Effects of Traditional vs. iPad-Enhanced Aerobic Exercise on Wayfinding Efficacy and Cognition: A Pilot Randomized Controlled Trial

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
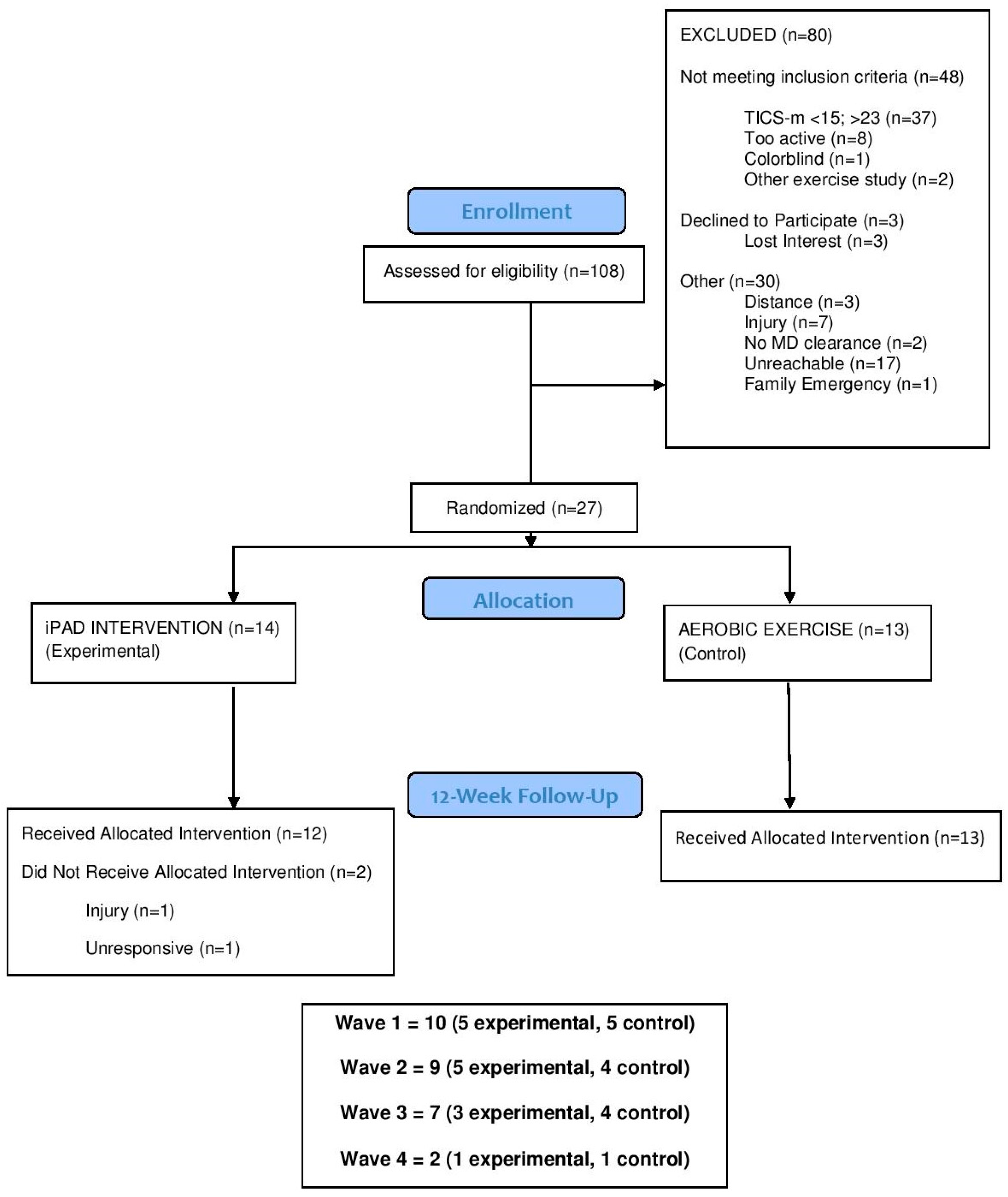
2.1. Participants & Procedure
2.2. Exercise Protocol for All Participants
2.3. Intervention Conditions
2.3.1. iPad-Enhanced Aerobic Exercise Condition (Experimental Group)
2.3.2. Aerobic Exercise-Only Condition (Control Group)
2.4. Primary Outcomes
2.4.1. Wayfinding Self-Efficacy
2.4.2. Wayfinding Task
2.5. Secondary Outcomes
2.5.1. Executive Function
2.5.2. Strategic Processing Task
2.5.3. Spatial Memory
2.5.4. Exercise Effort, Engagement, Attentional Focus and Affect
2.5.5. Physical Activity and Mobility
2.6. Statistical Analyses
3. Results
3.1. Feasibility and Acceptability
3.2. Primary Outcomes
3.3. Secondary Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Vandenberg, A.E. Human Wayfinding: Integration of Mind and Body. In Community Wayfinding: Pathways to Understanding; Springer: Berlin/Heidelberg, Germany, 2016; pp. 17–32. [Google Scholar]
- Spiers, H.J.; Maguire, E.A. The dynamic nature of cognition during wayfinding. J. Environ. Psychol. 2008, 28, 232–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mullen, S.P.; Palac, D.E.; Bryant, L.L. Maps to apps: Evaluating Wayfinding Technology. In Community Wayfinding: Pathways to Understanding; Springer: Berlin/Heidelberg, Germany, 2016; pp. 137–151. [Google Scholar]
- Passini, R. Wayfinding: A conceptual framework. Urban. Ecol. 1981, 5, 17–31. [Google Scholar] [CrossRef]
- Chebat, J.-C.; Gélinas-Chebat, C.; Therrien, K. Lost in a mall, the effects of gender, familiarity with the shopping mall and the shopping values on shoppers’ wayfinding processes. J. Bus. Res. 2005, 58, 1590–1598. [Google Scholar] [CrossRef]
- Taillade, M.; Sauzéon, H.; Dejos, M.; Arvind Pala, P.; Larrue, F.; Wallet, G.; Gross, C.; N’Kaoua, B. Executive and memory correlates of age-related differences in wayfinding performances using a virtual reality application. Aging Neuropsychol. Cogn. 2013, 20, 298–319. [Google Scholar] [CrossRef] [PubMed]
- Taillade, M.; Sauzéon, H.; Pala, P.A.; Déjos, M.; Larrue, F.; Gross, C.; N’Kaoua, B. Age-related wayfinding differences in real large-scale environments: Detrimental motor control effects during spatial learning are mediated by executive decline? PLoS ONE 2013, 8, e67193. [Google Scholar] [CrossRef] [PubMed]
- Poranen-Clark, T.; von Bonsdorff, M.B.; Rantakokko, M.; Portegijs, E.; Eronen, J.; Pynnönen, K.; Eriksson, J.G.; Viljanen, A.; Rantanen, T. The temporal association between executive function and life-space mobility in old age. J. Gerontol. Ser. A 2017, 73, 835–839. [Google Scholar] [CrossRef] [PubMed]
- Wiener, J.M.; Kmecova, H.; de Condappa, O. Route repetition and route retracing: Effects of cognitive aging. Front. Aging Neurosci. 2012, 4, 7. [Google Scholar] [CrossRef] [PubMed]
