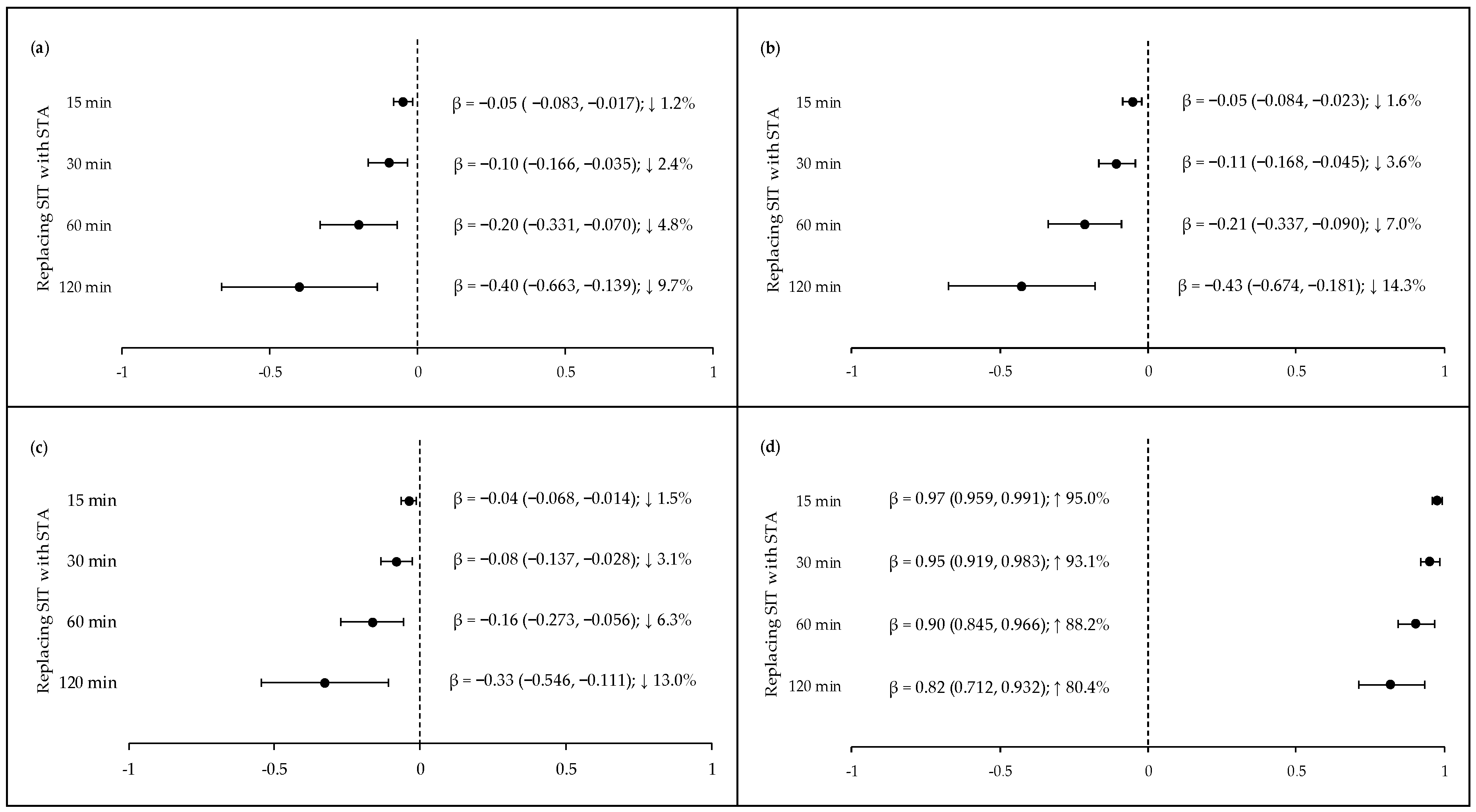
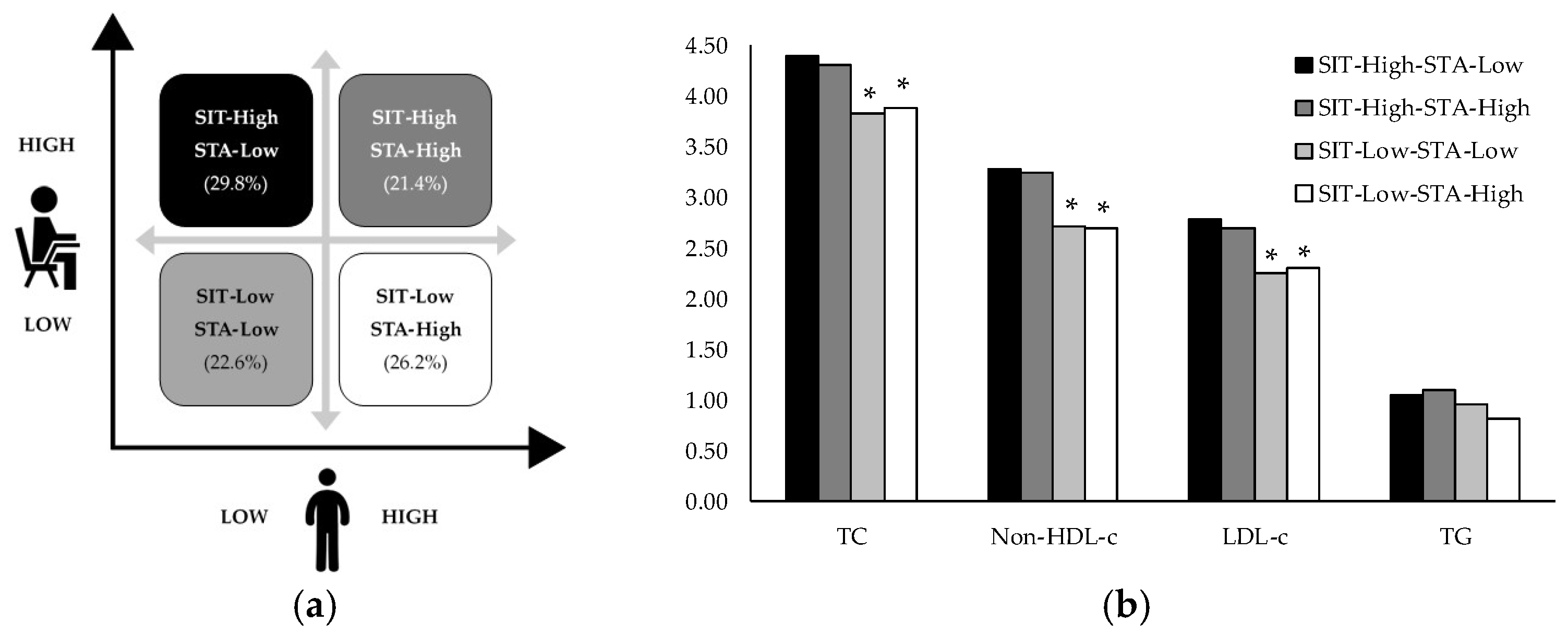
3.2. Replacing Sitting Time with Standing Time
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Contardo Ayala, A.M.; Salmon, J.; Timperio, A.; Sudholz, B.; Ridgers, N.D.; Sethi, P.; Dunstan, D.W. Impact of an 8-Month Trial Using Height-Adjustable Desks on Children’s Classroom Sitting Patterns and Markers of Cardio-Metabolic and Musculoskeletal Health. Int. J. Environ. Res. Public Health 2016, 13. [Google Scholar] [CrossRef] [PubMed]
- Hinckson, E.; Salmon, J.; Benden, M.; Clemes, S.A.; Sudholz, B.; Barber, S.E.; Aminian, S.; Ridgers, N.D. Standing Classrooms: Research and Lessons Learned from Around the World. Sports Med. 2016, 46, 977–987. [Google Scholar] [CrossRef] [PubMed]
- Sherry, A.P.; Pearson, N.; Clemes, S.A. The effects of standing desks within the school classroom: A systematic review. Prev. Med. Rep. 2016, 3, 338–347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sudholz, B.; Timperio, A.; Ridgers, N.D.; Dunstan, D.W.; Baldock, R.; Holland, B.; Salmon, J. The Impact and Feasibility of Introducing Height-Adjustable Desks on Adolescents’ Sitting in a Secondary School Classroom. AIMS Public Health 2016, 3, 274–287. [Google Scholar] [CrossRef] [PubMed]
- Silva, D.R.; Minderico, C.S.; Pinto, F.; Collings, P.J.; Cyrino, E.S.; Sardinha, L.B. Impact of a classroom standing desk intervention on daily objectively measured sedentary behavior and physical activity in youth. J. Sci. Med. Sport 2018, 21, 919–924. [Google Scholar] [CrossRef] [PubMed]
- Penning, A.; Okely, A.D.; Trost, S.G.; Salmon, J.; Cliff, D.P.; Batterham, M.; Howard, S.; Parrish, A.M. Acute effects of reducing sitting time in adolescents: A randomized cross-over study. BMC Public Health 2017, 17, 657. [Google Scholar] [CrossRef] [PubMed]
- Healy, G.N.; Winkler, E.A.; Owen, N.; Anuradha, S.; Dunstan, D.W. Replacing sitting time with standing or stepping: Associations with cardio-metabolic risk biomarkers. Eur. Heart J. 2015, 36, 2643–2649. [Google Scholar] [CrossRef]
- Stamatakis, E.; Gale, J.; Bauman, A.; Ekelund, U.; Hamer, M.; Ding, D. Sitting Time, Physical Activity, and Risk of Mortality in Adults. J. Am. Coll. Cardiol. 2019, 73, 2062–2072. [Google Scholar] [CrossRef]
