Exploring the Linkage between the Neighborhood Environment and Mental Health in Guangzhou, China

Abstract
:1. Introduction
2. Data and Methods
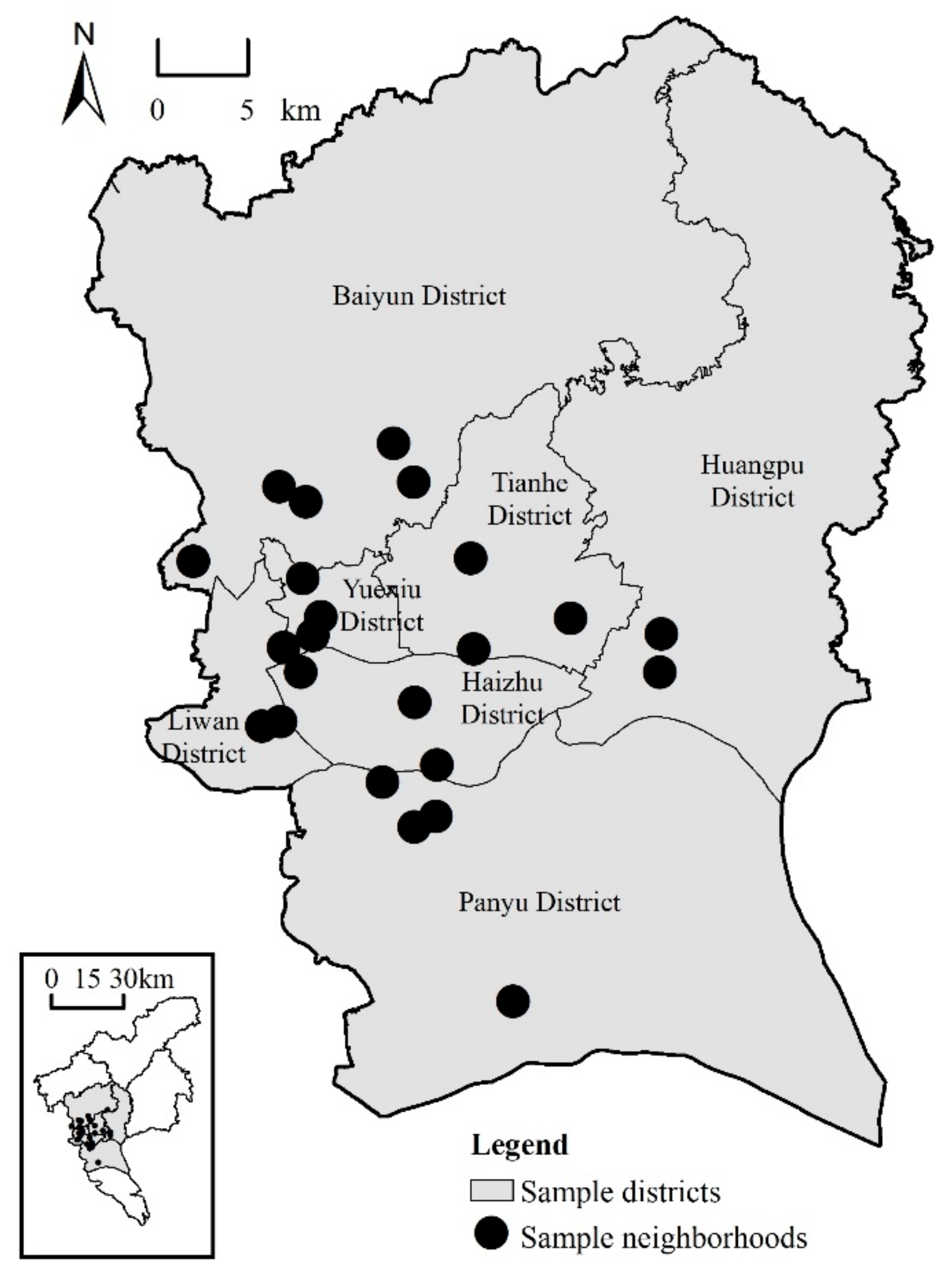
2.1. Data and Research Area
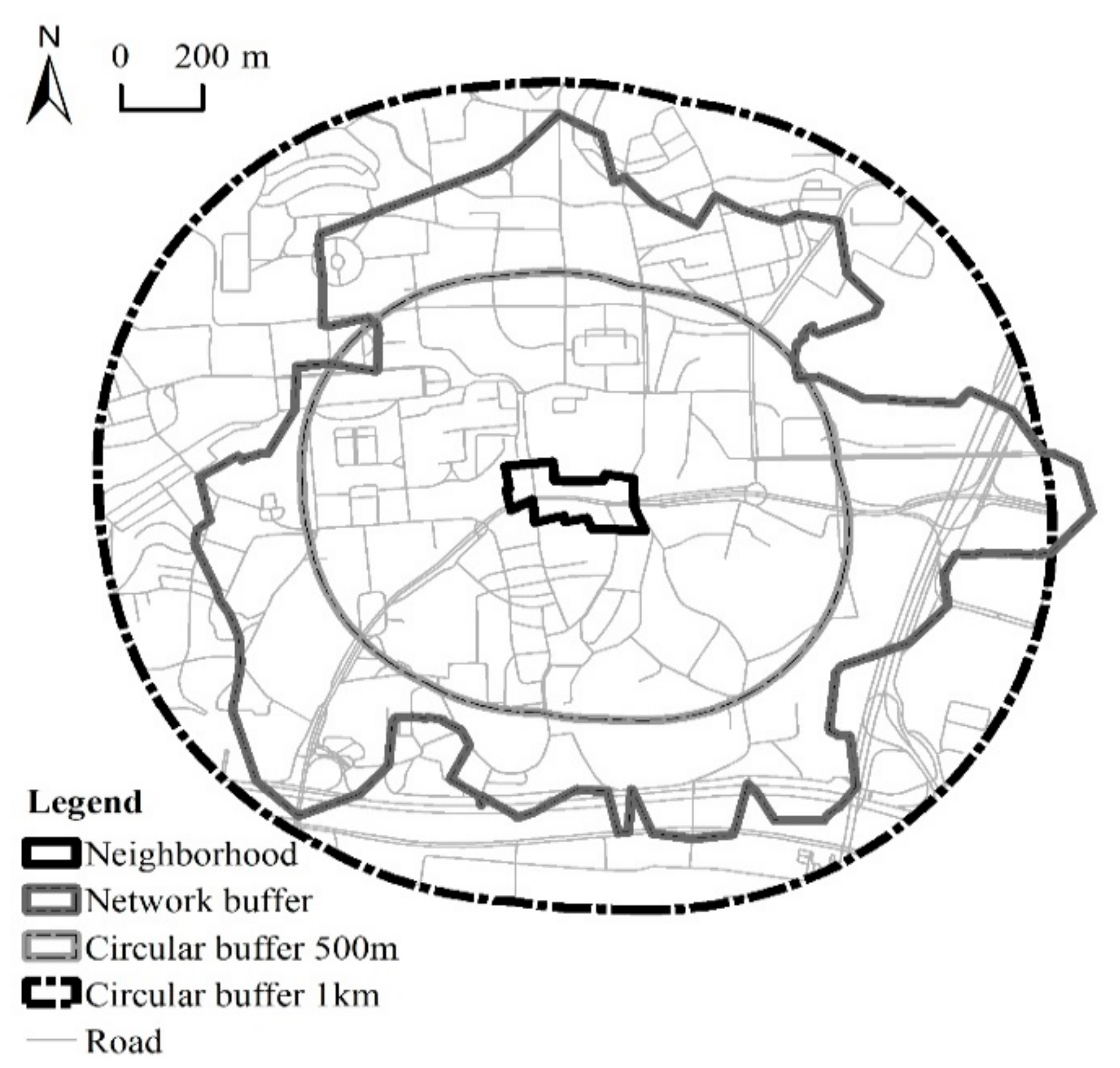
2.2. Delineation of Built-Environment Impact Area
2.3. Measures of Mental Health
2.4. Independent Variables
2.4.1. Built-Environment
2.4.2. Social Environment
2.4.3. Socio-Demographics
2.5. Multilevel Model Analysis
3. Results
3.1. Mental Health and Individual-Level Variables
3.2. Mental Health and Neighborhood Environment
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Mental Health Action Plan 2013–2020; World Health Organization Press: Geneva, Switzerland, 2014; p. 5. [Google Scholar]
- Lederbogen, F.; Kirsch, P.; Haddad, L.; Streit, F.; Tost, H.; Schuch, P.; Wüst, S.; Pruessner, J.C.; Rietschel, M.; Deuschle, M.; et al. City living and urban upbringing affect neural social stress processing in humans. Nature 2011, 474, 498–501. [Google Scholar] [CrossRef] [PubMed]
- Kwan, M. Geographies of health. Ann. Assoc. Am. Geogr. 2012, 102, 891–892. [Google Scholar] [CrossRef]
- Giles-Corti, B.; Vernez-Moudon, A.; Reis, R.; Turrell, G.; Dannenberg, A.L.; Badland, H.; Foster, S.; Lowe, M.; Sallis, J.F.; Stevenson, M.; et al. City planning and population health: A global challenge. Lancet 2016, 388, 2912–2924. [Google Scholar] [CrossRef]
- Almedom, A.M. Social capital and mental health: An interdisciplinary review of primary evidence. Soc. Sci. Med. 2005, 61, 943–964. [Google Scholar] [CrossRef] [PubMed]
- Evans, G.W.; Wells, N.M.; Moch, A. Housing and mental health: A review of the evidence and a methodological and conceptual critique. J. Soc. Issues 2003, 59, 475–500. [Google Scholar] [CrossRef]
- Markevych, I.; Schoierer, J.; Hartig, T.; Chudnovsky, A.; Hystad, P.; Dzhambov, A.M.; De Vries, S.; Triguero-Mas, M.; Brauer, M.; Nieuwenhuijsen, M.J.; et al. Exploring pathways linking greenspace to health: Theoretical and methodological guidance. Environ. Res. 2017, 158, 301–317. [Google Scholar] [CrossRef]
- Harpham, T. Urban health in developing countries: What do we know and where do we go? Health Place 2009, 15, 107–116. [Google Scholar] [CrossRef]
- Moore, M.; Gould, P.; Keary, B.S. Global urbanization and impact on health. Int. J. Hyg. Environ. Health 2003, 206, 269–278. [Google Scholar] [CrossRef]
- Li, B. Floating population or urban citizens? Status, social provision and circumstances of rural–urban migrants in China. Soc. Policy Admin. 2006, 40, 174–195. [Google Scholar] [CrossRef]
