Confidence in Health-Services Availability during Disasters and Emergency Situations—Does it Matter?—Lessons Learned from an Israeli Population Survey



Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Statistical Analysis
3. Results
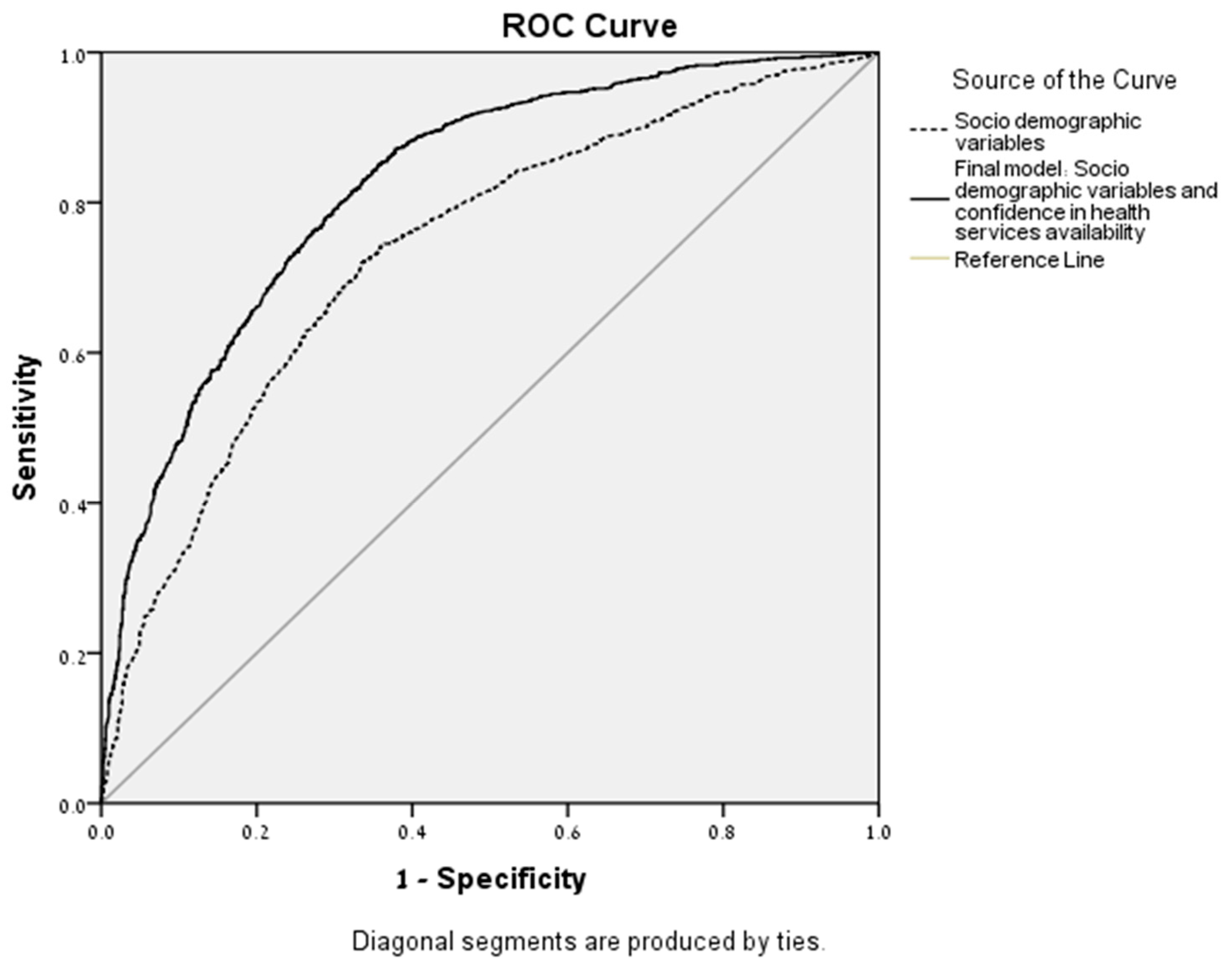
Hierarchical Logistic Regression (HLR)
4. Discussion
Limitation and Further Studies
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| No. | Phrase | Min | Max | Mean | SD |
|---|---|---|---|---|---|
| 1. | The municipal authority functions well. | 1 | 5 | 3.49 | 1.087 |
| 2. | There is mutual assistance and people care for one another. | 1 | 5 | 3.64 | 1.111 |
| 3. | My community is prepared for an emergency situation. | 1 | 5 | 3.26 | 1.070 |
| 4. | I am proud to tell others where I live. | 1 | 5 | 4.16 | 0.997 |
| 5. | Good relationships exist between the various groups. | 1 | 5 | 3.48 | 0.961 |
| 6. | I trust the local decision makers | 1 | 5 | 3.18 | 1.126 |
| 7. | I can count on people in my community to help me in a crisis situation. | 1 | 5 | 3.73 | 1.142 |
| 8. | Residents are aware of their roles in an emergency situation. | 1 | 5 | 2.91 | 1.159 |
| 9. | I have a sense of belonging to my community. | 1 | 5 | 3.94 | 1.057 |
| 10. | Residents in my community trust each other. | 1 | 5 | 3.46 | 0.963 |
| 11. | In my community, appropriate attention is given to the needs of children. | 1 | 5 | 3.58 | 1.062 |
| 12. | In my community, there are people who can help me cope with an emergency situation. | 1 | 5 | 3.76 | 1.023 |
| 13. | There are sufficient facilities for public protection (e.g., shelters, etc.) in my community | 1 | 5 | 3.07 | 1.212 |
| 14. | I remain in my community for ideological reasons. | 1 | 5 | 2.97 | 1.416 |
| 15. | I have faith in my mayor’s ability to lead the transfer from routine to emergency management. | 1 | 5 | 3.32 | 1.141 |
| 16. | I have faith in my community’s ability to overcome an emergency situation. | 1 | 5 | 3.79 | 0.987 |
| 17. | My family and I are acquainted with the emergency system in my town (to be activated in times of emergency). | 1 | 5 | 2.92 | 1.249 |
| 18. | I would be sorry to leave the town where I reside. | 1 | 5 | 3.95 | 1.228 |
| 19. | The municipal authorities provide services fairly. | 1 | 5 | 3.31 | 1.096 |
| 20. | The residents are greatly involved in the community’s activities. | 1 | 5 | 3.33 | 1.041 |
| 21. | The residents of my community will continue to receive municipal services even in an emergency situation. | 1 | 5 | 3.43 | 0.995 |
| 22. | I feel safe in my place of residence. | 1 | 5 | 3.72 | 1.011 |
| 23. | The health services in my town will continue to function appropriately in an emergency situation. | 1 | 5 | 3.39 | 1.096 |
| 24. | The information I receive from the municipal authority during emergency situations fulfills my needs. | 1 | 5 | 3.29 | 1.147 |
| 25. | Many of my neighbors are my friends. | 1 | 5 | 3.53 | 1.183 |
