What Is the Experience of Practitioners in Health, Education or Social Care Roles Following a Death by Suicide? A Qualitative Research Synthesis


Abstract
:1. Introduction
2. Materials and Methods
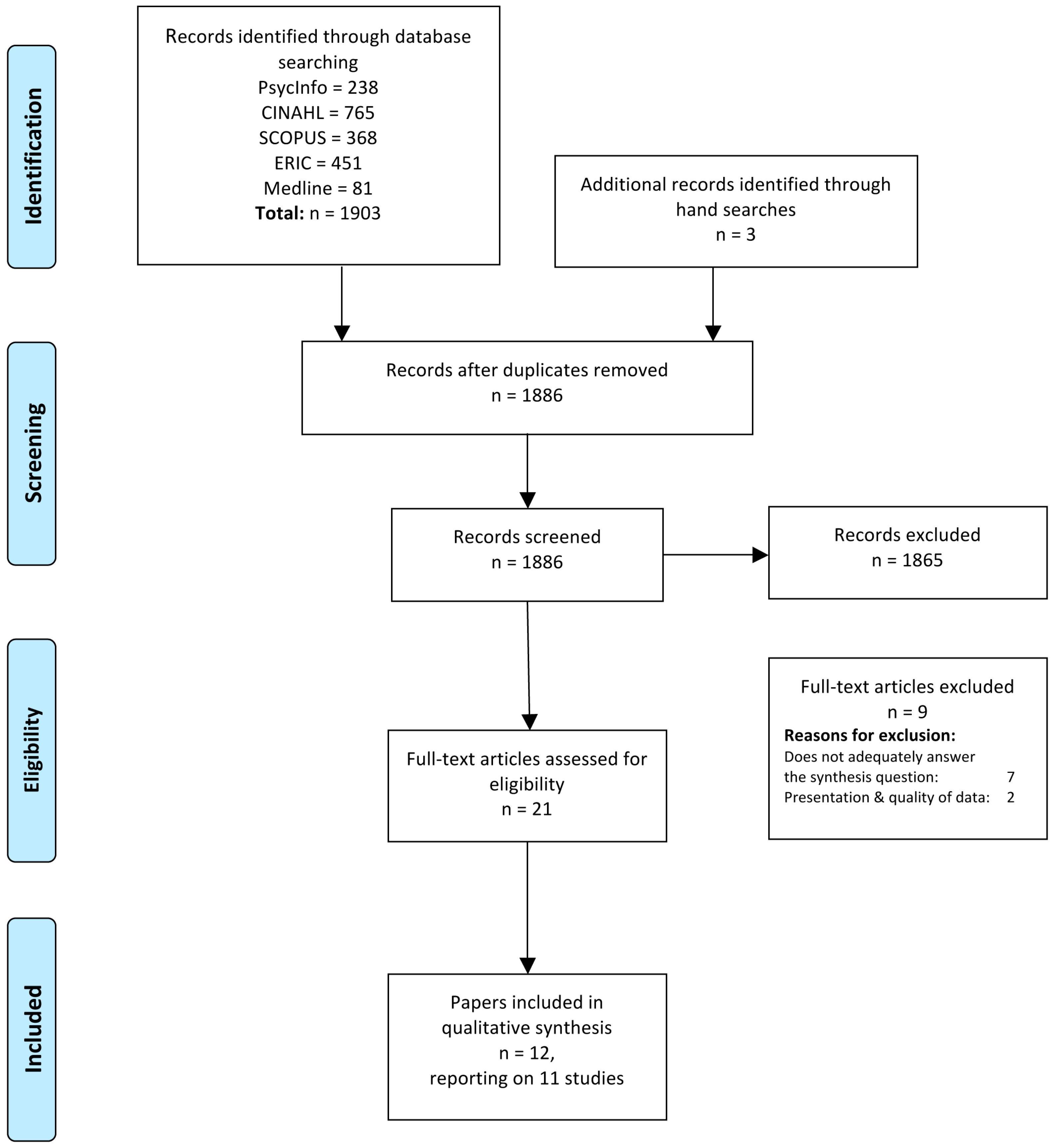
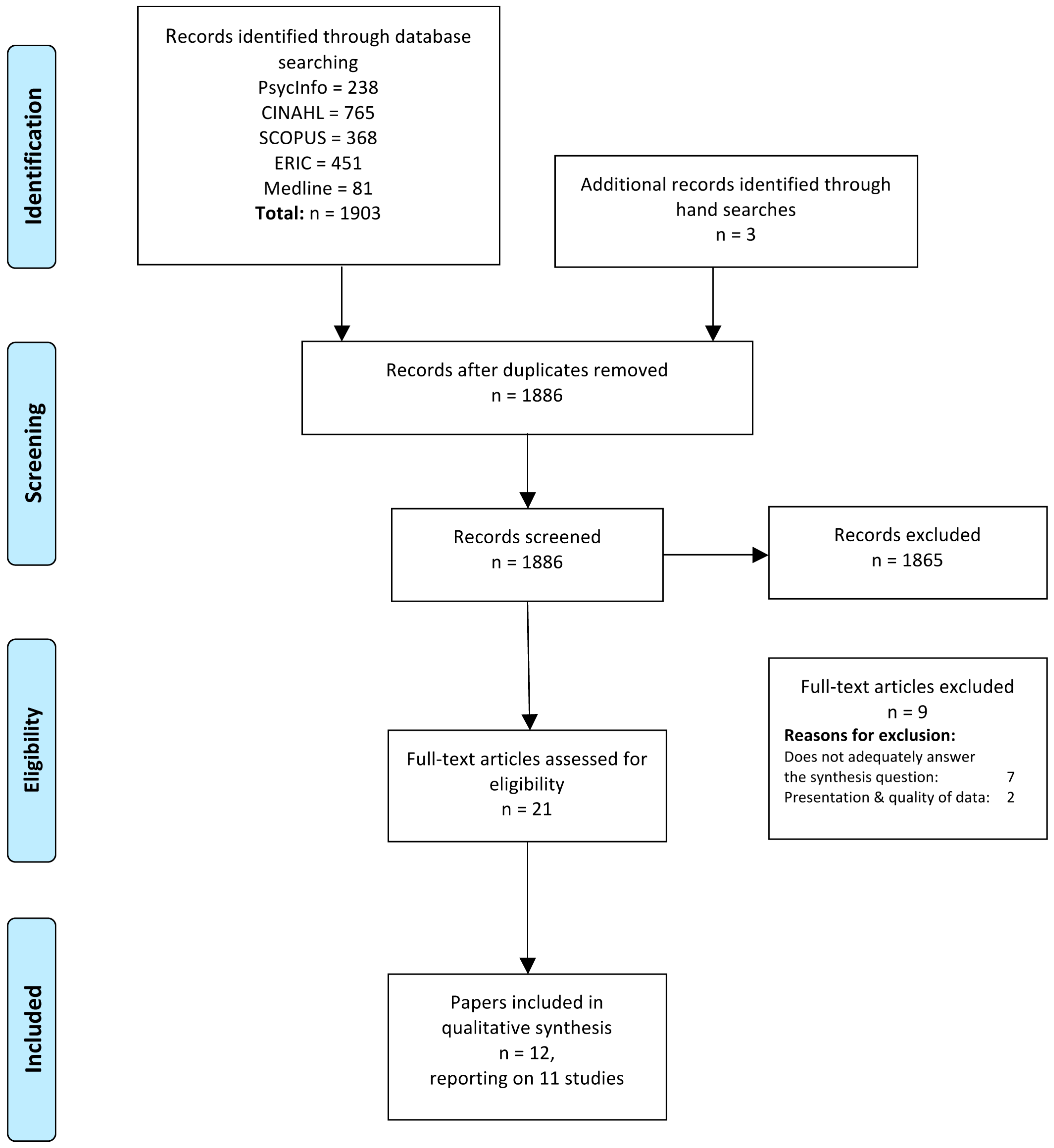
2.1. Search Strategy
| Medline: | Journal Article |
| PsycInfo: | Peer Review; Qualitative Studies |
| CINAHL: | Peer Review |
| SCOPUS: | Journal Article; Peer Review; Qualitative; Interview |
