A Systematic Review and Meta-Analysis of Nature-Based Mindfulness: Effects of Moving Mindfulness Training into an Outdoor Natural Setting

 , , ,
, , ,
Abstract
:1. Introduction
1.1. Mindfulness
1.2. Natural Environments and Exposure to Nature
1.3. Possible Interactions between Mindfulness and Exposure to Nature
1.4. Aims
2. Materials and Methods
2.1. Selection Criteria
2.1.1. Population
2.1.2. Intervention
2.1.3. Comparators
2.1.4. Outcomes
2.1.5. Study Design
2.2. Search Strategy
2.3. Data Extraction
2.4. Quality Assessment
2.5. Analytical Overview
3. Results
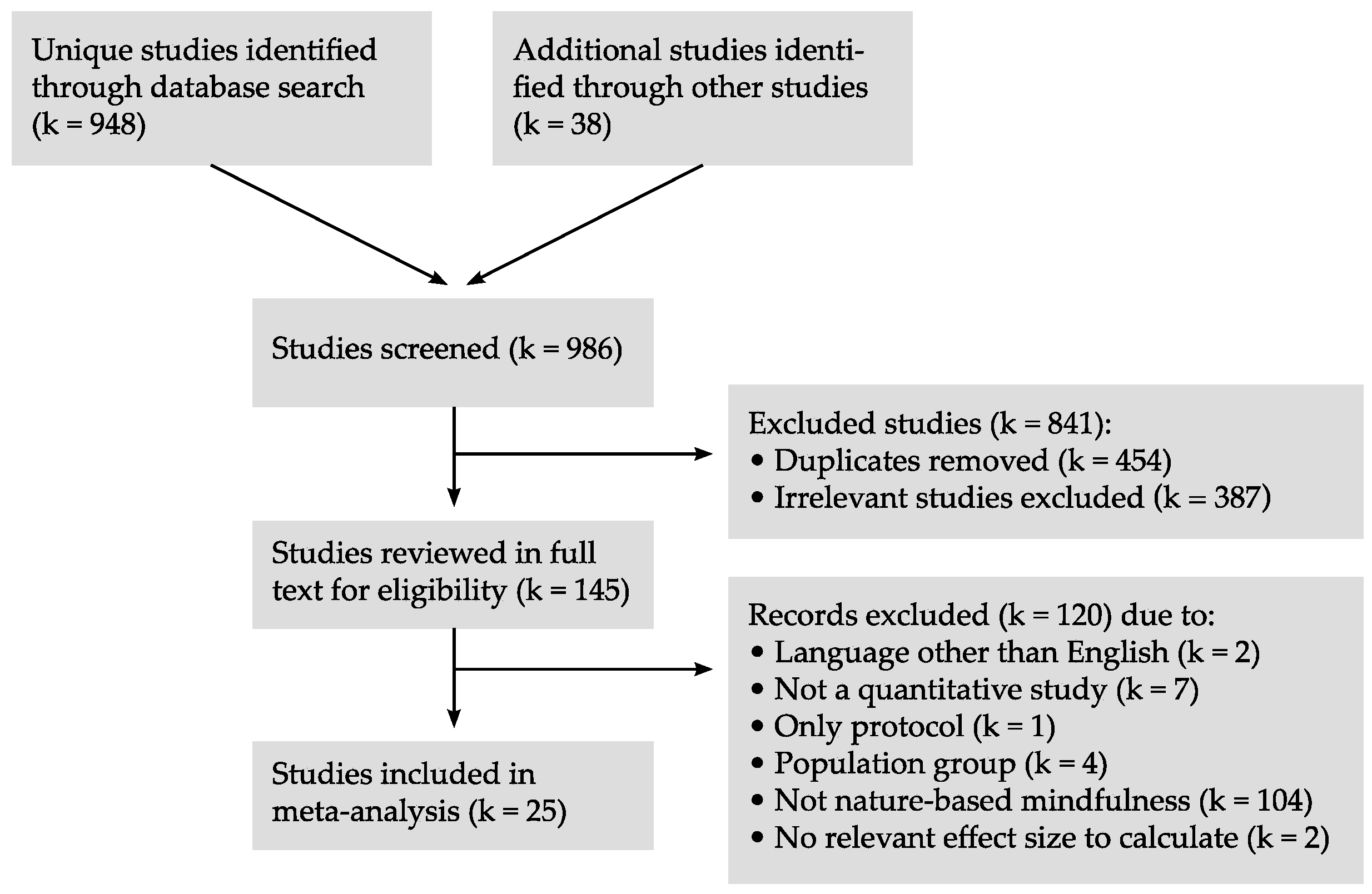
3.1. Search Results
3.2. Characteristics of Studies

{kind=link}
| Study Author, Year, Country | Population N = Included (Completed/Follow-up), Age = Range (Mean), Gender, Ethnicity, Target Group | Intervention Duration, Content | Comparators Duration, Content | Outcomes Measurements, Tools | Time Intervention, Timings of Data Collection | Setting Location of Study Group | EPHPP Quality |
|---|---|---|---|---|---|---|---|
| Comparator: interventions incl. mindfulness, but without nature contact | |||||||
| Ballew & Omoto (2018) [48] USA | N = 100 Age = 18–24 (19.3) % female = 55 % Whites = 21 Study group: Students, no diagnosis | 15 min in natural settings. Instructions to look at surrounding features and pay attention to all details, colors, and textures, to use all senses to take everything in. Note-taking. | Same program as study group, human-built outdoor environment. | Absorption, awe, happiness, joy, contentment (rating sentences) | T1: Survey just after 15-min. intervention | Arboretum, sitting on a bench, view of trees, creek, bamboo, etc. | 3 |
| Shin et al. (2012) [49] Korea | N = 69 (68) Age = 20.4 (±1.5) % female = 100 % Whites = N/A Study group: Students, no diagnosis | 35 min. walk, 10 min. rest, 35 min. walk, 10 min. rest. Mindful walking with focus on breath and sensations. | Same program as study group, indoor setting. | Anxiety (STAI), self-esteem (RSE), happiness (HI-K) | T1: Before intervention T2: Just after 90-min. intervention | Undisturbed rocky area with old-growth broad-leaved evergreen trees | 3 |
| Passmore & Holder [50] (2017) Canada | N = 395 (364) Age = 20.09 % female = 67 % Whites = N/A Study group: Students, no diagnosis | 2 weeks. Instructions to be mindful of emotions evoked by natural objects/scenes in everyday life; to describe strong emotions and take pictures of the nature that evoked them. | Same intervention as study group, human built environment. Passive controls: Continue regular routines. | Affect (PANAS), elevation (EES), meaning (SMS), connectedness (GSC), prosocial orientation (PSO), connectedness to nature (CNS), engaging with beauty (EWB) | T1: Just before intervention (PANAS only) T2: Just after 2-week intervention (all measurements) | Everyday environment of university students | 3 |
| Kim et al. (2009) [51] Korea | N = 73 (63) Age = 46.2 % female = 85.7 % Whites = N/A Study group: Major depressive disorder | 4 weeks, 3 hours weekly, for CBT, positive psychology tools, and mindfulness meditation on breath, wind, forest, and sounds (insight meditation). | Same program as study group, indoor setting. Meditation focus on breath and indoor or window objects. Passive control: TAU. | Depression (BDI, HRSD, MADRS), quality of life (SF-36), stress (HRV, cortisol) | T1: Just before treatment, all measurements T2: T1 + 1 week, depression questionnaires T3: T1 + 2 weeks, depression questionnaires T4: After 3 weeks of treatment, all measurements | 44-ha arboretum, 2035 species | 2 |
| Willert et al. (2014) [52] Denmark | N = 93 (66/49) Age = 25–59 (45.0) % female = 82.8 % Whites = N/A Study group: Stressed students | 16 weeks, 5 days a week, 9 a.m. to afternoon. Groups of max. 12. All-day exercises from meditation training programs (MBCT and Five Tibetans), horticultural activities, nature walks, stress management, job counseling, individual psychotherapy sessions. | Same program as study group, indoor setting. | Stress (PSS-10), sleep (BNSQ), mindfulness (FFMQ - 3 dimensions), self-efficacy (COPSOQ-II), Outcome Rating Scale, work ability (WAI) | T1: Just before treatment T2: Just after 3 months of treatment T3: T2 + 3 months | Garden incl. greenhouse, near forest and beach | 2 |
| Vujcic et al. (2017) [53] Serbia | N = 30 Age = 25–65 (45.35) % female = 70 % Whites = N/A Study group: Depressed, anxious | 4 weeks, 3 one-hour sessions per week of horticultural therapy, art therapy, and relaxation/meditation sessions. All main activities relate to work with living plants. | Parallel indoor activities with study group, incl. occupational, art, and conventional therapies. | Depression and anxiety (DASS21) | T1: Just before intervention T2: Just after 4 weeks’ intervention | Botanical garden incl. open space, greenhouse, Japanese garden, fountain | 3 |
