Workplace Violence in Chinese Hospitals: The Effects of Healthcare Disturbance on the Psychological Well-Being of Chinese Healthcare Workers


Abstract
:1. Introduction
2. Method
2.1. Sample and Procedure
2.2. Measures
2.3. Analysis
3. Results
3.1. Sample Characteristics
3.2. Association between Emotional Labour and Depressive symptoms with Sociodemographic Variables
3.3. Predicting Depressive symptoms from Healthcare Disturbance and Surface Acting
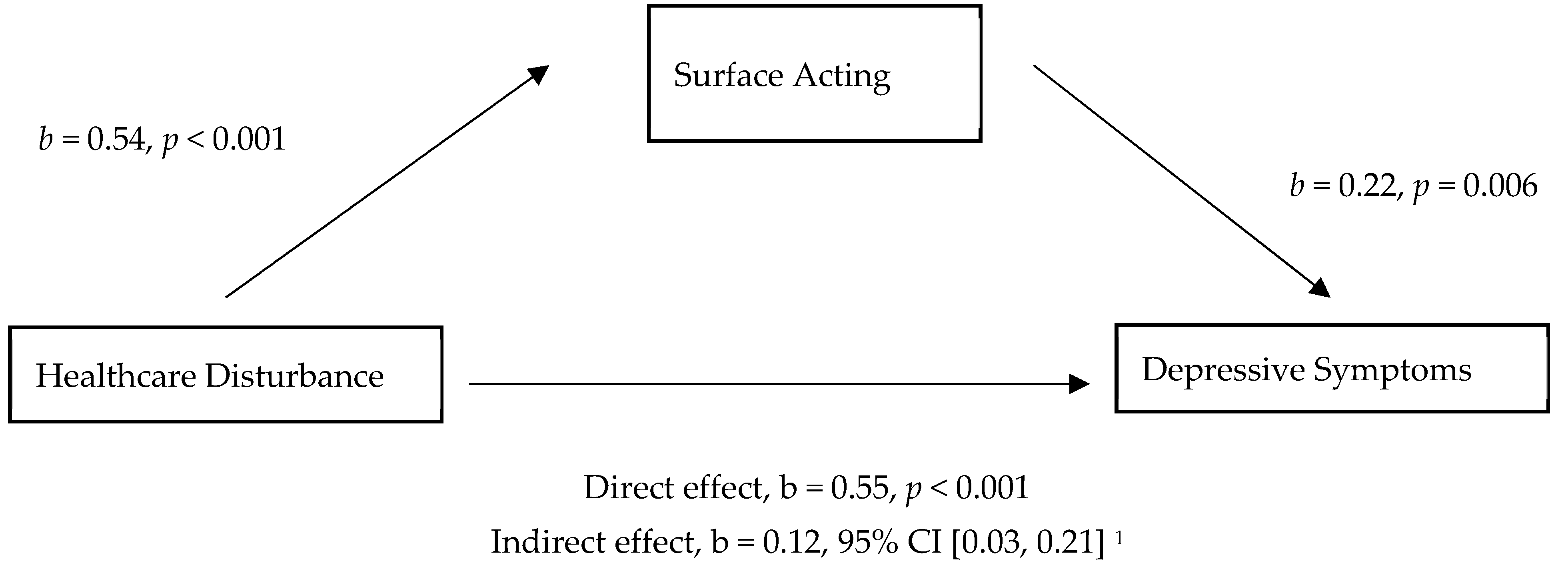
3.4. Mediation Relationship
4. Discussion
4.1. Study Implications
4.2. Potential Limitations and Future Directions
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- ILO Framework Guidelines for Addressing Workplace Violence in the Health Sector. International Labour Office: Geneva, 2002. Available online: https://www.who.int/violence_injury_prevention/violence/interpersonal/en/WVguidelinesEN.pdf?ua=1 (accessed on 11 September 2019).
