Identifying Risk Profiles of School Refusal Behavior: Differences in Social Anxiety and Family Functioning Among Spanish Adolescents

 ,
,  ,
,
Abstract
:1. Introduction
1.1. School Refusal Behavior Profiles
1.2. School Refusal Behavior and Social Anxiety
1.3. School Refusal Behavior and Family Functioning
1.4. The Present Study
2. Materials and Methods
2.1. Participants
2.2. Measures
2.3. Procedure
2.4. Statistical Analyses
3. Results
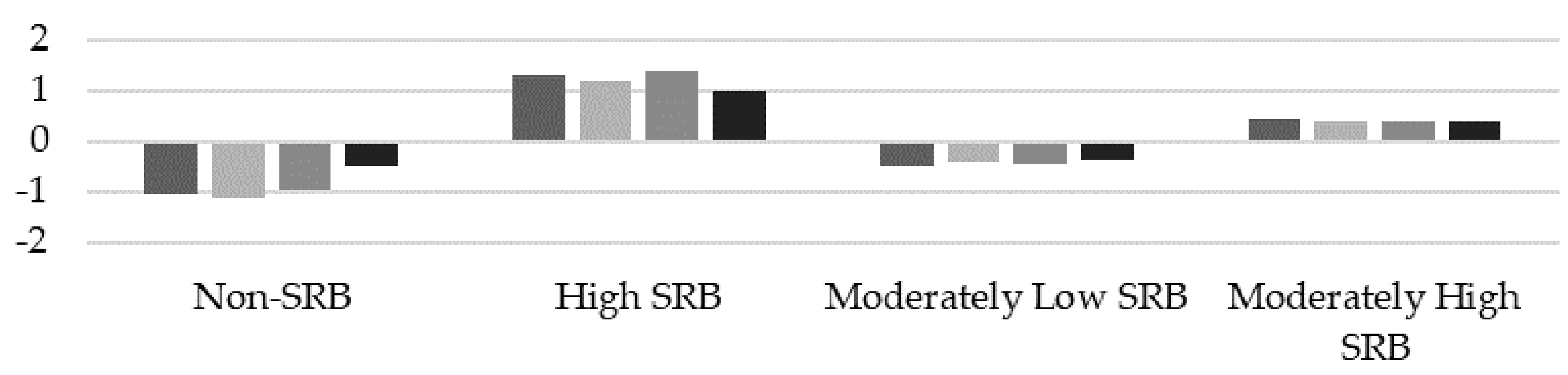
3.1. Identification of School Refusal Behavior Profiles
3.2. Intergroup Differences in Social Anxiety
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Hendron, M.; Kearney, C.A. Bridging the gap between assessment and treatment of youths with school refusal behavior: What to do when clients ask “what now”? J. Clin. Psychol. 2011, 2, 14–21. [Google Scholar]
- Pina, A.A.; Zerr, A.A.; Gonzales, N.A.; Ortiz, C.D. Psychosocial interventions for school refusal behavior in children and adolescents. Child Dev. Perspect. 2009, 3, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Ingul, J.M.; Klockner, C.A.; Silverman, W.K.; Nordahl, H.M. Adolescent school absenteeism: Modelling social and individual risk factors. Child Adolesc. Ment. Health 2012, 17, 93–100. [Google Scholar] [CrossRef]
- Thornton, M.; Darmody, M.; McCoy, S. Persistent absenteeism among Irish primary school pupils. Educ. Rev. 2013, 65, 488–501. [Google Scholar] [CrossRef]
- Prakash, R.; Beattie, T.; Javalkar, P.; Bhattacharjee, P.; Ramanaik, S.; Thalinja, R.; Murthy, S.; Davey, C.; Blanchard, J.; Watts, C.; et al. Correlates of school dropout and absenteeism among adolescent girls from marginalized community in north Karnataka, south India. J. Adolesc. 2017, 61, 64–76. [Google Scholar] [CrossRef]
- Nayak, A.; Sangoi, B.; Nachane, H. School Refusal Behavior in Indian Children: Analysis of Clinical Profile, Psychopathology and Development of a Best-Fit Risk Assessment Model. Indian J. Pediatr. 2018, 85, 1073–1078. [Google Scholar] [CrossRef]
- Dembo, R.; Briones-Robins, R.; Barrett, K.; Winters, K.C.; Schmeidler, J.; Ungaro, R.A.; Karas, L.; Belenko, S.; Gulledge, L. Mental health, substance use, and delinquency among truant youth in a brief intervention Project: A longitudinal study. J. Emot. Behav. Disord. 2013, 21, 176–192. [Google Scholar] [CrossRef]
- Bridgeland, J.M.; Dilulio, J.J.; Morison, K.B. The Silent Epidemic: Perspectives of High School Dropouts; Bill and Melinda Gates Foundation: Seattle, WA, USA, 2006. [Google Scholar]
- Eaton, D.K.; Brener, N.; Kann, L.K. Associations of Health Risk Behaviors with School Absenteeism. Does Having Permission for the Absence Make a Difference? J. Sch. Health 2008, 78, 223–229. [Google Scholar] [CrossRef]
- Kandel, D.B.; Treiman, D.; Faust, R.; Single, E. Adolescent involvement in legal and illegal drug use: A multiple classification analysis. Soc. Forces 1976, 55, 438–458. [Google Scholar] [CrossRef]
- Hill, D.; Mrug, S. School-level correlates of adolescent tobacco, alcohol, and marijuana use. Subst. Use Misuse 2015, 50, 1518–1528. [Google Scholar] [CrossRef]
- Henry, K.L.; Thornberry, T.P. Truancy and escalation of substance use during adolescence. J. Stud. Alcohol Drugs 2010, 71, 115–124. [Google Scholar] [CrossRef] [PubMed]