| ERIC: | Journal Article; Peer Review |
2.2. Screening the Literature
2.3. Study Eligibility
2.4. Quality Assessment
2.5. Data Extraction
2.6. Analysis
2.6.1. Comparison of Themes
- What happened—experiencing the event
- Emotional response—experiencing the feelings
- Impact on practice—how do I practice now?
- Internal responses/self scrutiny—Am I ok?
- Responses of others—do they blame me?
- Experiences of support—who will look after me?
- Self care/maintenance—can I look after myself?
- Training needs—what do/did I need to know?
2.6.2. Coding, Synthesis and Interpretation
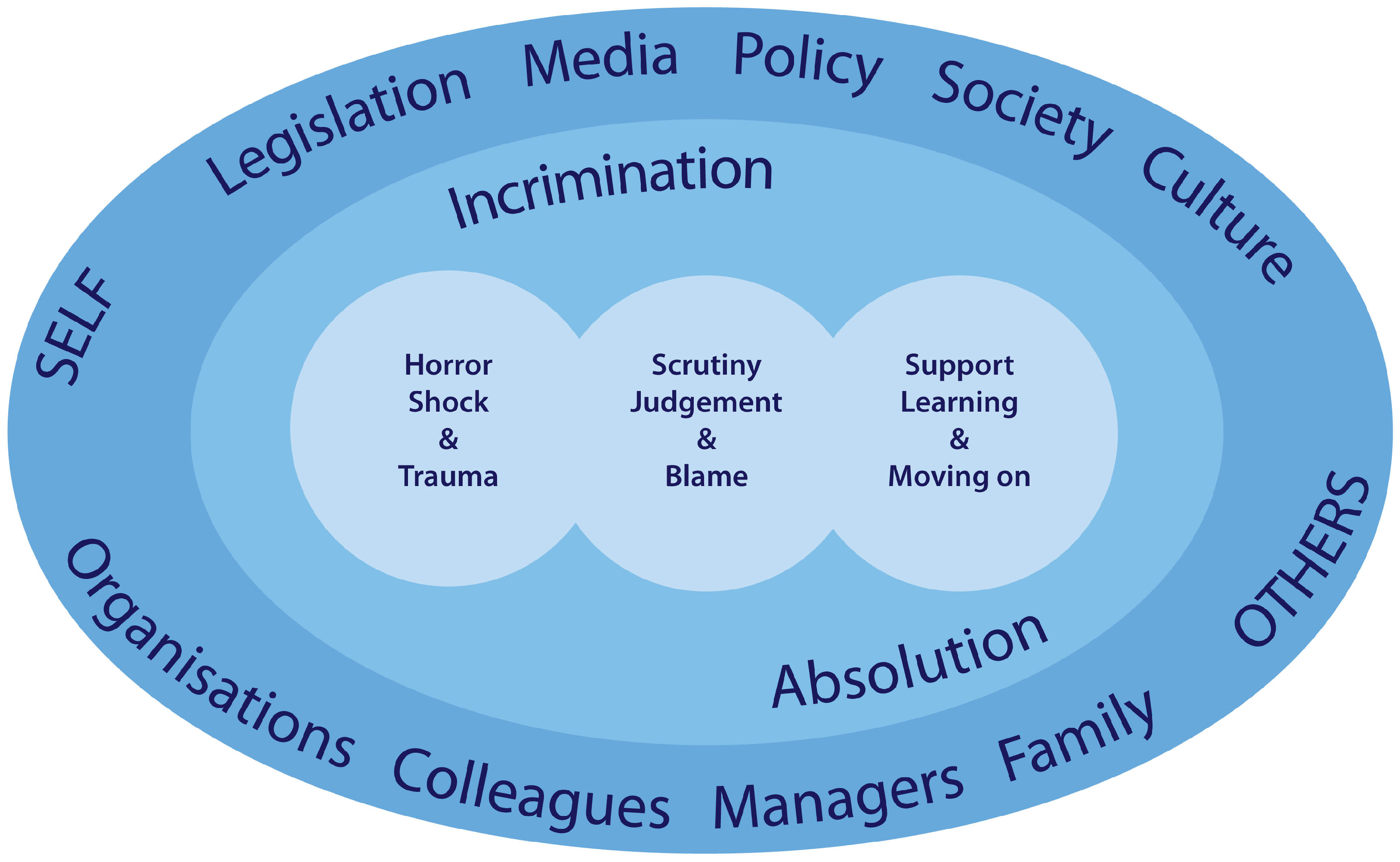
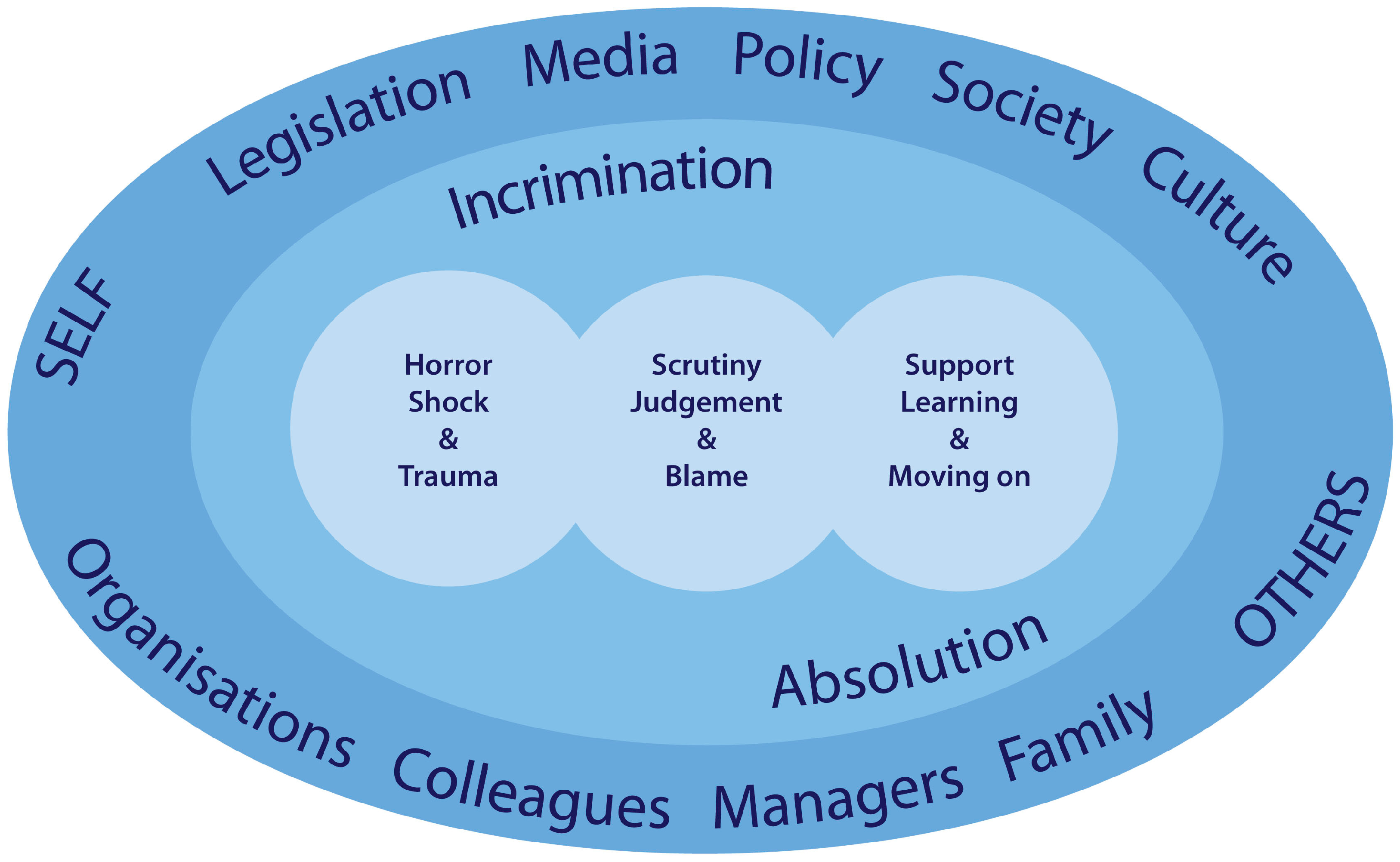
3. Results
- Horror, Shock and Trauma
- Scrutiny, Judgement and Blame
- Support, Learning and Living With
3.1. Horror, Shock and Trauma
3.1.1. Witnessing Suicide
“I had to do CPR with the inpatient vomiting blood. Bleeding profusely from the inpatient’s head, terror of the death scene made me all of a quiver”[31].
