An Intervention to Improve Uptake of Referrals for Children with Ear Disease or Hearing Loss in Thyolo District, Malawi: Acceptability and Feasibility


Abstract
:1. Introduction
2. Materials and Methods
2.1. The Intervention
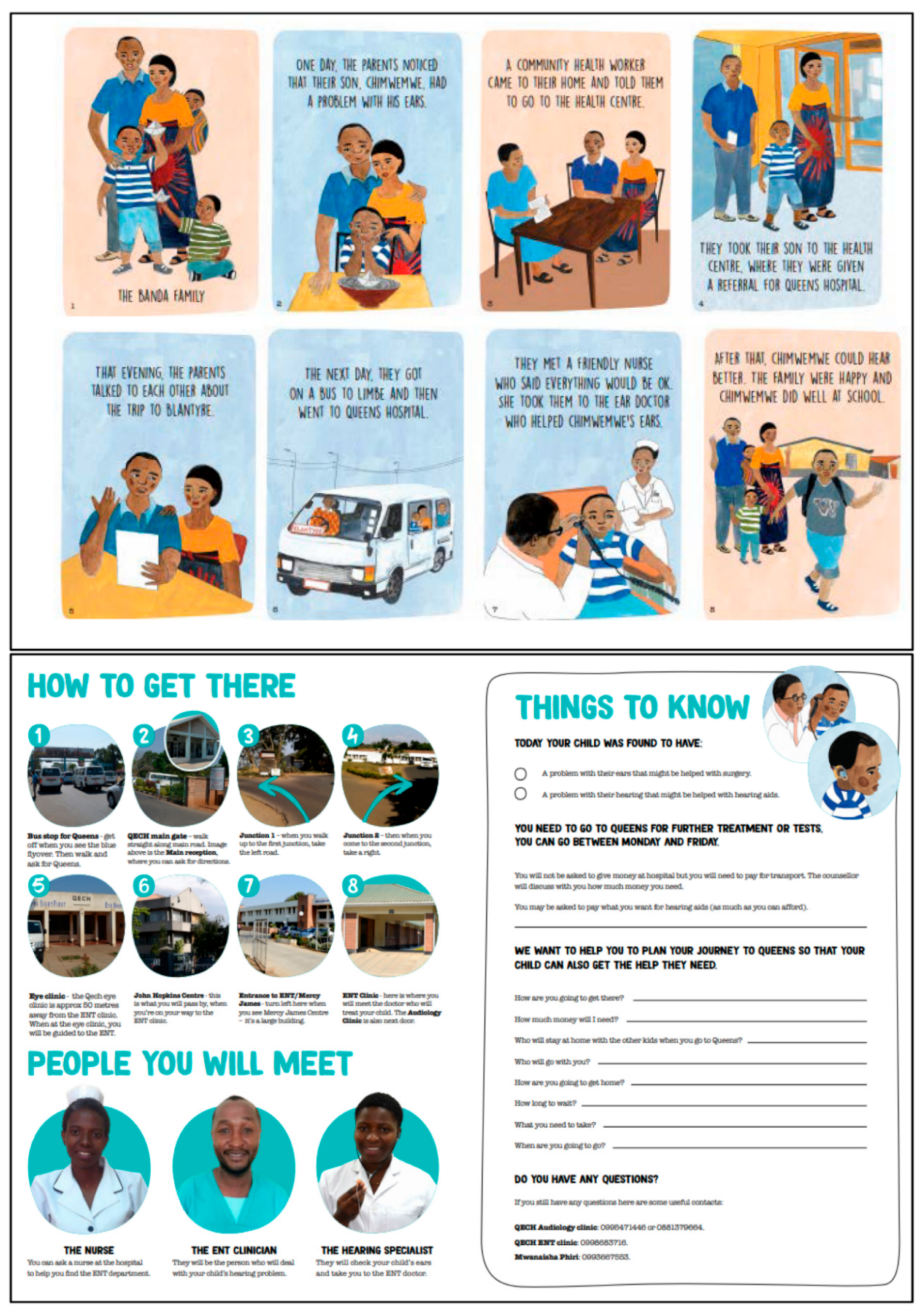
- An information booklet delivered with counselling by a trained health surveillance assistant (HSA) and an “expert mother” at the point at which the referral was made (in outreach camps). The booklet had three sections (Appendix A):
- An illustrated storyline of “The Banda Family” depicting a family going through the process of being referred and attending the referral at QECH;
- Information on getting to QECH, including photographs of key locations/buildings/roads that caregivers would see on the way to the ENT department;
- Tailored action planning section—including how to get to the hospital, how much money is needed, and what they need to bring with them. The majority of services are free at the point of care in Malawi. However, hearing aids may incur out of pocket costs. At the time of writing, the audiology services offered a pay-what-you can system.