- King, N.; Bernstein, G. School refusal in children and adolescents: A review of the past 10 years. J. Am. Acad. Child. Adolesc. Psychiatr. 2001, 40, 197–205. [Google Scholar] [CrossRef] [PubMed]
- Kearney, C.A. School absenteeism and school refusal behavior in youth: A contemporary review. Clin. Psychol. Rev. 2008, 28, 451–471. [Google Scholar] [CrossRef] [PubMed]
- Heyne, D.; Gren-Landell, M.; Melvin, G.; Gentle-Genity, C. Differentiation between school attendance problems: Why and how? Cogn. Behav. Pract. 2019, 26, 8–34. [Google Scholar] [CrossRef]
- Kearney, C.A.; Silverman, W.K. A preliminary analysis of a functional model of assessment and treatment for school refusal behavior. Behav. Modif. 1990, 14, 340–366. [Google Scholar] [CrossRef] [PubMed]
- Kearney, C.A.; Silverman, W.K. Measuring the function of school refusal behavior: The School Refusal Assessment Scale. J. Clin. Child Psychol. 1993, 22, 85–96. [Google Scholar] [CrossRef]
- Kearney, C.A. Identifying the function of school refusal behavior: A revision of the School Refusal Assessment Scale. J. Psychopathol. Behav. Assess. 2002, 24, 235–245. [Google Scholar] [CrossRef]
- Gonzálvez, C.; Inglés, C.J.; Kearney, C.A.; Vicent, M.; Sanmartín, R.; García-Fernández, J.M. School Refusal Assessment Scale-Revised: Factorial invariance and latent means differences across gender and age in Spanish children. Front. Psychol. 2016, 7. [Google Scholar] [CrossRef]
- Gonzálvez, C.; Kearney, C.A.; Lagos-San Martín, N.; Sanmartín, R.; Vicent, M.; Inglés, C.J.; García-Fernández, J.M. School Refusal Assessment Scale-Revised Chilean version: Factorial invariance and latent means differences across gender and age. J. Psychoeduc. Assess. 2017, 36, 835–843. [Google Scholar] [CrossRef]
- Gonzálvez, C.; Inglés, C.J.; Sanmartín, R.; Vicent, M.; Calderón, C.M.; García-Fernández, J.M. Testing factorial invariance and latent means differences of the School Refusal Assessment Scale-Revised in Ecuadorian adolescents. Curr. Psychol. 2018, 1–10. [Google Scholar] [CrossRef]
- Berg, I.; Butler, A.; Franklin, J.; Hayes, H.; Lucas, C.; Sims, R. DSM-III-R Disorders, social factors and management of school attendance problems in the normal population. J. Child Psychol. Psychiatry 1993, 34, 1187–1203. [Google Scholar] [CrossRef] [PubMed]
- Bools, C.; Foster, J.; Brown, I.; Berg, I. The identification of psychiatric disorders in children who fail to attend school: A cluster analysis of a non-clinical population. Psychol. Med. 1990, 20, 171–181. [Google Scholar] [CrossRef] [PubMed]
- Dube, S.R.; Orpinas, P. Understanding excessive school absenteeism as school refusal behavior. Child. Sch. 2009, 31, 87–95. [Google Scholar] [CrossRef]
- Gonzálvez, C.; Inglés, C.J.; Fernández-Sogorb, A.; Sanmartín, R.; Vicent, M.; García-Fernández, J.M. Profiles derived from the School Refusal Assessment Scale-Revised and its relationship to anxiety. Educ. Psychol. 2018, 1–14. [Google Scholar] [CrossRef]
- Gonzálvez, C.; Inglés, C.J.; Sanmartín, R.; Vicent, M.; Fernández-Sogorb, A.; García-Fernández, J.M. A cluster analysis of school refusal behavior: Identification of profiles and risk for school anxiety. Int. J. Educ. Res. 2018, 90, 43–49. [Google Scholar] [CrossRef]
