Evaluation of Public Health Emergency Management in China: A Systematic Review

Abstract
:1. Introduction
2. Materials and Methods
2.1. Document Inclusion and Exclusion Criteria
2.2. Inclusion Criteria
- Research object (sample): China Health Emergency Assessment Research.
- Research content (phenomenon of interest): explicitly mention health emergency assessment indicators and the health emergency assessment indicator system.
- Incorporate the research design (design): randomized controlled trial (RCT), non-randomized controlled trial (non-RCT), controlled trial (CBA), time series (interrupted) studies, and cross-sectional studies.
- Evaluation: the basic characteristics of China’s health emergency assessment indicator system and the main indictors according to laws and regulations and their application.
- Research Type: qualitative or quantitative research.
2.3. Exclusion Criteria
- Repeat published studies.
- Yearbooks, patents, conference abstracts, personal comments, letters, newspaper articles, work plans, and summaries.
- Theoretical research that only mentions the word “indicators of health emergency assessment” but has no specific evaluation index content or only partial evaluation indicators, epidemiological characteristic analysis, and epidemiological monitoring reports.
- There is no valid content literature, or the original language is from non-Chinese literature and the literature cannot be downloaded.
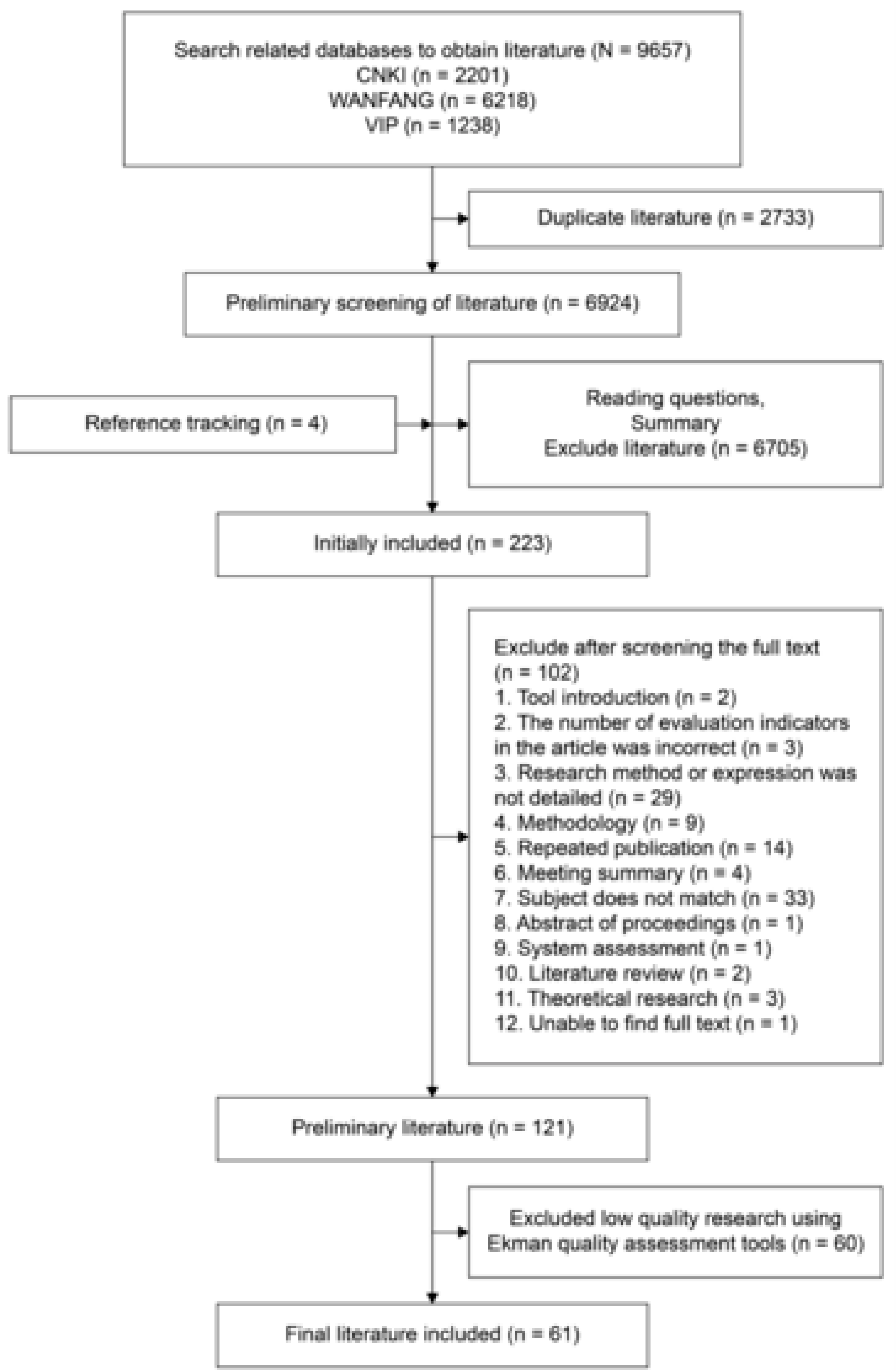
- Evaluation results fall within the scope of low quality research after using the Ekman quality assessment tool [1].