- A text message reminder is sent two days before the scheduled appointment, followed by a second text message reminder if they do not attend on the scheduled date. The text message is tailored to the individual, and includes the child’s name, appointment date, and a phone number to call in case of questions.
2.2. Pilot Testing the Intervention
2.2.1. Study Design
2.2.2. Setting
2.2.3. Study Sample
2.2.4. Data Collection
2.2.5. Analysis
2.2.6. Positionality
2.2.7. Ethical Considerations
3. Results
3.1. Study Sample
3.2. Counselling and Booklet: Acceptability
3.2.1. Counselling
Enabling Two-Way Conversation
Wonderful because we were being encouraged. The doctor can explain to you, yes, but you might have questions, and we were able to have a discussion with them.[Caregiver code 316]
Was helpful since it encouraged us. She told us that she also comes from Thyolo.[Caregiver 101]
Dispelling Misconceptions and Fear
It was good because they made us free to see that Queens is not a dangerous place, but [a place] where one can get assistance.[Caregiver 104]
3.2.2. Booklet
Motivation from Storyline
The story that I liked in the booklet is: the parents followed the counselling and their child’s hearing was restored. And the child was happy when he started hearing.[Caregiver 315]
Providing Instructions
They took it and looked at it and said that it was good that the booklet provided directions. It will be easy to travel because it showed where we were going and the doctors who will greet us.[Caregiver 105]
Sharing the Booklet with Networks
Their views about the booklet were that this is a good example, and they felt that this was a good time [to prioritise the problem]; maybe God was answering [our prayers] in that way and we should source money so that the child could go.[Caregiver 308]
I was refusing [uptake] since I didn’t have money for transport; if am not able to find soap in my house, and salt too; and to find 10 thousand kwacha for transport for two people, I wouldn’t make it. And that’s when another woman [neighbour] said “can you bring your booklet and let me look at it”. And they read the [referral] letter and they told me that no matter what, I should do what I can to find money for transport and go with the child.[Caregiver 104]
3.3. Counselling and Booklet: Acceptability
3.3.1. Time Taken
3.3.2. Comprehension
The good thing is that there are people who can read and others who cannot. Nowadays those who cannot read are few and if there is someone who can’t read, they always ask what is written. That means someone will read for them and they can keep the message that they have been told.[Expert mother]
3.3.3. Scale-Up
More HSAs should be trained so that this message can reach the villages. If the people get the message in their homes and villages, maybe they can do something about it. Most people do not know that an ear problem is a problem [that can be treated]. They just keep the children at home. But if they receive the message from us, some people would go on their own to QECH because the booklet has a map. It explains the directions very well. And it also explains the money—how much you will spend - so the person can understand, even be enlightened, about money. One can decide on their own that “this child of mine, I should do this to take her to the hospital, I should not wait for the camp”.[Counsellor]
3.4. Text Message Reminder: Acceptability
Prompt for Caregivers to Take Action
This message is very good and can help a lot of people and be an encouragement to say, ‘oh the trip is on and the hospital is reminding us that we have this problem’. …reminding you that you have a problem is very helpful because it seems that you have someone who cares for your problem.[Caregiver 108]
If the person who brought the [text] message told me that if you fail [to raise the money in time] you can also call and tell them that we’ve failed because of these reasons, then I would have tried to call, but they didn’t say that.[Caregiver 310]
3.5. Text Message Reminder: Feasibility
Network and Phone Coverage
Yes, they should explain the messages concerning ears since more people at this time they listen to the radios. I think in that way the government can take part and tell people about ears, more people may know and would love to go to the hospital. Since there are other people who [have] the problem but don’t know where to go with it.[Caregiver108]
3.6. Residual Barriers to Uptake of Referral
3.6.1. Costs of Seeking Care
I was thinking that I will [ask] people in Johannesburg to send me money, but when I called them to tell them that there is this problem, they told me that they hadn’t been paid and it was too difficult. Now that I’m not working, I’m worried [we won’t be able to go].[Caregiver 308]
There was no problem. Whatever happened here, everyone at home accepted it, and there was nothing to make us fail. We were just waiting. That’s when the sickness [of another family member] came. So when the time [for the child’s appointment] came close, we had spent the money [we had collected] for transport.[Caregiver 101]
3.6.2. Lack of Exposure to Hospitals and the City
3.7. Intervention Costs
4. Discussion
4.1. Acceptability and Feasibility of the Intervention
4.2. Overcoming Barriers
- Location of the hospital,
- Lack of and cost of transport,
- Other indirect costs of seeking care,
- Fear and uncertainty about the referral hospital,
- Lack of understanding about the referral,
- Lack of awareness and understanding of hearing loss,
- Lack of visibility and availability of services.