- Miao, J.; Wu, X. Urbanization, socioeconomic status and health disparity in China. Health Place 2016, 42, 87–95. [Google Scholar] [CrossRef]
- Xiang, Y.; Yu, X.; Sartorius, N.; Ungvari, G.S.; Chiu, H.F. Mental health in China: Challenges and progress. Lancet 2012, 380, 1715–1716. [Google Scholar] [CrossRef]
- Fan, Y.; Das, K.V.; Chen, Q. Neighborhood green, social support, physical activity, and stress: Assessing the cumulative impact. Health Place 2011, 17, 1202–1211. [Google Scholar] [CrossRef] [PubMed]
- De Vries, S.; Van Dillen, S.M.E.; Groenewegen, P.P.; Spreeuwenberg, P. Streetscape greenery and health: Stress, social cohesion and physical activity as mediators. Soc. Sci. Med. 2013, 94, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Wang, R.; Grekousis, G.; Liu, Y.; Yuan, Y.; Li, Z. Neighbourhood greenness and mental wellbeing in Guangzhou, China: What are the pathways? Landscape Urban Plan 2019, 190, 103602. [Google Scholar] [CrossRef]
- Hartig, T.; Mitchell, R.; Vries, D.S.; Frumkin, H. Nature and health. Annu. Rev. Public Health 2014, 35, 207–228. [Google Scholar] [CrossRef] [PubMed]
- Almanza, E.; Jerrett, M.; Dunton, G.; Seto, E.; Ann Pentz, M. A study of community design, greenness, and physical activity in children using satellite, GPS and accelerometer data. Health Place 2012, 18, 46–54. [Google Scholar] [CrossRef] [Green Version]
- Mytton, O.T.; Townsend, N.; Rutter, H.; Foster, C. Green space and physical activity: An observational study using Health Survey for England data. Health Place 2012, 18, 1034–1041. [Google Scholar] [CrossRef] [Green Version]
- Maas, J.; Van Dillen, S.M.E.; Verheij, R.A.; Groenewegen, P.P. Social contacts as a possible mechanism behind the relation between green space and health. Health Place 2009, 15, 586–595. [Google Scholar] [CrossRef] [Green Version]
- Guite, H.F.; Clark, C.; Ackrill, G. The impact of the physical and urban environment on mental well-being. Public Health 2006, 120, 1117–1126. [Google Scholar] [CrossRef]
- Liu, Y.; Dijst, M.; Faber, J.; Geertman, S.; Cui, C. Healthy urban living: Residential environment and health of older adults in Shanghai. Health Place 2017, 47, 80–89. [Google Scholar] [CrossRef]
- Wang, R.; Lu, Y.; Zhang, J.; Liu, Y.; Liu, P.; Yao, Y. The relationship between visual enclosure for neighbourhood street walkability and elders’ mental health in China: Using street view images. J. Transp. Health 2019, 13, 90–102. [Google Scholar] [CrossRef]