“I have incredible nightmares. To this day, at night-time, it’s like his face exploded and all I remember was blood and remnants”[22].
“A mother of two small girls, she jumped in front of a train, she wasn’t very old, it was awful.”[24].
“[I] had trouble conceiving that he had actually followed through”[28].
“to work as a team with all the other nurses to try and save this person”[20].
“I was absolutely stunned and completely and immediately traumatised. I was absolutely shocked.”[29].
3.1.2. Responses to Suicide
“I could not control my crying. I mean, I was grief-stricken. When I say I came undone that’s when I really let myself open up and sob and cry.”[30].
“the night he died, I got deathly ill: I had to go to the emergency room. I thought I was having a heart attack.”[30].
3.1.3. Dealing with Suicide
“I had a patient who took his life. Something was wrong, but I couldn’t find out what. I couldn’t get him to talk about it … I asked him 17 times if he was depressed, but he said that he was fine. It was terrible.”[24].
3.2. Scrutiny Judgement and Blame
3.2.1. Thinking about Responsibility
“It feels like an incredible responsibility. I know when I started with this woman, she was suicidal on and off; I spent a lot of emotional energy worrying if I screwed up on my decisions.”[30].
“I told myself I wasn’t responsible for this – that his social worker was away. I was merely covering her caseload. All in an attempt to distance myself”[28].
“I was just so stunned, and worried what people thought … would think ‘she did a terrible job or else her client wouldn’t have killed herself’”[30].
“I scrutinized like mad if he had – was there something special about him, was he miserable, was there something I completely overlooked – I really tried to rewind the film as well as possible. I really tried to scrutinize if there was anything in that consultation which I ought to have picked up, have caught …”[24].
“… did I give him the medication he then killed himself with?”[27].
“Well this is an awful failure, I think, as a doctor to have experienced that. It is horrible. I think, there we have actually failed”[24].
“… a fear that I will be accused of screwing up somehow … I was afraid the [students] wouldn’t ever want to talk to me again. That they would be really angry with me, and that nobody would trust me”[22].
“It’s a fact of life I’m afraid, you can’t stop some people from taking their own lives”[27].
“I was pissed [at the client]; felt like why the hell couldn’t they have called me? Why couldn’t they have talked to me?... They have not thought to turn to me?”[30].
“it’s not my responsibility because if they’re going to kill themselves they’re going to kill themselves. I have absolutely no control over that”[30].
“sometimes a person feels the only way they can attain complete autonomy is through their own demise”[28].
“She did what she felt she had to do. She was tired of trying to cope with life and never quite succeeding. Suicide was her first real success in life and she proved to everyone she was capable of doing it”[28].
3.2.2. Having to Carry on
“I don’t think anybody would be different in the amount of aloneness you feel about it all … it would have been nice to have someone to guide me through all of that”[21].
“Clinicians reporting dissociative phenomena were also those who experienced more isolation from colleague support, feeling alone with the trauma of their patient’s suicide and cut off not only from others, but also, in the dissociative experience, from themselves.”[29].
“there is a lot that is not under our control given the population of clients that is worked with in mental health treatment facilities”[28].
“I’ve been a GP for 30 years and you just have to deal with it and accept it”[27].
“It was very important for all of us involved in his treatment to share the last contacts we had with him and what he had said, what we had said, and where we were left. Not so much pointing the finger but searching for anything that could help us make sense of it”[29].
“I think that eventually I had to understand that there is no control in a lot of those situations and in that whole process that I had to take ownership of myself and let everything else go”[21].
“We came up with this policy, if a person has been actively suicidal within six months, we send them elsewhere. We used that six months I think to distance ourselves somewhat, to make us less involved in the most at-risk clients. It has impacted my practice. I try to create a little more distance from being that first responder”[30].
“I won’t enter the ward the patient lived if it was not really needed, lest recalling the suicide scene and making me nervous”[31].
“when I have a patient who is getting closer to thinking about suicide, my anxiety goes through the roof more than it did before, and I am clear that suicide is just not an option. I’m not open to bargaining … and I demand the patient seek hospitalisation”[29].
3.2.3. Dealing with Others
“All teachers weren’t caught talking about it for it was a top secret for the school. And the principal forbade the news about it from leaking out to anyone… Suicide brings about school … shame … [t]hat’s why schools tried to hide the news”[25].
“I had to be strong for everybody else right? I had to be strong for the students and I had to put my grieving aside so I could do that”[21].
“I remember this woman who pointed a finger at me and said I will make sure that you will never work again … this woman said you are responsible for my brother’s death. Actually your cruelty caused my brother to choose to jump through a window than be taken care of by you”[26].
“I just broke down and cried in the meeting [with the family] and there was nothing from them, nothing at all. This had been their daughter, and their coldness and indifference … was terribly uncomfortable, painful, and confusing”[29].
“I felt angry about having to consider legal implications when I was trying to deal with my own grief and help others deal with their grief”[29].
“There’s so much litigation that even sitting down and talking about a case you’re concerned that whatever is said might be somehow subpoenaed … some attorney will if they hear about a discussion, they’ll subpoena everyone that was there …”[30].
“Teachers assumed that mentioning the suicide is an insult to the deceased and their family who broke the social norms. And school community members accept it as a disgrace to the school.”[25].
3.3. Support, Learning and Living with
3.3.1. Experiences of Support
“I had a fiancé and I had one roommate, so they gave me whatever support they could, but they weren’t professionals either … they weren’t trained in dealing with grief or anything like that”[21].
“No, we don’t receive any support, we’re good at supporting each other within the practice … so we have a supportive network within the practice and talk it through ourselves but we don’t have any formal back up or counselling involved.”[27].