2.4. Literature Search Strategy
2.5. Literature Screening
2.6. Data Extraction
2.7. Quality Evaluation Criteria
2.8. Data Analysis
3. Results
3.1. Literature Screening
3.2. Basic Characteristics
3.3. Quality Evaluation
3.4. Dimensional Characteristics of Assessment System
3.5. Indicator Characteristics and Application of Assessment System
3.5.1. State and Health Administrative Department Assessment Research
3.5.2. Disease Prevention and Control Institutions Assessment Research
3.5.3. Health Institution Assessment Research
3.5.4. Health Supervision Agency Assessment Research
3.5.5. School Assessment Research
3.5.6. Military Assessment Research
3.5.7. Border Port Health and Quarantine Department Assessment Research
3.5.8. Health Emergency Assessment Practice Research
3.6. Legal and Policy Basis for the Evaluation System
4. Discussion
4.1. Wide Range of Assessments
4.2. Health Emergency Management Assessment Methods
4.3. Health Emergency Management Assessment Dimensions and Indicators Are Complex
4.4. Legal and Policy Basis Require Further Reinforcement
4.5. Relevance of Health Emergency Management Evaluation System
4.6. Need to Strengthen Practical Application of Assessment Systems
4.7. Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A. Representative Laws and Regulations, Policy Documents
- US CDC “Public Health Preparation and Response Capacity Scale”
- People’s Republic of China Law on the Prevention and Control of Infectious Diseases
- National Emergency Response to Public Health Incidents Plan
- Emergency Regulations for Public Health Emergencies
- National Health Emergency Response Survey and Evaluation Standards
- Ministry of Health, “National Health Emergency Basic Situation Investigation Plan”
- Emergency Management of Public Health Emergencies - Theory and Practice, Guangdong Health Emergency
- National Health Organization Health Emergency Work Regulations (Trial)
- National Health Control Organization Health Emergency Work Regulations (Trial)
- Disease Prevention and Control Center Performance Appraisal Operation Manual
References
- Ekman, B. Community-based health insurance in low-income countries: A systematic review of the evidence. Health Policy Plan. 2004, 19, 249–270. [Google Scholar] [CrossRef]
- Liang, Y.; Wang, X.N.; Guan, X.H.; Zheng, L.G.; Tong, Y.Q. Construction of evaluation index system for public health emergency preparedness capacity of provincial disease control institutions. Chin. Health Serv. Manag. 2017, 12, 888–891. [Google Scholar]
- Sun, G.Y.; Dong, A.P.; Zhou, J.; Wu, H.T.; Jin, Q.; Xing, Y.; Wang, C.P. Competency model construction of health emergency personnel based on exploratory factor analysis. Modern Prevent. Med. 2017, 44, 3154–3158. [Google Scholar]
- Zhang, H.W.; Li, F.K.; Wei, P.J. Evaluation of health emergency response capability of Xinjiang Production and Construction Corps. Bull. Dis. Cont. Prevent. 2016, 31, 86–87. [Google Scholar]
- Zhou, Z.H.; Wang, C.X.; Yu, C.Z.; Zheng, C.J.; Wang, J.J.; Liang, W.N. Assessment of the current situation of related emergency clinics and system setting of community medical institution in Guangdong province. Chin. Gen. Pract. 2014, 17, 2189–2192. [Google Scholar]
- Kang, J.; Zhao, Q.H. Weight analysis of evaluation factors in contingency plans to public health emergencies. J. Modern Med. Health 2013, 29, 2446–2448. [Google Scholar]
- Huang, G.M. Evaluation of Emergency Response Capability of Public Health Event for CDC at All Levels in Guangxi; Guangxi Medical University: Nanning, China, 2017. [Google Scholar]
- Cao, M.H.; Wu, J.B.; Zhang, J.; Chen, G.P.; Gong, L.; Hou, S. Evaluation of factor analysis model on capacity for health emergency at county-level in Anhui Province. Anhui J. Prev. Med. 2016, 22, 79–82. [Google Scholar]
- Zhou, X.Q.; Hu, Q.; Wang, P.; Kong, D.Q.; Jin, X.M. The public health emergency in Wuhan 2008-2012. Third-party assessment of virological characteristics and regulatory disposal. J. Prev. Med. Public Health 2013, 24, 122–124. [Google Scholar]
- Yang, X.M. The evaluation of social vulnerability and the analysis of influencing factors to major epidemics. Chin. Health Econ. 2013, 32, 51–53. [Google Scholar]
- Lin, L.; Li, Y.; Chi, X.W. Construction of evaluation index system for hospital nurses’ public health emergency response ability. Today Nurse 2016, 3, 1–2. [Google Scholar]
- Liu, Z.; Hao, X.N.; Bo, T.; Wu, J.; Xu, M.; Zhang, Z.Z.; Liu, J.C.; Xu, L.B.; Ta, N. The study on building the frame of public health emergencies monitoring and early-warning system with Delphi method. Chin. J. Health Policy 2013, 6, 46–52. [Google Scholar]
- Cui, N.; Sun, J.; Wang, Y.D.; Zhao, J.; Ding, L.; Liu, Y.Y.; Liang, W.N. Establishment of assessment index system for community health emergency plan. Chin. Gen. Pract. 2013, 16, 3293–3297. [Google Scholar]
- Zhang, L. A Study on the Capability Evaluation and Development Strategy of Health Emergency Rescue Team from Chinese People’s Armed Police Forces (PAPF); Academy of Military Medical Sciences: Beijing, China, 2015. [Google Scholar]
- Wang, M.L.; Hu, X.J.; Wang, Y.D.; Fu, C.; Cui, N.; Liu, Y.Y.; Sun, J.; Zhao, J.; Ding, L.; Yang, W.Z. The study of quality evaluation index system for health emergency management teaching case by grounded theory. Chin. Health Serv. Manag. 2014, 7, 531–533. [Google Scholar]
- Ning, N.; Wu, O.H.; Hao, Y.H.; Gao, L.J.; Kang, Z. Empirical study on emergency response capacity of county-level CDCs. Chin. Prev. Med. 2012, 13, 889–891. [Google Scholar]
- Song, T.; Dai, J.Y.; Wu, F.H.; Guo, R.N.; Liu, G.H.; Fang, Y.; Fu, J.H.; Yi, J.R. Assessment of CDC’s emergency capability with Delphi method and analytic hierarchy process. South China J. Prev. Med. 2014, 40, 1–6. [Google Scholar]