| Lymeus (2018) [54] Sweden | Study 1: N = 89 Age = (23) % female = 64 % Whites = N/A Study 2: N = 51 Age = (23) % female = 72.5 % Whites = N/A Study groups: Stressed | 5 weeks, 1 weekly 90-min. session. Manual-based meditation training program (REST), each session beginning and ending with 15–20 min. guided open monitoring meditation (no specific tradition). Exercises and themes. Homework: 15 min. meditation most days. | Classroom setting. Same schedule as study group. Beginning and end of sessions: Focused attention meditation (no specific tradition), exercises and themes. | Attention (LDST; TMT study 2), affect (SCAS) | Study 1: T1: Before/after session 1 T2: Before/after session 3 T3: Before/after session 5 Study 2: T1: Enrollment T2: Before/after initial 20-min. meditation in session 1 T3: Before/after initial 20-min. meditation in session 3 T4: Before/after initial 20-min. meditation in session 5 | Botanical garden incl. tropical greenhouse, water bodies, orangery | 3 |
| Comparator: Non-active control conditions (see also Kim 2009 and Passmore 2017 above) | |||||||
| Han (2016) [55] Korea | N = 61 Age = 25–49 (39.75) % female = 57.4 % Whites = N/A Study group: Chronic pain | 24-hour residential intervention (noon to noon). In forest: Walking, therapeutic activities, physical exercises, mindfulness meditation. Indoor music therapy, psycho-education on stress and pain. | Usual weekend routines, except visiting natural environment or heavy loads of work. | Stress (HRV, HR) natural killer cells (NK), pain (VAS), depression (BDI), health-related quality of life (EQ-VAS) | T1: Just before treatment T2: T1 + 1 day just after 24 hours’ treatment | Foot of a mountain: forest valley, “spectacular” views | 3 |
| Won (2012) [56] Korea | N = 92 Age = 45.26 % female = 8.7 % Whites = N/A Study group: Detoxified chronic alcoholics | 9 days: 3 days actively interacting with nature, 3 days challenging activities in nature, 3 days activities for introspection (nature meditation, counseling in nature etc.). | Inpatients, no specific treatment described. | Depression (BDI) | T1: Just before treatment T2: T1 + 9 days just after treatment | 2140-ha recreational forest | 2 |
| Warber et al. (2011) [57] USA | N = 58 (47/41) Age = 25–75 (59.3) % female = 40.4 % Whites = 85.1 Study group: Coronary syndrome | 4-day residential program. Study group 1 (MFTE): Meditation, guided imagination, journaling, drawing, nature activities, nature imagination. Study group 2 (LCP): Nutrition, physical exercise, stress management based on mindfulness and whole-person approach. Both groups: Telephone coaching biweekly for 3 months. | No treatment. | Depression (BDI, BSI), stress (PSS), hope (SHS), gratitude (SG), quality of life (SF-36), spirituality (ISWBS), personal transformation (TCQ), physical activity (PPAQ), stress (HR, BP, BMI, lipid levels, lipid particle size, high sensitivity C-reactive protein, biomarkers IL-6 and IL-10) | T1: Just before treatment T2: Just after 4 days’ treatment T3: T2 + 3 months T4: T2 + 6 months Biophysical measurements only at T1 and T2 | “Beautiful” rural settings | 3 |
| Sung et al. (2012) [58] Korea | N = 56 Age = 66.0 % female = 60.7 % Whites = N/A Study group: Hypertension stage 1 | 3-day forest therapy program: Relationship-building, stress and health management, mindfulness and gratitude meditation in forest. | Written material on hypertension management. | Stress (BP), salivary cortisol level, quality of life (QoL, 5 dimensions) | T1: Just before intervention, all measurements T2: Just after 3-day intervention, all measurements Follow-up: Self- monitoring BP, 8 weeks | Recreational forest in mountain region | 2 |
| Passmore (2014) [59] Canada | N = 86 (84) Age = 18–45 (20.96) % female = 86.9 % Whites = N/A Study group: Students, no diagnosis | 14 days. Written instructions to immerse themselves in nature activities whenever possible in everyday lives. Keeping logbook of nature activities for each day. | Solving anagram puzzles whenever possible in their everyday lives. | Affect (PANAS), elevation (EES), meaning (SMS), motivation (SCM) | T1: Just before intervention T2: T1 + 14 days just after intervention | Everyday environment of Canadian students | 1 |
| Studies with no comparators relevant for this review | |||||||
| Jung (2015) [60] Korea | N = 19 Age = 29.4 % female = 100 % Whites = N/A Study group: No diagnosis | 2 days, noon day 1 to noon day 3. Indoors: lectures on coping with stress, counseling, cognitive therapy, music therapy. In forest: 5 hours’ meditation, walking, exercises. | Stress (HR, HRV, cortisol), natural killer cell activity (NK), burnout (MBI-GS), stress (WSRI), recovery (REQ) | T1: Just before intervention T2: T1 + 2 days just after intervention T3: T2 + 14 days All measures at T1 and T2, except MBI-GS second measure at T3 | 2140-ha recreational forest | 3 | |
