A Systematic Review of the Antecedents and Prevalence of Suicide, Self-Harm and Suicide Ideation in Australian Aboriginal and Torres Strait Islander Youth


Abstract
:1. Introduction
2. Methods and Materials
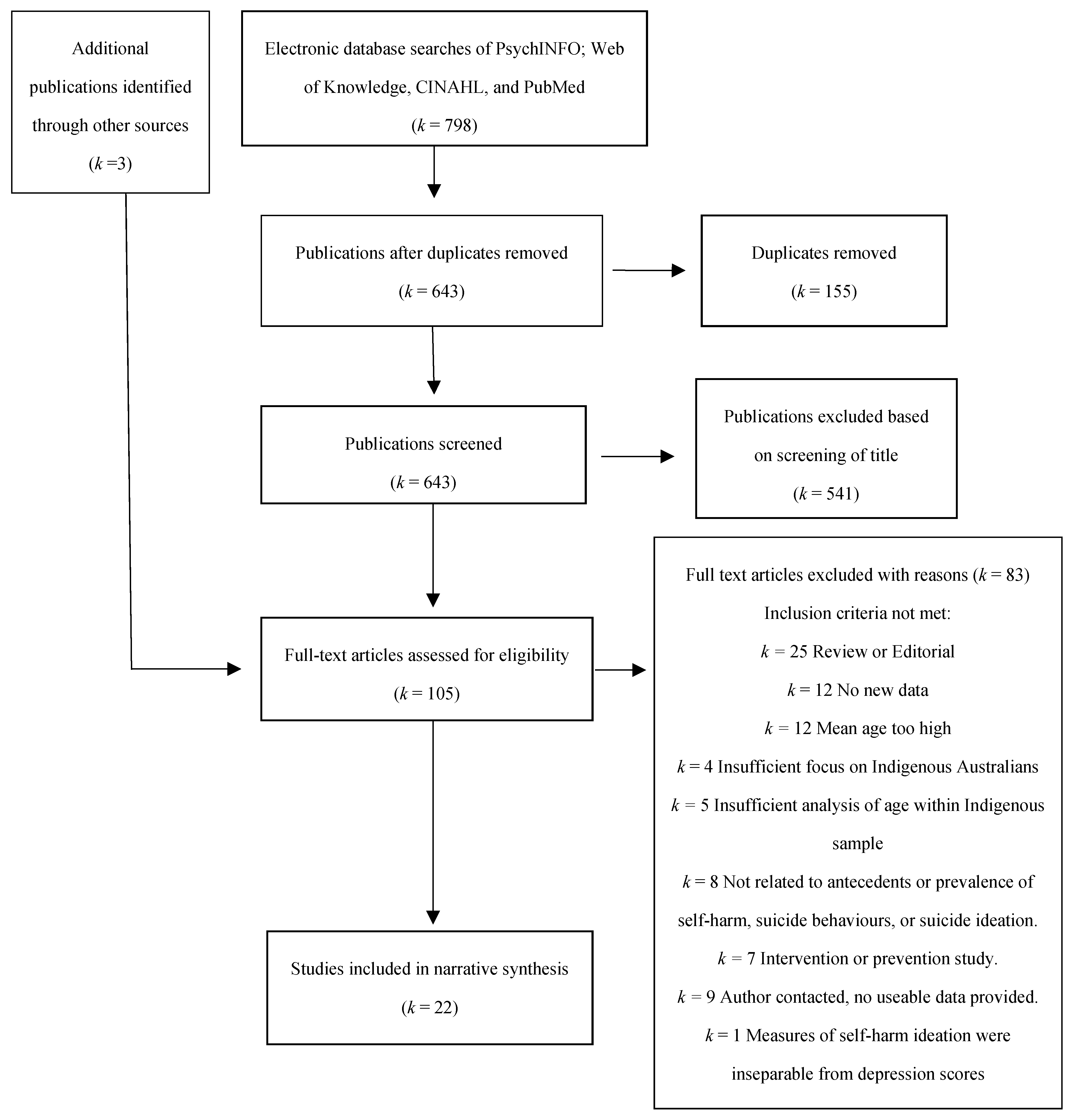
2.1. Search Strategy and Selection Criteria
2.2. Risk of Bias
3. Results
4. Discussion
5. Conclusions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Preventing Suicide: A Global Imperative; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Bergen, H.; Hawton, K.; Waters, K.; Ness, J.; Cooper, J.; Steeg, S.; Kapur, N. Premature death after self-harm: A multicentre cohort study. Lancet 2012, 380, 1568–1574. [Google Scholar] [CrossRef]
- Hawton, K.; Bergen, H.; Cooper, J.; Turnbull, P.; Waters, K.; Ness, J.; Kapur, N. Suicide following self-harm: Findings from the Multicentre Study of self-harm in England 2000–2012. J. Affect. Disord. 2015, 175, 147–151. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, J.D.; Franklin, J.C.; Fox, K.R.; Bentley, K.H.; Kleiman, E.M.; Chang, B.P.; Nock, M.K. Self-injurious thoughts and behaviors as risk factors for future suicide ideation, attempts, and death: A meta-analysis of longitudinal studies. Psychol. Med. 2016, 46, 225–236. [Google Scholar] [CrossRef] [PubMed]
- De Leo, D.; Heller, J.S. Who are the kids who self-harm? An Australian self-report school survey. Med. J. Aust. 2004, 181, 140–144. [Google Scholar] [PubMed]
- National Collaborating Centre for Mental Health. Self-Harm: The Short-Term Physical and Psychological Management and Secondary Prevention of Self-Harm in Primary and Secondary Care; NICE: London, UK, 2004. [Google Scholar]
- Royal College of Psychiatrists. Self-Harm, Suicide and Risk: Helping People Who Self-Harm; Royal College of Psychiatrists: London, UK, 2010. [Google Scholar]
- Schmidtke, A.; Bille-Brahe, U.; De Leo, D.; Kerkhof, A.; Bjerke, T.; Crepet, P.; Haring, C.; Hawton, K.; Lönngvist, J.; Michel, K.; et al. Attempted suicide in Europe: Rates, trends, and sociodemographic characteristics of suicide attempters during the period of 1989-1992. Results of the WHO/EURO multicentre study on parasuicide. Acta Psychiatr. Scand. 1996, 93, 327–338. [Google Scholar] [CrossRef] [PubMed]
- Beautrais, A.L. Risk factors for suicide and attempted suicide among young people. Aust. N. Z. J. Psychiatry 2000, 34, 420–436. [Google Scholar] [CrossRef]
- Christensen, H.; Batterham, P.J.; Mackinnon, A.J.; Donker, T.; Soubelete, A. Predictors of the risk factors of suicide identified by interpersonal psychological theory of suicidal behaviour. Psychiatry Res. 2014, 219, 290–297. [Google Scholar] [CrossRef] [PubMed]
- Hawton, K.; Saunder, K.E.; O’Connor, R.C. Self-harm and suicide in adolescents. Lancet 2012, 379, 2373–2382. [Google Scholar] [CrossRef]
- Reinherz, H.Z.; Tanner, J.L.; Berger, S.R.; Beardslee, W.R.; Fitzmaurice, G.M. Adolescent suicidal ideation as predictive of psychopathology, suicide behaviors and compromised functioning at age 30. Am. J. Psychiatry 2006, 163, 1226–1232. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. Causes of Death, Australia. 2016. Available online: http://www.abs.gov.au/ausstats/[email protected]/Lookup/by%20Subject/3303.0~2016~Main%20Features~Intentional%20self-harm%20in%20Aboriginal%20and%20Torres%20Strait%20Islander%20people~8 (accessed on 11 August 2017).
- Australian Institute of Health and Welfare. Australia’s Health 2014; AIHW: Canberra, Australia, 2014. Available online: https://www.aihw.gov.au/reports/australias-health/australias-health-2014/ (accessed on 11 August 2017).
- Calma, T.; Dudgeon, P.; Bray, A. Aboriginal and Torres Strait Islander social and emotional wellbeing and mental health. Aust. Psychol. 2017, 52, 255–260. [Google Scholar] [CrossRef]