4.3. Adaptations Prior to Randomised Trial
4.4. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

References
- World Health Organization. Hear the Future 2018. Available online: http://www.who.int/deafness/world-hearing-day/World-Hearing-Day-Infographic-EN.pdf?ua=1 (accessed on 20 July 2019).
- Tesni, S. Going to school with a hearing impairment. Ear Hear. J. 2014, 11, 4–5. [Google Scholar]
- Woodcock, K.; Pole, J.D. Educational attainment, labour force status and injury: A comparison of Canadians with and without deafness and hearing loss. Int. J. Rehabil. Res. 2008, 31, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Asghari, A.; Farhadi, M.; Daneshi, A.; Khabazkhoob, M.; Mohazzab-Torabi, S.; Jalessi, M.; Emamjomeh, H. The Prevalence of Hearing Impairment by Age and Gender in a Population-based Study. Iran. J. Public Health 2017, 46, 1237–1246. [Google Scholar] [PubMed]
- Olusanya, B.O.; Neumann, K.J.; Saunders, J.E. The global burden of disabling hearing impairment: A call to action. Bull. World Health Organ. 2014, 92, 367–373. [Google Scholar] [CrossRef] [PubMed]
- Banks, L.M.; Kuper, H.; Polack, S. Poverty and disability in low- and middle-income countries: A systematic review. PLoS ONE 2017, 12, e0189996. [Google Scholar] [CrossRef] [PubMed]
- Skilton, M.K.; Poole, N.; Metcalfe, C.W.; Martin, T.P.C.; Smith, M.C.F. The impact of ear disease and hearing impairment on the lives of Nepali patients in Pokhara: A qualitative study. Int. Health 2016, 8, 101–107. [Google Scholar] [CrossRef]
- World Health Organization. Childhood Hearing Loss: Strategies for Prevention and Care 2015. Available online: http://apps.who.int/iris/bitstream/handle/10665/204632/9789241510325_eng.pdf?sequence=1 (accessed on 17 April 2018).
- World Health Organization. Multi-Country Assessment of National Capacity to Provide Hearing Care. 2013. Available online: http://www.who.int/pbd/publications/WHOReportHearingCare_Englishweb.pdf (accessed on 16 May 2017).
- Mulwafu, W.; Ensink, R.; Kuper, H.; Fagan, J. Survey of ENT services in sub-Saharan Africa: Little progress between 2009 and 2015. Global Health Action 2017, 10, 1289736. [Google Scholar] [CrossRef] [PubMed]
- Bright, T.; Mulwafu, W.; Thindwa, R.; Zuurmond, M.; Polack, S. Reasons for low uptake of referrals to ear and hearing services for children in Malawi. PLoS ONE 2017, 12, e0188703. [Google Scholar] [CrossRef]
- Bright, T.; Felix, L.; Kuper, H.; Polack, S. A systematic review of strategies to increase access to health services among children in low and middle income countries. BMC Health Serv. Res. 2017, 17, 252. [Google Scholar] [CrossRef]
- Bright, T.; Felix, L.; Kuper, H.; Polack, S. Systematic review of strategies to increase access to health services among children over five in low- and middle-income countries. Trop. Med. Int. Health 2018, 23, 476–507. [Google Scholar] [CrossRef] [Green Version]
- Medical Research Council. Developing and Evaluating Complex Interventions: New Guidance 2006. Available online: https://mrc.ukri.org/documents/pdf/complex-interventions-guidance/ (accessed on 26 July 2018).