- Chen, Y.; Wong, G.H.Y.; Lum, T.Y.; Lou, V.W.Q.; Ho, A.H.Y.; Luo, H.; Tong, T.L.W. Neighborhood support network, perceived proximity to community facilities and depressive symptoms among low socioeconomic status Chinese elders. Aging Mental Health 2016, 20, 423–431. [Google Scholar] [CrossRef]
- Berke, E.M.; Gottlieb, L.M.; Moudon, A.V.; Larson, E.B. Protective association between neighborhood walkability and depression in older men. J. Am. Geriatr. Soc. 2007, 55, 526–533. [Google Scholar] [CrossRef] [PubMed]
- Elliott, M. The stress process in neighborhood context. Health Place 2000, 6, 287–299. [Google Scholar] [CrossRef]
- Yang, T.; Matthews, S.A. The role of social and built environments in predicting self-rated stress: A multilevel analysis in Philadelphia. Health Place 2010, 16, 803–810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van den Berg, A.E.; Maas, J.; Verheij, R.A.; Groenewegen, P.P. Green space as a buffer between stressful life events and health. Soc. Sci. Med. 2010, 70, 1203–1210. [Google Scholar] [CrossRef] [Green Version]
- McEachan, R.R.C.; Prady, S.L.; Smith, G.; Fairley, L.; Cabieses, B.; Gidlow, C.; Wright, J.; Dadvand, P.; Van Gent, D.; Nieuwenhuijsen, M.J. The association between green space and depressive symptoms in pregnant women: Moderating roles of socioeconomic status and physical activity. J. Epidemiol. Commun. H. 2016, 70, 253–259. [Google Scholar] [CrossRef]
- Dong, H.; Qin, B. Exploring the link between neighborhood environment and mental wellbeing: A case study in Beijing, China. Landscape Urban Plan 2017, 164, 71–80. [Google Scholar] [CrossRef]
- Sugiyama, T.; Leslie, E.; Giles-Corti, B.; Owen, N. Associations of neighbourhood greenness with physical and mental health: Do walking, social coherence and local social interaction explain the relationships? J. Epidemiol. Commun. H. 2008, 62, e9. [Google Scholar] [CrossRef]
- Kwan, M. The uncertain geographic context problem. Ann. Assoc. Am. Geogr. 2012, 102, 958–968. [Google Scholar] [CrossRef]
- Diez-Roux, A.V.; Mair, C. Neighborhoods and health. Ann. Ny. Acad. Sci. 2010, 1186, 125–145. [Google Scholar] [CrossRef] [Green Version]
- Browning, M.; Lee, K. Within what distance does “greenness” best predict physical health? A systematic review of articles with GIS buffer analyses across the lifespan. Int. J. Environ. Res. Public Health 2017, 14, 675. [Google Scholar] [CrossRef]
- Li, D.; Deal, B.; Zhou, X.; Slavenas, M.; Sullivan, W.C. Moving beyond the neighborhood: Daily exposure to nature and adolescents’ mood. Landscape Urban Plan 2018, 173, 33–43. [Google Scholar] [CrossRef]