- Gonzálvez, C.; Inglés, C.J.; Kearney, C.A.; Sanmartín, R.; Vicent, M.; García-Fernández, J.M. Relationship between school refusal behavior and social functioning: A cluster analysis approach. Eur. J. Educ. Psychol. 2019, 12, 17–29. [Google Scholar] [CrossRef]
- Gonzálvez, C.; Kearney, C.A.; Jiménez-Ayala, C.E.; Sanmartín, R.; Vicent, M.; Inglés, C.J.; García-Fernández, J.M. Functional profiles of school refusal behavior and their relationship with depression, anxiety and stress. Psychiatry Res. 2018, 269, 140–144. [Google Scholar] [CrossRef]
- Costello, E.J.; Egger, H.L.; Copeland, W.; Erkanli, A.; Angold, A. The developmental epidemiology of anxiety disorders: Phenomenology, prevalence, and comorbidity. In Anxiety Disorders in Children and Adolescents: Research, Assessment and Intervention; Silverman, W.K., Field, A., Eds.; Cambridge University Press: Cambridge, UK, 2011; pp. 56–75. [Google Scholar]
- Martín, L.; Reyes, Z. Sexual behavior, pregnancy and abortion in adolescence. A comprehensive approach to health promotion. Rev. Cubana Salud Pública 2003, 29, 183–187. [Google Scholar]
- Bernstein, G.A.; Bernat, D.H.; Davis, A.A.; Layne, A.E. Symptom presentation and classroom functioning in a nonclinical sample of children with social phobia. Depress. Anxiety 2008, 25, 752–760. [Google Scholar] [CrossRef]
- Khalid-Khan, S.; Santibanez, M.P.; McMicken, C.; Rynn, M.A. Social anxiety disorder in children and adolescents: Epidemiology, diagnosis and treatment. Paediatr. Drugs 2007, 9, 227–237. [Google Scholar] [CrossRef]
- Van Amerigen, M.; Mancini, C.; Farvolden, P. The impact of anxiety disorders on educational achievement. J. Anxiety Disord. 2003, 17, 561–571. [Google Scholar] [CrossRef]
- Beidel, D.C.; Turner, S.M.; Young, B.J.; Ammerman, R.T.; Sallee, F.R.; Crosby, L. Psychopathology of adolescent social phobia. J. Psychopathol. Behav. Assess. 2007, 29, 47–54. [Google Scholar] [CrossRef]
- Blote, A.W.; Kint, M.J.; Westenberg, P.M. Peer behavior toward socially anxious adolescents: Classroom observations. Behav. Res. Ther. 2007, 45, 2773–2779. [Google Scholar] [CrossRef] [PubMed]
- Erath, S.A.; Flanagan, K.S.; Bierman, K.L. Social anxiety and peer relations in early adolescence: Behavioral and cognitive factors. J. Abnorm. Child. Psychol. 2007, 35, 405–416. [Google Scholar] [CrossRef] [PubMed]
- Greco, L.A.; Morris, T.L. Factors influencing the link between social anxiety and peer acceptance: Contributions of social skills and close friendships during middle childhood. Behav. Ther. 2005, 36, 197–205. [Google Scholar] [CrossRef]
- Kingery, J.N.; Erdley, C.A.; Marshall, K.C.; Whitaker, K.G.; Reuter, T.R. Peer experiences of anxious and socially withdrawn youth: An integrative review of the developmental and clinical literature. Clin. Child Fam. Psychol. Rev. 2010, 13, 91–128. [Google Scholar] [CrossRef]
- La Greca, A.M.; López, N. Social anxiety among adolescents: Linkages with peer relations and friendships. J. Abnorm. Child Psychol. 1998, 26, 83–94. [Google Scholar] [CrossRef]
- Schneier, B.H.; Tessier, N.G. Close friendship as understood by socially withdrawn, anxious early adolescents. Child Psychiatry Hum. Dev. 2007, 38, 339–351. [Google Scholar] [CrossRef]