- Australian Institute of Health and Wellness. Substance Use among Aboriginal and Torres Strait Islander People; AIHW: Canberra, Australia, 2011. Available online: https://www.aihw.gov.au/getmedia/7eb356be-c2cd-4562-a240-010cbbe257f2/11503.pdf.aspx?inline=true (accessed on 11 August 2017).
- Form, A.F.; Bourchler, S.J.; Cvetkowski, S.; Stewart, G. Mental health of Indigenous Australians: A review of findings from community surveys. Med. J. Aust. 2012, 196, 118–121. [Google Scholar] [CrossRef]
- Hunter, E. Disadvantage and discontent: A review of issues relevant to the mental health of rural and remote Indigenous Australians. Aust. J. Rural Health. 2007, 15, 88–93. [Google Scholar] [CrossRef] [PubMed]
- O’Moran, P.; Coffey, C.; Romaniuk, H.; Olsson, C.; Borschmann, R.; Carlin, J.B. The natural history of self-harm from adolescence to young adulthood: A population-based cohort study. Lancet 2012, 379, 236–243. [Google Scholar] [CrossRef]
- Senate Community Affairs Reference Committee. The Hidden Toll: Suicide in Australia 2011; Commonwealth of Australia: Canberra, Australia, 2011. [Google Scholar]
- Tighe, J.; McKay, K.; Maple, M. ‘I’m going to kill myself if you don’t …’: Contextual aspects of suicide in Australian Aboriginal communities. Int. J. Cult. Ment. Health 2015, 8, 1–12. [Google Scholar] [CrossRef]
- World Health Organisation. Recognizing Adolescence. Available online: http://apps.who.int/adolescent/second-decade/section2/page1/recognizing-adolescence.html (accessed on 11 August 2017).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.W.; Plassman, B.L.; Burke, J.; Holsinger, T.; Benjamin, S. Preventing Alzheimer’s Disease and Cognitive Decline; Duke Evidence-Based Practice Center: Durham, NC, USA, 2010. [Google Scholar]
- Taylor, P.J.; Jomar, K.; Dhingra, K.; Forrester, R.; Shahmalak, U.; Dickson, J.M. A meta-analysis of the prevalence of different functions of non-suicidal self-injury. J. Affect. Disord. 2017, 227, 759–769. [Google Scholar] [CrossRef] [PubMed]
- Byard, R.W.; Austin, A.E.; van den Heuvel, C. Characteristics of asphyxial deaths in adolescence. Forensic Leg. Med. 2011, 18, 107–109. [Google Scholar] [CrossRef] [PubMed]
- Campbell, A.; Chapman, M.; McHugh, C.; Sng, A.; Balaratnasingam, S. Rising indigenous suicide rates in Kimberley and implications for suicide prevention. Australas Psychiatry 2016, 24, 561–564. [Google Scholar] [CrossRef]
- Clayer, J.R.; Czechowicz, A.S. Suicide by Aboriginal people in South Australia: Comparisons with suicide deaths in the total urban and rural populations. Med. J. Aust. 1991, 154, 683–685. [Google Scholar]
- De Leo, D.; Sveticic, J.; Milner, A. Suicide in indigenous people in Queensland, Australia: Trends and methods, 1994–2007. Aust. N. Z. J. Psychiatry 2011, 45, 532–538. [Google Scholar] [CrossRef]
- Pridmore, S.; Fujiyama, H. Suicide in the Northern Territory, 2001–2006. Aust. N. Z. J. Psychiatry 2009, 43, 1126–1130. [Google Scholar] [CrossRef] [PubMed]
- Robinson, J.; Too, L.S.; Pirkis, J.; Spittal, M.J. Spatial suicide clusters in Australia between 2010 and 2012: A comparison of cluster and non-cluster among young people and adults. BMC Psychiatry 2016, 16, 417. [Google Scholar] [CrossRef] [PubMed]
- Soole, R.; Kõlves, K.; De Leo, D. Factors related to childhood suicides: Analysis of the Queensland Child Death Register. Crisis 2014, 35, 292–300. [Google Scholar] [CrossRef] [PubMed]
- Soole, R.; Kolves, K.; De Leo, D. Suicides in Aboriginal and Torres Strait Islander children: Analysis of Queensland Suicide Register. Aust. N. Z. J. Public Health 2014, 38, 574–578. [Google Scholar] [CrossRef] [PubMed]