- Li, S.G. Evaluation on Public Health Emergency Capability of County-Level CDCs; Fudan University: Shanghai, China, 2012. [Google Scholar]
- Gan, Q.L.; Li, H.; Hu, M.H.; Wu, J.W. Evaluation and analysis on emergency practical exercises of county-level Centers for Disease Control and Prevention in Nanchang City. Occup. Health 2013, 29, 1668–1671. [Google Scholar]
- Wang, X.D.; Wu, Q.H.; Hao, Y.H.; Kang, Z.; Liang, L.B.; Chen, H.P. Study on the construction of the evaluation index system for public health emergency response capacity. Chin. Health Econ. 2013, 32, 47–50. [Google Scholar]
- Yu, E.M. A Preliminary Study of Early Precaution Indicator System for Influenza Outbreak; Zhengzhou University: Zhengzhou, China, 2012. [Google Scholar]
- Zhao, Q. Development and Application of Assessment Tools for Response Capacity of Public Health Emergency Response System and Exploratory Research of Capacity Assessment Models; Fudan University: Shanghai, China, 2009. [Google Scholar]
- Bo, T. The Theory and Evaluation Research on Emergency Response Capability for Public Health Incidents of CDC Institution; Shandong University: Jinan, China, 2009. [Google Scholar]
- Song, F. Military Response to Major Natural Disasters in the Health Emergency Capability Evaluation System Construction; SunYat-Sen University: Guangzhou, China, 2017. [Google Scholar]
- Qi, Y.B.; Chen, S.; Guo, H.; Hao, L.H.; He, J.B.; Peng, X. Assessment on health emergency response capability of CDC at county (district) level in Yunnan province. Chin. J. Public Health Manag. 2018, 34, 538–540. [Google Scholar]
- Feng, J.; Chen, Q.W.; Meng, X.H.; Luo, H.Y.; Li, Y.N.; Liu, D.C.; Feng, Q.M. Comprehensive evaluation of public health emergency response capacities of county-level hospitals in border areas of Guangxi. Chin. Health Serv. Manag. 2018, 11, 877–880. [Google Scholar]
- Chen, R.; He, Y.C.; Zhang, F.; Lu, Y.; He, Y. Establishing assessment indexes for emergency response capability of disease control and prevention institutions. Zhejiang Da Xue Xue Bao Yi Xue Ban 2018, 47, 137–142. [Google Scholar]
- Zhang, X.C.; Liu, T.T.; Wang, C.P.; Li, W.C.; Zhang, L.P. Application of data envelopment analysis in evaluating the allocation efficiency of health emergency manpower in centers for disease control and prevention. Chin. Health Resour. 2018, 21, 155–160. [Google Scholar]
- Li, D.; Zhang, H.X.; Wang, Y.B.; Wu, J. Establishment of a quantitative evaluation system for school public health emergency response capacity. South China J. Prevent. Med. 2018, 44, 59–62. [Google Scholar]
- Qiu, L.J.; Ma, G.F.; Zhang, X.W.; Ma, A.N.; Li, B.H.; Sheng, H.Q.; Zheng, W.G. Study on the Construction of the Evaluation Index System for Public Health Emergency Response Capacity in Rural Areas. Chin. Health Serv. Manag. 2018, 11, 801–804. [Google Scholar]
- Wei, Y.D.; Zhang, R.J.; Wang, J.; Wang, Z.; Liu, B.Y.; Zhang, X.H.; Xia, S.C. The comprehensive assessment for emergency response capacity of centers for disease control and prevention under the “New Normal”. Chin. Prevent. Med. 2017, 18, 827–831. [Google Scholar]
- Li, Z. An Evaluation Study on Primary Health Care Institutions’ Capacities in Public Health Emergency Preparedness in Border Areas with Minorities of Guangxi Province; Guangxi Medical University: Nanning, China, 2017. [Google Scholar]
- Yao, F.; Fu, L.Y.; Liu, C.Q.; Chen, H.C.; Wu, A.L. Study on vulnerability appraising of PHEIC at ports. Chin. Front. Health Quaran. 2016, 39, 433–436. [Google Scholar]
- Li, Z.; Chen, Q.W.; Feng, Q.M.; Luo, H.Y.; Liu, D.C.; Wei, B.; Wu, W.M.; Meng, X.H. Construction of evaluation index system for public health emergency response capacity of county-level health bureau in Guangxi. Chin. Prevent. Med. 2016, 17, 327–330. [Google Scholar]
- Lin, X.Q.; Lin, Z.B.; Huang, S.C.; Li, L.; Li, L.H.; Zhong, H.J.; Huang, Y.S.; Gan, R.H.; Wu, X.J.; Chen, Z.S.; et al. Double-blind emergency comprehensive drill mode for public health emergencies construction and practice. South China J. Prev. Med. 2016, 42, 188–191. [Google Scholar]
- Zhan, M.R.; Cai, S.J.; Chen, W.; Wu, S.G.; Hong, R.T. A comprehensive assessment of the managing of public health emergencies in Fujian in 2014. Chin. Prev. Med. 2016, 17, 288–291. [Google Scholar]
- Yu, J.P. Study on Evaluation of Effectiveness of the Hospital Emergency Rescue Plan-Take One Hospital in Tang Shan City for Example; North China University of Science and Technology: Tangshan, China, 2016. [Google Scholar]
- Huang, C.P.; Ding, H.; Song, S.J.; Xu, J.; Liu, M.W. Establishment of public health emergency work ability questionnaire. J. Occup. Environ. Med. 2015, 32, 528–534. [Google Scholar]
- Bian, L.L. Analysis of the evaluation of 2013 National Nuclear and Radiation Health Emergency Response team exercise. Chin. J. Disaster Med. 2014, 2, 330–332. [Google Scholar]
- Chen, H.P.; Hao, Y.H.; Wu, Q.H.; Liu, J.; Dong, X.; Wang, X.D. Establishment of comprehensive evaluation index system for impact assessment of public health emergency. Chin. J. Public Health 2013, 29, 628–631. [Google Scholar]
- Wang, W.N. Study on Evaluation of the Response to Public Health Emergencies Ability of F Hospital in Qiqihar; Harbin Engineering University: Harbin, China, 2013. [Google Scholar]
- Aiketaguli, W.E.J. Evaluation Index System of Emergency Capacity for Major Infectious Diseases Prevention and Control in Xinjiang Frontier Ports; Xinjiang Medical University: Wulumuqi, China, 2013. [Google Scholar]
- Xing, D.M. An Evaluation Study on Centers of Disease Control and Prevention in Communicable Diseases Control; Inner Mongolia University of Science and Technology Baotou Medical College: Baotou, China, 2013. [Google Scholar]