- Eanes, L. CE: Too Much Sitting: A Newly Recognized Health Risk. Am. J. Nurs. 2018, 118, 26–34. [Google Scholar] [CrossRef]
- Bouchard, C.; Blair, S.N.; Katzmarzyk, P.T. Less Sitting, More Physical Activity, or Higher Fitness? Mayo Clin. Proc. 2015, 90, 1533–1540. [Google Scholar] [CrossRef] [Green Version]
- Ekblom-Bak, E.; Ekblom, O.; Bergstrom, G.; Borjesson, M. Isotemporal substitution of sedentary time by physical activity of different intensities and bout lengths, and its associations with metabolic risk. Eur. J. Prev. Cardiol. 2016, 23, 967–974. [Google Scholar] [CrossRef]
- Butler, K.M.; Ramos, J.S.; Buchanan, C.A.; Dalleck, L.C. Can reducing sitting time in the university setting improve the cardiometabolic health of college students? Diabetes Metab. Syndr. Obes. 2018, 11, 603–610. [Google Scholar] [CrossRef]
- Katzmarzyk, P.T.; Church, T.S.; Craig, C.L.; Bouchard, C. Sitting time and mortality from all causes, cardiovascular disease, and cancer. Med. Sci. Sports Exerc. 2009, 41, 998–1005. [Google Scholar] [CrossRef]
- van der Ploeg, H.P.; Chey, T.; Korda, R.J.; Banks, E.; Bauman, A. Sitting time and all-cause mortality risk in 222 497 Australian adults. Arch. Intern. Med. 2012, 172, 494–500. [Google Scholar] [CrossRef]
- Katzmarzyk, P.T. Standing and mortality in a prospective cohort of Canadian adults. Med. Sci. Sports Exerc. 2014, 46, 940–946. [Google Scholar] [CrossRef]
- Judice, P.B.; Hamilton, M.T.; Sardinha, L.B.; Zderic, T.W.; Silva, A.M. What is the metabolic and energy cost of sitting, standing and sit/stand transitions? Eur. J. Appl. Physiol. 2016, 116, 263–273. [Google Scholar] [CrossRef]
- Australian Department of Health. Australia’s Physical Activity & Sedentary Behaviour Guidelines for Young People (13–17 years). Available online: http://www.health.gov.au/internet/main/publishing.nsf/Content/health-pubhlth-strateg-phys-act-guidelines#apa1317 (accessed on 13 January 2019).
- Tremblay, M.S.; Carson, V.; Chaput, J.P.; Connor Gorber, S.; Dinh, T.; Duggan, M.; Faulkner, G.; Gray, C.E.; Gruber, R.; Janson, K.; et al. Canadian 24-Hour Movement Guidelines for Children and Youth: An Integration of Physical Activity, Sedentary Behaviour, and Sleep. Appl. Physiol. Nutr. Metab. 2016, 41, S311–S327. [Google Scholar] [CrossRef]