- Burvill, P.W. Attempted suicide in the Perth statistical division 1971–1972. Aust. N. Z. J. Psychiatry 1975, 9, 273–279. [Google Scholar] [CrossRef]
- Leckning, B.A.; Li, S.Q.; Cunningham, T.; Guthridge, S.; Robinson, G.; Nagel, T.; Silburn, S. Trends in hospital admissions involving suicidal behaviour in the Northern Territory, 2001–2013. Australas Psychiatry 2016, 24, 300–304. [Google Scholar] [CrossRef]
- Rock, D.J.; Franz Hallmayer, J. The seasonal risk for deliberate self-harm. Crisis 2008, 29, 191–201. [Google Scholar] [CrossRef]
- Adams, K.; Halacas, C.; Cincoita, M.; Pesich, C. Mental health and Victorian Aboriginal people: What can data mining tell up? Aust. J. Prim. Health 2014, 20, 350–355. [Google Scholar] [CrossRef]
- Jamieson, L.M.; Paradies, Y.C.; Gunthorpe, W.; Cairney, S.J.; Sayers, S.M. Oral health and social and emotional well-being in a birth cohort of Aboriginal Australian young adults. BMC Public Health 2011, 11, 656. [Google Scholar] [CrossRef]
- Luke, J.N.; Anderson, I.P.; Gee, G.J.; Thorpe, R.; Rowley, K.G.; Reilly, R.E.; Thorpe, A.; Stewart, P.J. Suicide ideation and attempt in a community cohort of urban Aboriginal youth: A cross-sectional study. Crisis 2013, 34, 251–261. [Google Scholar] [CrossRef]
- Priest, N.C.; Paradies, Y.C.; Gunthorpe, W.; Cairney, S.J.; Sayers, S.M. Racism as a determinant of social and emotional wellbeing for Aboriginal youth. Med. J. Aust. 2011, 194, 546–550. [Google Scholar] [PubMed]
- Zubrick, S.R.; Mitrou, F.; Lawrence, D.; Silburn, S.R. Maternal death and the onward psychosocial circumstances of Australian Aboriginal children and young people. Psychol. Med. 2011, 41. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, G.; Pirkis, J.; Arabena, K.; Currier, D.; Spittal, M.J.; Jorm, A.F. Suicidal behaviour in Indigenous compared to non-Indigenous males in urban and regional Australia: Prevalence data suggest disparities increase across age groups. Aust. N. Z. J. Psychiatry 2017, 51, 1240–1248. [Google Scholar] [CrossRef] [PubMed]
- Rouen, C.; Clough, A.R.; West, C. Non-fatal deliberate self-harm in three remote Indigenous communities in far north Queensland, Australia. Crisis 2019. [Google Scholar] [CrossRef] [PubMed]
- Fasher, A.M.; Dunbar, N.; Rothenbury, B.A.; Bebb, D.K.; Young, S.J.W. The health of a group of young Australians in a New South Wales juvenile detention centre: A pilot study. J. Paediatr. Child Health 1997, 33, 426–429. [Google Scholar] [CrossRef] [PubMed]
- Lawlor, D.; Kosky, R. Serious suicide attempts among adolescents in custody. Aust. N. Z. J. Psychiatry 1992, 26, 474–478. [Google Scholar] [CrossRef] [PubMed]
- Sawyer, M.G.; Guidolin, M.; Schulz, K.L.; McGinnes, B.; Zubrick, S.R.; Baghurst, P.A. The mental health and wellbeing of adolescents on remand in Australia. Aust. N. Z. J. Psychiatry 2010, 44, 551–559. [Google Scholar] [PubMed]
- Stathis, S.L.; Doolan, I.; Letters, P.; Arnett, A.; Cory, S.; Quinlan, L. Use of the Westerman Aboriginal Symptoms Checklist—Youth (WASC-Y) to screen for mental health problems in Indigenous youth in custody. Adv. Ment. Health 2012, 10, 235–239. [Google Scholar] [CrossRef]
- Tatz, C. Aboriginal Suicide Is Different. Aboriginal Youth Suicide in New South Wales, Australian Capital Territory, and New Zealand. Towards a Model of Explanation and Alleviation; Macquarie University: Sydney, Australia, 1999. [Google Scholar]
- Dudgeon, P.; Milroy, J.; Calma, T.; Luxford, Y.; Ring, I.; Walker, R.; Cox, A.; Georgatos, G.; Holland, C. Solutions That Work: What the Evidence and Our People Tell Us. Aboriginal and Torres Strait Islander Suicide Prevention Evaluation Project University of Western Australia. Available online: http://www.atsispep.sis.uwa.edu.au/#final-report (accessed on 10 August 2017).