- Cheung, T.; Yip, P.S. Workplace violence towards nurses in Hong Kong: Prevalence and correlates. BMC Public Health 2017, 17, 196. [Google Scholar] [CrossRef] [PubMed]
- Sun, T.; Gao, L.; Li, F.J.; Shi, Y.; Xie, F.Z.; Wang, J.; Wang, S.; Zhang, S.; Liu, W.; Duan, X.; et al. Workplace violence, psychological stress, sleep quality and subjective health in Chinese doctors: A large cross-sectional study. BMJ Open 2017, 7, e017182. [Google Scholar] [CrossRef] [PubMed]
- Jiao, M.; Ning, N.; Li, Y.; Gao, L.; Cui, Y.; Sun, H.; Kang, Z.; Liang, L.; Wu, Q.; Hao, Y. Workplace violence against nurses in Chinese hospitals: A cross-sectional survey. BMJ Open 2015, 5, e006719. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Stone, T.E.; Zhang, J. Understanding the rise of Yinao in China: A commentary on the little-known phenomenon of healthcare violence. Nurs. Health Sci. 2017, 19, 183–187. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Kwan, H.; Chiu, R. Customer sexual harassment and frontline employees’ service performance in China. Hum. Relat. 2014, 67, 333–356. [Google Scholar] [CrossRef]
- Xiong, C. Medical malpractice and medical disputes. In Chinese Hospital Association Guide; Chinese Hospital Association: Beijing, China, 2006. [Google Scholar]
- Hesketh, T.; Wu, D.; Mao, L.; Ma, N. Violence against doctors in China. Br. Med. J. 2012, 345, e5730. [Google Scholar] [CrossRef] [PubMed]
- Adler, D.; Mclaughlin, T.; Rogers, W.; Chang, H.; Lapitsky, L.; Lerner, D. Job Performance Deficits Due to Depression. Am. J. Psychiatry 2006, 163, 1569–1576. [Google Scholar] [CrossRef] [PubMed]
- Milcent, C. The Rise of Violence as a Result of Inefficiency in the Healthcare System. In IDEAS Working Paper Series from RePEc; Palgrave Pivot: Cham, Switzerland, 2018. [Google Scholar]
- Grandey, A.A. Emotion regulation in the workplace: A new way to conceptualize emotional labor. J. Occup. Health Psychol. 2000, 5, 59–100. [Google Scholar] [CrossRef]
- Larson, E.B.; Yao, X. Clinical empathy as emotional labor in the patient-physician relationship. J. Am. Med. Assoc. 2005, 293, 1100–1106. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Sleeboom-Faulkner, M. Tensions between medical professionals and patients in mainland China. Camb. Q. Healthc. Ethics 2011, 20, 458–465. [Google Scholar] [CrossRef]
- Kim, G.H.; Lee, H.S.; Jung, S.W.; Lee, J.G.; Lee, J.H.; Lee, K.J.; Kim, J.J. Emotional labor, workplace violence, and depressive symptoms in female Bank employees: A questionnaire survey using the K-ELS and K-WVS. Ann. Occup. Environ. Med. 2018, 30, 17. [Google Scholar] [CrossRef] [PubMed]
- Fang, H.; Zhao, X.; Yang, H.C.; Sun, P.; Li, Y.; Jiang, K.; Wu, Q. Depressive symptoms and workplace violence-related risk factors among otorhinolaryngology nurses and physicians in Northern China: A cross-sectional study. BMJ Open 2018, 8, e019514. [Google Scholar] [CrossRef] [PubMed]
- Hall, B.; Xiong, P.; Chang, K.; Yin, M.; Sui, X. Prevalence of medical workplace violence and the shortage of secondary and tertiary interventions among healthcare workers in China. J. Epidemiol. Community Health 2018, 72, 516–518. [Google Scholar] [CrossRef] [PubMed]