- Petersen, R.C.; Caracciolo, B.; Brayne, C.; Gauthier, S.; Jelic, V.; Fratiglioni, L. Mild cognitive impairment: A concept in evolution. J. Intern. Med. 2014, 275, 214–228. [Google Scholar] [CrossRef]
- Keynejad, R.C.; Marková, H.; Šiffelová, K.; Kumar, N.; Vlček, K.; Laczó, J.; Migo, E.M.; Hort, J.; Kopelman, M.D. Spatial navigation deficits in amnestic mild cognitive impairment with neuropsychiatric comorbidity. Aging Neuropsychol. Cogn. 2018, 25, 277–289. [Google Scholar] [CrossRef]
- Peter, J.; Sandkamp, R.; Minkova, L.; Schumacher, L.V.; Kaller, C.P.; Abdulkadir, A.; Klöppel, S. Real-world navigation in amnestic mild cognitive impairment: The relation to visuospatial memory and volume of hippocampal subregions. Neuropsychologia 2018, 109, 86–94. [Google Scholar] [CrossRef]
- Ruggiero, G.; Iavarone, A.; Iachini, T. Allocentric to egocentric spatial switching: Impairment in aMCI and Alzheimer’s Disease patients? Curr. Alzheimer Res. 2018, 15, 229–236. [Google Scholar] [CrossRef] [PubMed]
- Satariano, W.A.; Guralnik, J.M.; Jackson, R.J.; Marottoli, R.A.; Phelan, E.A.; Prohaska, T.R. Mobility and aging: New directions for public health action. Am. J. Public Health 2012, 102, 1508–1515. [Google Scholar] [CrossRef] [PubMed]
- Onen, F.; Henry-Feugeas, M.C.; Roy, C.; Baron, G.; Ravaud, P. Mobility decline of unknown origin in mild cognitive impairment: An MRI-based clinical study of the pathogenesis. Brain Res. 2008, 1222, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Pettersson, A.; Olsson, E.; Wahlund, L.-O. Motor function in subjects with mild cognitive impairment and early Alzheimer’s disease. Dement. Geriatr. Cogn. Disord. 2005, 19, 299–304. [Google Scholar] [CrossRef] [PubMed]
- Mullen, S.P.; McAuley, E.; Satariano, W.A.; Kealey, M.; Prohaska, T.R. Physical activity and functional limitations in older adults: The influence of self-efficacy and functional performance. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2012, 67, 354–361. [Google Scholar] [CrossRef] [PubMed]
- Peel, C.; Baker, P.S.; Roth, D.L.; Brown, C.J.; Bodner, E.V.; Allman, R.M. Assessing mobility in older adults: The UAB Study of Aging Life-Space Assessment. Phys. Ther. 2005, 85, 1008–1019. [Google Scholar]
- Curcio, C.-L.; Alvarado, B.E.; Gomez, F.; Guerra, R.; Guralnik, J.; Zunzunegui, M.V. Life-Space Assessment scale to assess mobility: Validation in Latin American older women and men. Aging Clin. Exp. Res. 2013, 25, 553–560. [Google Scholar] [CrossRef]
- Portegijs, E.; Rantakokko, M.; Mikkola, T.M.; Viljanen, A.; Rantanen, T. Association between physical performance and sense of autonomy in outdoor activities and life-space mobility in community-dwelling older people. J. Am. Geriatr. Soc. 2014, 62, 615–621. [Google Scholar] [CrossRef]
- Portegijs, E.; Iwarsson, S.; Rantakokko, M.; Viljanen, A.; Rantanen, T. Life-space mobility assessment in older people in Finland; measurement properties in winter and spring. BMC Res. Notes 2014, 7, 323. [Google Scholar] [CrossRef]
- Lo, A.X.; Brown, C.J.; Sawyer, P.; Kennedy, R.E.; Allman, R.M. Life-space mobility declines associated with incident falls and fractures. J. Am. Geriatr. Soc. 2014, 62, 919–923. [Google Scholar] [CrossRef]