- Australian Government. National Aboriginal and Torres Strait Islander Suicide Prevention Strategy; Department of Health and Aging: Canberra, Australian, 2013. Available online: http://www.health.gov.au/internet/main/publishing.nsf/content/mental-pub-atsi-suicide-prevention-strategy (accessed on 10 August 2017).
- Armstrong, G.; Ironfield, N.; Kelly, C.M.; Dart, K.; Arabena, K.; Bond, K.; Jorm, A.F. Re-development of mental health first aid guidelines for supporting Aboriginal and Torres Strait Islanders who are engaging in non-suicidal self-injury. BMC Psychiatry 2017, 17. [Google Scholar] [CrossRef] [PubMed]
- Isaacs, A.; Sutton, K. An Aboriginal youth suicide prevention project in rural Victoria. Adv. Ment. Health 2016, 14, 118–125. [Google Scholar] [CrossRef]
- Hawton, K.; Witt, K.G.; Salisbury, T.L.T.; Arensman, E.; Gunnell, D.; Hazell, P. Psychosocial interventions following self-harm in adults: A systematic review and meta-analysis. Lancet Psychiatry 2016, 3, 740–750. [Google Scholar] [CrossRef]
- Leske, S.; Harris, M.G.; Charlson, F.J.; Ferrari, A.J.; Baxter, A.J.; Logan, J.M.; Toombs, M.; Whitelfor, H. Systematic review of interventions for Indigenous adults with mental and substance use disorders in Australia, Canada, New Zealand and the United States. Aust. N. Z. J. Psychiatry 2016, 50, 1040–1054. [Google Scholar] [CrossRef] [PubMed]
- Shand, F.; Mackinnon, A.; O’Moore, K.; Ridani, R.; Reda, B.; Hoy, M.; Heard, T.; Duffy, L.; Shanahan, M.; Pulver, L.J.; et al. The iBobbly Aboriginal and Torres Strait Islander app project: Study protocol for a randomised controlled trial. Trials 2019, 20, 198. [Google Scholar] [CrossRef] [PubMed]
- Kuipers, P.; Lindeman, M.A.; Grant, L.; Dingwall, K. Front-line worker perspectives on Indigenous youth suicide in Central Australia: Initial treatment and response. Adv. Ment. Health 2016, 14, 106–117. [Google Scholar] [CrossRef]
- Nasir, B.; Kisely, S.; Hides, L.; Ranmuthugala, G.; Brennan-Olsen, S.; Nicholson, G.C.; Gill, N.S.; Hayman, N.; Kondalsamy-Chennakesavan, S.; Toombs, M. An Australian Indigenous community-led suicide intervention skills training program: Community consultation findings. BMC Psychiatry 2017, 17, 219. [Google Scholar] [CrossRef] [PubMed]
- Skerrett, D.M.; Gibson, M.; Darwin, L.; Lewis, S.; Rallah, R.; Diego, D.L. Closing the gap in Aboriginal and Torres Strait Islander youth suicide: A social–emotional wellbeing service innovation project. Aust. Psychol. 2018, 53, 13–22. [Google Scholar] [CrossRef]


{kind=link}
| Title | Unbiased Sample Selection | Selection Minimise Baseline Difference | Sample Size Calculated | Adequate Description of Cohort | Aboriginal Status Clearly Stated | Validated Method for Ascertaining Suicide/Self-Harm | Blind to Exposure | Adequate Follow up Period | Minimal Missing Data | Analysis Controls for Confounding | Analytic Methods Appropriate |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Adams et al. (2014) [37] | Yes | n/a | n/a | Partial | Yes | Partial | n/a | n/a | Yes | n/a | n/a |
| Armstrong et al. (2017) [42] | Yes | n/a | n/a | Yes | Yes | Yes | n/a | n/a | Yes | n/a | Yes |
| Burvill (1975) [34] | Yes | n/a | n/a | Yes | Yes | Yes | n/a | n/a | Yes | n/a | Yes |
| Byard et al. (2011) [26] | Yes | n/a | n/a | Yes | Yes | Yes | n/a | Partial | Yes | n/a | n/a |
| Campbell et al. (2016) [27] | Yes | n/a | n/a | Yes | Yes | Yes | n/a | n/a | Yes | n/a | Yes |
| Clayer & Czechowicz (1991) [28] | Yes | n/a | n/a | Yes | Yes | Yes | n/a | n/a | Yes | n/a | n/a |
| De Leo et al. (2011) [29] | Yes | n/a | No | Yes | Yes | Yes | n/a | Partial | Yes | n/a | Yes |
| Fascher et al. (1997) [44] | Yes | n/a | n/a | Yes | Yes | Partial | No | n/a | Yes | n/a | n/a |
| Jamieson et al. (2011) [38] | Yes | n/a | No | Yes | Yes | Yes | n/a | Partial | Yes | Yes | Yes |
| Lawlor & Kosky (1992) [45] | Yes | n/a) | n/a | Yes | Yes | Yes | n/a | n/a | Yes | n/a | n/a |
| Leckning et al. (2016) [35] | Yes | n/a | No | Yes | Yes | Yes | n/a | n/a | Yes | n/a | Yes |
| Luke et al. (2013) [39] | Yes | n/a | No | Yes | Yes | Partial | No | n/a | Yes | Yes | |
| Pridmore & Fujiyama (2009) [30] | Yes | n/a | No | No | Yes | Yes | n/a | n/a | Yes | n/a | Yes |
| Priest et al. (2011) [40] | Yes | n/a | Partial | Yes | Yes | Partial | No | n/a | No | Yes | Yes |
| Robinson et al. (2016) [31] | Yes | n/a | No | No | Yes | Yes | n/a | Yes | Yes | n/a | Yes |
| Rock & Hallmayer (2008) [36] | Yes | n/a | No | Partial | Yes | Yes | n/a | Yes | Yes | No | Yes |
| Rouen et al. (2019) [43] | Yes | n/a | n/a | Partial | Yes | Yes | n/a | n/a | Yes | n/a | Yes |
| Sawyer et al. (2010) [46] | Yes | No | No | Yes | Yes | Partial | No | n/a | Yes | No | Yes |
| Soole et al. (2014a) [32] | Yes | n/a | No | Yes | Yes | Yes | n/a | n/a | Yes | n/a | Yes |
| Soole et al. (2014b) [33] | Yes | n/a | No | Yes | Yes | Yes | n/a | n/a | Yes | No | Yes |
| Stathis et al. (2012) [47] | Yes | n/a | No | Partial | Yes | Yes | No | n/a | Yes | No | Yes |