- Diefendorff, J.M.; Croyle, M.H.; Gosserand, R.H. The Dimensionality and Antecedents of Emotional Labor Strategies. J. Vocat. Behav. 2005, 66, 339–357. [Google Scholar] [CrossRef]
- Yasar, H.; Demir, S. The Mediating Role of Teachers’ Depression Levels on the Relationship between Emotional Labor and Burn-Out. Int. J. Educ. Methodol. 2015, 1, 1–8. [Google Scholar] [CrossRef]
- Pisaniello, S.L.; Winefield, H.R.; Delfabbro, P.H. The Influence of Emotional Labour and Emotional Work on the Occupational Health and Wellbeing of South Australian Hospital Nurses. J. Vocat. Behav. 2012, 80, 579–591. [Google Scholar] [CrossRef]
- Liu, L.; Xu, P.; Zhou, K.; Xue, J.; Wu, H. Mediating role of emotional labor in the association between emotional intelligence and fatigue among Chinese doctors: A cross-sectional study. BMC Public Health 2018, 18, 881. [Google Scholar] [CrossRef] [PubMed]
- Tang, K. A reciprocal interplay between psychosocial job stressors and worker well-being? A systematic review of the “reversed” effect. Scand. J. Work Environ. Health 2014, 40, 441–456. [Google Scholar] [CrossRef] [PubMed]
- Zapf, D. Emotion work and psychological well-being: A review of the literature and some conceptual considerations. Hum. Resour. Manag. Rev. 2002, 12, 237–268. [Google Scholar] [CrossRef]
- Netterstrøm, C.; Bech, F.; Olsen, R.; Stansfeld, S. The Relation between Work-related Psychosocial Factors and the Development of Depression. Epidemiol. Rev. 2008, 30, 118–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, J.A.; Feldman, D.C. Managing emotions in the workplace. J. Manag. Issues 1997, 9, 257–274. [Google Scholar]
- Hochschild, A. The Managed Heart: Commercialization of Human Feeling; University of California Press: Berkeley, CA, USA, 2003. [Google Scholar]
- Humphrey, R.; Ashforth, B.; Diefendorff, J. The bright side of emotional labor. J. Organ. Behav. 2015, 36, 749–769. [Google Scholar] [CrossRef]
- Riley, R.; Weiss, M.C. A qualitative thematic review: Emotional labour in healthcare settings. J. Adv. Nurs. 2016, 72, 6–17. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Han, S. Relationship between Emotional Labor Consequences and Employees’ Coping Strategy. Asia Pac. J. Tour. Res. 2009, 14, 225–239. [Google Scholar] [CrossRef]
- Hülsheger, U.; Schewe, A. On the Costs and Benefits of Emotional Labor: A Meta-Analysis of Three Decades of Research. J. Occup. Health Psychol. 2011, 16, 361–389. [Google Scholar] [CrossRef]
- Martínez-Iñigo, D.; Totterdell, P.; Alcover, C.M.; Holman, D. Emotional labour and emotional exhaustion: Interpersonal and intrapersonal mechanisms. Work Stress 2007, 21, 30–47. [Google Scholar] [CrossRef]
- Totterdell, P.; Holman, D.; Barling, J. Emotion Regulation in Customer Service Roles: Testing a Model of Emotional Labor. J. Occup. Health Psychol. 2003, 8, 55–73. [Google Scholar] [CrossRef]
- Schmidt, K.H.; Diestel, S. Are emotional labour strategies by nurses associated with psychological costs? A cross-sectional survey. Int. J. Nurs. Stud. 2014, 51, 1450–1461. [Google Scholar] [CrossRef]