- Richards, H.J.; Hadwin, J.A. An exploration of the relationship between trait anxiety and school attendance in young people. Sch. Ment. Health 2011, 3, 236–244. [Google Scholar] [CrossRef]
- Kearney, C.A.; Albano, A. The functional profiles of school refusal behavior: Diagnostic aspects. Behav. Modif. 2004, 28, 147–161. [Google Scholar] [CrossRef]
- Egger, H.L.; Costello, E.J.; Angold, A. School refusal and psychiatry disorders: A community study. J. Am. Acad. Child Adolesc. Psychiatry 2003, 42, 797–807. [Google Scholar] [CrossRef] [PubMed]
- Ingul, J.M.; Nordahl, H.M. Anxiety as a risk factor for school absenteeism: What differentiates anxious school attenders from non-attenders? Ann. Gen. Psychiatry 2013, 12, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Birmaher, B.; Brent, D.A.; Chiappetta, L.; Bridge, J.; Monga, S.; Baugher, M. Psychometric properties of the Screen for Child Anxiety Related Emotional Disorders (SCARED): A replication study. J. Am. Acad. Child Adolesc. Psychiatry 1999, 38, 1230–1236. [Google Scholar] [CrossRef]
- Strayhorn, T.L. Student Development Theory in Higher Education: A Social Psychological Approach; Routledge Taylor & Francis: New York, NY, USA, 2016. [Google Scholar]
- Arias, W. Aggression and violence in adolescence: The importance of the family. Av. Psicol. 2013, 22, 23–34. [Google Scholar]
- Cezar, P.K.; Rodrigues, P.M.; Arpini, D.M. Psychology in the Family Health Strategy: Multiprofessional Residence Experiences. Psicol. Ciênc. Prof. 2015, 35, 211–224. [Google Scholar] [CrossRef]
- Smilkstein, G. The Family APGAR: A proposal for a family function test and its use by physicians. J. Fam. Pract. 1978, 6, 1231–1239. [Google Scholar] [PubMed]
- Weymouth, B.B.; Buehler, C.; Zhou, N.; Henson, R.A. A meta-analysis of parent-adolescent conflict: Disagreement, hostility, and youth maladjustment. J. Fam. Theory Rev. 2016, 8, 95–112. [Google Scholar] [CrossRef]
- Hersov, L. School refusal. In Child and Adolescent Psychiatry: Modern Approaches, 2nd ed.; Rutter, M., Hersov, L., Eds.; Blackwell Scientific Publications: Oxford, UK, 1985; pp. 382–399. [Google Scholar]
- Waldron, S.; Shrier, D.K.; Stone, B.; Tobin, S. School phobia and other childhood neuroses. Am. J. Psychiatry 1975, 132, 802–808. [Google Scholar]
- Gubbels, J.; Van der Put, C.E.; Assink, M. Risk Factors for School Absenteeism and Dropout: A Meta-Analytic Review. J. Youth Adolesc. 2019, 48, 1637–1667. [Google Scholar] [CrossRef] [Green Version]
- Lagana, M.T. Protective factors for inner-city adolescents at risk of school dropout: Family factors and social support. Child. Sch. 2004, 26, 211–220. [Google Scholar] [CrossRef]
- Sahin, S.; Arseven, Z.; Kiliç, A. Causes of student absenteeism and school dropouts. Int. J. Instr. 2016, 9, 195–210. [Google Scholar] [CrossRef]
- Bernstein, G.A.; Garfinkel, B.D.; Borchardt, C.M. Comparative studies of pharmacotherapy for school refusal. J. Am. Acad. Child Adolesc. Psychiatry 1990, 29, 773–781. [Google Scholar] [CrossRef] [PubMed]
- Skinner, H.A.; Steinhauer, P.D.; Santa-Barbara, J. The Family Assessment Measure. Can. J. Commun. Ment. Health 1983, 2, 91–105. [Google Scholar] [CrossRef]