- Tan, Y.; Xia, M.; Luo, X.M.; Lu, J.J. Assessment on preparedness and response capability of emergent public health hazards in rural prevention and health care organizations. In Compilation of the Academic Annual Meeting of the Guangdong Preventive Medicine Association; Guang Dong Province Preventive Medicine Association China: Guangzhou, China, 2012; pp. 422–431. [Google Scholar]
- Wang, W.J. Analysis and Evaluation of Current Situation on Health Emergency in Qinghai Province; Shanxi Medical University: Taiyuan, China, 2012. [Google Scholar]
- Wu, C.R.; Hong, R.T.; Chen, W. Status quo and problems of performance evaluation of public health emergencies in Fujian province. Strait J. Prev. Med. 2012, 18, 80–82. [Google Scholar]
- Chen, H. Evaluation of Hospital Preparedness Capacity for Public Health Emergency in Digital Hospital of PLA; Third Military Medical University: Chongqing, China, 2011. [Google Scholar]
- Huang, X.M.; Dai, B. Establishment and application of township public health emergency response capability evaluation system. Chin. Health Serv. Manag. 2010, 9, 635–637. [Google Scholar]
- Zhang, W.S.; Zhang, Z.L.; Zhou, P. Selection of priority improvement indicators for emergency response capability of disease control institutions in Tianjin. Chin. J. Public Health Manag. 2009, 25, 467–468. [Google Scholar]
- Wang, H. Study on the Indexes System of Comprehensive Evaluation of the Social Mobilization in Public Health Emergencies; Shandong University: Jinan, China, 2009. [Google Scholar]
- Zhu, D.X. A Study on Hospitals’ Capacities Evaluation System in Public Health Emergency; Guangdong Pharmaceutical University: Guangzhou, China, 2009. [Google Scholar]
- Wu, X.J.; Wang, C.C.; Chen, W.L. Ability of military health service to handle sudden public health events exploration of its elements’ system. Mil. Med. Sci. 2006, 30, 457–460. [Google Scholar]
- Zhang, H. An Evaluation Study on Secondary and Tertiary Care Hospitals’ Capacities in Public Health Emergency Preparedness in Beijing, China; Peking Union Medical College: Beijing, China, 2006. [Google Scholar]
- Zhu, X. Capacities Assessment of Response Public Health Emergencies in the Field of County Disease Prevention and Control Organs in Luoyang City; Shandong University: Jinan, China, 2005. [Google Scholar]
- Chang, Y.B. Evaluation of Emergency Response Capability for Public Health Events of CDC at Provincial Cities in Henan Province; Zhengzhou University: Zhengzhou, China, 2014. [Google Scholar]
- Tan, Y. An Evaluation Study and Application on Response Capacity of Emergent Public Health Hazards in Rural Prevention and Health Care Organization; Sun Yat-Sen University: Guangzhou, China, 2010. [Google Scholar]
- Dai, R. A Study on Evaluation of Response Capacity for Public Health Emergencies at District Level; SunYat-Sen University: Guangzhou, China, 2010. [Google Scholar]
- Dai, J.Y. Cross-Sectional Investigation of Emergency Response Capability for Public Health Events of CDC at All Levels in Guangdong Province; SunYat-Sen University: Guangzhou, China, 2006. [Google Scholar]
- Sun, H.Y.; Zhao, M.Y. A study on evaluation index system for district-level public health emergency response core competency. Chin. Health Resour. 2017, 20, 178–181. [Google Scholar]
- Wang, C.N.; Mi, Y.P.; Yang, J.; Wang, Z.F. Analysis on International Health Regulations (2005) public health emergency core capacity for health departments in China. Chin. J. Health Policy 2014, 7, 56–61. [Google Scholar]
- Hu, G.Q. Study on the Assessment System of Preparedness and Response Capacity for Public Health Emergencies in China; Central South University: Changsha, China, 2006. [Google Scholar]


{kind=link}
| Database | Literature Search Strategy |
|---|---|
| CNKI | |
| #1 | SU = “health emergency” |
| #2 | SU = “public health emergency” |
| #3 | SU = “health and epidemic prevention” |
| #4 | SU = “assessment” |
| #5 | SU = “evaluation” |
| #6 | SU = “monitor” |
| #7 | SU = “performance” |
| #8 | (#1 OR #2 OR #3)AND(#4 OR #5 OR #6 OR #7) |
| WANFANG | |
| #1 | theme:(health emergency) |
| #2 | theme:(public health emergency) |
| #3 | theme:(health and epidemic prevention) |
| #4 | theme:(assessment) |
| #5 | theme:(evaluation) |
| #6 | theme:(monitor) |
| #7 | theme:(performance) |
| #8 | (#1 OR #2 OR #3)AND(#4 OR #5 OR #6 OR #7) |
| VIP | |
| #1 | M = health emergency |
| #2 | M = public health emergency |
| #3 | M= health and epidemic prevention |
| #4 | M = assessment |
| #5 | M = evaluation |
| #6 | M = monitor |
| #7 | M = performance |
| #8 | (#1 OR #2 OR #3)AND(#4 OR #5 OR #6 OR #7) |
| Ekman Quality Evaluation Score | Study |
|---|---|
| 3: 16–0 | None |
| 2: 21–17 | 1 [25], 2 [26], 3 [27], 4 [2], 5 [28], 6 [29], 7 [30], 8 [31], 9 [32], 10 [7], 11 [3], 12 [33], 13 [34], 14 [4], 15 [35], 16 [8], 17 [36], 18 [11], 19 [37], 20 [38], 21 [14], 22 [15], 23 [5], 24 [39], 25 [17], 26 [12], 27 [13], 28 [6], 29 [19], 30 [9], 31 [20], 32 [10], 33 [40], 34 [41], 35 [42], 36 [43], 37 [44], 38 [16], 39 [45], 41 [21], 42 [46], 43 [47], 44 [48], 45 [49], 47 [22], 48 [50], 49 [23], 50 [51], 51 [52], 52 [53], 54 [54], 55 [55], 56 [56], 57 [57], 58 [58], 59 [24], 60 [59], 61 [60] |
| 1: 25–22 | 40 [18], 46 [22], 53 [61] |
| No | Indicator System Name (Build System/Application Existing System) | Number of Dimensions | Number of Indicators | Composition of Primary Indicators |
|---|---|---|---|---|
| 1 | Disease control agency health emergency capacity evaluation index. | 1 | 11 | number of drills, number of participants, number of teams, number of senior titles in team, number of trainings, training participants, number of vehicles, protective materials, sanitation disposal state, special funds, communication equipment. |