| Yu et al. (2017) [61] Taiwan | N = 128 Age = 45–86 (60) % female = 65.6 % Whites = N/A Study group: 46% chronic diseases (e.g., diabetes) | 2 hours, 2.5 km sensory forest walk incl. guided stimulation of senses (visual, auditory, olfactory, tactile). Groups of 6–12 participants. | Mood (POMS-SF), anxiety (STAI), stress (pulse rate, BP, HR, HRV) | T1: Just before intervention T2: Just after 2-hour intervention | Sensory forest, in valley surrounded by mountains on three sides (part of Xitou Nature Education Area in Japan) | 3 | |
| Korpela et al. (2017) [62] Finland, Luxembourg, Sweden | N = 283 Age = 13–82 (47.2) % female = 74 % Whites = N/A Study group: No diagnosis | Well-being trails in the 3 countries, 4.4–6.6 km, containing the same 9 signposts with tasks: Self-monitoring (first and last), relaxation, letting oneself be fascinated, observing nature and one’s own body and mood. | Restorative change (4 items), mood (1 item), nature connectedness (3 items) | T1: At first signpost on the trail T2: At last signpost on the trail | Hiking tracks incl. forests, lakesides, fields, cultural landscapes | 3 | |
| Yang (2018) [63] USA | N = 29 (27/26) Age = 66–89 (73.2) % female = 83 % Whites = 79 Study group: No diagnosis | 4 weeks, 8 sessions of 30 min. individual mindful walking. Before walking, guidance either to become familiar with the environment, to focus on breath or movement, or to scan through the body. | Affect (PROMIS), mindfulness (SMS) | T1: Just before treatment T2: Just after 30 min. mindful walking | Flat designated route in arboretum | 2 | |
| Corazon et al. (2018) [64] & Stigsdotter (2018) [65] Denmark | N = 43 (42/29) Age = 47.9 % female = 81.6 % Whites = N/A Study group: Severely stressed | 10-week nature-based therapy, 3 times, 3 hours per week. Activities individually and in groups: Exercises in accordance with MBSR and related to nature experiences, such as mindful walking in natural setting. Gardening and relaxation/reflection time. Individual therapeutic sessions (CBT) and support for return to work. | Sick leave and contact with GP (from national database), well-being (PGWBI), burnout (SMBQ) | T0-T1: 1-year time span T1: Treatment start T2: Just after 10 weeks’ treatment T3: T2 + 3 months T4: T2 + 6 months T5: T2 + 12 months | 1.4-ha wild forest garden located in larger arboretum | 2 | |
| Sahlin et al. (2014) [66] Sweden | N = 44 (33) Age = N/A % female = 100 % Whites = N/A Study group: Stressed | 12 weeks, 3 hours weekly. 3 intervention groups Activities: Walks, relaxation, mindfulness, therapeutic painting, group therapy, information about stress and health, garden and nature activities. | Burnout (SMBQ), work ability I (WAI, adjusted), stress (scale tools created for this study), sleep (KSQ) | T1: Just after first session T2: Just after 12-week program T3: T2 + 6 months T4: T2 + 12 months | 225-ha wild nature, incl. forest, ponds, moorland, hills; wooden house, greenhouse | 3 | |
| Nacau et al. (2013) [67] Japan | N = 22 Age = 58.2 % female = 81.8 % Whites = N/A Study group: Cancer, after treatment | 12 weeks, once per week, 6 hours. 40 min. walks, 60 min. horticultural therapy, 90 min. indoor yoga and meditation (1 session), 60 min. supportive group therapy (5 sessions). Homework: yoga (video). | Well-being (FACIT) incl. physical, cancer fatigue (CFS), quality of life (SF-36), mood (POMS-SF), anxiety (STAI), natural killer cell activity (NK) | T1: Just before treatment T2: Just after 12 weeks’ treatment | Park incl. forest, streams, lawns, gardens; yoga and meditation indoors in the park | 3 | |
| Combs et al. (2016) [68] USA | N = 704 (659) Age = 16 % female = 32 % Whites = 85 Study group: behavior/ substance/ mood issues | 90-day program. Nomadic hiking and/or expeditions and tasks associated with outdoor living. Therapeutic tools: The wilderness itself, CBT, choice therapy, family systems, mindfulness techniques, diet, physical exercise. Individual/ group therapy sessions twice a week. | Psychological and behavioral symptoms and social functioning (Y-OQ_SR) | T1: At intake T2: T1 + 3 weeks T3: T1 + 5 weeks T4: At discharge T5: T4 + 6 months T6: T4 + 18 months. | Wilderness in undeveloped areas | 3 | |
| Russell (2016) [69] Canada | N = 43 (32) Age = 18–24 (22.9) % female = 0 % Whites = N/A Study group: Substance abuse | 90-day, 10-bed outdoor behavioral healthcare program (Shunda Creek), incl. weekly 1–5-day adventure trips integrating mindfulness-based experience (MBE) with psychotherapy. | Subjective discomfort, interpersonal relations, social roles (OQ-45.2), mindfulness (FFMQ) | T1: At intake T2: At discharge (average T1 + 93.7 days) | Wild nature, incl. mountains | 3 | |