- Bernstein, G.A.; Borchardt, C.M. School refusal: Family constellation and family functioning. J. Anxiety Disord. 1996, 10, 1–19. [Google Scholar] [CrossRef]
- Kearney, C.A.; Silverman, W.K. Family environment of youngsters with school refusal behavior: A synopsis with implications for assessment and treatment. Am. J. Fam. Ther. 1995, 23, 59–72. [Google Scholar] [CrossRef]
- Moos, R.H.; Moos, B.S. Family Environment Scale Manual, 2nd ed.; Consulting Psychologists Press: Palo Alto, CA, USA, 1986. [Google Scholar]
- Smith, J.C.; Ryan, B.A.; Adams, G.R.; Dalicandro, T. Distinguishing absentee students from regular attenders: The combined influence of personal, family and school factors. J. Youth Adolesc. 1998, 27, 629–640. [Google Scholar] [CrossRef]
- Kawash, G.F.; Clewes, J.L. A factor analysis of a short form of the CRPBI: Are childrens’ perceptions of control and discipline multidimensional? J. Psychol. 1987, 122, 57–67. [Google Scholar] [CrossRef]
- Bernstein, G.A.; Warren, S.L.; Massie, E.D.; Thuras, P.D. Family dimensions in anxious-depressed school refusers. J. Anxiety Disord. 1999, 13, 513–528. [Google Scholar] [CrossRef]
- Olson, D.H.; McCubbin, H.I.; Barnes, H.; Larsen, A.; Muxen, M.; Wilson, M. Families: What Makes Them Work; Sage: Beverly Hills, CA, USA, 1983. [Google Scholar]
- Kiani, C.; Otero, K.; Taufique, S.; Ivanov, I. Chronic Absenteeism: A Brief Review of Causes, Course and Treatment. Adolesc. Psychiatry 2018, 8, 214–230. [Google Scholar] [CrossRef]
- Bahali, K.; Tahiroglu, A.Y.; Avci, A.; Seydaoglu, G. Parental psychological symptoms and familial risk factors of children and adolescents who exhibit school refusal. East. Asian Arch. Psychiatry 2011, 21, 164–169. [Google Scholar]
- Schreiber, J.B. Latent class analysis: An example for reporting results. Res. Soc. Adm. Pharm. 2017, 13, 1196–1201. [Google Scholar] [CrossRef] [PubMed]
- Lanza, S.T.; Rhoades, B.L. Latent class analysis: An alternative perspective on subgroup analysis in prevention and treatment. Prev. Sci. 2013, 14, 157–168. [Google Scholar] [CrossRef] [PubMed]
- Heyne, D.; Sauter, F.M.; Van Widenfelt, B.M.; Vermeiren, R.; Westenberg, P.M. School refusal and anxiety in adolescence: Non-randomized trial of a developmentally sensitive cognitive behavioral therapy. J. Anxiety Disord. 2011, 25, 870–878. [Google Scholar] [CrossRef] [PubMed]
- Prabhuswamy, M.; Srinath, S.; Girimaji, S.; Seshadri, S. Outcome of children with school refusal. Indian J. Pediatr. 2007, 74, 375–379. [Google Scholar] [CrossRef] [PubMed]
- Smilkstein, G.; Ashworth, C.; Montano, D. Validity and reliability of the family APGAR as a test of family function. J. Fam. Pract. 1982, 15, 303–311. [Google Scholar] [PubMed]
- Bellón, J.; Delgado, A.; Luna, J.; Lardelli, P. Validity and reliability of family function insurance Apgar familiar. Aten. Primaria 1996, 8, 289–295. [Google Scholar]
- Nyland, K.L.; Asparouhov, T.; Muthén, B.O. Deciding on the number of classes in latent class analysis and growth mixture modelling: A monte carlo simulation study. Struct. Equ. Modeling 2007, 14, 535–569. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Academic Press: New York, NY, USA, 1988. [Google Scholar]
- Knollmann, M.; Reissner, V.; Kiessling, S.; Hebebrand, J. The differential classification of school avoidance: A cluster-analytic investigation. Z. Kinder Jugendpsychiatr. Psychother. 2013, 41, 335–345. [Google Scholar] [CrossRef]