| 26. | I intend to leave my place of residence in an emergency. | 1 | 5 | 2.03 | 1.234 |
| 27. | In an emergency, the public transportation where I live will function. | 1 | 5 | 2.53 | 1.106 |
| 28. | Officials in my place of residence demonstrate leadership abilities. | 1 | 5 | 3.28 | 1.118 |
| CCRAM Factors | Min | Max | Mean | SD |
|---|---|---|---|---|
| CCRAM total score | 1 | 5 | 3.46 | 0.73 |
| Leadership | 1 | 5 | 3.39 | 0.89 |
| Collective efficacy | 1 | 5 | 3.65 | 0.86 |
| Preparedness | 1 | 5 | 3.04 | 0.94 |
| Place attachment | 1 | 5 | 3.76 | 0.90 |
| Social trust | 1 | 5 | 3.47 | 0.89 |
| No. | CCRAM’s Items | Correlation |
|---|---|---|
| 1 | The municipal authority functions well. | 0.482 ** |
| 2 | There is mutual assistance and people care for one another. | 0.322 ** |
| 3 | My community is prepared for an emergency situation. | 0.490 ** |
| 4 | I am proud to tell others where I live. | 0.284 ** |
| 5 | Good relationships exist between the various groups. | 0.286 ** |
| 6 | I trust the local decision makers. | 0.517 ** |
| 7 | I can count on people in my community to help me in a crisis situation. | 0.300 ** |
| 8 | Residents are aware of their roles in an emergency situation. | 0.406 ** |
| 9 | I have a sense of belonging to my community. | 0.297 ** |
| 10 | Residents in my community trust each other. | 0.287 ** |
| 11 | In my community, appropriate attention is given to the needs of children. | 0.419 ** |
| 12 | In my community, there are people who can help me cope with an emergency situation. | 0.427 ** |
| 13 | There are sufficient facilities for public protection (e.g., shelters, etc.) in my community | 0.324 ** |
| 14 | I remain in my community for ideological reasons. | 0.187 ** |
| 15 | I have faith in my mayor’s ability to lead the transfer from routine to emergency management. | 0.527 ** |
| 16 | I have faith in my community’s ability to overcome an emergency situation. | 0.424 ** |
| 17 | My family and I are acquainted with the emergency system in my town (to be activated in times of emergency). | 0.381 ** |
| 18 | I would be sorry to leave the town where I reside. | 0.235 ** |
| 19 | The municipal authorities provide services fairly. | 0.507 ** |
| 20 | The residents are greatly involved in the community’s activities. | 0.365 ** |
| 21 | The residents of my community will continue to receive Municipal services even in an emergency situation. | 0.600 ** |
References
- Cohen, O.; Leykin, D.; Lahad, M.; Goldberg, A.; Aharonson-Daniel, L. The conjoint community resiliency assessment measure as a baseline for profiling and predicting community resilience for emergencies. Technol. Forecast Soc. Chang. 2013, 80, 1732–1741. [Google Scholar] [CrossRef]
- Plough, A.; Fielding, J.E.; Chandra, A.; Williams, M.; Eisenman, D.; Wells, K.B.; Law, G.L.; Fogleman, S.; Magaña, A. Building community disaster resilience: Perspectives from a large urban county department of public health. Am. J. Public Health 2013, 103, 1190–1197. [Google Scholar] [CrossRef] [PubMed]