- Yoon, S.; Kim, J. Job-related stress, emotional labor, and depressive symptoms among Korean nurses. J. Nurs. Scholarsh. Off. Publ. Sigma Theta Tau Int. Honor Soc. Nurs. 2013, 45, 169–176. [Google Scholar] [CrossRef]
- Yan, Z.; Xi, C.; Yiwen, C. Impact of emotional intelligence on emotional labor strategy: The mediating effects of general self-efficacy and organizational identification. In Proceedings of the 3rd International Conference on Computer Science and Service System, Bangkok, Thailand, 13–15 June 2014; Atlantis Press: Paris, France, 2014; pp. 207–210. [Google Scholar]
- Zung, W.W.K. A Self-Rating Depression Scale. Arch. Gen. Psychiatry 1965, 12, 63–70. [Google Scholar] [CrossRef]
- Field, A. Discovering Statistics Using IBM SPSS Statistics, 4th ed.; Sage: London, UK, 2013. [Google Scholar]
- Shi, J.; Wang, S.; Zhou, P.; Shi, L.; Zhang, Y.; Bai, F.; Xue, D.; Sun, Q. The Frequency of Patient-Initiated Violence and Its Psychological Impact on Physicians in China: A Cross-Sectional Study. PLoS ONE 2015, 10, e0128394. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.L. Sexual violence against women and children in Chinese societies. Trauma Violence Abuse 2009, 10, 69–85. [Google Scholar] [CrossRef] [PubMed]
- Geiger-Brown, J.; Muntaner, C.; Lipscomb, J.; Trinkoff, A. Demanding work schedules and mental health in nursing assistants working in nursing homes. Work Stress 2004, 18, 292–304. [Google Scholar] [CrossRef]
- Hayasaka, Y.; Nakamura, K.; Yamamoto, M.; Sasaki, S. Work environment and mental health status assessed by the general health questionnaire in female Japanese doctors. Ind. Health 2007, 45, 781–786. [Google Scholar] [CrossRef] [PubMed]
- Sparks, K.; Cooper, C.; Fried, Y.; Shirom, A. The effects of hours of work on health: A meta-analytic review. J. Occup. Organ. Psychol. 1997, 70, 391–408. [Google Scholar] [CrossRef]
- Dai, Y.; Zhang, B.; Sun, H.; Li, Z.; Shen, L.; Liu, Y. Prevalence and Correlates of Psychological Symptoms in Chinese Doctors as Measured with the SCL-90-R: A Meta-Analysis. Res. Nurs. Health 2015, 38, 369–383. [Google Scholar] [CrossRef] [PubMed]
- Shattell, M. Nurse–patient interaction: A review of the literature. J. Clin. Nurs. 2004, 13, 714–722. [Google Scholar] [CrossRef]
- Gabriel, A.; Daniels, M.; Diefendorff, J.; Greguras, G.; Chen, G. Emotional Labor Actors: A Latent Profile Analysis of Emotional Labor Strategies. J. Appl. Psychol. 2015, 100, 863–879. [Google Scholar] [CrossRef]
- Ye, M.; Chen, Y. A Literature Review on Teachers’ Emotional Labour. Creat. Educ. 2015, 6, 2232–2240. [Google Scholar] [CrossRef]
- Aytac, S.; Dursun, S. The effect on employees of violence climate in the workplace. Work 2012, 41, 3026–3031. [Google Scholar] [Green Version]
- Kim, H.; Choo, J. Emotional Labor: Links to Depression and Work-Related Musculoskeletal Disorders in Call Center Workers. Workplace Health Saf. 2017, 65, 346–354. [Google Scholar] [CrossRef] [PubMed]
- Yang, T.; Zhang, H.; Shen, F.; Li, J.W.; Wu, M.C. Appeal from Chinese doctors to end violence. Lancet 2013, 382, 1703–1704. [Google Scholar] [CrossRef]