“Our immediate line managers came in and we were offered basic counselling, a debriefing session immediately … we were allowed to go off work, to go home, we got follow-up phone calls at home to make sure that everything was ok and everything, and we were offered debriefing over the next few days”[20].
3.3.2. Learning
“[Participants stated] that they felt “poorly prepared for a client suicide”, through their [professional] education, and that the event left them “aware of how untrained and naïve I was …”[28].
3.3.3. Living with
“I still feel sorry that she is gone. Still occasionally go over and over the events leading up to the suicide wondering if I could have done something different”[28].
“I have acknowledged that I can not possibly save all my clients. I try to do my best always and be on top of things”[28].
“I take care of myself and take quiet time for myself”; “one of my personal supports is prayer and a spiritual community where we are all working on our spiritual growth”[22].
“I spent a good year seeing a career counsellor because I wasn’t sure I wanted to stay in this job”[21].
4. Discussion
4.1. Strengths and Limitations
4.2. Implications and Recommendations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Andriessen, K. Can postvention be prevention? Crisis 2009, 30, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Jordan, J.R.; McIntosh, J.L. Grief after Suicide: Understanding the Consequences and Caring for the Survivors; Brunner-Routledge: New York, NY, US, 2011. [Google Scholar]
- Cerel, J.; Brown, M.M.; Maple, M.; Singleton, M.; van de Venne, J.; Moore, M.; Flaherty, C. How many people are exposed to suicide? Not six. Suicide Life Threat Behav. 2018. [Google Scholar] [CrossRef] [PubMed]
- Andriessen, K. Suicide bereavement and postvention in major suicidology journals: Lessons learned for the future of postvention. Crisis 2014, 35, 338–348. [Google Scholar] [CrossRef] [PubMed]
- Bartik, W.; Maple, M.; Edwards, H.; Kiernan, M. Adolescent survivors after suicide: Australian young people’s bereavement narratives. Crisis 2013, 34, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Halligan, P.; Corcoran, P. The impact of patient suicide on rural general practitioners. Br. J. Gen. Pract. J. R. Coll. Gen. Pract. 2001, 465, 295–296. [Google Scholar]
- Takahashi, C.; Chida, F.; Nakamura, H.; Akasaka, H.; Yagi, J.; Koeda, A.; Takusari, E.; Otsuka, K.; Akio Sakai, A. The impact of inpatient suicide on psychiatric nurses and their need for support. BMC Psychiatry 2011. [Google Scholar] [CrossRef] [PubMed]
- Yousaf, F.; Hawthorne, M.; Sedgwick, P. Impact of patient suicide on psychiatric trainees. Psychiatr. Bull. 2002, 26, 53–55. [Google Scholar] [CrossRef]
- Kolves, K.; Ross, V.; Hawgood, J.; Spence, H.H.; De Leo, D. The impact of a student’s suicide: Teachers’ perspectives. J. Affect. Disord. 2017, 207, 276–281. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, J.; Ting, S.; Sanders, S.; Harrington, D. Prevalence of and reactions to fatal and nonfatal client suicidal behavior; A national study of mental health workers. OMEGA J. Death Dying 2005, 49, 237–248. [Google Scholar] [CrossRef]
- Andriessen, K.; Rahman, B.; Draper, B.; Dudley, M.; Mitchell, P.B. Prevalence of exposure to suicide: A meta-analysis of population-based studies. J. Psychiatr. Res. 2017, 88, 113–120. [Google Scholar] [CrossRef]
- Cerel, J.; McIntosh, J.L.; Neimeyer, R.A.; Maple, M.; Marshall, D. The continuum of “survivorship”: Definitional issues in the aftermath of suicide. Suicide Life-Threat. Behav. 2014, 44, 591–600. [Google Scholar] [CrossRef]
- Cerel, J.; Maple, M.; van de Venne, J.; Brown, M.; Moore, M.; Flaherty, C. Suicide exposure in the population: Perceptions of impact and closeness. Suicide Life-Threat. Behav. 2017, 47, 696–708. [Google Scholar] [CrossRef]
- Castelli-Dransart, D.A.; Treven, M.; Grad, O.T.; Andriessen, K. Impact of client suicide on health and mental health professionals. In Postvention in Action: The International Handbook of Suicide Bereavement Support; Andriessen, K., Krysinska, K., Grad, O.T., Eds.; Hogrefe: Göttingen, Germany, 2017; pp. 245–254. [Google Scholar]
- Gaffney, P.; Russell, V.; Collins, K.; Bergin, A.; Halligan, P.; Carey, C.; Coyle, S. Impact of patient suicide on front-line staff in Ireland. Death Stud. 2009, 33, 639–656. [Google Scholar] [CrossRef]
- Wurst, F.M.; Kunz, I.; Skipper, G.; Wolfersdorf, M.; Beine, K.H.; Vogel, R.; Muller, S.; Petitjean, S.; Thon, N. How therapists react to patient’s suicide: findings and consequences for health care professionals’ wellbeing. Gen. Hosp. Psychiatry 2013, 35, 565–570. [Google Scholar] [CrossRef]
- Castelli-Dransart, D.A.; Gutjahr, E.; Gulfi, A.; Kaufmann Didisheim, N.; Séguin, M. Patient suicide in institutions: emotional responses and traumatic impact on Swiss Mental Health Professionals. Death Stud. 2014, 38, 315–321. [Google Scholar] [CrossRef]
- Andriessen, K.; Castelli Dransart, D.A.; Cerel, J.; Maple, M. Current postvention research and priorities for the future: Results of a survey. Crisis 2017. [Google Scholar] [CrossRef]
- Willig, C. Introducing Qualitative Research in Psychology; Open University: London, UK, 2008. [Google Scholar]