- Lautenschlager, N.T.; Cox, K.L.; Flicker, L.; Foster, J.K.; van Bockxmeer, F.M.; Xiao, J.; Greenop, K.R.; Almeida, O.P. Effect of physical activity on cognitive function in older adults at risk for Alzheimer disease: A randomized trial. J. Am. Med. 2008, 300, 1027–1037. [Google Scholar] [CrossRef]
- Kramer, A.F.; Erickson, K.I. Capitalizing on cortical plasticity: Influence of physical activity on cognition and brain function. Trends Cogn. Sci. 2007, 11, 342–348. [Google Scholar] [CrossRef] [PubMed]
- Ströhle, A.; Schmidt, D.K.; Schultz, F.; Fricke, N.; Staden, T.; Hellweg, R.; Priller, J.; Rapp, M.A.; Rieckmann, N. Drug and exercise treatment of Alzheimer disease and mild cognitive impairment: A systematic review and meta-analysis of effects on cognition in randomized controlled trials. Am. J. Geriatr. Psychiatry 2015, 23, 1234–1249. [Google Scholar] [CrossRef] [PubMed]
- Gates, N.; Singh, M.A.F.; Sachdev, P.S.; Valenzuela, M. The effect of exercise training on cognitive function in older adults with mild cognitive impairment: A meta-analysis of randomized controlled trials. Am. J. Geriatr. Psychiatry 2013, 21, 1086–1097. [Google Scholar] [CrossRef] [PubMed]
- Hillman, C.H.; Erickson, K.I.; Kramer, A.F. Be smart, exercise your heart: Exercise effects on brain and cognition. Nat. Rev. Neurosci. 2008, 9, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Baker, L.D.; Frank, L.L.; Foster-Schubert, K.; Green, P.S.; Wilkinson, C.W.; McTiernan, A.; Plymate, S.R.; Fishel, M.A.; Watson, G.S.; Cholerton, B.A. Effects of aerobic exercise on mild cognitive impairment: A controlled trial. Arch. Neurol. 2010, 67, 71–79. [Google Scholar] [CrossRef] [PubMed]
- McAuley, E.; Kramer, A.F.; Colcombe, S.J. Cardiovascular fitness and neurocognitive function in older adults: A brief review. Brain Behav. Immun. 2004, 18, 214–220. [Google Scholar] [CrossRef] [PubMed]
- Colcombe, S.; Kramer, A.F. Fitness effects on the cognitive function of older adults: A meta-analytic study. Psychol. Sci. 2003, 14, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Boulos, M.N.K.; Yang, S.P. Exergames for health and fitness: The roles of GPS and geosocial apps. Int. J. Health Geographics 2013, 12, 18. [Google Scholar] [CrossRef] [PubMed]
- Anderson-Hanley, C.; Arciero, P.J.; Brickman, A.M.; Nimon, J.P.; Okuma, N.; Westen, S.C.; Merz, M.E.; Pence, B.D.; Woods, J.A.; Kramer, A.F. Exergaming and older adult cognition: A cluster randomized clinical trial. Am. J. Prev. Med. 2012, 42, 109–119. [Google Scholar] [CrossRef]
- Read, J.L.; Shortell, S.M. Interactive games to promote behavior change in prevention and treatment. J. Am. Med. 2011, 305, 1704–1705. [Google Scholar] [CrossRef] [PubMed]
- Guderian, B.; Borreson, L.; Sletten, L.; Cable, K.; Stecker, T.; Probst, M.; Dalleck, L. The cardiovascular and metabolic responses to Wii Fit video game playing in middle-aged and older adults. J. Sports Med. Phys. Fit. 2010, 50, 436–442. [Google Scholar]