| 2 | Evaluation index for public health emergency response capacity of township hospitals. | 2 | 15 | planning, monitoring, early warning, and service capabilities. |
| 3 | Disease control agency health emergency capacity assessment index. | 3 | 115 | system construction, team building, monitoring and early warning capabilities, response capabilities, support capabilities, and information communication and departmental collaboration, research, and cooperation and communication capabilities. |
| 4 | Public health emergency preparedness assessment index for provincial Center for Disease Control (CDC). | 2 | 59 | emergency management and coordination, risk monitoring and information management, reserve materials, site disposal, detection, and safety protection. |
| 5 | Human resource allocation efficiency evaluation index. | 3 | 24 | number of employees in the organization, proportion of employees with undergraduate degrees or greater, and emergency knowledge training participation rate in past three years. |
| 6 | Quantitative evaluation of overall school response capabilities to public health emergencies. | 3 | 49 | pre-preparation, event discovery, event handling, and post-recovery abilities. |
| 7 | Evaluation index of rural grassroots emergency response capability to public health emergencies. | 3 | 74 | human, financial, material, information, and technical resources, and population health levels. |
| 8 | Comprehensive evaluation of emergency response capabilities of disease prevention and (disaster) control institutions in Zhejiang (county). | 3 | 106 | system construction, team construction, support, response, monitoring, and early warning, scientific research and cooperation and communication, information communication and departmental collaboration capabilities. |
| 9 | Comprehensive evaluation model of county general hospitals response capabilities to public health emergencies. | 2 | 37 | command coordination, emergency plan, monitoring and early warning capability, information report exchange, emergency personnel, emergency beds, and material reserve. |
| Comprehensive evaluation model of township hospitals response capabilities to public health emergencies. | 2 | 15 | emergency documents, emergency monitoring, and capacity building. | |
| 10 | Guangxi CDC Public Health Emergency Response Capability Evaluation Index. | 3 | 79 | emergency organization system, emergency team construction, monitoring and early warning capability, actual emergency response capability, emergency protection, information communication, and departmental collaboration capabilities. |
| 11 | Shanghai Urban Health Emergency Core Competency Evaluation Index. | 2 | 41 | organizational command, work norms, emergency teams, equipment reserves, training drills, monitoring and early warning capability, publicity and education, laboratory energy, and force and emergency response. |
| 12 | Multi-criteria crisis early warning extension model (based on Public Health Emergency of International Concern (PHEIC) subject vulnerability assessment). | 2 | 16 | disaster response, population, environmental, and safety measure risk factors. |
| 13 | Guangxi county-level health and family planning bureau response capacity for public health emergencies. | 2 | 30 | emergency management and command, monitoring and early warning capability, information reporting, on-site disposal and personnel, material reserves and exercises, and recovery and evaluation. |
| 14 | National Health and Family Planning Commission, Health Assessment Capacity Assessment Standard. | 1 | 8 | system construction, emergency team, equipment reserves, training drills, mission research, monitoring and early warning capability, emergency response, and after-care assessment. |
| 15 | Self-made drill evaluation index. | 2 | 27 | pre-rescue preparation, epidemic situation verification and consultation, on-site investigation, laboratory testing, epidemic control, risk communication and health education, and emergency termination and summary report. |
| 16 | National Health Emergency Response Survey and Evaluation Standards. | 1 | 8 | system construction, emergency team, equipment reserve, training drill, mission research, monitoring and early warning capability, emergency response, and aftercare assessment |
| 17 | Public Health Emergency Report Management Information System. | 1 | 7 | number of public health emergencies, county reporting rate, monitoring sensitivity, timeliness of reporting, control effects, integrity rate, and accuracy. |
| 18 | Comprehensive evaluation index of hospital nurses’ ability to respond to public health emergencies. | 2 | 24 | basic information, professional background, knowledge system, and practical skills. |
| 19 | Tertiary hospitals’ emergency rescue plan effectiveness evaluation index. | 2 | 21 | plan integrity, operability, efficiency, flexibility, sociality, and plan management. |
| 20 | Public Health Emergency Work Ability Questionnaire. | 2 | 25 | work capacity self-evaluation, professional knowledge training effect, work capacity constraints, factors improvement, and work ability prediction. |
| 21 | Construction of an evaluation system and development of software for the evaluation index of the capacity of the armed police unit’s health emergency rescue team. | 3 | 65 | including organizational command, emergency maneuver, injury and treatment, medicinal materials protection, classified and sent, epidemic prevention and anti-health preservation. |
| 22 | Indicator system for health emergency teaching case evaluation. | 3 | 47 | including material value dimension, structure value dimension, practical value dimension and literary value dimension. |