- Bohan, F.; Doyle, L. Nurses’ experiences of patient suicide and suicide attempts in an acute unit. Ment. Health Pract. 2008, 11, 12–16. [Google Scholar] [CrossRef]
- Christianson, C.L.; Everall, R.D. Constructing bridged of support: School Counsellors’ experiences of student suicide. Can. J. Couns. 2008, 42, 209–221. [Google Scholar]
- Christianson, C.L.; Everall, R.D. Breaking the silence: School counsellors’ expeirences of client suicide. Br. J. Guid. Couns. 2009, 37, 157–168. [Google Scholar] [CrossRef]
- Darden, A.; Rutter, P. Psychologists’ experiences of grief after client suicide: A qualitative study. OMEGA J. Death Dying 2011. [Google Scholar] [CrossRef]
- Davidsen, A.S. ‘And then one day he’d shot himself. Then I was really shocked’: General practitioners’ reaction to patient suicide. Patient Educ. Couns. 2011, 85, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.E. Korean teachers’ experience following student suicide: A phenomenological study. Crisis 2019. Advance online publication. [Google Scholar] [CrossRef] [PubMed]
- Matandela, M.; Matlakala, M.C. Nurses’ experiences of inpatients suicide in a general hospital. Health SA Gesondheid 2016, 21, 54–59. [Google Scholar]
- Saini, P.; Chantler, K.; While, D.; Kapur, N. Do GPs want or need formal support following a patient suicide?: A mixed methods study. Fam. Pract. 2016. [Google Scholar] [CrossRef] [PubMed]
- Sanders, S.; Jacobson, J.; Ting, L. Reactions of mental health social workers following a client suicide completion: A qualitative investigation. OMEGA 2005, 51, 197–216. [Google Scholar] [CrossRef]
- Tillman, J.G. When a patient commits suicide: an empirical study of psychoanalytic clinicians. Int. J. Psycho-Anal. 2006, 87, 159–177. [Google Scholar] [CrossRef] [PubMed]
- Ting, L.; Sanders, S.; Jacobson, J.M.; Power, J.R. Dealing with the aftermath: A qualitative analysis of mental health social workers’ reactions after a client suicide. Soc. Work. 2006, 51, 329–341. [Google Scholar] [CrossRef]
- Wang, S.; Ding, X.; Hu, D.; Zhang, K. A qualitative study on nurses’ reactions to inpatient suicide in a general hospital. Int. J. Nurs. Sci. 2016, 3, 354–361. [Google Scholar] [CrossRef]
- Major, C.M.; Savin-Baden, M. An Introduction to Qualitative Research Synthesis: Managing the Information Explosion in Social Science Research; Routledge: London, UK, 2010. [Google Scholar]
- Noblit, G.W.; Hare, R.D. Meta-Ethnography: Synthesizing Qualitative Studies; Sage: Los Angeles, CA, USA, 1988. [Google Scholar]
- Sandelowski, M.; Barosso, J. Handbook for Synthesizing Qualitative Research; Springer: New York, NY, USA, 2007. [Google Scholar]
- Tong, A.; Flemming, E.; McInnes, E.; Oliver, S.; Craig, J. Enhancing transparency in reporting the synthesis of qualitative research: ENTREQ. BMC Med. Res. Methodol. 2012, 12, 181. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, G.; The PRISMA Group. Preferred reporting items for systematic review and meta-analyses: The PRISMA Statement. PLoS Med 2009, 6. [Google Scholar] [CrossRef]
- Critical Appraisal Skills Programme. CASP Qualitative Checklist. Available online: https://casp-uk.net/casp-tools-checklists/ (accessed on 3 February 2018).
- Pearce-Smith, N. CASP Bibliography. Available online: https://casp-uk.net/wp-content/uploads/2018/01/CASP-Bibliography.pdf (accessed on 10 July 2019).
- Burnard, P. A method of analysing interview transcripts in qualitative research. Nurse Educ. Today 1991, 11, 461–466. [Google Scholar] [CrossRef]
- Davidsen, A. How does the general practitioner understand the patient? A qualitative study about psychological interventions in general practice. Psychol. Psychother. Res. Pract. 2009, 82, 199–217. [Google Scholar] [CrossRef]
- Colaizzi, P.F. Psychological research as the phenomenologist views it. In Existential-Phenomenological Alternatives for Psychology; Valle, R.S., King, M., Eds.; Oxford University Press: New York, NY, USA, 1978; pp. 48–71. [Google Scholar]
- Clark, J. The Taboo of Client Suicide: Silenced Therapist Narratives. Unpublished Doctoral Thesis. Available online: https://e-publications.une.edu.au/vital/access/manager/Repository/une:2734 (accessed on 7 February 2018).
- Cook, F.J. Key concepts in the national guidelines: “suicide exposure” and “levels of care”. Death Stud. 2017, 41, 680–684. [Google Scholar] [CrossRef]
- Mitchell, A.; Terhorst, L. PTSD symptoms in survivors bereaved by the suicide of a significant other. J. Am. Psychiatr. Nurses Assoc. 2017, 23, 61–65. [Google Scholar] [CrossRef]
- Malt, U.F.; Karlehagen, S.; Hoff, H.; Herrstromer, U.; Hildingson, K.; Tibell, E.; Leymann, H. The effect of major railway accidents on the psychological health of train drivers: Acute Psychological responses to accident. J. Psychosom. Res. 1993, 37, 793–805. [Google Scholar] [CrossRef]
- Cerel, J.; Jones, B.; Brown, M.; Weisenhorn, D.A.; Patel, K. Suicide exposure in law enforcement officers. Suicide Life-Threat. Behav. 2018. [Google Scholar] [CrossRef]
- British Association for Counselling and Psychotherapy. Ethical Framework for the Counselling Professions. Available online: https://www.bacp.co.uk/events-and-resources/ethics-and-standards/ethical-framework-for-the-counselling-professions/ (accessed on 7 July 2019).