- Sheldon, S.B.; Epstein, J.L. Getting students to school: Using family and community involvement to reduce chronic absenteeism. Sch. Comm. J. 2004, 14, 39–56. [Google Scholar]
- Carless, B.; Melvin, G.A.; Tonge, B.J.; Newman, L.K. The role of parental self-efficacy in adolescent school-refusal. J. Family Psychol. 2015, 29, 162–170. [Google Scholar] [CrossRef]
- Chen, Y.; Chen, C.; Hsu, S.; Lin, C. A preliminary study of family APGAR index. Acta Paediatr. Sinica 1980, 21, 210–217. [Google Scholar]
- Gardner, W.; Ntting, P.; Kelleher, K.; Werner, J.; Farley, T.; Stewart, L.; Hartsell, M.; Orzano, A. Does the family APGAR effectively measure family functioning? J. Fam. Pract. 2001, 50, 19–25. [Google Scholar] [PubMed]
- Forero, L.; Avendaño, M.; Duarte, Z.; Campo-Arias, A. Internal Consistency and Analysis of APGAR Scale Factors to Evaluate Family Functioning in Secondary School Students. Revista Colombiana de Psiquiatría 2006, 35, 23–39. [Google Scholar]
- Castilla, H.; Caycho, T.; Ventura, J.; Palomino, M.; De la Cruz, M. Factorial analysis confirming Smilkstein’s family functioning perception scale in Peruvian adolescents. Salud Soc. 2015, 6, 140–153. [Google Scholar] [CrossRef]
- Fuentes, M.C.; García-Ros, R.; Pérez-González, F.; Sancerni, D. Effects of parenting styles on self-regulated learning and academic stress in Spanish adolescents. Int. J. Environ. Res. Public Health 2019, 16, 2778. [Google Scholar] [CrossRef] [PubMed]
- García, O.F.; Serra, E. Raising children with poor school performance: Parenting styles and short- and long-term consequences for adolescent and adult development. Int. J. Environ. Res. Public Health 2019, 16, 1089. [Google Scholar] [CrossRef]
- García, F.; Serra, E.; García, O.F.; Martínez, I.; Cruise, E. A third emerging stage for the current digital society? optimal parenting styles in Spain, the United States, Germany, and Brazil. Int. J. Environ. Res. Public Health 2019, 16, 2333. [Google Scholar] [CrossRef] [PubMed]
- Musitu, G.; García, F. ESPA29: Parental Socialization Scale in Adolescence; TEA: Madrid, Spain, 2001. [Google Scholar]
- Rohner, R.P. Parental Acceptance-Rejection/Control Questionnaire (PARQ/Control); Rohner Research Publications: Storrs, CT, USA, 1989. [Google Scholar]
- King, N.J.; Heyne, D.; Tonge, B.; Gullone, E.; Ollendick, T.H. School refusal: Categorical diagnoses, functional analysis and treatment planning. Clin. Psychol. Psychother. 2001, 8, 352–360. [Google Scholar] [CrossRef]
- World Health Organization. Health for the World’s Adolescents. A Second Chance in the Second Decade; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Salam, R.A.; Das, J.K.; Lassi, Z.S.; Bhutta, Z.A. Adolescent health and well-being: Background and methodology for review of potential interventions. J. Adolesc. Health 2016, 59, 4–10. [Google Scholar] [CrossRef]
- Kearney, C.A. Managing School Absenteeism at Multiple Tiers: An Evidence-Based and Practical Guide for Professionals; Oxford University Press: New York, NY, USA, 2016. [Google Scholar]