| Zubrick et al. (2011) [41] | Yes | n/a | No | Yes | Yes | No | No | n/a | unclear | No | Yes |
| Author | Sample | Data Period | State of Australia | Method | Measure or Suicidality/Self-Harm |
|---|---|---|---|---|---|
| Adams et al. (2014) [37] | Total calls to Kids Helpline: N = 16,687 (5–25 years) Aboriginal: N = 450 calls Non-Aboriginal: N = 16,237 calls | 2012 | Victoria (VIC) | Analysed data from Kids Helpline, a counselling service for young people | Call categorisation by call centre workers |
| Armstrong et al. (2017) [42] | Indigenous males: N = 432 (2.7% of sample) Nonindigenous males: N = 15,859 (97.3% of sample) 14–17 years n = 48 Indigenous males n = 1135 Nonindigenous males18–24 years n = 71 Indigenous males n = 1853 Nonindigenous males | 2013–2014 | All | Relevant cross-sectional prevalence data extracted from large-scale cohort study of Australian males aged a 10-years and older. The Australian Longitudinal Study on Male Health (Ten to Men) | Item 9 (PHQ-9) to assess prevalence of suicidal thoughts. Single item to assess suicide attempts |
| Burvill (1975) [34] | Total attempted suicides: N = 2036; (age range: 15–24) Aboriginal: N = 18 Non-Aboriginal: N = 2018 | 1971–1972 | Western Australia (WA) | Examined hospital data on attempted suicide rates in Perth | Hospital morbidity data |
| Byard et al. (2011) [26] | Total adolescent deaths: N = 522 Suicide attributed to asphyxia: N = 62; Mage 16.6 years (SD not reported) (age range: 10–18) Breakdown by ethnicity not reported. | 1994–2010 | South Australia (SA) | Examined Coronial reports of adolescent asphyxial deaths | Coroner’s reports |
| Campbell et al. (2017) [27] | Reported deaths by suicide: N = 125 (age range: 0–14; 15–19; 20–24) Indigenous suicide: N = 102 Nonindigenous suicide: N = 16 Ethnicity not known: N = 7 | 2005–2014 | Western Australia (WA) | Audit of suicide data provided to Kimberly Mental Health and Drug Service | Coroner’s reports |
| Clayer & Czechowicz (1991) [28] | Total Suicides: N = 125 (age range: 10–19) Aboriginal: N = 15 (12 Male) Non-Aboriginal: N = 110 (93 Male) | 1981–1988 | South Australia (SA) | Examined coroner’s records | Coroner’s reports |
| De Leo et al. (2011) [29] | Not Reported | 1994–2007 | Queensland (QLD) | Analysis of Queensland Suicide Register | Coroner’s reports |
| Fasher et al. (1997) [44] | Total detainees: N = 100; Mage: 15.9 ± 1.37 (range 12–18) Aboriginal N = 30 Non-Aboriginal: N = 70 | 1994 | New South Wales (NSW) | Analysed nursing admission forms and semistructured interviews with detainees at Cobham Juvenile Justice Centre | Nursing admission assessment forms. Suicide ideation recorded as positive for any individual who reported ever having thought about suicide. Attempted suicide recorded as positive for any individual who reported that they had attempted suicide. Self-injurious behaviour referred to physical injury caused by impulsive behaviour while angry |
| Jamieson et al. (2011) [38] | Aboriginal young people: N = 336; age range <18 years. | 1987–1990 | Northern Territory (NT) | Longitudinal analysis of mental & dental health of birth cohort from Royal Darwin Hospital | Strong Souls questionnaire. Suicide risk rated on 10-point scale, 3 items (have you wished you were dead? Have you felt like hurting yourself? Have you felt like killing yourself? Prevalence = past few months’ |
| Lawlor & Kosky (1992) [45] | Total Suicide attempts: N = 12 Non-suicidal adolescents: N = 30 (age range= 11.11–17.10 years; Mage: 16.9, SD not reported) Aboriginal suicide attempts: N = 4 Non-Aboriginal suicide attempts: N = 8 | 1987–1989 | Western Australia (WA) | Analysed records of attempted suicide at Longmore Remand Centre | Longmore Remand Centre records of attempted suicide. Suicidal attempt defined as a suicide attempt which could have led to death if intervention had not been successful. Information on past suicide attempt and suicide ideation obtained from staff reports of “unusual occurrences” |
| Leckning et al. (2016) [35] | Hospital admissions for intentional self-harm and suicidal ideation N = 4495. (age-range: 10–24) Indigenous: N = 2367 admissions. Nonindigenous: 2127 admissions not reported: N = 2. No information reported for number of young person hospital admission | 2001–2013 | Northern Territory (NT) | Examination of hospital dataset for admissions related to intentional self-harm or ideation via ICD-10 codes | Analysis of hospital records. Intentional self-harm (ICD-10-AM codes X60-X84) and suicidal ideation (ICD-10-AM code R45.81) |
| Luke et al. (2013) [39] | Aboriginal (Koori) young people: N = 172; (age range 12–26; M age: 19 ± 4); (75 Male) No Non-Aboriginal group. | 1997–1998 | Victoria (VIC) | VAHS Young People’s Project. Data from health questionnaire and health check | Adapted Gatehouse Survey questionnaire. Suicide ideation: In the last two weeks, have you had thoughts that you would be better off dead in some way?; Suicide attempt: Have you ever tried to kill yourself?; (Y/N) |