- Testoni, I.; Francescon, E.; De Leo, D.; Santini, A.; & Zamperini, A. Forgiveness and blame among suicide survivors: A qualitative analysis on reports of 4-year self-help-group meetings. Community Ment. Health J. 2019, 55, 360–368. [Google Scholar] [CrossRef]
- Clarke, D.M. Autonomy, rationality and the wish to die. J. Med. Ethics 1999, 25, 457–462. [Google Scholar] [CrossRef]
- Séguin, M.; Bordeleau, V.; Drouin, M.-S.; Castelli-Dransart, D.A.; Glasson, F. Professionals’ reactions following a patient’s suicide: Review and future investigation. Arch. Suicide Res. 2014, 18, 340–362. [Google Scholar] [CrossRef]
- Maple, M.; McKay, K.; Hess, N.C.L.; Wayland, S.; Pearce, T. Providing support following exposure to sucide: A mixed methods study. Health Soc. Care Community 2018, 1–8. [Google Scholar] [CrossRef]
- Talseth, A.-G.; Gilje, F.L. Liberating burdensomeness of suicide survivorship loss: A critical interpretative synthesis. J. Clin. Nurs. 2017, 26, 3843–3858. [Google Scholar] [CrossRef] [PubMed]
- Public Health England., & National Suicide Prevention Alliance. Help Is at Hand: Support after Someone May Have Died by Suicide. Available online: https://www.nhs.uk/Livewell/Suicide/Documents/Help%20is%20at%20Hand.pdf (accessed on 22 July 2019).
- Public Health England. Support after A Suicide: A Guide to Providing Local Services: A Practical resource. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/590838/support_after_a_suicide.pdf. (accessed on 22 July 2019).
- Survivors of Suicide Loss Task Force. Responding to Grief, Trauma, & Distress after A Suicide: U.S. National Guidelines; National Action Alliance for Suicide Prevention: Washington, DC, USA, 2015. [Google Scholar]
- Dyregrov, K. What do we know about needs for help after suicide in different parts of the world? A phenomenological perspective. Crisis 2011, 32, 310–318. [Google Scholar] [CrossRef] [PubMed]
- Grad, O.T. Guidelines to Assist Clinical Staff after the Suicide of a Patient. Available online: https://www.iasp.info/pdf/postvention/guidelines_to_assist_clinical_staff_after_suicide_patient_grad.pdf (accessed on 1 September 2019).
- Juhnke, G.A.; Granello, P.F. Shattered dreams of professional competence: the impact of client suicides on mental health practitioners and how to prepare for it. J. Creat. Ment. Health 2005. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Author and Date | Location of Research | Participant Population and Number | Aim of Study | Data Collection | Data Analysis | Results/Findings |
|---|---|---|---|---|---|---|
| Bohan and Doyle (2008) [20] | Ireland | Psychiatric nurses on acute inpatient units within three large hospitals N = 9 | To describe psychiatric nurses’ experience of suicide and suicide attempts in an acute unit and explore their perceptions of the support they received after the incident. | Semi-structured interviews—audio taped and transcribed | Burnard’s [39] method of data analysis – detailed systematic description of themes. | Four themes: Nurses’ experiences of patient suicide/suicide attempts Nursing care following an incident of suicide/suicide attempt Feelings experienced by nurses following a suicide/suicide attempt Support for nurses following a suicide/suicide attempt |
| Christianson and Everall (2008) [21] | Canada | School Counsellors N = 7 | To gain an in-depth understanding of school counsellors experiences of client suicide from their perspective. | Telephone semi-structured interviews. Digitally recorded and transcribed. | Grounded Theory | Three themes related to training, resources and self-care: National training/practice standards Support resources Self care |
| Christianson and Everall (2009) [22] Reports the same study as Christian and Everall (2008) [21] | Canada | School Counsellors N = 7 | To explore the experiences of school counsellors who had lost clients to suicide. Qu’s = ‘What are school counsellors’ experiences of client suicide?’ ‘What impact do participants believe client suicide had on their lives?’ | Telephone interviews (geographically diverse population) – two interviews per participant. | Grounded Theory | Four themes: Taming the control beast Wearing the mask Interpreting the dance Staying in the game |
| Darden and Rutter (2011) [23] | US | Clinical Psychologists N = 6 | An in-depth exploration of the clinician’s experience in losing a client to suicide. | In-person semi-structured interview. | Consensual qualitative research (CQR) methods followed—themes, domains and categories. | Six domains: Psychologist’s view of suicide Clinical aspects of the case The suicide Impact Recovery Client’s Family |
| Davidsen (2010) [24] | Denmark | General Practitioners N = 1 4 | To investigate how GPs were affected by patients’ suicides and whether their reaction was linked to their inclination to explore suicide risk in the patient who died by suicide, and whether the GP’s current inclination to explore suicide risk has been influenced by their experience of a patient death by suicide. | Semi structured interviews—conducted as part of larger study (Davidsen, 2009) [40] | Interpretative Phenomenological Analysis (IPA) | Super-ordinate theme: patients’ suicides. Underlying themes: Emotional impact Self-scrutiny Talking about suicide |
| Kim (2019) [25] | Korea | School Teachers N = 5 | To explore the bereavement experiences of teachers and the challenges they face in coping with student suicide. | Semi-structured interviews | Colaizzi’s [41] Phenomenological approach | Four themes: Examination of the suicide Suspension of grief Tolerance of the suicide Renewed perception of role in preventing student suicide |
| Matandela and Matlakala (2016) [26] | South Africa | Nurses in General Hospital N = 6 | To present the experience of nurses who cared for patients who died by suicide while admitted in a general hospital | Interviews audio recorded and transcribed | Manual general qualitative content analysis. | Five themes: Experience of disbelief and helplessness Feelings of blame and condemnation Feelings of guilt and inadequacy Emotional reaction Fear of reprisal |