| 23 | Community Medical Institutions Health Emergency Capability Survey and Evaluation Form in Guangdong Province. | 2 | 34 | condition of community medical institutions, community health human resources, health emergency related personnel and department setting, health emergency related work system, and health emergency plan construction. |
| 24 | 2013 National Nuclear and Radiation Emergency Health Emergency Team Exercise Evaluation System. | 2 | 35 | program development, exercise preparation, on-site drills, and summary assessment. |
| 25 | Emergency response capability evaluation index system for disease control institutions in Guangdong Province. | 3 | 92 | emergency management system construction, emergency human resources, monitoring and early warning capabilities, emergency response capabilities, laboratory testing capabilities, emergency support capabilities, training and drills, and health education and media communication. |
| 26 | Tertiary monitoring and early warning system framework. | 3 | 62 | including monitoring system, risk assessment system, early warning system, and system guarantee. |
| 27 | Index system for evaluation of community health emergency plan. | 3 | 63 | structure, process, and results. |
| 28 | Emergency plan for public health emergencies. | 1 | 7 | time factors, personnel loss factors, economic loss factors, social impact factors, resource consumption factors, transportation and security factors, and program dynamic adjustable factors. |
| 29 | Evaluation of emergency drill activities of county-level disease control institutions in Nanchang City. | 1 | 4 | program development, exercise preparation, on-site drills, and summary assessment. |
| 30 | Disease Prevention and Control Work Performance Assessment Operation Manual (2009 Edition). | 1 | 6 | event report, event confirmation, event preparation, event site disposal, control measures implementation, and summary assessment. |
| 31 | Emergency evaluation index system for public health emergencies. | 3 | 72 | preparation stage evaluation, monitoring and early warning stage evaluation, response process evaluation, and post-event evaluation. |
| 32 | Constructing a social vulnerability assessment function for sudden epidemics of major infectious diseases. | 2 | 14 | social system vulnerability and social system resilience. |
| 33 | Comprehensive evaluation index system for the impact of public health emergencies. | 3 | 75 | health effects, economic impact, and social impact. |
| 34 | Hospital emergency ability evaluation index system. | 3 | 56 | emergency system, emergency agencies, monitoring and early warning of public health emergencies, on-site rescue and medical treatment, logistics support, emergency training and drills, and public education. |
| 35 | Comprehensive Evaluation Model of Xinjiang Frontier Ports’ Emergency Response Capability for Major Infectious Diseases. | 3 | 101 | basic conditions, emergency response system, monitoring and early warning capability, emergency support, laboratory capabilities, on-site disposal capabilities, information network systems, training, and exercises. |
| 36 | Disease Prevention and Control Center Infectious Disease Prevention and Control Capability Evaluation Index System. | 2 | 61 | comprehensive guarantees, immunization prevention, infectious disease emergency plans and drills, infectious disease monitoring, on-site disposal capabilities, information analysis and utilization, laboratory capabilities, publicity and education, and training. |
| 37 | Grassroots preventive health care centers emergency response capacity evaluation index. | 2 | 29 | organization management, technology implementation, resource reservation, monitoring and early warning, coordination, and cooperation. |
| 38 | County-level disease prevention and control institution emergency capability evaluation. | 2 | 15 | emergency preparedness, monitoring and reporting, emergency response, after-treatment, and integration. |
| 39 | Main indicators reflecting the emergency response capacity of health institutions at all levels. | 1 | 15 | number of institutional staff, emergency team count, number of emergency team members, number of senior members among emergency team members, simulation exercises, number of times, number of training courses in unit, number of participants in training class, number of participants in emergency training, number of emergency special vehicles, number of emergency on-site inspection vehicles, value of physical reserves, daily work expenses of the emergency department, annual emergency budget reserve, total number of beds (health institutions), and number of emergency beds. |
| 40 | County-level CDC emergency public health emergency response capability evaluation index system. | 3 | 31 | resource allocation, capacity building, and function implementation. |
| 41 | Influenza outbreak early warning indicator system suitable for China’s national conditions. | 3 | 36 | pre-emergency, atypical symptoms, and typical symptom. |
| 42 | According to the Ministry of Health, December 2008, the basics of disease prevention and control institutions at all levels. Responsibilities and Disease Surveillance Control Performance Evaluation Standards. | 1 | 5 | completion rate of the plan system, simulation exercise index, reserve rate of emergency items, standard disposal index, and event investigation rate. |
| 43 | Digital hospital emergency public health response capacity evaluation index. | 3 | 82 | emergency system, monitoring and early warning, medical treatment inside and outside the hospital, emergency reserve, personnel and equipment safety, education, and improvement. |
| 44 | Township public health emergency response evaluation system. | 3 | 72 | regional socio-economic population status, public health emergency basic support capacity, disease prevention and control, and health emergency business development level. |