- Oliver, L.N.; Schuurman, N.; Hall, A.W. Comparing circular and network buffers to examine the influence of land use on walking for leisure and errands. Int. J. Health Geogr. 2007, 6, 41. [Google Scholar] [CrossRef]
- Stafford, M.; Marmot, M. Neighbourhood deprivation and health: Does it affect us all equally? Int. J. Epidemiol. 2003, 32, 357–366. [Google Scholar] [CrossRef] [PubMed]
- Gary-Webb, T.L.; Baptiste-Roberts, K.; Pham, L.; Wesche-Thobaben, J.; Patricio, J.; Pi-Sunyer, F.X.; Brown, A.F.; Jones-Corneille, L.; Brancati, F.L. Neighborhood socioeconomic status, depression, and health status in the Look AHEAD (Action for Health in Diabetes) study. BMC Public Health 2011, 11, 349. [Google Scholar] [CrossRef]
- Fone, D.; White, J.; Farewell, D.; Kelly, M.; John, G.; Lloyd, K.; Williams, G.; Dunstan, F. Effect of neighbourhood deprivation and social cohesion on mental health inequality: A multilevel population-based longitudinal study. Psychol. Med. 2014, 44, 2449–2460. [Google Scholar] [CrossRef] [PubMed]
- Kawachi, I.; Kennedy, B.P.; Glass, R. Social capital and self-rated health: A contextual analysis. Am. J. Public Health 1999, 89, 1187–1193. [Google Scholar] [CrossRef]
- Kawachi, I.; Kennedy, B.P.; Lochner, K.; Prothrow-Stith, D. Social capital, income inequality, and mortality. Am. J. Public Health 1997, 87, 1491–1498. [Google Scholar] [CrossRef]
- Kawachi, I.; Subramanian, S.V.; Kim, D. Social Capital and Health; Springer: New York, NY, USA, 2008; pp. 15–18. [Google Scholar]
- Berkman, L.F.; Glass, T. Social integration, social networks, social support, and health. In Social Epidemiology; Berkman, L.F., Kawachi, I., Eds.; Oxford University Press: Oxford, NY, USA, 2000; pp. 137–173. [Google Scholar]
- Aneshensel, C.S.; Sucoff, C.A. The neighborhood context of adolescent mental health. J. Health Soc. Behav. 1996, 37, 293–310. [Google Scholar] [CrossRef] [PubMed]
- Stafford, M.; Chandola, T.; Marmot, M. Association between fear of crime and mental health and physical functioning. Am. J. Public Health 2007, 97, 2076–2081. [Google Scholar] [CrossRef] [PubMed]
- Lorenc, T.; Clayton, S.; Neary, D.; Whitehead, M.; Petticrew, M.; Thomson, H.; Cummins, S.; Sowden, A.; Renton, A. Crime, fear of crime, environment, and mental health and wellbeing: Mapping review of theories and causal pathways. Health Place 2012, 18, 757–765. [Google Scholar] [CrossRef] [PubMed]