- Eldridge, S.M.; Lancaster, G.A.; Campbell, M.J.; Thabane, L.; Hopewell, S.; Coleman, C.L.; Bond, C.M. Defining Feasibility and Pilot Studies in Preparation for Randomised Controlled Trials: Development of a Conceptual Framework. PLoS ONE 2016, 11, e0150205. [Google Scholar] [CrossRef] [PubMed]
- Ásbjörnsdóttir, K.H.; Ajjampur, S.S.R.; Anderson, R.M.; Bailey, R.; Gardiner, I.; Halliday, K.E.; Ibikounle, M.; Kalua, K.; Kang, G.; Littlewood, D.T.J.; et al. Assessing the feasibility of interrupting the transmission of soil-transmitted helminths through mass drug administration: The DeWorm3 cluster randomized trial protocol. PLoS Negl. Trop. Dis. 2018, 12, e0006166. [Google Scholar]
- Lewycka, S.; Mwansambo, C.; Kazembe, P.; Phiri, T.; Mganga, A.; Rosato, M.; Chapota, H.; Malamba, F.; Vergnano, S.; Newell, M.-L.; et al. A cluster randomised controlled trial of the community effectiveness of two interventions in rural Malawi to improve health care and to reduce maternal, newborn and infant mortality. Trials 2010, 11, 88. [Google Scholar] [CrossRef] [PubMed]
- Arain, M.; Campbell, M.J.; Cooper, C.L.; Lancaster, G.A. What is a pilot or feasibility study? A review of current practice and editorial policy. BMC Med. Res. Methodol. 2010, 10, 67. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.A. Evaluating the contribution of interpretative phenomenological analysis. Health Psychol. Rev. 2011, 5, 9–27. [Google Scholar] [CrossRef]
- Smith, J.A.; Osborn, M. Doing Interpretative Phenomenological Analysis. In Qualitative Health Psychology: Theories and Methods; SAGE Publications: London, UK, 1999. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Allen, M. The SAGE Encyclopedia of Communication Research Methods; SAGE Publications: London, UK, 2017. [Google Scholar]
- Wilbur, J.; Bright, T.; Mahon, T.; Hameed, S.; Torondel, B.; Mulwafu, W.; Kuper, H.; Polack, S. Developing Behaviour Change Interventions for Improving Access to Health and Hygiene for People with Disabilities: Two Case Studies from Nepal and Malawi. Int. J. Environ. Res. Public Health 2018, 15, 2746. [Google Scholar] [CrossRef]
- Shilling, V.; Morris, C.; Thompson-Coon, J.; Ukoumunne, O.; Rogers, M.; Logan, S. Peer support for parents of children with chronic disabling conditions: A systematic review of quantitative and qualitative studies. Develop. Med. Child Neurol. 2013, 55, 602–609. [Google Scholar] [CrossRef]
- Peers for Progress. Global Evidence for Peer Support: Humanizing Health Care 2014. Peers for Progress, 16 September 2014. [Google Scholar]
- Kaunda-Khangamwa, B.N.; Steinhardt, L.C.; Rowe, A.K.; Gumbo, A.; Moyo, D.; Nsona, H.; Troell, P.; Zurovac, D.; Mathanga, D. The effect of mobile phone text message reminders on health workers’ adherence to case management guidelines for malaria and other diseases in Malawi: Lessons from qualitative data from a cluster-randomized trial. Malar. J. 2018, 17, 481. [Google Scholar] [CrossRef]
- Zurovac, D.; Sudoi, R.K.; Akhwale, W.S.; Ndiritu, M.; Hamer, D.H.; Rowe, A.K.; Snow, R.W. The effect of mobile phone text-message reminders on Kenyan health workers’ adherence to malaria treatment guidelines: A cluster randomised trial. Lancet 2011, 378, 795–803. [Google Scholar] [CrossRef]
- Mahande, M.; Tharaney, M.; Kirumbi, E.; Ngirawamungu, E.; Geneau, R.; Tapert, L.; Courtright, P. Uptake of trichiasis surgical services in Tanzania through two village-based approaches. Br. J. Ophthalmol. 2007, 91, 139–142. [Google Scholar] [CrossRef] [PubMed]
- Naugle, D.A.; Hornik, R.C. Systematic review of the effectiveness of mass media interventions for child survival in low- and middle-income countries. J. Health Commun. 2014, 19 (Suppl. 1), 190–215. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, B.; Ir, P.; Bigdeli, M.; Annear, P.L.; Van Damme, W. Addressing access barriers to health services: An analytical framework for selecting appropriate interventions in low-income Asian countries. Health Policy Plan. 2012, 27, 288–300. [Google Scholar] [CrossRef] [PubMed]
- Kazibwe, H.; Struthers, P. Barriers experienced by parents of children with clubfoot deformity attending specialised clinics in Uganda. Trop. Doct. 2009, 39, 15–18. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.W.; Sathyan, P.; John, R.K.; Singh, K.; Robin, A.L. Predictors of and barriers associated with poor follow-up in patients with glaucoma in South India. Arch. Ophthalmol. 2008, 126, 1448–1454. [Google Scholar] [CrossRef] [PubMed]
- Raje, F. Rural Transport Interventions to Improve Maternal Health Outcomes 2018. Available online: https://assets.publishing.service.gov.uk/media/5b69d458e5274a1521d88e95/Maternal_health_and_transport.pdf (accessed on 11 February 2019).