| 45 | Tianjin City and County Disease Control Agency Emergency Capability Priority Improvement Indicators. | 2 | 27 | organizational management, material resources, information management, and professional skills. |
| 46 | Assessment of suitability of China’s existing emergency response capability system evaluation framework and index system. | 2 | 37 | primary disease prevention and control center: plans, monitoring, laboratories, manpower, information, training, disposal, and reserves. |
| 2 | 36 | county-level general hospitals: documents, monitoring, laboratories, manpower, information, training, emergency, and reserves. | ||
| 2 | 15 | township hospitals: documentation, monitoring, and capacity building. | ||
| 47 | Comprehensive evaluation index of social mobilization apparatus for public health emergencies. | 3 | 59 | domestic unified command, mobilization of other social resources, human mobilization, information culture mobilization, material mobilization, and economic mobilization. |
| 48 | Constructing hospital emergency response evaluation index. | 3 | 56 | emergency system, emergency agencies, monitoring and early warning of public health emergencies, on-site rescue and medical treatment, logistics support, emergency training and drills, public awareness, and education. |
| 49 | Evaluation of emergency capability evaluation system. | 2 | 29 | including forecasting and early warning capabilities, technology implementation capabilities, resource reserve capacity, operational management capabilities, and access to foreign aid. |
| 50 | Network Quality Evaluation Index for Public Health Reports. | 2 | 16 | report timeliness, report integrity, report accuracy, and disposal effectiveness. |
| 51 | Components of the military health response capability for public health emergencies index. | 3 | 71 | organizational command capability, disease prevention and control capabilities, medical treatment capabilities, and support capabilities. |
| 52 | Hospital Coping Ability Evaluation Index System. | 2 | 53 | emergency command coordination mechanism, emergency plan, monitoring and early warning capability, laboratory management and diagnosis, information report exchange, emergency personnel, emergency bed, emergency drug reserve, medical treatment measures, and disinfection and purification. |
| 53 | A comprehensive assessment tool of the ability of all provinces, autonomous regions (municipalities)/prefectures (states) to respond to public health emergencies. | 2 | 214 | command coordination and evaluation, preparation of emergency plans for public health emergencies, training and exercises, risk identification, assessment, and mitigation, monitoring, early warning, epidemiological investigation and response capabilities, laboratory testing, on-site first aid and medical treatment, information reporting, communication, and dissemination, logistics support, public education, and personnel training. |
| 54 | Evaluation Index for Emergency Treatment of Sudden Epidemic Event in Luoyang City. | 2 | 14 | epidemic situation detection, epidemic response, on-site investigation, on-site treatment, and epidemic event. |
| 55 | Henan Province Municipal-level CDC’s assessment system for public health emergencies. | 3 | 66 | basic conditions, system construction, monitoring and early warning, on-site disposal, assessment, safeguard measures, and education and training. |
| 56 | Grassroots preventive health care center emergency response capacity and evaluation index. | 2 | 29 | organization management, technology implementation, resource reserve, monitoring and early warning capability, coordination and cooperation. |
| 57 | District-level public health emergency response capability assessment index: (i) The health administrative department evaluation system. | 2 | 54 | organizational command, emergency work management system, monitoring and early warning capability, information reporting and release, on-site disposal, emergency team, equipment reserve, training drill, mobilization propaganda, scientific and technological exchanges, and co-operation, recovery, reconstruction, and response assessment. |
| (ii) The disease prevention and control institution evaluation system. | 2 | 45 | organizational command, emergency work management system, monitoring and early warning, information reporting and release, on-site disposal, laboratory capabilities, equipment reserve, training drills, mobilization publicity, and technology exchange and cooperation. | |
| (iii) The medical institution evaluation system. | 2 | 23 | organizational command, emergency work management system, monitoring and early warning capability, information reporting and release, on-site disposal, equipment reserve, training drills, scientific and technological exchange (and cooperation). | |
| 2 | 14 | organizational command, emergency work management system, information reporting and release, on-site disposal, equipment reserve, and training drills. | ||
| 58 | Emergency capability survey indicator system. | 2 | 38 | basic personnel conditions, emergency management mechanism, monitoring and early warning, on-site investigation and handling, laboratory testing, emergency materials reserve, staff training drills, and public information and information channels. |
| 59 | The index system of the military’s ability to respond to major natural disasters’ health emergency support capabilities. | 3 | 48 | organizational command capability, medical rescue capability, professional strength construction, and service support capability. |