- Colombo, M.; Marelli, E.; Vaccaro, R.; Valle, E.; Colombani, S.; Polesel, E.; Garolfi, S.; Fossi, S.; Guaita, A. Virtual Reality for Persons with Dementia: An Exergaming Experience. In Proceedings of the International Symposium on Automation and Robotics in Construction, Eindhoven, The Netherlands, 26–29 June 2012; pp. 1–4. [Google Scholar] [CrossRef]
- van der Kuil, M.; van der Ham, I.; Visser-Meily, J. Game Technology in Cognitive Rehabilitation of Spatial Navigation Impairment. In Proceedings of the International Conference on Virtual Rehabilitation, Montreal, QC, Canada, 19–22 June 2017; pp. 1–2. [Google Scholar]
- Thompson Coon, J.; Boddy, K.; Stein, K.; Whear, R.; Barton, J.; Depledge, M.H. Does participating in physical activity in outdoor natural environments have a greater effect on physical and mental wellbeing than physical activity indoors? A systematic review. Environ. Sci. Technol. 2011, 45, 1761–1772. [Google Scholar] [CrossRef] [PubMed]
- Anderson-Hanley, C.; Maloney, M.; Barcelos, N.; Striegnitz, K.; Kramer, A. Neuropsychological benefits of neuro-exergaming for older adults: A pilot study of an interactive physical and cognitive exercise system (iPACES). J. Aging Phys. Act. 2017, 25, 73–83. [Google Scholar] [CrossRef] [PubMed]
- Wall, K.; Stark, J.; Schillaci, A.; Saulnier, E.; McLaren, E.; Striegnitz, K.; Cohen, B.; Arciero, P.; Kramer, A.; Anderson-Hanley, C. The enhanced interactive physical and cognitive exercise system (iPACESTM v2. 0): Pilot clinical trial of an in-home iPad-based neuro-exergame for mild cognitive impairment (MCI). J. Clin. Med. 2018, 7, 249. [Google Scholar] [CrossRef] [PubMed]
- Mrakic-Sposta, S.; Di Santo, S.G.; Franchini, F.; Arlati, S.; Zangiacomi, A.; Greci, L.; Moretti, S.; Jesuthasan, N.; Marzorati, M.; Rizzo, G. Effects of combined physical and cognitive virtual reality-based training on cognitive impairment and oxidative stress in MCI patients: A pilot study. Front. Aging Neurosci. 2018, 10, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Gadler, E.; Grassi, A.; Riva, G. A rehabilitation protocol for empowering spatial orientation in MCI. A pilot study. In Annual Review of Cybertherapy and Telemedicine 2009: Advanced Technologies in the Behavioral, Social, and Neurosciences; Wiederhold, B.K., Riva, G., Eds.; IOS Press: Amsterdam, The Netherlands, 2009; pp. 234–236. [Google Scholar]
- Knopman, D.S.; Roberts, R.O.; Geda, Y.E.; Pankratz, V.S.; Christianson, T.J.; Petersen, R.C.; Rocca, W.A. Validation of the telephone interview for cognitive status-modified in subjects with normal cognition, mild cognitive impairment, or dementia. Neuroepidemiology 2010, 34, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Welsh, K.A.; Breitner, J.C.; Magruder-Habib, K.M. Detection of dementia in the elderly using telephone screening of cognitive status. Neuropsychiatry Neuropsychol. Behav. Neurol. 1993, 6, 103–110. [Google Scholar]