- Norris, F.H.; Stevens, S.P.; Pfefferbaum, B.; Wyche, K.F.; Pfefferbaum, R.L. Community resilience as a metaphor, theory, set of capacities, and strategy for disaster readiness. Am. J. Commun. Psychol. 2008, 41, 127–150. [Google Scholar] [CrossRef] [PubMed]
- Herrman, H.; Stewart, D.E.; Diaz-Granados, N.; Berger, E.L.; Jackson, B.; Yuen, T. What is resilience? Can. J. Psychiatry 2011, 56, 258–265. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Public Health Preparedness Capabilities: National Standards for State and Local Planning; Centers for Disease Control, and Prevention: Atlanta, GA, USA, 2011. Available online: https://www.cdc.gov/phpr/readiness/00_docs/DSLR_capabilities_July.pdf (accessed on 22 August 2019).
- World Health Organization. Official Records of the World Health Organization; World Health Organization: Geneva, Switzerland, 1946. [Google Scholar]
- Chandra, A. State of community resilience approaches in public health. In Proceedings of the 142nd APHA Annual Meeting and Exposition, New Orleans, LA, USA, 15–19 November 2014; American Public Health Association: New Orleans, LA, USA, 2014. [Google Scholar]
- MacQueen, K.M.; McLellan, E.; Metzger, D.S.; Kegeles, S.; Strauss, R.P.; Scotti, R.; Roseanne, S.; Blanchard, L.; Trotter, R.T. What is community? An evidence-based definition for participatory public health. Am. J. Public Health 2001, 91, 1929–1938. [Google Scholar] [CrossRef] [PubMed]
- Chandra, A.; Williams, M.; Plough, A.; Stayton, A.; Wells, K.B.; Horta, M.; Tang, J. Getting actionable about community resilience: The Los Angeles county community disaster resilience project. Am. J. Public Health 2013, 103, 1181–1189. [Google Scholar] [CrossRef] [PubMed]
- Gray, L.; MacDonald, C.; Mackie, B.; Paton, D.; Johnston, D.; Baker, M.G. Community responses to communication campaigns for influenza A (H1N1): A focus group study. BMC Public Health 2012, 12, 1. [Google Scholar] [CrossRef]
- Nuwayhid, I.; Zurayk, H.; Yamout, R.; Cortas, C.S. Summer 2006 war on Lebanon: A lesson in community resilience. Glob. Public Health 2011, 6, 505–519. [Google Scholar] [CrossRef]
- Beiser, M.; Wiwa, O.; Adebajo, S. Human-initiated disaster, social disorganization and post-traumatic stress disorder above Nigeria’s oil basins. Soc Sci. Med. 2010, 71, 221–227. [Google Scholar] [CrossRef]
- Cox, R.S.; Perry, K.M.E. Like a fish out of water: Reconsidering disaster recovery and the role of place and social capital in community disaster resilience. Am. J. Commun. Psychol. 2011, 48, 395–411. [Google Scholar] [CrossRef]
- UNISDR. Sendai Framework for Disaster Risk Reduction 2015–2030; UNISDR: Sendai, Japan, 2015; Available online: http://www.unisdr.org/we/inform/publications/43291 (accessed on 22 August 2019).