- Schieman, S.; Meersman, S.C. Neighborhood problems and health among older adults: Received and donated social support and the sense of mastery as effect modifiers. J. Gerontol. B Psychol. Sci. Soc. Sci. 2004, 59, S89–S97. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Wang, R.; Xiao, Y.; Huang, B.; Chen, H.; Li, Z. Exploring the linkage between greenness exposure and depression among Chinese people: Mediating roles of physical activity, stress and social cohesion and moderating role of urbanicity. Health Place 2019, 58, 102168. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Helbich, M.; Yao, Y.; Zhang, J.; Liu, P.; Yuan, Y.; Liu, Y. Urban greenery and mental wellbeing in adults: Cross-sectional mediation analyses on multiple pathways across different greenery measures. Environ. Res. 2019, 176, 108535. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Y.; Miao, S.; Sarkar, C.; Geng, H.; Lu, Y. Exploring the impacts of housing condition on migrants’ mental health in Nanxiang, Shanghai: A structural equation modelling approach. Int. J. Environ. Res. Public Health 2018, 15, 225. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y. Community building and mental health in mid-life and older life: Evidence from China. Soc. Sci. Med. 2014, 107, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Chen, S. Mental health effects of perceived living environment and neighborhood safety in urbanizing China. Habitat Int. 2015, 46, 101–110. [Google Scholar] [CrossRef]
- Chen, H.; Jia, B.; Lau, S.S.Y. Sustainable urban form for Chinese compact cities: Challenges of a rapid urbanized economy. Habitat Int. 2008, 32, 28–40. [Google Scholar] [CrossRef]
- Drukker, M.; Kaplan, C.; Feron, F.; Van Os, J. Children’s health-related quality of life, neighbourhood socio-economic deprivation and social capital. A contextual analysis. Soc. Sci. Med. 2003, 57, 825–841. [Google Scholar] [CrossRef]
- Cotterill, L.; Taylor, D. Promoting mental health and wellbeing amongst housebound older people. Qual. Ageing Older Adults 2001, 2, 32–46. [Google Scholar] [CrossRef]
- Frank, L.D.; Schmid, T.L.; Sallis, J.F.; Chapman, J.; Saelens, B.E. Linking objectively measured physical activity with objectively measured urban form. Am. J. Prev. Med. 2005, 28, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, D.P.; Blackwell, B. Psychiatric illness in general practice: A detailed study using a new method of case identification. Brit. Med. J. 1970, 2, 439–443. [Google Scholar] [CrossRef] [PubMed]
- Chong, M.; Wilkinson, G. Validation of 30- and 12-item versions of the Chinese Health Questionnaire (CHQ) in patients admitted for general health screening. Psychol. Med. 1989, 19, 495–505. [Google Scholar] [CrossRef] [PubMed]