- Castanho, T.J.C. Cognitive Functioning From Normal Aging to Mild Cognitive Impairment: Combining Rapid Cognitive Testing and Informant Reports to Improve Screening in Clinical and Research Contexts. Ph.D. Thesis, Universidade do Minho, Braga, Portugal, 2017. [Google Scholar]
- Haskell, W.L.; Lee, I.-M.; Pate, R.R.; Powell, K.E.; Blair, S.N.; Franklin, B.A.; Macera, C.A.; Heath, G.W.; Thompson, P.D.; Bauman, A. Physical activity and public health: Updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Circulation 2007, 116, 1081. [Google Scholar] [CrossRef]
- Berry, J.M.; West, R.L.; Dennehey, D.M. Reliability and validity of the Memory Self-Efficacy Questionnaire. Dev. Psychol. 1989, 25, 701. [Google Scholar] [CrossRef]
- Dogu, U.; Erkip, F. Spatial factors affecting wayfinding and orientation: A case study in a shopping mall. Environ. Behav. 2000, 32, 731–755. [Google Scholar] [CrossRef]
- Chebat, J.-C.; Gélinas-Chebat, C.; Therrien, K. Gender-related wayfinding time of mall shoppers. J. Bus. Res. 2008, 61, 1076–1082. [Google Scholar] [CrossRef]
- Hölscher, C.; Meilinger, T.; Vrachliotis, G.; Brösamle, M.; Knauff, M. Up the down staircase: Wayfinding strategies in multi-level buildings. J. Environ. Psychol. 2006, 26, 284–299. [Google Scholar] [CrossRef]
- Wong, D.; Hockenberry-Eaton, M.; Wilson, D.; Winkelstein, M.; Schwarts, P. Face scale. In Wong. Face Facets P. Face; Schwarts, P., Ed.; Mosby: St. Louis, MO, USA, 2001; p. 1301. [Google Scholar]
- Stern, R.; Arruda, J.; Hooper, C.; Wolfner, G.; Morey, C. Visual analogue mood scales to measure internal mood state in neurologically impaired patients: Description and initial validity evidence. Aphasiology 1997, 11, 59–71. [Google Scholar] [CrossRef]
- Burdon, J.G.W.; Juniper, E.F.; Killian, K.J.; Hargreave, F.E.; Campbell, E.J.M. The perception of breathlessness in asthma. Am. Rev. Respir. Dis. 1982, 126, 825–828. [Google Scholar]
- Wong, C.N.; Chaddock-Heyman, L.; Voss, M.W.; Burzynska, A.Z.; Basak, C.; Erickson, K.I.; Prakash, R.S.; Szabo-Reed, A.N.; Phillips, S.M.; Wojcicki, T. Brain activation during dual-task processing is associated with cardiorespiratory fitness and performance in older adults. Front. Aging Neurosci. 2015, 7, 154–164. [Google Scholar] [CrossRef] [PubMed]
- Prakash, R.S.; Erickson, K.I.; Colcombe, S.J.; Kim, J.S.; Voss, M.W.; Kramer, A.F. Age-related differences in the involvement of the prefrontal cortex in attentional control. Brain Cogn. 2009, 71, 328–335. [Google Scholar] [CrossRef] [Green Version]
- Kramer, A.F.; Humphrey, D.G.; Larish, J.F.; Logan, G.D. Aging and inhibition: Beyond a unitary view of inhibitory processing in attention. Psychol. Aging 1994, 9, 491–513. [Google Scholar] [CrossRef] [PubMed]
- Castel, A.D.; Humphreys, K.L.; Lee, S.S.; Galván, A.; Balota, D.A.; McCabe, D.P. The development of memory efficiency and value-directed remembering across the life span: A cross-sectional study of memory and selectivity. Dev. Psychol. 2011, 47, 1553–1564. [Google Scholar] [CrossRef]