- Phibbs, S.; Kenney, C.; Severinsen, C.; Mitchell, J.; Hughes, R. Synergising Public Health Concepts with the Sendai Framework for Disaster Risk Reduction: A Conceptual Glossary. Int. J. Environ. Res. Public Health 2016, 13, 1241. [Google Scholar] [CrossRef] [PubMed]
- Brodie, M.; Weltzien, E.; Altman, D.; Blendon, R.J.; Benson, J.M. Experiences of Hurricane Katrina evacuees in Houston shelters: Implications for future planning. Am. J. Public Health 2006, 96, 1402–1408. [Google Scholar] [CrossRef] [PubMed]
- Charney, R.L.; Rebmann, T.; Esguerra, C.R.; Lai, C.W.; Dalawari, P. Public perceptions of hospital responsibilities to those presenting without medical injury or illness during a disaster. J. Emerg. Med. 2013, 45, 578–584. [Google Scholar] [CrossRef] [PubMed]
- Wulff, K.; Donato, D.; Lurie, N. What is health resilience and how can we build it? Annu. Rev. Public Health 2015, 36, 361–374. [Google Scholar] [CrossRef] [PubMed]
- Shapira, S.; Aharonson-Daniel, L.; Bar-Dayan, Y.; Sykes, D.; Adini, B. Knowledge, perceptions, attitudes and willingness to report to work in an earthquake: A pilot study comparing Canadian versus Israeli hospital nursing staff. Int. Emerg. Nurs. 2016, 25, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Paturas, J.; Smith, D.; Smith, S.; Albanese, J. Collective response to public health emergencies and large-scale disasters: Putting hospitals at the core of community resilience. J. Bus. Contin. Emer. Plan. 2010, 4, 286–2955. [Google Scholar] [PubMed]
- Bonanno, G.A.; Romero, S.A.; Klein, S.I. The temporal elements of psychological resilience: An integrative framework for the study of individuals, families, and communities. Psychol. Inq. 2015, 26, 139–169. [Google Scholar] [CrossRef]
- Cutter, S.L. The landscape of disaster resilience indicators in the USA. Nat. Hazards 2016, 80, 741–758. [Google Scholar] [CrossRef]
- Leykin, D.; Lahad, M.; Cohen, O.; Goldberg, A.; Aharonson-Daniel, L. Conjoint community resiliency assessment measure-28/10 items (CCRAM28 and CCRAM10): A self-report tool for assessing community resilience. Am. J. Commun. Psychol. 2013, 52, 313–323. [Google Scholar] [CrossRef]
- Central Bureau of Statistics, 2018. Available online: https://www.cbs.gov.il/EN/pages/default.aspx (accessed on 22 August 2019).
- Bland, J.M.; Altman, D.G. The odds ratio. BMJ 2000, 320, 1468. [Google Scholar] [CrossRef]
- Metz, C.E. Basic principles of ROC analysis. Semin. Nucl. Med. 1978, 8, 283–298. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services. National Health Security Strategy of the United States of America.; U.S. Department of Health and Human Services: Washington, DC, USA, 2009.
- European Commission, Humanitarian Aid and Civil Protection. Resilience Marker: General Guidance, 2014. Available online: http://ec.europa.eu/echo/files/policies/resilience/resilience_marker_guidance_en.pdf (accessed on 22 August 2019).
- Cohen, O.; Bolotin, A.; Lahad, M.; Goldberg, A.; Aharonson-Daniel, L. Increasing sensitivity of results by using quantile regression analysis for exploring community resilience. Ecol. Indic. 2016, 66, 497–502. [Google Scholar] [CrossRef] [Green Version]
- Cohen, O.; Geva, D.; Lahad, M.; Bolotin, A.; Leykin, D.; Goldberg, A.; Aharonson-Daniel, L. Community resilience throughout the lifespan—The potential contribution of healthy elders. PLoS ONE 2016, 11, e0148125. [Google Scholar] [CrossRef] [PubMed]
- Morton, M.J.; Lurie, N. Community resilience and public health practice. Am. J. Public Health 2013, 103, 1158–1160. [Google Scholar] [CrossRef] [PubMed]
- National Research Council. Disaster Resilience: A National Imperative.; National Academic Press: Washington, DC, USA, 2012. [Google Scholar]
- Chandra, A.; Acosta, J.; Stern, S.; Uscher-Pines, L.; Williams, M.V. Building Community Resilience to Disasters: A Way Forward to Enhance National Health Security; Rand Corporation: Santa Monica, CA, USA, 2011. [Google Scholar]
- Ray-Bennett, N.S.; Collins, A.; Bhuiya, A.; Edgeworth, R.; Nahar, P.; Alamgir, F. Exploring the meaning of health security for disaster resilience through people’s perspectives in Bangladesh. Health Place 2010, 16, 581–589. [Google Scholar] [CrossRef] [PubMed]
- Smith, G. Does Gender Influence Online Survey Participation?: A Record-Linkage Analysis Of University Faculty Online Survey Response Behavior. 2008. Available online: https://scholarworks.sjsu.edu/cgi/viewcontent.cgi?article=1003&context=elementary_ed_pub (accessed on 22 August 2019).