- Ksoll, C.; Lilleør, H.B.; Lønborg, J.H.; Rasmussen, O.D. Impact of Village Savings and Loan Associations: Evidence from a cluster randomized trial. J. Develop. Econ. 2016, 120, 70–85. [Google Scholar] [CrossRef] [Green Version]
- Mulwafu, W.; Kuper, H.; Viste, A.; Goplen, F.K. Feasibility and acceptability of training community health workers in ear and hearing care in Malawi: A cluster randomised controlled trial. BMJ Open 2017, 7, e016457. [Google Scholar] [CrossRef]

{kind=link}
| Child Characteristics | n (%) |
|---|---|
| Mean age (range) (years) | 10.5 (4–16) |
| Sex | |
| Male | 13 (43%) |
| Female | 17 (57%) |
| Duration of hearing difficulty | |
| <1 year | 7 (23%) |
| Between 1–5 years | 18 (60%) |
| >5 years | 4 (13%) |
| Don’t know | 1 (3%) |
| Attend school (among those of school age) | 27 (100%) |
| Grade | |
| Same year as other children | 10 (37%) |
| Lower grade than other children their age | 16 (59%) |
| Higher grade than other children their age | 1 (3%) |
| Referral type | |
| Hearing assessment/hearing aids | 11 (37%) |
| Surgery | 19 (63%) |
| Caregiver characteristics ** | |
| Sex | |
| Male | 6 (20%) |
| Female | 24 (80%) |
| Age group (years) | |
| 19–29 | 9 (30%) |
| 30–39 | 14 (47%) |
| 40–49 | 7 (23%) |
| Mean age (range) (years) | 34.0 (19–49) |
| Primary caregiver | |
| Yes | 26 (87%) |
| No | 4 (13%) |
| Relationship to child | |
| Mother | 19 (63%) |
| Father | 5 (17%) |
| Grandparent | 1 (3%) |
| Other | 5 (17%) |
| Father lives in same household | |
| Yes | 16 (53%) |
| No | 14 (47%) |
| Father contact in last 6 months | |
| Daily | 16 (53%) |
| Monthly | 3 (10%) |
| Once every 6 months | 2 (7%) |
| Less often | 1 (3%) |
| Father not alive | 6 (20%) |
| Unknown | 2 (7%) |
| Literacy | |
| Literate | 25 (83%) |
| Illiterate | 5 (17%) |
| Currently Working | |
| Yes, full time | 8 (26%) |
| Part time | 4 (13%) |
| No | 18 (60%) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baum, A.; Mulwafu, W.; Phiri, M.; Polack, S.; Bright, T. An Intervention to Improve Uptake of Referrals for Children with Ear Disease or Hearing Loss in Thyolo District, Malawi: Acceptability and Feasibility. Int. J. Environ. Res. Public Health 2019, 16, 3144. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16173144
Baum A, Mulwafu W, Phiri M, Polack S, Bright T. An Intervention to Improve Uptake of Referrals for Children with Ear Disease or Hearing Loss in Thyolo District, Malawi: Acceptability and Feasibility. International Journal of Environmental Research and Public Health. 2019; 16(17):3144. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16173144
Chicago/Turabian StyleBaum, Antonia, Wakisa Mulwafu, Mwanaisha Phiri, Sarah Polack, and Tess Bright. 2019. "An Intervention to Improve Uptake of Referrals for Children with Ear Disease or Hearing Loss in Thyolo District, Malawi: Acceptability and Feasibility" International Journal of Environmental Research and Public Health 16, no. 17: 3144. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16173144