| Russell et al. (2017) [70] USA | N = 168 Age = 21.5 % female = 0 % Whites = 40 Study group: Substance abuse | 90-day outdoor behavioral healthcare program (Shunda Creek): Weekly 1–5-day adventure trips integrating MBE with psychotherapy. | Helpfulness and mindfulness (subscales of OQ-45.2), adventure therapy experience (ATES) | T1: At admission T2–T13: Every second week until discharge | Wild nature, incl. mountains | 3 | |
| Russell (2018) [71] Canada | N = 57 (46) Age = 12–17 (16.6) % female = 43.9 % Whites = 57.9 Study group: 74% diagnoses, ADHD/substance use | 8-week, 15-bed program: family therapy, daily individual/group therapy, educational programming. Base camp model: Adventure therapy and development of mindfulness skills. | Emotional and behavioral symptoms (Y-OQ SR 2.0), mindfulness (CAMM) | T1: Just before treatment T2: Just after 8 weeks’ treatment | Wild nature, incl. mountains | 3 | |
| Chapman et al. (2018) [72] Canada | N = 177 Age = 18–24 (21.5) % female = 0 % Whites = 42.1 Study group: Substance use | 90-day outdoor behavioral healthcare program (Shunda Creek): Weekly 1–5-day adventure trips integrating MBE with psychotherapy. | Subjective discomfort, interpersonal relations, social roles (OQ-45.2) | T1: At intake T2: At discharge (average T1 + 79.6 days) | Wild nature, incl. mountains | 3 | |
| Unsworth et al. (2016) [73] study 2 USA | N = 39 Age = 21 % female = 64.1 % Whites = N/A Study group: No diagnosis | 3 days’ Aztec adventure camp in nature, incl. 15 min. formal daily morning meditation, and encouragement to continue mindfulness practice throughout the day. | Self-nature interconnectedness, nature in self (INS), mindfulness (FMI) | T1: Just before treatment T2: Just after 3 days’ treatment | Wild nature | 3 | |
3.3. Intervention Characteristics
- Short single-instruction intervention studies (k = 7) aimed at healthy participants, who were guided either to be mindful on their own while sitting or walking, or to be more extensively mindful in their everyday lives.
- Weekly meetings (once or more per week) targeting stressed, anxious, or depressed people (k = 6), mostly with gardening activities and psychotherapy. One study stood out in this format as only containing meditation training.
- Residential interventions (k = 11), of which five were wilderness therapy of several weeks’ duration. Participants in these studies were young people, mostly males diagnosed with substance use disorders. The other six residential interventions were shorter and in diverse settings.
3.4. Pooled Effect Sizes and Between-Study Differences
3.5. Publication Bias
4. Discussion
4.1. Implications for Research and Practice
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lymeus, F.; Lundgren, T.; Hartig, T. Attentional effort of beginning mindfulness training is offset with practice directed toward images of natural scenery. Environ. Behav. 2017, 49, 536–559. [Google Scholar] [CrossRef]
- Ambrose-Oji, B. Mindfulness Practice in Woods and Forests: An Evidence Review. In Research Report for The Mersey Forest, Forest Research; Alice Holt Lodge Farnham: Surrey, UK, 2013. [Google Scholar]
- Schutte, N.S.; Malouff, J.M. Mindfulness and connectedness to nature: A meta-analytic investigation. Pers. Individ. Differ. 2018, 127, 10–14. [Google Scholar] [CrossRef]
- Kaplan, S. Meditation, Restoration, and the Management of Mental Fatigue. Environ. Behav. 2001, 33, 480–506. [Google Scholar] [CrossRef] [Green Version]
- Bishop, S.; Lau, M.; Shapiro, S.; Carlson, L.; Anderson, N.; Carmody, J.; Devins, G. Mindfulness: A Proposed Operational Definition. Clin. Psychol. Sci. Pract. 2004, 11, 230–241. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. Full Catastrophe Living: Using the Wisdom of Your Body and Mind to Face Stress, Pain, and Illness; rev. ed.; Bantam Books: New York, NY, USA, 2013. [Google Scholar]
- Dahl, C.J.; Lutz, A.; Davidson, R.J. Reconstructing and deconstructing the self: Cognitive mechanisms in meditation practice. Trends Cogn. Sci. 2015, 19, 515–523. [Google Scholar] [CrossRef] [PubMed]
- Johnson, S.; Gur, R.M.; David, Z.; Currier, E. One-session mindfulness meditation: A randomized controlled study of effects on cognition and mood. Mindfulness 2015, 6, 88–98. [Google Scholar] [CrossRef]
- Piet, J.; Hougaard, E. The effect of mindfulness-based cognitive therapy for prevention of relapse in recurrent major depressive disorder: A systematic review and meta-analysis. Clin. Psychol. Rev. 2011, 31, 1032–1040. [Google Scholar] [CrossRef]