- UK Department of Health and Social Care. Start Active, Stay Active: A Report on Physical Activity from the Four Home Countries’ Chief Medical Officers; Department of Health, Physical Activity, Health Improvement and Protection: London, UK, 2011. [Google Scholar]
- Edwardson, C.L.; Henson, J.; Bodicoat, D.H.; Bakrania, K.; Khunti, K.; Davies, M.J.; Yates, T. Associations of reallocating sitting time into standing or stepping with glucose, insulin and insulin sensitivity: A cross-sectional analysis of adults at risk of type 2 diabetes. BMJ Open 2017, 7, e014267. [Google Scholar] [CrossRef]
- Henson, J.; Edwardson, C.L.; Bodicoat, D.H.; Bakrania, K.; Davies, M.J.; Khunti, K.; Talbot, D.C.S.; Yates, T. Reallocating sitting time to standing or stepping through isotemporal analysis: Associations with markers of chronic low-grade inflammation. J. Sports Sci. 2018, 36, 1586–1593. [Google Scholar] [CrossRef]
- Mekary, R.A.; Willett, W.C.; Hu, F.B.; Ding, E.L. Isotemporal substitution paradigm for physical activity epidemiology and weight change. Am. J. Epidemiol. 2009, 170, 519–527. [Google Scholar] [CrossRef]
- Santos-Lozano, A.; Marin, P.J.; Torres-Luque, G.; Ruiz, J.R.; Lucia, A.; Garatachea, N. Technical variability of the GT3X accelerometer. Med. Eng. Phys. 2012, 34, 787–790. [Google Scholar] [CrossRef]
- Romanzini, M.; Petroski, E.L.; Ohara, D.; Dourado, A.C.; Reichert, F.F. Calibration of ActiGraph GT3X, Actical and RT3 accelerometers in adolescents. Eur. J. Sport Sci. 2014, 14, 91–99. [Google Scholar] [CrossRef]
- Choi, L.; Liu, Z.; Matthews, C.E.; Buchowski, M.S. Validation of accelerometer wear and nonwear time classification algorithm. Med. Sci. Sports Exerc. 2011, 43, 357–364. [Google Scholar] [CrossRef]
- Migueles, J.H.; Cadenas-Sanchez, C.; Ekelund, U.; Delisle Nystrom, C.; Mora-Gonzalez, J.; Lof, M.; Labayen, I.; Ruiz, J.R.; Ortega, F.B. Accelerometer Data Collection and Processing Criteria to Assess Physical Activity and Other Outcomes: A Systematic Review and Practical Considerations. Sports Med. 2017, 47, 1821–1845. [Google Scholar] [CrossRef]