- Lundin, A.; Hallgren, M.; Theobald, H.; Hellgren, C.; Torgén, M. Validity of the 12-item version of the General Health Questionnaire in detecting depression in the general population. Public Health 2016, 136, 66–74. [Google Scholar] [CrossRef]
- Salama-Younes, M.; Montazeri, A.; Ismaïl, A.; Roncin, C. Factor structure and internal consistency of the 12-item General Health Questionnaire (GHQ-12) and the Subjective Vitality Scale (VS), and the relationship between them: A study from France. Health Qual. Life Out 2009, 7, 22. [Google Scholar] [CrossRef] [PubMed]
- Duncan, C.; Jones, K.; Moon, G. Context, composition and heterogeneity: Using multilevel models in health research. Soc. Sci. Med. 1998, 46, 97–117. [Google Scholar] [CrossRef]
- Wang, R.; Xue, D.; Liu, Y.; Liu, P.; Chen, H. The relationship between air pollution and depression in China: Is neighbourhood social capital protective? Int. J. Env. Res. Pub. He. 2018, 15, 1160. [Google Scholar] [CrossRef]
- Flowerdew, R.; Manley, D.J.; Sabel, C.E. Neighbourhood effects on health: Does it matter where you draw the boundaries? Soc. Sci. Med. 2008, 66, 1241–1255. [Google Scholar] [CrossRef]
- Zhao, P.; Kwan, M.; Zhou, S. The uncertain geographic context problem in the analysis of the relationships between obesity and the built environment in Guangzhou. Int. J. Env. Res. Pub. He. 2018, 15, 308. [Google Scholar] [CrossRef]
- Saelens, B.E.; Sallis, J.F.; Frank, L.D.; Cain, K.L.; Conway, T.L.; Chapman, J.E.; Slymen, D.J.; Kerr, J. Neighborhood environment and psychosocial correlates of adults’ physical activity. Med. Sci. Sport. Exer. 2012, 44, 637–646. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Li, F.; Li, J.; Zhang, Y. The relationships between urban parks, residents’ physical activity, and mental health benefits: A case study from Beijing, China. J. Environ. Manage. 2017, 190, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Helbich, M.; Yao, Y.; Liu, Y.; Zhang, J.; Liu, P.; Wang, R. Using deep learning to examine street view green and blue spaces and their associations with geriatric depression in Beijing, China. Environ. Int. 2019, 126, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Rose, N. Urban social exclusion and mental health of China’s rural-urban migrants—A review and call for research. Health Place 2017, 48, 20–30. [Google Scholar] [CrossRef] [PubMed]
- Astell-Burt, T.; Feng, X.; Kolt, G.S. Green space is associated with walking and moderate-to-vigorous physical activity (MVPA) in middle-to-older-aged adults: Findings from 203 883 Australians in the 45 and Up Study. Brit. J. Sport. Med. 2014, 48, 404. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Zhang, F.; Wu, F.; Liu, Y.; Li, Z. The subjective wellbeing of migrants in Guangzhou, China: The impacts of the social and physical environment. Cities 2017, 60, 333–342. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Proportion/Mean (S.D.) |