| Pridmore & Fujiyama (2009) [30] | Total suicides reported in NT: N = 256 Age range: (<15–24) Indigenous: N = 130 Nonindigenous: N = 126 | 2001–2006 | Northern Territory (NT) | Examined National Coroner’s Information System | Coroner’s reports |
| Priest et al. (2011) [40] | Aboriginal young people: N = 345; (age range 16–20.5; Mage: 18.27 ± 1.06); (162 Males) | 2006–2008 | Northern Territory (NT) | Cross-sectional analysis of Aboriginal Birth Cohort Study | Strong Souls questionnaire. Suicide risk assessed via 3 items (details not reported). Binary coding (0 = present; 0 = not present) |
| Robinson et al. (2016) [31] | Youth suicides: N = 940 (age: <24 years) | 2010–2012 | National | Analysis of deaths classified as intentional self-harm; National Coronial Information System | National Coronial Information System |
| Rock & Hallmayer (2008) [36] | Suicide: 15–24 years Indigenous: N = 24 (23 males, 1 female) Nonindigenous: N = 305 (262 males, 43 females) Self-harm: 15–24 years Indigenous self-harm: N = 643 (265 males, 378 females) Nonindigenous: N = 5400; (2141 males, 3259 females) | 1984–1993 | Western Australia (WA) | Analysed data extract from Western Australian linked case registers of suicide and deliberate self-harm in Aboriginals, Australians & UK Migrants | Linked case registers: hospitalisations with an ICD-9-CM diagnosis of deliberate self-harm (E950–958). Suicide (E950–958) on Register of Births, Deaths, and Marriages |
| Rouen et al. (2019) [43] | Indigenous sample from 3 communities (N = 2262) Community A (n = 1063) Community B (n = 578) Community C (n = 621) | 2006–2011 | N. Queensland | Audit over 10–14 days re self-harm data from clinical files in community primary health care centres by registered nurse | ICD-10-CM: 2014. Classification of Diseases—Injury Classification System |
| Sawyer et al. (2010) [46] | Adolescents remanded into custody: N = 159 (age-range: 13–17 years) Aboriginal: N = 52 Non-Aboriginal: N= 107 | 2008–2009 | South Australia (SA) | Cross-sectional analysis of adolescents remanded to Magill Youth Centre | Youth Risk Behaviour Surveillance System Questionnaire. Experience of suicidal ideation, plan for suicide, attempted suicide, and/or initiated a suicide attempt which required medical treatment (Y/N) |
| Soole et al. (2014a) [32] | Child/adolescent deaths due to external causes: N = 469 (age range: 10–17 years); (308 male) Indigenous: N = 42; (age range: 10–17) Nonindigenous: N = 99; (age range: 10–17 years) | 2004–2012 | Queensland (QLD) | Analysis of Queensland Suicide Register (QSR) | Causes of death classified according to ICD-10 (self-harm X60-X84) |
| Soole et al. (2014b) [33] | Child deaths by suicide: N = 45; (age range: 10–14 years); (25 Male) Indigenous: N = 21; Mage: 13.05 (SD not reported); (12 Male) | 2000–2010 | Queensland (QLD) | Analysis of Queensland Suicide Register (QSR) | QSR data cross-referenced with National Coronial Information System |
| Stathis et al. (2012) [47] | Indigenous young people in custody: N = 47; (Mage 14.5 ± 1.3 years); (37 Male) No nonindigenous group | Not reported | Not specified | Cross-sectional assessment of admissions to MHATODS | Westerman Aboriginal Symptoms Checklist—Youth |
| Author | Suicide | Self-Harm | Suicide Ideation |
|---|---|---|---|
| Adams et al. (2014) [37] | Not Investigated | Fifty-nine percent of Aboriginal callers sought assistance for self–injury and/or self-harm concern. | Forty-six percent of Aboriginal callers reported suicide related concern and/or ideation |
| Armstrong et al. (2017) [42] | Not Investigated | 18–24 years: significantly higher prevalence rate of suicide attempts among Indigenous males (14.7%; n = 11/71) than non-Indigenous males (n = 116/1853; 6.3%) OR = 2.5, 95% CI = 1.2, 5.2 (p = 0.014) 14–17 years: prevalence of suicide attempts among Indigenous (3.4%) (n = 2/48) and non-Indigenous males (3.6%) (n = 43/1135) OR = 0.9, 95% CI = 0.2, 4.4 (p = 0.862), non–significant. | 18–24 years: no significant difference in prevalence of suicidal thoughts among Indigenous males (10.8%; n = 7/70) than non-Indigenous males (11.4%; n = 214/1850); OR = 0.9, 95% CI = 0.4, 2.4 (p = 0.877). 14–17 years: no significant difference in prevalence of suicidal thoughts among Indigenous males (9.1%; n = 11/98) and non-Indigenous (9.0%; n = 163/1943); OR = 1.0, 95% CI = 0.4, 2.3 (p = 0.994). |
| Burvill (1975) [34] | 15–24 years: a rate of 21 per 10,000 attempted suicides per male Aboriginals and a rate of 74 per 10,000 attempted suicides per female Aboriginals between 1971 and 1972 in Perth, West Australia. | Not Investigated | |
| Byard et al. (2011) [26] | Asphyxia reported as cause of death for 19.4% (n = 12) of Aboriginal suicides and 80.6% (n = 50) of suicides for non-Indigenous people. | Not Investigated | Not Investigated |
| Campbell et al. (2016) [27] | 48% (n = 71) of Indigenous deaths by suicide were reported among those aged <20 years. | Not Investigated | Not Investigated |