- Carr, L.J.; Mahar, M.T. Accuracy of intensity and inclinometer output of three activity monitors for identification of sedentary behavior and light-intensity activity. J. Obes. 2012, 2012, 460271. [Google Scholar] [CrossRef]
- Edwardson, C.L.; Rowlands, A.V.; Bunnewell, S.; Sanders, J.; Esliger, D.W.; Gorely, T.; O’Connell, S.; Davies, M.J.; Khunti, K.; Yates, T. Accuracy of Posture Allocation Algorithms for Thigh- and Waist-Worn Accelerometers. Med. Sci. Sports Exerc. 2016, 48, 1085–1090. [Google Scholar] [CrossRef] [Green Version]
- ActiGraph Corp. ActiGraph White Paper: Estimating Human Position with the ActiGraph GT3X Triaxial Activity Monitor. Available online: https://s3.amazonaws.com/actigraphcorp.com/wp-content/uploads/2017/11/26205804/Inclination-White-Paper.pdf (accessed on 5 October 2018).
- Lohman, T.G.; Roche, A.F.; Martorell, R. Anthropometric Standardization Reference Manual; Human Kinects: Champaign, IL, USA, 1988. [Google Scholar]
- World Health Organization. Growth reference 5–19 years. BMI-for-age (5–19 years). Available online: https://www.who.int/growthref/who2007_bmi_for_age/en/ (accessed on 13 January 2019).
- Hoffman, D.J.; Toro-Ramos, T.; Sawaya, A.L.; Roberts, S.B.; Rondo, P. Estimating total body fat using a skinfold prediction equation in Brazilian children. Ann. Hum. Biol. 2012, 39, 156–160. [Google Scholar] [CrossRef]
- Malachias, M.; Plavnik, F.L.; Machado, C.A.; Malta, D.; Scala, L.C.N.; Fuchs, S. 7th Brazilian Guideline of Arterial Hypertension: Chapter 1—Concept, Epidemiology and Primary Prevention. Arq. Bras. Cardiol. 2016, 107, 1–6. [Google Scholar] [CrossRef]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar]
- Bays, H.E.; Jones, P.H.; Orringer, C.E.; Brown, W.V.; Jacobson, T.A. National Lipid Association Annual Summary of Clinical Lipidology 2016. J. Clin. Lipidol. 2016, 10, S1–S43. [Google Scholar] [CrossRef] [Green Version]
- Hines, G.; Kennedy, I.; Holman, R. The HOMA2 Calculator. Available online: https://www.dtu.ox.ac.uk/homacalculator/ (accessed on 10 December 2018).
- Moura, B.P.; Rufino, R.L.; Faria, R.C.; Sasaki, J.E.; Amorim, P.R.S. Dataset of article: Can. replacing sitting time with standing time improve adolescents cardiometabolic health? Available online: https://data.mendeley.com/datasets/svv8f82rn5/2 (accessed on 10 July 2019).