- Sedlmeier, P.; Eberth, J.; Schwarz, M.; Zimmermann, D.; Haarig, F.; Jaeger, S.; Kunze, S. The psychological effects of meditation: A meta-analysis. Psychol. Bull. 2012, 138, 1139–1171. [Google Scholar] [CrossRef]
- Chiesa, A.; Serretti, A. Mindfulness-Based Interventions for Chronic Pain: A Systematic Review of the Evidence. J. Altern. Complement. Med. 2011, 17, 83–93. [Google Scholar] [CrossRef]
- Black, D.S.; Slavich, G.M. Mindfulness meditation and the immune system: A systematic review of randomized controlled trials. Ann. N. Y. Acad. Sci. 2016, 1373, 13–24. [Google Scholar] [CrossRef]
- Beauchemin, J.; Hutchins, T.L.; Patterson, F. Mindfulness meditation may lessen anxiety, promote social skills, and improve academic performance among adolescents with learning disabilities. Complement. Health Pract. Rev. 2008, 13, 34–45. [Google Scholar] [CrossRef]
- De Vibe, M. Mindfulness based stress reduction (MBSR) for improving health, quality of life, and social functioning in adults. Campbell Syst. Rev. 2012, 8, 1–127. [Google Scholar] [CrossRef]
- Gu, J.; Strauss, C.; Bond, R.; Cavanagh, K. How do mindfulness-based cognitive therapy and mindfulness-based stress reduction improve mental health and wellbeing? A systematic review and meta-analysis of mediation studies. Clin. Psychol. Rev. 2015, 37, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Bratman, G.N.; Hamilton, J.P.; Daily, G.C. The impacts of nature experience on human cognitive function and mental health. Ann. N. Y. Acad. Sci. 2012, 1249, 118–136. [Google Scholar] [CrossRef] [PubMed]
- Mausner, C. A Kaleidoscope model: Defining natural environments. J. Environ. Psychol. 1996, 16, 335–348. [Google Scholar]
- Hartig, T.; Mitchell, R.; De Vries, S.; Frumkin, H. Nature and Health. Annu. Rev. Public Health 2014, 35, 207–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mcmahan, E.A.; Estes, D. The effect of contact with natural environments on positive and negative affect: A meta-analysis. J. Posit. Psychol. 2015, 10, 507–519. [Google Scholar] [CrossRef]
- Beyer, K.M.M.; Kaltenbach, A.; Szabo, A.; Bogar, S.; Nieto, F.J.; Malecki, K.M. Exposure to neighborhood green space and mental health: Evidence from the survey of the health of Wisconsin. Int. J. Environ. Res. Public Health 2014, 11, 3453–3472. [Google Scholar] [CrossRef]
- Kuo, M. How might contact with nature promote human health? Promising mechanisms and a possible central pathway. Front. Psychol. 2015, 6, 1093. [Google Scholar] [CrossRef]
- De Vries, S.; Van Dillen, S.M.; Groenewegen, P.P.; Spreeuwenberg, P. Streetscape greenery and health: Stress, social cohesion and physical activity as mediators. Soc. Sci. Med. 2013, 94, 26–33. [Google Scholar] [CrossRef]
- Frumkin, H.; Bratman, G.N.; Breslow, S.J.; Cochran, B.; Kahn, P.H., Jr.; Lawler, J.J.; Levin, P.S.; Tandon, P.S.; Varanasi, U.; Wolf, K.L.; et al. Nature Contact and Human Health: A Research Agenda. Environ. Health Perspect. 2017, 125, 075001. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Kawada, T. Effect of forest environments on human natural killer (NK) activity. Int. J. Immunopathol. Pharmacol. 2011, 24, 39S–44S. [Google Scholar] [PubMed]
- Hansen, M.M.; Jones, R.; Tocchini, K. Shinrin-Yoku (Forest Bathing) and Nature Therapy: A State-of-the-Art Review. Int. J. Environ. Res. Public Health 2017, 14, 851. [Google Scholar] [CrossRef] [PubMed]
- Oh, B.; Lee, K.J.; Zaslawski, C.; Yeung, A.; Rosenthal, D.; Larkey, L.; Back, M. Health and well-being benefits of spending time in forests: Systematic review. Environ. Health Prev. Med. 2017, 22, 71. [Google Scholar] [CrossRef] [PubMed]
- Bettmann, J.E.; Gillis, H.L.; Speelman, E.A.; Parry, K.J.; Case, J.M. A Meta-analysis of Wilderness Therapy Outcomes for Private Pay Clients. J. Child Fam. Stud. 2016, 25, 2659–2673. [Google Scholar] [CrossRef]
- Bowen, D.J.; Neill, J.T.; Crisp, S.J. Wilderness adventure therapy effects on the mental health of youth participants. Eval. Program Plan. 2016, 58, 49–59. [Google Scholar] [CrossRef] [Green Version]
- Soga, M.; Gaston, K.J.; Yamaura, Y. Gardening is beneficial for health: A meta-analysis. Prev. Med. Rep. 2017, 5, 92–99. [Google Scholar] [CrossRef]
- Shapiro, S.L.; Carlson, L.E.; Astin, J.A.; Freedmanm, B. Mechanisms of mindfulness. J. Clin. Psychol. 2006, 62, 373–386. [Google Scholar] [CrossRef]
- Li, D.; Sullivan, W.C. Impact of views to school landscapes on recovery from stress and mental fatigue. Landsc. Urban Plan. 2016, 148, 149–158. [Google Scholar] [CrossRef] [Green Version]
- Evensen, K.H.; Raanaas, R.K.; Hagerhall, C.M.; Johansson, M.; Patil, G.G. Restorative elements at the computer workstation: A comparison of live plants and inanimate objects with and without window view. Environ. Behav. 2015, 47, 288–303. [Google Scholar] [CrossRef]