- Nguyen, L.T.; Marini, F.; Zacharczuk, L.; Llano, D.A.; Mudar, R.A. Theta and alpha band oscillations during value-directed strategic processing. Behav. Brain Res. 2019, 367, 210–214. [Google Scholar] [CrossRef]
- Ekstrom, R.; French, J. The Hidden Patterns Test. In Educational Testing Service; Educational Testing Service: Princeton, NJ, USA, 1976. [Google Scholar]
- Ekstrom, R.; French, J.; Harman, H.; Derman, D. Card Rotations Test. In Kit of Factor-Referenced Cognitive Tests; Educational Testing Service: Princeton, NJ, USA, 1976. [Google Scholar]
- Brockmyer, J.H.; Fox, C.M.; Curtiss, K.A.; McBroom, E.; Burkhart, K.M.; Pidruzny, J.N. The development of the Game Engagement Questionnaire: A measure of engagement in video game-playing. J. Exp. Soc. Psychol. 2009, 45, 624–634. [Google Scholar] [CrossRef]
- Tenenbaum, G.; Connolly, C.T. Attention allocation under varied workload and effort perception in rowers. Psychol. Sport Exerc. 2008, 9, 704–717. [Google Scholar] [CrossRef]
- Watson, D.; Clark, L.A.; Tellegen, A. Development and validation of brief measures of positive and negative affect: The PANAS scales. J. Personal. Soc. Psychol. 1988, 54, 1063–1070. [Google Scholar] [CrossRef]
- Adam Noah, J.; Spierer, D.K.; Gu, J.; Bronner, S. Comparison of steps and energy expenditure assessment in adults of Fitbit Tracker and Ultra to the Actical and indirect calorimetry. J. Med. Eng. Technol. 2013, 37, 456–462. [Google Scholar] [CrossRef] [PubMed]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [PubMed]
- McGough, E.L.; Kelly, V.E.; Logsdon, R.G.; McCurry, S.M.; Cochrane, B.B.; Engel, J.M.; Teri, L. Associations between physical performance and executive function in older adults with mild cognitive impairment: Gait speed and the timed “up & go” test. Phys. Ther. 2011, 91, 1198–1207. [Google Scholar] [PubMed]
- IBM Corp. IBM SPSS Statistics for Windows; Version 25.0; IBM Corp: Armonk, NY, USA, 2017. [Google Scholar]
- Kramer, A.; Erickson, K.I.; Colcombe, S.J. Exercise, cognition and the aging brain. J. Appl. Physiol. 2006, 101, 1237–1242. [Google Scholar] [CrossRef]
- Schoene, D.; Valenzuela, T.; Lord, S.R.; de Bruin, E.D. The effect of interactive cognitive-motor training in reducing fall risk in older people: A systematic review. BMC Geriatr. 2014, 14, 107–129. [Google Scholar] [CrossRef]
- Gheysen, F.; Poppe, L.; DeSmet, A.; Swinnen, S.; Cardon, G.; De Bourdeaudhuij, I.; Chastin, S.; Fias, W. Physical activity to improve cognition in older adults: Can physical activity programs enriched with cognitive challenges enhance the effects? A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 63–76. [Google Scholar] [CrossRef]
- Matthews, F.E.; Stephan, B.C.; Robinson, L.; Jagger, C.; Barnes, L.E.; Arthur, A.; Brayne, C.; Collaboration, A.S.C.; Comas-Herrera, A.; Wittenberg, R. A two decade dementia incidence comparison from the Cognitive Function and Ageing Studies I and II. Nat. Commun. 2016, 7, 11398–11406. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | Intervention (n = 14) | Control (n = 13) |
|---|---|---|