| Variable | n | % | CCRAM Score | p-Value (t-Test or ANOVA) | Confidence in Health Services Availability | p-Value (t-Test or ANOVA) |
|---|---|---|---|---|---|---|
| Total | 3478 | 100 | 3.46 | 3.37 | ||
| Gender | ||||||
| Female | 2014 | 57.9 | 3.46 | 0.069 | 3.40 | 0.978 |
| Male | 1424 | 40.9 | 3.43 | 3.32 | ||
| Family status | ||||||
| In a permanent relationship | 2668 | 76.7 | 3.49 | 0.001 | 3.40 | 0.001> |
| Not in a permanent relationship | 765 | 22.0 | 3.28 | 3.27 | ||
| Community type | ||||||
| Midsize town (up to 50,000) | 1615 | 46.4 | 3.14 | <0.001 | 3.10 | 0.001> |
| Small community (up to 10,000) | 1813 | 52.1 | 3.74 | 3.62 | ||
| Income | ||||||
| Below average | 804 | 23.1 | 3.26 | <0.001 | 3.16 | 0.001> |
| About average | 1195 | 34.4 | 3.47 | 3.36 | ||
| Above average | 1354 | 38.9 | 3.52 | 3.50 | ||
| CERT volunteer | ||||||
| No | 2951 | 84.8 | 3.81 | <0.001 | 3.69 | 0.06 |
| Yes | 474 | 13.6 | 3.38 | 3.32 | ||
| Physical or mental disability | ||||||
| No | 3024 | 86.9 | 3.46 | 0.001 | 3.38 | 0.124 |
| Yes | 424 | 12.2 | 3.33 | 3.29 | ||
| Previous involvement in an emergency situation | ||||||
| No | 1547 | 44.5 | 3.44 | 0.418 | 3.36 | 0.766 |
| Yes | 1257 | 36.1 | 3.47 | 3.35 | ||
| Odds Ratio | p | 95% Confidence Interval | ||
|---|---|---|---|---|
| Variable | (OR) | Lower | Upper | |
| Gender | ||||
| Female | 1 | |||
| Male | 0.872 | 0.131 | 0.730 | 1.042 |
| Age (per year) | 1.001 | 0.878 | 0.994 | 1.007 |
| Permanent relationship | ||||
| Yes | 1 | |||
| No | 0.772 | 0.023 | 0.617 | 0.964 |
| Physical or mental disability | ||||
| No | 1 | |||
| Yes | 0.916 | 0.534 | 0.695 | 1.208 |
| Community type | ||||
| Midsized city | 1 | |||
| Small community | 4.009 | <0.001 | 3.358 | 4.786 |
| Income | ||||
| Average | 1 | |||
| Below | 0.709 | 0.005 | 0.559 | 0.900 |
| Above | 0.823 | 0.059 | 0.673 | 1.007 |
| CERT volunteer | ||||
| No | 1 | |||
| Yes | 2.120 | <0.001 | 1.614 | 2.785 |
| Confidence in health services availability | 2.677 | <0.001 | 2.433 | 2.946 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cohen, O.; Shapira, S.; Aharonson-Daniel, L.; Shamian, J. Confidence in Health-Services Availability during Disasters and Emergency Situations—Does it Matter?—Lessons Learned from an Israeli Population Survey. Int. J. Environ. Res. Public Health 2019, 16, 3519. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16193519
Cohen O, Shapira S, Aharonson-Daniel L, Shamian J. Confidence in Health-Services Availability during Disasters and Emergency Situations—Does it Matter?—Lessons Learned from an Israeli Population Survey. International Journal of Environmental Research and Public Health. 2019; 16(19):3519. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16193519
Chicago/Turabian StyleCohen, Odeya, Stav Shapira, Limor Aharonson-Daniel, and Judith Shamian. 2019. "Confidence in Health-Services Availability during Disasters and Emergency Situations—Does it Matter?—Lessons Learned from an Israeli Population Survey" International Journal of Environmental Research and Public Health 16, no. 19: 3519. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16193519