| Clayer & Czechowicz (1991) [28] | 32.6% (n = 15) of Aboriginal suicides occurred among 10–19 year olds compared to 8.4% (n = 110) of non-Aboriginal young people of the same age range. | Not Investigated | Not Investigated |
| De Leo et al. (2011) [29] | 5–14 year olds: Indigenous: 4.61 per 100,000 vs. non-Indigenous 0.48 per 100,000 (Risk Ratio 9.6, 95%CI = 1.24–74.3) 15–24 year olds: Indigenous: 57.50 per 100,000 vs. non-Indigenous 14.33 per 100,000 (Risk Ratio 4.0, 95% CI = 2.24–7.18). | Not Investigated | Not Investigated |
| Fasher et al. (1997) [44] | No significant difference in the proportion of Aboriginal (6.7%) and non-Aboriginal detainees (10.0%) reporting a history of attempted suicide (p = 0.594) | No significant difference in the proportion of Aboriginal (23.3%) and non-Aboriginal (27.1%) detainees reporting suicidal ideation (p = 0.691) | |
| Lawlor & Kosky (1992) [45] | Majority of suicide attempts were made by Non-Indigenous adolescents. 33.3% (n = 4/12) of suicide attempts were made by Aboriginal adolescents. | Not Investigated | |
| Leckning et al. (2016) [35] | Average percentage increase (2001–2013) in rates of hospital admission for suicidal behaviour in children aged 10–14 years was greater for Indigenous populations (23.5%) than non-Indigenous (12.8%) Average percentage increase (2001–2013) in rates of hospital admission for suicidal behaviour in young people aged 15–24 years was greater for Indigenous populations (11.0%) than non-Indigenous (6.6%) (p < 0.05). | ||
| Luke et al. (2013) [39] | 24.4% (n = 42) reports of past suicide attempt. Sig greater number of suicide attempts among 17–21 (31.6%) and 22–26 (30%) age range than <16 age range (4.7%) (p = 0.002) | 23.2% (n = 40) reported suicidal ideation in previous two weeks. Sig higher prevalence of suicidal ideation reported by Aboriginal youth aged 17–21 years than to <16 years (p = 0.008) | |
| Pridmore & Fujiyama (2009) [30] | Suicide rates for Aboriginal children (<15 years) was 1.5 per 100,000 compared to 0 per 100,000 for non-Indigenous. Young people (15–24 year olds) was 35.6 per 100,000 compared to 11.7 per 100,000 for non-Indigenous youth. | Not Investigated | Not Investigated |
| Priest et al. (2011) [40] | 25% (n = 87) of young Aboriginal people surveyed reported a risk of suicide. | Not Investigated | |
| Robinson et al. (2016) [31] | Suicides by Indigenous young people were significantly more likely to occur in a cluster (58.5%) than suicides by non-Indigenous people (13.1%) (p < 0.001) | Not Investigated | Not Investigated |
| Rock & Hallmayer (2008) [36] | Suicide rate for the 15–24 year olds Aboriginal population was 2.77 per 10,000 compared to 1.65 per 10,000 for non-Aboriginal Australians, and 2.31 per 10,000 for UK born migrants. | Self-harm rates were 74.23 per 10,000 for 15–24 year old Aboriginal population, compared to 29.18 per 10,000 for non-Aboriginal Australians, and 40.22 per 10,000 for UK born migrants. | Not Investigated |
| Rouen et al. (2019) [43] | Not Investigated | 15–24 years: significantly higher incidence rate of self-harm presentations (per 1000 population) among Indigenous young people in this age group, IR 30.1 (n = 71 presentations), CI = 23.1–37.1, relative to Indigenous young people aged 15 years and younger, IR 1.6 (n = 6 presentations) CI = 0.3–2.9 (p < 0.001). Rates of self-harm not significantly different between genders. | Not Investigated |
| Sawyer et al. (2010) [46] | No sig difference in prevalence of suicide behaviour between Aboriginal and non-Aboriginal adolescents on remand (p-values not reported). | Not Investigated | No significant difference in prevalence of suicidal ideation between Aboriginal and non-Aboriginal adolescents on remand (p-values not reported). |
| Soole et al. (2014a) [32] | Indigenous children and adolescents were sig more likely to die by suicide than by other external causes (OR = 14.47, 95% CI = 4.63–45.20 for children; OR = 2.89, 95% CI = 1.54–5.40 for adolescents) Indigenous children sig more likely to die by suicide aged 10–14 years than aged 15–17 years (OR = 2.68, 95% CI = 1.18–6.08). No sex difference in rate of suicide 0–14 year olds (male OR = 0.89; female OR = 1; 95% CI 0.27–2.88. | No sig difference in the percentage of indigenous children (25.8%, n = 8) and indigenous adolescents (30.5%, n = 32) reporting previous self-harm (OR = 0.79, 95% CI = 0.32–1.96) | No sig difference in percentage of indigenous children (29.4, n = 10) and indigenous adolescents (41.7%, n = 45) reporting previous suicidal ideation (OR = 58, 95% CI = 0.25–1.34) indigenous adolescents. |
| Soole et al. (2014b) [33] | Suicide rate for Indigenous children 10.63 per 100,000 (11.23 for males and 9.00 for females) compared to <1 per 100,000 (0.85 for males and 0.76 for females) (RR = 12.63, 95% CI = 6.77–23.51). | Not Investigated | Not Investigated |