- Banerjee, R.; Weare, K.; Farr, W. Working with Social and Emotional Aspects of Learning (SEAL): Association with school ethos, pupil social experiences, attendance and attainment. Br. Educ. Res. 2013, 40, 718–742. [Google Scholar] [CrossRef]
- Snyder, F.; Flay, B. Impact of a social-emotional and character development program on school-level indicators of academic achievement, absenteeism, and disciplinary outcomes: A matched-pair, cluster randomized, controlled trial. J. Res. Educ. Eff. 2010, 3, 26–55. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Gender | Age | Total | |||
|---|---|---|---|---|---|
| 15 | 16 | 17 | 18 | ||
| Boys | 204 | 299 | 228 | 134 | 865 |
| 11.1% | 16.2% | 12.4% | 7.3% | 47% | |
| Girls | 260 | 310 | 259 | 148 | 977 |
| 14.1% | 16.8% | 14.1% | 8% | 53% | |
| Total | 464 | 609 | 487 | 282 | 1842 |
| 25.2% | 33% | 26.5% | 15.3% | 100% | |
| Number of Classes | Bayesian Information Criterion (BIC) | Entropy |
|---|---|---|
| 2 classes | 18101.54 | 0.72 |
| 3 classes | 17427.31 | 0.74 |
| 4 classes | 17199.87 | 0.75 |
| 5 classes | 17262.62 | 0.70 |
| SAS-A 1 Dimensions | Non-SRB 5 | High SRB | Moderately Low SRB | Moderately High SRB | Statistical Significance | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | M | SD | F (3,1839) | η2p | |
| FNE 2 | 14.07 | 5.74 | 19.59 | 7.49 | 16.04 | 5.33 | 18.97 | 6.18 | 59.34 * | 0.09 |
| SAD-New 3 | 12.01 | 4.78 | 16.53 | 5.47 | 13.78 | 4.43 | 15.29 | 4.71 | 46.38 * | 0.07 |
| SAD-General 4 | 7.55 | 3.29 | 10.35 | 3.97 | 8.74 | 3.13 | 10.21 | 3.48 | 48.23 * | 0.08 |
| APGAR | 14.92 | 3.16 | 12.31 | 2.80 | 14.15 | 2.91 | 12.88 | 2.89 | 51.22 * | 0.08 |
| Dimensions SAS-A 1 | Moderately Low SRB 5 vs. Moderately High SRB | Moderately Low SRB vs. High SRB | Moderately Low SRB vs. Non-SRB | Moderately High SRB vs. High SRB | Moderately High SRB vs. Non-SRB | High SRB vs. Non-SRB |
|---|---|---|---|---|---|---|
| FNE 2 | −0.51 | −0.60 | 0.36 | - | 0.81 | 0.82 |
| SAD-N 3 | −0.33 | −0.58 | 0.39 | −0.25 | 0.69 | 0.88 |
| SAD-G 4 | −0.45 | −0.48 | 0.38 | - | 0.78 | 0.77 |
| APGAR | 0.44 | 0.64 | −0.26 | - | −0.69 | −0.88 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gonzálvez, C.; Díaz-Herrero, Á.; Sanmartín, R.; Vicent, M.; Pérez-Sánchez, A.M.; García-Fernández, J.M. Identifying Risk Profiles of School Refusal Behavior: Differences in Social Anxiety and Family Functioning Among Spanish Adolescents. Int. J. Environ. Res. Public Health 2019, 16, 3731. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16193731
Gonzálvez C, Díaz-Herrero Á, Sanmartín R, Vicent M, Pérez-Sánchez AM, García-Fernández JM. Identifying Risk Profiles of School Refusal Behavior: Differences in Social Anxiety and Family Functioning Among Spanish Adolescents. International Journal of Environmental Research and Public Health. 2019; 16(19):3731. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16193731
Chicago/Turabian StyleGonzálvez, Carolina, Ángela Díaz-Herrero, Ricardo Sanmartín, María Vicent, Antonio M. Pérez-Sánchez, and José M. García-Fernández. 2019. "Identifying Risk Profiles of School Refusal Behavior: Differences in Social Anxiety and Family Functioning Among Spanish Adolescents" International Journal of Environmental Research and Public Health 16, no. 19: 3731. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16193731