- Stevenson, M.P.; Schilhab, T.; Bentsen, P. Attention Restoration Theory II: A systematic review to clarify attention processes affected by exposure to natural environments. J. Toxicol. Environ. Health Part B 2018, 21, 227–268. [Google Scholar]
- Kaplan, S.; Kaplan, R. The Experience of Nature: A Psychological Perspective; Cambridge University Press: New York, NY, USA, 1989. [Google Scholar]
- Kaplan, S. The restorative benefits of nature: Towards an integrative framework. J. Environ. Health 1995, 16, 169–182. [Google Scholar] [CrossRef]
- Jiang, B.; Schmillen, R.; Sullivan, W.C. How to waste a break: Using portable electronic devices substantially counteracts attention enhancement effects of green spaces. Environ. Behav. 2018. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; A Stewart, L. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [PubMed]
- Mennin, D.S.; Ellard, K.K.; Fresco, D.M.; Gross, J.J. United We Stand: Emphasizing Commonalities Across Cognitive-Behavioral Therapies. Behav. Ther. 2013, 44, 234–248. [Google Scholar] [Green Version]
- Mennin, D.S.; Fresco, D.M. Emotion regulation therapy. In Handbook of Emotion Regulation, 2nd ed.; Guilford Press: New York, NY, USA, 2014; pp. 469–490. [Google Scholar]
- Thomas, B.H.; Ciliska, D.; Dobbins, M.; Micucci, S. A process for systematically reviewing the literature: Providing the research evidence for public health nursing interventions. Worldviews Evid. Based Nurs. 2004, 1, 176–184. [Google Scholar] [CrossRef] [PubMed]
- Hedges, L.V.; Olkin, I. Statistical Methods for Meta-Analysis; Academic Press: London, UK, 1985. [Google Scholar]
- Cohen, J. Applied Power Analysis for the Behavioral Science; Lawrence Erlbaum: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Hedges, L.V.; Pigott, T.D. The power of statistical tests in meta-analysis. Psychol. Methods 2001, 6, 203–217. [Google Scholar]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [Green Version]
- Duval, S.; Tweedie, R. Trim and Fill: A Simple Funnel-Plot-Based Method of Testing and Adjusting for Publication Bias in Meta-Analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef]
- Rosenthal, R. The file drawer problem and tolerance for null results. Psychol. Bull. 1979, 86, 638–641. [Google Scholar] [CrossRef]
- Ballew, M.T.; Omoto, A.M. Absorption: How Nature Experiences Promote Awe and Other Positive Emotions. Ecopsychology 2018, 10, 26–35. [Google Scholar] [Green Version]
- Shin, Y.; Kim, D.; Jung-Choi, K.; Son, Y.; Koo, J.; Min, J.; Chae, J. Differences of psychological effects between meditative and athletic walking in a forest and gymnasium. Scand. J. For. Res. 2012, 28, 1–9. [Google Scholar]
- Passmore, H.; Holder, M. Noticing nature: Individual and social benefits of a two-week intervention. J. Posit. Psychol. 2017, 12, 537–546. [Google Scholar]
- Kim, W.; Lim, S.; Chung, E.; Woo, J. The Effect of Cognitive Behavior Therapy-Based Psychotherapy Applied in a Forest Environment an Physiological Changes and Remission of Major Depressive Disorder. Psychiatry Investig. 2009, 6, 245–254. [Google Scholar] [PubMed]
- Willert, M.V.; Wieclaw, J.; Thulstrup, A.M. Rehabilitation of individuals on long-term sick leave due to sustained stress-related symptoms: A comparative follow-up study. Scand. J. Public Health 2014, 42, 719–727. [Google Scholar] [CrossRef] [PubMed]
- Vujcic, M.; Tomicevic-Dubljevic, J.; Grbic, M.; Lecic-Tosevski, D.; Vukovic, O.; Toskovic, O. Nature based solution for improving mental health and well-being in urban areas. Environ. Res. 2017, 158, 385–392. [Google Scholar] [PubMed]
- Lymeus, F.; Lindberg, P.; Hartig, T. Building mindfulness bottom-up: Meditation in natural settings supports open monitoring and attention restoration. Conscious. Cogn. 2018, 59, 40–56. [Google Scholar] [PubMed]
- Han, J.-W.; Choi, H.; Jeon, Y.-H.; Yoon, C.-H.; Woo, J.-M.; Kim, W. The Effects of Forest Therapy on Coping with Chronic Widespread Pain: Physiological and Psychological Differences between Participants in a Forest Therapy Program and a Control Group. Int. J. Environ. Res. Public Health 2016, 13, 255. [Google Scholar] [Green Version]
- Won, S.; Chang, S.; Poung, Y. The influence of forest therapy camp on depression in alcoholics. Environ. Health Prev. Med. 2012, 17, 73–76. [Google Scholar]
- Warber, S.L.; Ingerman, S.; Moura, V.L.; Wunder, J.; Northrop, A.; Gillespie, B.W.; Durda, K.; Smith, K.; Rhodes, K.S.; Rubenfire, M. Healing the Heart: A Randomized Pilot Study of a Spiritual Retreat for Depression in Acute Coronary Syndrome Patients. Explore 2011, 7, 222–233. [Google Scholar] [CrossRef] [PubMed]