| Saini et al., (2016) [27] | England | General Practitioners N = 198 | To explore GPs views on how they are affected by a patient suicide and the formal support available to them following a patient suicide. | Semi-structured interviews, audio recorded and transcribed. | Descriptive statistics and a framework thematic approach | Three inter-related themes: Part and parcel Failing patients Informal support systems |
| Sanders et al., (2005) [28] | US | Mental Health Social Workers N = 145 Sample taken from a larger quantitative study—this sample being all participants who responded that they had experienced a completed client suicide. | To expand the understanding of the reactions of social workers to client suicide. Three research questions: 1. What professional and personal reactions do social workers experience immediately following a client suicide completion? 2. What professional and personal reactions do social workers experience long term, following a client suicide completion? 3. What is the relationship between time since the client suicide completion and the social workers’ reactions? The first two being relevant for this study. | Two open-ended questions at the end of a questionnaire. • Please describe how you felt in the seven days immediately following the client suicide. • Please describe how you feel now when you think about the client suicide. | Coding and constant comparative methods by two researchers working independently and comparing their results. Reviewed by third researcher. | Major themes immediately following client suicide: Deep sadness and depression Trauma and shock Feelings of professional failure Anger and Irritability Self blame Worries and Fear Major themes at time of survey: Continued emotional reactions Changes in practice Reconciliation Power and control issues Nothingness |
| Tillman (2006) [29] | US | Psychoanalysts/psychoanalytic psychotherapists N = 12 | Interview question: ‘I am conducting a study about the effect of patient suicide on clinicians; I am interested in how this event has affected you. Would you tell me, in as much detail as possible about you’re your experience?’ | Semi-structured interviews. Transcribed and audio recorded. | Coded by two researchers—using a psychoanalytic lens—‘a synthesis was made of the categories to arrive at a ‘best fit’ thematic analysis.’ | A research vignette is presented in the paper to ‘illustrate the depth and range of experiences reported by the clinicians’ Eight themes: Traumatic responses Affective responses Treatment specific relationship Relationships with colleagues Risk management Grandiosity, shame, humiliation, guilt, judgement, blame A sense of crisis Effect on work with other patients Sit within three domains Traumatic loss and grief Interpersonal relationships Professional identity concerns |
| Ting et al., (2006) [30] | US | Mental Health Social Workers N = 25 | What are the reactions experienced by a group of mental health social workers after a client suicide. | Semi-structured telephone interviews. Audio recorded and transcribed. | Constant comparative method with open coding. | Twelve Themes: Denial and Disbelief Grief and Loss Anger at client Agency and society Self-blame and guilt Professional failure and Incompetence Responsibility Isolation Avoidant behaviours Intrusion Change in professional behaviour changes in practice Changes in the professional environment Justification Acceptance |
| Wang et al., (2016) [31] | China | Nurses in a General Hospital N = 15 | To explore the impact of inpatient suicides on nurses working in front-line, the patterns of regulation and their needs for support. | Semi-structured in-depth interviews | Colaizzi’s seven-step phenomenological method by two interviewers. | Four ‘centre themes’ and associated ‘sub-themes’ were identified. Nurses’ cognition about inpatient suicide Inpatients are at a high risk of suicide Inpatient suicide is difficult to prevent Shortage of suicide preventing skills Psychological reaction Shock and panic Sense of fear Self-accusation or guilt Frustrated or self-doubt Impact on practice Stress Excessive vigilance Burnout Patterns of regulation Pouring out bitterness Avoidance |
| Category | Theme | Concept |
|---|---|---|
| Horror, Shock and Trauma | Witnessing suicide | The horror |
| In the moment responses | ||
| Shock and trauma | ||
| Responses to suicide | Loss and grief | |
| Mind and body responses | ||
| Dealing with suicide | Connections and closeness | |
| Absence and distance | ||
| The dual role | ||
| Scrutiny, Judgment and Blame | Thinking about responsibility | Am I responsible? |
| The un/expected death | ||
| Professional failure—guilt, reprisal and reputation | ||
| The autonomous client | ||
| Having to carry on | Aloneness | |
| Issues of control | ||
| Avoidance strategies | ||
| Hyper-vigilance | ||
| Dealing with others | The organization and colleagues | |
| The family | ||
| Cultural and social norms | ||
| Support, Learning and Living with | Experiences of support | |
| Learning | ||
| Living with |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Causer, H.; Muse, K.; Smith, J.; Bradley, E. What Is the Experience of Practitioners in Health, Education or Social Care Roles Following a Death by Suicide? A Qualitative Research Synthesis. Int. J. Environ. Res. Public Health 2019, 16, 3293. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16183293
Causer H, Muse K, Smith J, Bradley E. What Is the Experience of Practitioners in Health, Education or Social Care Roles Following a Death by Suicide? A Qualitative Research Synthesis. International Journal of Environmental Research and Public Health. 2019; 16(18):3293. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16183293
Chicago/Turabian StyleCauser, Hilary, Kate Muse, Jo Smith, and Eleanor Bradley. 2019. "What Is the Experience of Practitioners in Health, Education or Social Care Roles Following a Death by Suicide? A Qualitative Research Synthesis" International Journal of Environmental Research and Public Health 16, no. 18: 3293. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16183293