|---|---|
| GHQ Score | 22.63 (5.27) |
| Gender | |
| Male | 52.26% |
| Female | 47.74% |
| Age | 40.55 (11.07) |
| Marital status and family organization | |
| Single, divorced, or widowed | 15.31% |
| Married and living with family | 78.17% |
| Married but not living with family | 6.52% |
| Education | |
| Junior high school and below | 31.82% |
| Technical school/high school | 33.48% |
| College/university and above | 34.70% |
| Per capita household income per year (10 thousand Yuan) | 4.01 (4.31) |
| Per capita living space (m2) | 30.78 (21.74) |
| Housing tenure | |
| Yes | 54.17% |
| No | 45.83% |
| Hukou status | |
| Guangzhou hukou holders | 59.39% |
| Non-Guangzhou hukou holders | 40.61% |
| Built-environment | |
| Building density (network buffer) (%) | 37.28 (10.57) |
| Building density (circular buffer 1 km) (%) | 41.82 (11.53) |
| Building density (circular buffer 500 m) (%) | 37.06 (12.00) |
| Per capita green area (network buffer) | 18.68 (19.29) |
| Per capita green area (circular buffer 1 km) | 34.82 (38.12) |
| Per capita green area (circular buffer 500 m) | 24.32 (23.47) |
| Neighborhood floor area ratio | 1.83 (0.89) |
| Social environment | |
| Percentage of high interaction | 0.31 (0.12) |
| Percentage of high participation | 0.15 (0.11) |
| Percentage of high reciprocity | 0.66 (0.15) |
| Percentage of high trust | 0.56 (0.19) |
| Neighborhood dispute | 22.01 (37.33) |
| Model Predictors | Null Model | Model 1 (only Control Variables) | Model 2 (Road Network Buffer) | Model 3 (Linear Buffer 1 km) | Model 4 (Linear Buffer 500 m) | ||||
|---|---|---|---|---|---|---|---|---|---|
| Coeff. (Z Value) | Coeff. | Z Value | Coeff | Z Value | Coeff | Z Value | Coeff. | Z Value | |
| Controlled variables | |||||||||
| Gender (ref: male) | 0.14 | 0.46 | 0.28 | 0.86 | 0.28 | 0.84 | 0.28 | 0.86 | |
| Age | 0.02 | 1.24 | 0.03 * | 1.68 | 0.03 | 1.62 | 0.03 | 1.62 | |
| Marital status and family organization (ref: married and living with family) | |||||||||
| Single, divorced, or widowed | 0.79 * | 1.67 | 0.90 | 1.49 | 0.87 | 1.47 | 0.86 | 1.46 | |
| Married but not living with family | −0.85 | −1.30 | −0.55 | −0.66 | −0.57 | −0.68 | −0.56 | −0.66 | |
| Education (ref: Technical school/high school) | |||||||||
| Junior high school and below | 0.95 ** | 2.40 | 0.69 * | 1.71 | 0.70 | 1.66 | 0.68 | 1.61 | |