- Parry, R. Are interventions to enhance communication performance in allied health professionals effective, and how should they be delivered? Direct and indirect evidence. Patient Educ. Couns. 2008, 73, 186–195. [Google Scholar] [CrossRef] [PubMed]
- Kolb, D. Experiential Learning: Experience as the Source of Learning and Development; FT Press: London, UK, 2014. [Google Scholar]
- Yardley, S.; Teunissen, P.W.; Dornan, T. Experiential learning: Transforming theory into practice. Med. Teach. 2012, 34, 161–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stewart, M. Towards a global definition of patient centred care: The patient should be the judge of patient centred care. BMJ 2001, 322, 444–445. [Google Scholar] [CrossRef] [PubMed]
- Hahn, S.; Hantikainen, V.; Needham, I.; Kok, G.; Dassen, T.; Halfens, R. Patient and visitor violence in the general hospital, occurrence, staff interventions and consequences: A cross-sectional survey. J. Adv. Nurs. 2012, 68, 2685–2699. [Google Scholar] [CrossRef] [PubMed]
- Nie, Y.; Mao, X.; Cui, H.; He, S.; Li, J.; Zhang, M. Hospital survey on patient safety culture in China. BMC Health Serv. Res. 2013, 13, 228. [Google Scholar] [CrossRef]
- Liu, C.; Liu, W.; Wang, Y.; Zhang, Z.; Wang, P. Patient safety culture in China: A case study in an outpatient setting in Beijing. BMJ Qual. Saf. 2014, 23, 556–564. [Google Scholar] [CrossRef]
- Aiken, L.H.; Sloane, D.M.; Clarke, S.; Poghosyan, L.; Cho, E.; You, L.; Finlayson, M.; Kanai-Pak, M.; Aungsuroch, Y. Importance of work environments on hospital outcomes in nine countries. Int. J. Qual. Health Care 2011, 23, 357–364. [Google Scholar] [CrossRef] [Green Version]
- Park, K.; Wilson, M.; Lee, M. Effects of social support at work on depression and organizational productivity. Am. J. Health Behav. 2004, 28, 444–455. [Google Scholar] [CrossRef]
- Hao, J.; Wang, J.; Liu, L.; Wu, W.; Wu, H.; Cooper, C. Perceived Organizational Support Impacts on the Associations of Work-Family Conflict or Family-Work Conflict with Depressive Symptoms among Chinese Doctors. Int. J. Environ. Res. Public Health 2016, 13, 326. [Google Scholar] [CrossRef] [PubMed]
- LaMontagne, A.D.; Martin, A.; Page, K.M.; Reavley, N.J.; Noblet, A.J.; Milner, A.J. Workplace mental health: Developing an integrated intervention approach. BMC Psychiatry 2014, 14, 131. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Groups | Frequency (N) | Percentage (%) |
|---|---|---|---|
| Age | ≤29 | 234 | 56.0 |
| 30–39 | 134 | 32.1 | |
| 40–49 | 39 | 9.3 | |
| ≥50 | 11 | 2.6 | |
| Gender | Male | 67 | 16.0 |
| Female | 351 | 84.0 | |
| Education | College | 117 | 28.0 |
| Bachelor’s degree | 239 | 57.2 | |
| Master’s degree | 56 | 13.4 | |
| Doctor | 6 | 1.1 | |
| Marital Status | Single | 183 | 43.8 |
| Married | 228 | 54.5 | |
| Divorced | 7 | 1.7 | |
| Job Role | Nurse | 306 | 73.2 |
| Physician | 112 | 26.8 | |
| Years of Employment | ≤9 | 276 | 66.0 |
| 10–19 | 107 | 25.6 | |
| 20–29 | 26 | 6.2 | |
| ≥30 | 9 | 2.2 | |
| Work Hours per Week | ≤39 | 70 | 16.7 |
| 40–49 | 268 | 64.1 | |
| 50–59 | 54 | 12.9 | |