| Age (M (SD)) | 49.36 (5.08) | 53.23 (4.71) |
| Sex (% female) | 85.7 | 69.2 |
| Race (%) | ||
| White | 64.3 | 69.2 |
| Black or African American | 21.4 | 15.4 |
| Asian | 7.1 | 7.7 |
| American Indian | 0.0 | 7.7 |
| Decline Response | 7.1 | 0.0 |
| Ethnicity (%) | ||
| Not Hispanic or Latino | 78.6 | 92.3 |
| Hispanic or Latino | 21.4 | 7.7 |
| Education (% college degree) | 85.7 | 76.9 |
| BMI (M (SD)) | 31.75 (8.46) | 32.49 (16.70) |
| TICS (M (SD)) | 21.07 (2.53) | 21.46 (1.13) |
| GDS (M (SD)) | 0.43 (0.85) | 0.69 (1.03) |
| Wayfinding Performance Measure | Conditions | |||
|---|---|---|---|---|
| Experimental (n = 14) | Control (n = 13) | |||
| Baseline | Follow-up | Baseline | Follow-up | |
| Total steps | 840.36 (358.89) | 1071.89 (507.00) | 968.54 (469.50) | 997.77 (719.22) |
| Distance covered (miles) | 0.18 (0.08) | 0.24 (0.11) | 0.21 (0.09) | 0.21 (0.15) |
| Total time (seconds) | 245.58 (117.90) | 315.67 (169.15) | 298.69 (144.44) | 300.12 (204.40) |
| Hovers | 2.14 (2.98) | 1.97 (1.87) | 4.08 (4.17) | 1.38 (1.89) |
| Mood | 80.00% (11.09%) | 64.17% (21.51%) | 73.85% (17.10%) | 69.23% (17.54%) |
| Exertion | 3.21 (1.72) | 3.70 (2.05) | 3.23 (1.92) | 3.77 (1.48) |
| Familiarity (Yes/No) | 4/10 | 4/10 | ||
| Maze SE | 58.29 (18.73) | 85.00 * (16.19) | 59.69 (21.12) | 74.46 * (16.58) |
| Cognitive Task | Experimental (n = 14) | Control (n = 13) | ||
|---|---|---|---|---|
| Baseline M (SD) | Follow-up M (SD) | Baseline M (SD) | Follow-up M (SD) | |
| Stroop Task—RT | 781.16 * (113.50) | 735.78 * (105.75) | 727. 20 (110.82) | 753.96 (119.26) |
| Flanker Task—RT | 627.62 (89.29) | 616.0 (78.11) | 615.92 (83.83) | 593.67 (88.51) |
| Dual Task—RT of Second Selection | 1585.77 (219.52) | 1504.15 (256.07) | 1563.50 (514.07) | 1629.22 (234.17) |
| Hidden Figures (Summation) | 161.93 (74.24) | 200.10 (73.89) | 155.08 (57.76) | 202.62 (50.79) |
| Card Rotations (Summation) | 100.93 (34.30) | 114.36 (34.48) | 97.31 (25.81) | 112.15 (26.59) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palac, D.; Bullard, T.; Cohen, J.D.; Nguyen, L.T.; Mudar, R.A.; Mullen, S.P. Effects of Traditional vs. iPad-Enhanced Aerobic Exercise on Wayfinding Efficacy and Cognition: A Pilot Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2019, 16, 3495. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16183495
Palac D, Bullard T, Cohen JD, Nguyen LT, Mudar RA, Mullen SP. Effects of Traditional vs. iPad-Enhanced Aerobic Exercise on Wayfinding Efficacy and Cognition: A Pilot Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2019; 16(18):3495. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16183495
Chicago/Turabian StylePalac, Daniel, Tiffany Bullard, Jason D. Cohen, Lydia T. Nguyen, Raksha A. Mudar, and Sean P. Mullen. 2019. "Effects of Traditional vs. iPad-Enhanced Aerobic Exercise on Wayfinding Efficacy and Cognition: A Pilot Randomized Controlled Trial" International Journal of Environmental Research and Public Health 16, no. 18: 3495. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16183495