| 60 | Competency model of health emergency personnel in county-level disease control institutions. | 1 | 4 | personal characteristics, basic knowledge, emergency knowledge concepts, and emergency skills. |
| 61 | China’s health sector International Health Regulations (IHR) (2005) analysis of the standard of public health emergency core competency. | 2 | 59 | monitoring description, response, risk communication, preparation, infection control, laboratory capabilities, and material and financial support. |
| Institution Category | Most Frequent Indicators | Number of Indicators | Application |
|---|---|---|---|
| State and health administrative department | Management capabilities, improvement capabilities, drill capabilities, reporting capabilities, system construction, monitoring capability, material reserve capability, training capability, early warning capability, social mobilization capability, site disposal capability, risk assessment. | 12 | District Health Emergency Capability Survey and Evaluation (Shanghai). Township Public Health Emergency Response Assessment (Sichuan Province). Evaluation of the ability of public health emergency response in a province/autonomous region/municipality directly under the central government (National). District-level public health emergency response capacity assessment (Guangdong Province). |
| Disease prevention and control institutions | Technical expertise, management capabilities, response capabilities, participation capabilities, response capabilities, monitoring capabilities, alert capabilities, response capacity, drill capability, materials reserve support capability, training capability, system construction, cooperation capability, team-building capability. | 14 | City CDC and District Center for Disease Control and Prevention Health Assessment Capacity Assessment (Shanghai). Evaluation of relative efficiency of health emergency human resource allocation in county and district CDCs (Shandong Province). City and county-level disease prevention and control centers to respond to public health emergencies (Guangxi Zhuang Autonomous Region). Municipal disease prevention and control agency emergency capability assessment (Guangdong Province). Evaluation of infectious disease prevention and control capability of municipal and county-level disease prevention and control centers (Inner Mongolia Autonomous Region). Evaluation of public health emergency response capability in district and township defense offices (Guangdong Province). County-level CDC emergency public health emergency response capability evaluation (national). City district-level disease prevention and control center emergency public health emergency response capability evaluation (Shandong Province). County-level disease prevention and control agency/epidemic station emergency public health incident on-site emergency response capability evaluation (Henan Province). City-level disease prevention and control center emergency public health emergency response capability evaluation (Henan Province). Evaluation of public health emergency response capacity of district and township preventive health care centers (Guangdong Province). Municipal, county-level disease prevention and control center (Guangdong Province). |
| Medical institutions | Monitoring capability, plan capability, material reserve, training, early warning, management command, information monitoring report, system, personnel, medical technology, education, laboratory, medical treatment, bed, logistics support, communication, on-site disposal, drills. | 18 | County general hospital and township health center (Guangxi Zhuang Autonomous Region). Top three hospitals (Hebei Province). Hospital (Heilongjiang Province). Basic-level emergency public health emergency response assessment (national). Secondary hospitals (Beijing). |
| Health supervision agencies | Organizational command, management system, equipment reserve, training drill, response. | 5 | District Health Emergency Capability Survey and Evaluation (Shanghai). District-level public health emergency response capacity assessment (Guangdong Province). |
| Schools | Value education, preparation and recovery, detection and monitoring, response, materials learning. | 5 | No. |
| Military | Command capability, support capability, equipment and other reserve capability, system construction, response capacity, monitoring capability, medical treatment capacity, early warning capability, education, control capability, service capability, survival capability, team construction, response capability, research capability, drill, rescue capability, mission, medicine reserve. | 19 | Digital hospitals (all military). |
| Border port health and quarantine department | Vulnerability, environment, system construction, laboratory construction, network construction, drill, support, on-site disposal measures, monitoring, training, warning. | 11 | Xinjiang border port. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, J.; Yuan, B.; Li, Z.; Wang, Z. Evaluation of Public Health Emergency Management in China: A Systematic Review. Int. J. Environ. Res. Public Health 2019, 16, 3478. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16183478
Wang J, Yuan B, Li Z, Wang Z. Evaluation of Public Health Emergency Management in China: A Systematic Review. International Journal of Environmental Research and Public Health. 2019; 16(18):3478. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16183478
Chicago/Turabian StyleWang, Jia, Beibei Yuan, Zhengmao Li, and Zhifeng Wang. 2019. "Evaluation of Public Health Emergency Management in China: A Systematic Review" International Journal of Environmental Research and Public Health 16, no. 18: 3478. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16183478