- Sung, J.; Woo, J.; Kim, W.; Lim, S.; Chung, E. The Effect of Cognitive Behavior Therapy-Based “Forest Therapy” Program on Blood Pressure, Salivary Cortisol Level, and Quality of Life in Elderly Hypertensive Patients. Clin. Exp. Hypertens. 2012, 34, 1–7. [Google Scholar] [PubMed]
- Passmore, H.; Howell, A. Nature Involvement Increases Hedonic and Eudaimonic Well-Being: A Two-Week Experimental Study. Ecopsychology 2014, 6, 148–154. [Google Scholar]
- Jung, W.H.; Woo, J.-M.; Ryu, J.S. Effect of a forest therapy program and the forest environment on female workers’ stress. Urban For. Urban Green. 2015, 14, 274–281. [Google Scholar]
- Yu, C.-P.; Lin, C.-M.; Tsai, M.-J.; Tsai, Y.-C.; Chen, C.-Y. Effects of Short Forest Bathing Program on Autonomic Nervous System Activity and Mood States in Middle-Aged and Elderly Individuals. Int. J. Environ. Res. Public Health 2017, 14, 897. [Google Scholar] [CrossRef] [PubMed]
- Korpela, K.; Savonen, E.-M.; Anttila, S.; Pasanen, T.; Ratcliffe, E. Enhancing wellbeing with psychological tasks along forest trails. Urban For. Urban Green. 2017, 26, 25–30. [Google Scholar] [CrossRef] [Green Version]
- Yang, C.-H.; Conroy, D.E. Feasibility of an Outdoor Mindful Walking Program for Reducing Negative Affect in Older Adults. J. Aging Phys. Act. 2019, 27, 18–27. [Google Scholar] [CrossRef] [PubMed]
- Corazon, S.S.; Nyed, P.K.; Sidenius, U.; Poulsen, D.V.; Stigsdotter, U.K. A Long-Term Follow-Up of the Efficacy of Nature-Based Therapy for Adults Suffering from Stress-Related Illnesses on Levels of Healthcare Consumption and Sick-Leave Absence: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2018, 15, 137. [Google Scholar] [CrossRef] [PubMed]
- Stigsdotter, U.K.; Corazon, S.S.; Sidenius, U.; Nyed, P.K.; Larsen, H.B.; Fjorback, L.O. Efficacy of nature-based therapy for individuals with stress-related illnesses: Randomised controlled trial. Br. J. Psychiatry 2018, 213, 404–411. [Google Scholar]
- Sahlin, E.; Ahlborg, G.; Matuszczyk, J.V.; Grahn, P. Nature-Based Stress Management Course for Individuals at Risk of Adverse Health Effects from Work-Related Stress—Effects on Stress Related Symptoms, Workability and Sick Leave. Int. J. Environ. Res. Public Health 2014, 11, 6586–6611. [Google Scholar]
- Nakau, M.; Imanishi, J.; Imanishi, J.; Watanabe, S.; Imanishi, A.; Baba, T.; Hirai, K.; Ito, T.; Chiba, W.; Morimoto, Y. Spiritual Care of Cancer Patients by Integrated Medicine in Urban Green Space: A Pilot Study. Explore 2013, 9, 87–90. [Google Scholar] [PubMed]
- Combs, K.M.; Hoag, M.J.; Javorski, S.; Roberts, S.D. Adolescent Self-Assessment of an Outdoor Behavioral Health Program: Longitudinal Outcomes and Trajectories of Change. J. Child Fam. Stud. 2016, 25, 3322–3330. [Google Scholar]
- Russell, K.C.; Gillis, H.L.L.; Heppner, W. An examination of mindfulness-based experiences through adventure in substance use disorder treatment for young adult males: A pilot study. Mindfulness 2016, 7, 320–328. [Google Scholar] [CrossRef]
- Russell, K.C.; (Lee) Gillis, H.L.; Kivlighan, D.M. Process factors explaining psycho-social outcomes in adventure therapy. Psychotherapy 2017, 54, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Russell, K.C.; Gillis, H.L.; Law, L.; Couillard, J. A Pilot Study Examining Outcomes Associated with the Implementation of Progress Monitoring at a Substance Use Disorder Treatment Program for Adolescents. Child Youth Care Forum 2018, 47, 403–419. [Google Scholar]
- Chapman, J.; Groark, S.; Beale, M.M.; Mandas, P.; Argo, K.; Gillis, H.L.L. The Relationship Between Self-Reported Prior Drug Use and Treatment Effectiveness in Substance Use Disorder during Outdoor Behavioral Healthcare Treatment for Young Adult Males. J. Ther. Sch. Programs 2018, 10, 3227. [Google Scholar]
- Unsworth, S.; Palicki, S.-K.; Lustig, J. The Impact of Mindful Meditation in Nature on Self-Nature Interconnectedness. Mindfulness 2016, 7, 1052–1060. [Google Scholar]
- Segal, Z.V.; Williams, J.M.G.; Teasdale, J.D. Mindfulness-Based Cognitive Therapy for Depression: A New Approach to Preventing Relapse; Guilford Press: New York, NY, USA, 2002. [Google Scholar]
- Grahn, P.; Stigsdotter, U.K. The relation between perceived sensory dimensions of urban green space and stress restoration. Landsc. Urban Plan. 2010, 94, 264–275. [Google Scholar] [CrossRef]
- Corazon, S.S.; Schilhab, T.S.S.; Stigsdotter, U.K. Developing the therapeutic potential of embodied cognition and metaphors in nature-based therapy: Lessons from theory to practice. J. Adventure Educ. Outdoor Learn. 2011, 11, 161–171. [Google Scholar]
- Schuling, R.; Van Herpen, N.; De Nooij, R.; De Groot, W.T.; Speckens, A. Silent into Nature: Factors Enabling Improvement in a Mindful Walking Retreat in Nature of People with Psychological Symptoms. Ecopsychology 2018, 10, 77–86. [Google Scholar]