| Stathis et al. (2012) [47] | Not Investigated | Not Investigated | 34% (n = 18) of Indigenous youth reported suicidal ideation. Indigenous females were sig more likely to report suicidal thoughts than males (p < 0.001; d = 0.78). |
| Author | Suicide | Self-Harm | Suicide Ideation |
|---|---|---|---|
| Jamieson et al. (2011) [38] | Not Investigated | Not Investigated | Young Aboriginal females reported sig higher levels of suicidal ideation than young Aboriginal males (β = 0.49, 95% CI = 0.25–0.74). Aboriginal youth experienced racial discrimination were at a significantly higher risk of suicide ideation than those who did not (β = 0.34, 95% CI = 0.08–0.60). No significant difference in level of suicidal ideation among Aboriginal youth living in regional and remote areas. No significant difference in level of suicide ideation among Aboriginal youth who were employed vs. unemployed. No significant difference in level of suicidal ideation among Aboriginal youth who use tobacco, marijuana, or alcohol and those who do not. |
| Luke et al. (2013) [39] | No significant difference between males and females in number of past suicide attempts (p = 0.123). Suicide attempt 2.5 times greater (95% CI = 0.45–4.46, p = 0.001) with an increase of 1 unit in emotional distress. Suicide attempt 3.2 times greater (95% CI = 1.75–6.05; p < 0.001) with an increase of one unit in social distress B (see footnote). Suicide attempt 2.5 times greater (95% CI = 1.38–4.62, p = 0.003) with an increase of one unit in social distress A (see footnote). No significant association between cultural connection and past suicide attempt (p = 0.370). Trend towards significant association between behavioural component and past suicide attempt (OR = 1.82, 95% CI = 0.99–3.37, p = 0.055). | Not Investigated | No significant difference between males and females in level of suicidal ideation (p = 0.872). Suicide ideation 7.6 times greater (95% CI = 3.41–16.95, p < 0.001) with an increase of 1 unit in emotional distress. Suicide ideation 2.0 times greater (95% CI = 1.15–3.65, p = 0.015) with an increase of one unit in social distress B. No significant association between cultural connection and suicidal ideation (p = 0.062). No significant associations between behavioural component and level of suicidal ideation (OR = 1.47, 95% CI = 0.78–2.78, p = 0.22) |
| Priest et al. (2011) [40] | Not Investigated | Not Investigated | Racial discrimination associated with significant increased risk of suicidal ideation (OR, 2.32 (95% CI, 1.25–4.00; p = 0.001)). |
| Soole et al. (2014b) [33] | Rates of suicide among indigenous children higher in remote (33.75 per 100,000) than regional (9.54 per 100,000) and metropolitan areas (0 per 100,000). Suicide rates higher among indigenous than non-Indigenous in remote and regional areas (non-Indigenous: remote = 0 per 100,000; regional = 1.4 per 100,000; RR = 6.81, 95% CI = 2.76–16.50, p < 0.001). In metropolitan areas, low rates among indigenous and non-Indigenous children (0.56 per 10,000). Significantly higher number of Indigenous children consumed alcohol prior to suicide compared to non-Indigenous children (33.3%, n = 7, 4.2%, n = 1, p = 0.014). No significant difference in physical health conditions between indigenous and non-Indigenous children who died by suicide (p = 0.267). | Not Investigated | Not Investigated |
| Zubrick et al. (2011) [41] | Aboriginal children whose birth mother had died were at a sig higher risk for parent-reported suicide attempts (OR = 7.0, 95% CI = 1.6–31.1 p value not reported). | No significant difference between Aboriginal children who lived with their birth mother or whose birth mother had died with regards to self-harm. | Aboriginal children whose birth mother had died were at a sig higher risk for parent-reported suicidal ideation (OR = 2.6, 95% CI = 1.2–5.7; p value not reported). |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dickson, J.M.; Cruise, K.; McCall, C.A.; Taylor, P.J. A Systematic Review of the Antecedents and Prevalence of Suicide, Self-Harm and Suicide Ideation in Australian Aboriginal and Torres Strait Islander Youth. Int. J. Environ. Res. Public Health 2019, 16, 3154. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16173154
Dickson JM, Cruise K, McCall CA, Taylor PJ. A Systematic Review of the Antecedents and Prevalence of Suicide, Self-Harm and Suicide Ideation in Australian Aboriginal and Torres Strait Islander Youth. International Journal of Environmental Research and Public Health. 2019; 16(17):3154. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16173154
Chicago/Turabian StyleDickson, Joanne M., Kate Cruise, Clare A. McCall, and Peter J. Taylor. 2019. "A Systematic Review of the Antecedents and Prevalence of Suicide, Self-Harm and Suicide Ideation in Australian Aboriginal and Torres Strait Islander Youth" International Journal of Environmental Research and Public Health 16, no. 17: 3154. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16173154