| ≥60 | 26 | 6.3 | |
| Frequency of Healthcare Disturbance in the past 12 months | 0 | 157 | 37.5 |
| 1–4 times | 214 | 51.0 | |
| 5–8 times | 33 | 7.9 | |
| ≥9 times | 15 | 3.6 |
| M | SD | α | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Age | 30.40 | 7.39 | - | |||||||||||
| 2 | Gender | 1.84 | 0.37 | −0.182 *** | - | ||||||||||
| 3 | Education Level | 1.88 | 0.68 | 0.570 *** | −0.214 *** | - | |||||||||
| 4 | Marital Status | 1.60 | 0.59 | 0.706 *** | −0.139 ** | 0.395 *** | - | ||||||||
| 5 | Job Role | 1.27 | 0.44 | 0.348 *** | −0.339 *** | 0.573 *** | 0.156 ** | - | |||||||
| 6 | Years of Employment | 8.46 | 7.40 | 0.918 *** | −0.103 * | 0.409 *** | 0.682 *** | 0.144 ** | - | ||||||
| 7 | Hours of Work per Week | 43.23 | 7.64 | −0.073 | −0.043 | 0.096 * | −0.058 | 0.020 | −0.133 ** | - | |||||
| 8 | Healthcare Disturbance | 1.95 | 2.39 | 0.020 | −0.023 | 0.086 | 0.059 | 0.079 | −0.010 | 0.211 *** | - | ||||
| 9 | Surface Acting | 18.72 | 5.00 | 0.85 | 0.069 | 0.083 | 0.145 ** | 0.058 | 0.149 ** | 0.027 | 0.128 ** | 0.284 *** | - | ||
| 10 | Deep Acting | 12.33 | 2.88 | 0.70 | 0.071 | −0.013 | 0.039 | −0.080 | 0.109 * | −0.047 | 0.093 | 0.163 *** | 0.348 *** | - | |
| 11 | Depressive symptoms | 42.37 | 7.83 | 0.86 | −0.130 ** | 0.043 | −0.040 | −0.087 | −0.225 *** | −0.099 * | 0.163 *** | 0.214 *** | 0.166 *** | −0.037 | - |
| Variable | B [95% CI] | Std. Error B | Sr2 | ß | R | R2 | ΔR2 |
|---|---|---|---|---|---|---|---|
| Step 1 | 0.29 | 0.08 | 0.08 | ||||
| Job Role | −4.29 [−5.93, −2.65] *** | 0.84 | 0.006 | −0.24 | |||
| Work Hours | 0.20 [0.10, 0.29] *** | 0.048 | 0.004 | 0.19 | |||
| Step 2 | |||||||
| Job Role | −4.85 [−6.45, −3.24] *** | 0.82 | 0.007 | −0.28 | 0.38 | 0.14 | 0.136 |
| Work Hours | 0.14 [0.05, 0.24] ** | 0.05 | 0.002 | 0.14 | |||
| Healthcare Disturbance | 0.54 [0.23, 0.85] ** | 0.16 | 0.002 | 0.17 | |||
| Surface Acting | 0.24 [0.09, 0.39] ** | 0.08 | 0.002 | 0.15 |
| DV | M | Effect of IV on M | Effect of M on DV | Direct Effect | Indirect Effect | Total Effect |
|---|---|---|---|---|---|---|
| DS | SA | 0.54 *** | 0.22 ** | 0.55 *** | 0.12 * | 0.67 *** |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tang, N.; Thomson, L.E. Workplace Violence in Chinese Hospitals: The Effects of Healthcare Disturbance on the Psychological Well-Being of Chinese Healthcare Workers. Int. J. Environ. Res. Public Health 2019, 16, 3687. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16193687
Tang N, Thomson LE. Workplace Violence in Chinese Hospitals: The Effects of Healthcare Disturbance on the Psychological Well-Being of Chinese Healthcare Workers. International Journal of Environmental Research and Public Health. 2019; 16(19):3687. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16193687
Chicago/Turabian StyleTang, Nan, and Louise E. Thomson. 2019. "Workplace Violence in Chinese Hospitals: The Effects of Healthcare Disturbance on the Psychological Well-Being of Chinese Healthcare Workers" International Journal of Environmental Research and Public Health 16, no. 19: 3687. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16193687