| College/university and above | −0.74 * | −1.76 | −0.76 * | −1.75 | −0.69 | −1.59 | −0.67 | −1.54 | |
| Per capita household income | 0.03 | 0.68 | 0.04 | 1.10 | 0.04 | 1.00 | 0.04 | 0.97 | |
| Per capita living space per year | 0.22 | 1.20 | −0.02 | −0.09 | −0.02 | −0.11 | −0.02 | −0.12 | |
| Hukou status (ref: Non−Guangzhou hukou holders) | −0.37 | −0.87 | −0.56 | −1.57 | −0.52 | −1.42 | −0.5 | −1.41 | |
| Housing tenure (ref: Yes) | 1.03 ** | 2.41 | 1.57 *** | 2.85 | 1.51 *** | 2.73 | 1.51 *** | 2.71 | |
| Neighborhood-level variables | |||||||||
| Building density | −0.08 *** | −3.18 | −0.04 | −1.46 | −0.03 | −1.20 | |||
| Per capita green area | −0.18 ** | −2.11 | −0.08 | −0.73 | −0.18 * | −1.81 | |||
| Neighborhood floor area ratio | −0.56 *** | −3.00 | −0.75 *** | −3.17 | −0.77 *** | −3.17 | |||
| Percentage of high interaction | −2.86 * | −1.69 | −2.28 | −1.14 | −2.29 | −1.16 | |||
| Percentage of high participation | 3.19 | 1.17 | 4.18 | 1.41 | 4.74 * | 1.72 | |||
| Percentage of high reciprocity | −3.25 * | −1.85 | −1.79 | −0.87 | −2.36 | −1.21 | |||
| Percentage of high trust | 0.44 | 0.31 | −0.58 | −0.33 | 0.19 | 0.13 | |||
| Neighborhood dispute | 0.01 *** | 3.00 | 0.01 *** | 2.65 | 0.01 *** | 3.37 | |||
| Constant | 10.64 *** (31.79) | 10.13 *** | 26.76 | 9.97 *** | 22.51 | 9.98 *** | 22.61 | 9.978 *** | 22.78 |
| Interclass variance | 1.38 | — | 0.41 | 0.66 | 0.69 | ||||
| Intra−class variance | 5.12 | 5.17 | 5.04 | 5.04 | 5.04 | ||||
| Log likelihood | −3447.17 | −3523.29 | −3416.67 | −3420.19 | −3420.43 | ||||
| ICC | 21.23% | — | 7.52% | 11.58% | 12.04% | ||||
| Variance reduction ratio | — | — | 70.29% | 52.17% | 50.00% | ||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qiu, Y.; Liu, Y.; Liu, Y.; Li, Z. Exploring the Linkage between the Neighborhood Environment and Mental Health in Guangzhou, China. Int. J. Environ. Res. Public Health 2019, 16, 3206. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16173206
Qiu Y, Liu Y, Liu Y, Li Z. Exploring the Linkage between the Neighborhood Environment and Mental Health in Guangzhou, China. International Journal of Environmental Research and Public Health. 2019; 16(17):3206. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16173206
Chicago/Turabian StyleQiu, Yingzhi, Yuqi Liu, Yi Liu, and Zhigang Li. 2019. "Exploring the Linkage between the Neighborhood Environment and Mental Health in Guangzhou, China" International Journal of Environmental Research and Public Health 16, no. 17: 3206. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16173206