- Dunstan, D.W.; Howard, B.; Healy, G.N.; Owen, N. Too much sitting—A health hazard. Diabetes Res. Clin. Pract. 2012, 97, 368–376. [Google Scholar] [CrossRef]
- Dunstan, D.W.; Kingwell, B.A.; Larsen, R.; Healy, G.N.; Cerin, E.; Hamilton, M.T.; Shaw, J.E.; Bertovic, D.A.; Zimmet, P.Z.; Salmon, J.; et al. Breaking up prolonged sitting reduces postprandial glucose and insulin responses. Diabetes Care 2012, 35, 976–983. [Google Scholar] [CrossRef]
- Matthews, C.E.; Moore, S.C.; Sampson, J.; Blair, A.; Xiao, Q.; Keadle, S.K.; Hollenbeck, A.; Park, Y. Mortality Benefits for Replacing Sitting Time with Different Physical Activities. Med. Sci. Sports Exerc. 2015, 47, 1833–1840. [Google Scholar] [CrossRef] [Green Version]
- Winkler, E.A.H.; Chastin, S.; Eakin, E.G.; Owen, N.; Lamontagne, A.D.; Moodie, M.; Dempsey, P.C.; Kingwell, B.A.; Dunstan, D.W.; Healy, G.N. Cardiometabolic Impact of Changing Sitting, Standing, and Stepping in the Workplace. Med. Sci. Sports Exerc. 2018, 50, 516–524. [Google Scholar] [CrossRef] [Green Version]
- Chastin, S.F.; Palarea-Albaladejo, J.; Dontje, M.L.; Skelton, D.A. Combined Effects of Time Spent in Physical Activity, Sedentary Behaviors and Sleep on Obesity and Cardio-Metabolic Health Markers: A Novel Compositional Data Analysis Approach. PLoS ONE 2015, 10, e0139984. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables (n = 84) | Mean | (SD) |
|---|---|---|
| Age (years) | 16.69 | (0.93) |
| Weight (kg) | 62.62 | (9.56) |
| Height (m) | 1.74 | (0.06) |
| BMI (kg·m−2) | 20.59 | (2.87) |
| WC (cm) | 73.51 | (6.59) |
| FM (% weight) | 24.33 | (3.73) |
| TC (mmol/L) | 4.11 | (0.62) |
| HDL-c (mmol/L) * | 1.11 | (0.28) |
| Non-HDL-c (mmol/L) | 2.99 | (0.58) |
| LDL-c (mmol/L) | 2.52 | (0.51) |
| TG (mmol/L) * | 0.95 | (0.41) |
| Glucose (mmol/L) | 4.32 | (0.42) |
| Insulin (pmol/L) * | 35.18 | (43.53) |
| HOMA2-β (%) * | 102.35 | (64.80) |
| HOMA2-S (%) * | 156.65 | (141.50) |
| HOMA2-IR * | 0.64 | (0.82) |
| SBP (mmHg) | 111.35 | (11.21) |
| DBP (mmHg) | 72.38 | (7.81) |
| Daily waking hours (DWH) | 15.21 | (2.32) |
| Device wear (days) | 6.69 | (0.64) |
| Sitting time (min·day−1) | 391.79 | (81.43) |
| Lying time (min·day−1) | 111.32 | (75.73) |
| Standing time (min·day−1) | 409.20 | (89.98) |
| Sitting time (% of DWH) | 43.16 | (7.71) |
| Lying time (% of DWH) | 11.68 | (6.57) |
| Standing time (% of DWH) | 45.16 | (9.16) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moura, B.P.; Rufino, R.L.; Faria, R.C.; Sasaki, J.E.; Amorim, P.R.S. Can Replacing Sitting Time with Standing Time Improve Adolescents’ Cardiometabolic Health? Int. J. Environ. Res. Public Health 2019, 16, 3115. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16173115
Moura BP, Rufino RL, Faria RC, Sasaki JE, Amorim PRS. Can Replacing Sitting Time with Standing Time Improve Adolescents’ Cardiometabolic Health? International Journal of Environmental Research and Public Health. 2019; 16(17):3115. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16173115
Chicago/Turabian StyleMoura, Bruno P., Rogério L. Rufino, Ricardo C. Faria, Jeffer E. Sasaki, and Paulo Roberto S. Amorim. 2019. "Can Replacing Sitting Time with Standing Time Improve Adolescents’ Cardiometabolic Health?" International Journal of Environmental Research and Public Health 16, no. 17: 3115. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16173115