- Poulsen, D.V.; Stigsdotter, U.K.; Djernis, D.; Sidenius, U. ‘Everything just seems much more right in nature’: How veterans with post-traumatic stress disorder experience nature-based activities in a forest therapy garden. Health Psychol. Open 2016, 3. [Google Scholar] [CrossRef] [PubMed]
- Sidenius, U.; Stigsdotter, U.K.; Poulsen, D.V.; Bondas, T. “I look at my own forest and fields in a different way”: The lived experience of nature-based therapy in a therapy garden when suffering from stress-related illness. Int. J. Qual. Stud. Health Well-Being 2017, 12, 1324700. [Google Scholar] [PubMed]

| Sample Size | Heterogeneity | Global Effect Aizes | Fail-Safe N c | Criterion | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| k | N | Q b | df | p | I2 | Hedges’ g | 95% CI | p | |||
| Outcome from pre- to post-treatment | |||||||||||
| Combined effect across designs and outcomes | 25 | 241.1 | 24 | <0.001 | 90.0 | 0.54 | 0.34–0.75 | <0.001 | 2146 | 135 | |
| Adjusted for publication bias a | 32 | 0.83 | 0.55–0.91 | ||||||||
| Open trials | 13 | 1737 | 170.4 | 12 | <0.001 | 93.0 | 0.66 | 0.38–0.94 | <0.001 | 1211 | 75 |
| Adjusted for publication bias | 15 | 0.76 | 0.50–1.02 | ||||||||
| Studies with passive control group | 6 | 821 | 10.3 | 5 | 0.068 | 51.4 | 0.58 | 0.34–0.82 | <0.001 | 67 | 45 |
| Studies with active control group | 7 | 900 | 12.1 | 7 | 0.096 | 42.3 | 0.26 | 0.04–0.49 | 0.023 | 11 | 50 |
| Combined effect across designs for each type of outcome | |||||||||||
| Psychological | 24 | 2990 | 215.7 | 23 | <0.001 | 89.3 | 0.55 | 0.36–0.74 | <0.001 | 2169 | 130 |
| Adjusted for publication bias | 30 | 0.69 | 0.52–0.87 | ||||||||
| Physical | 7 | 439 | 18.6 | 6 | 0.005 | 67.7 | 0.36 | 0.08–0.63 | 0.011 | 29 | 45 |
| Adjusted for publication bias | 1 | 0.29 | 0.02–0.55 | ||||||||
| Social | 4 | 432 | 3.9 | 2 | 0.143 | 48.6 | 0.39 | 0.13–0.65 | 0.004 | 13 | 25 |
| Adjusted for publication bias | 5 | 0.22 | −0.03–0.48 | ||||||||
| Outcome from pre-treatment to follow-up | |||||||||||
| Combined effect across designs | 8 | 1071 | 13.5 | 7 | 0.060 | 48.3 | 0.56 | 0.34–0.78 | <0.001 | 97 | 50 |
| Adjusted for publication bias | 11 | 0.73 | 0.59–0.86 | ||||||||
| Open trials | 4 | 791 | 8.9 | 4 | 0.064 | 55.2 | 0.66 | 0.39–0.92 | <0.001 | 66 | 35 |
| Categorical moderators | |||||||||||
| Type of nature: | |||||||||||
| Garden/park | 8 | 501 | 17.3 | 8 | 0.027 | 53.7 | 0.33 | 0.09–0.56 | 0.008 | 28 | 55 |
| Wild/forest | 15 | 1578 | 169.5 | 13 | <0.001 | 92.3 | 0.66 | 0.40–0.93 | <0.001 | 14 | 80 |
| Adjusted for publication bias | 17 | 0.80 | 0.56–1.04 | ||||||||
| Between-group difference | 3.4 | 1 | 0.065 | ||||||||
| Type of mindfulness: | |||||||||||
| Formal | 9 | 544 | 18.1 | 8 | 0.021 | 55.7 | 0.37 | 0.15–0.59 | 0.001 | 53 | 55 |
| Adjusted for publication bias | 10 | 0.31 | 0.08–0.53 | ||||||||
| Informal | 8 | 1309 | 127.6 | 7 | <0.001 | 94.5 | 0.80 | 0.38–1.23 | <0.001 | 463 | 50 |
| Between-group difference | 3.1 | 1 | 0.078 | ||||||||
| Trait building | 4 | 276 | 14.8 | 3 | 0.002 | 79.8 | 10 | −0.49–0.69 | 0.732 | ||
| State inducing | 21 | 2624 | 214.6 | 20 | <0.001 | 90.7 | 0.62 | 0.41–0.83 | <0.001 | 2041 | 115 |
| Between-group difference | 2.6 | 1 | 0.107 | ||||||||
| Moderator | B | SE | p |
|---|---|---|---|
| Participant characteristics | |||
| Mean sample age | <0.01 | 0.01 | 0.893 |
| % women | <−0.01 | <0.01 | 0.425 |
| % Whites | 0.01 | 0.01 | 0.506 |
| Intervention characteristics | |||
| Intervention duration | <0.01 | <0.01 | 0.716 |
| Sessions with mindfulness | <−0.01 | 0.01 | 0.597 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Djernis, D.; Lerstrup, I.; Poulsen, D.; Stigsdotter, U.; Dahlgaard, J.; O’Toole, M. A Systematic Review and Meta-Analysis of Nature-Based Mindfulness: Effects of Moving Mindfulness Training into an Outdoor Natural Setting. Int. J. Environ. Res. Public Health 2019, 16, 3202. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16173202
Djernis D, Lerstrup I, Poulsen D, Stigsdotter U, Dahlgaard J, O’Toole M. A Systematic Review and Meta-Analysis of Nature-Based Mindfulness: Effects of Moving Mindfulness Training into an Outdoor Natural Setting. International Journal of Environmental Research and Public Health. 2019; 16(17):3202. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16173202
Chicago/Turabian StyleDjernis, Dorthe, Inger Lerstrup, Dorthe Poulsen, Ulrika Stigsdotter, Jesper Dahlgaard, and Mia O’Toole. 2019. "A Systematic Review and Meta-Analysis of Nature-Based Mindfulness: Effects of Moving Mindfulness Training into an Outdoor Natural Setting" International Journal of Environmental Research and Public Health 16, no. 17: 3202. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16173202