Patient Input in Regional Healthcare Planning—A Meaningful Contribution


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Data Collection
2.2. Statistical Analysis
3. Results
3.1. Study Regions and Population
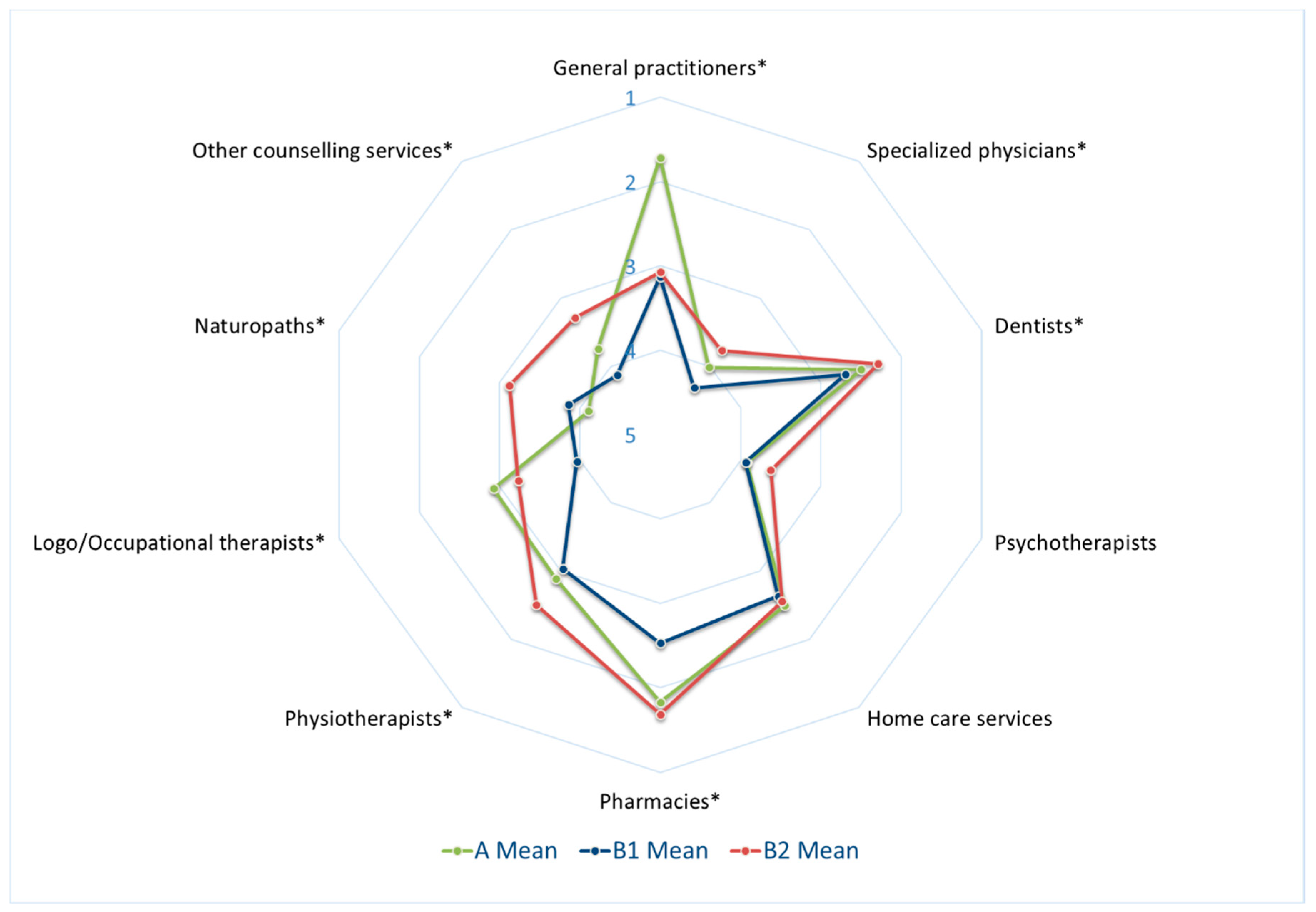
3.2. Differences of HCS Ratings across Regions
3.3. Influence of Regional and Socioeconomic Characteristics on Ratings of HCS
3.3.1. Ratings of HCS Provided by GPs
3.3.2. Ratings of HCS Provided by Specialist Physicians
4. Discussion
4.1. Study Population and Self-Reported Health
4.2. Specific Rating of Different Healthcare Providers
4.3. Factors Influencing Perception of Healthcare Quality
4.3.1. Age: Young Citizens Tend to Give Lower Ratings
4.3.2. Income: Lower Income and Better Rating
4.3.3. Region Has the Strongest Influence
4.3.4. Citizens Can Provide Important Additional Insights for Planning
4.4. Limitations
4.5. Future Prospects
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Osborn, R.; Squires, D.; Doty, M.M.; Sarnak, D.O.; Schneider, E.C. In New Survey of 11 Countries, U.S. Adults Still Struggle with Access to and Affordability of Health Care. Health Aff. 2016, 33, 2327–2336. [Google Scholar] [CrossRef] [PubMed]
- Busse, R.; Stahl, J. Integrated care experiences and outcomes in Germany, the Netherlands, and England. Health Aff. 2014, 33, 1549–1558. [Google Scholar] [CrossRef] [PubMed]
- Hajek, A.; Bock, J.O.; König, H.H. Which factors affect health care use among older Germans? Results of the German ageing survey. BMC Health Serv. Res. 2017, 17, 30. [Google Scholar] [CrossRef] [PubMed]
- Bauer, J.; Maier, W.; Muller, R.; Groneberg, D.A. Primary Care in Germany—Equal Access for Everyone? Dtsch. Med. Wochenschr. 2018, 143, e9–e17. [Google Scholar] [CrossRef] [PubMed]
- Steinhauser, J.; Annan, N.; Roos, M.; Szecsenyi, J.; Joos, S. Approaches to reduce shortage of general practitioners in rural areas--results of an online survey of trainee doctors. Dtsch. Med. Wochenschr. 2011, 136, 1715–1719. [Google Scholar] [CrossRef]
- Fendrich, K.; van den Berg, N.; Siewert, U.; Hoffmann, W. Demographic change: Demands on the health care system and solutions using the example of Mecklenburg-Western Pomerania. Bundesgesundheitsblatt Gesundh. Gesundh. 2010, 53, 479–485. [Google Scholar] [CrossRef]
- Gerlach, F.M.; Greiner, W.; Haubitz, M.; Schaeffer, D.; Thürmann, P.; Thüsing, G.; Wille, E. Bedarfsgerechte Versorgung—Perspektiven für Ländliche Regionen und ausgewählte Leistungsbereiche [Needs-Based Care—Perspectives for Rural Regions and Selected Service Areas]. Sachverständigenrats zur Begutachtung der Entwicklung im Gesundheitswesen [Subject Council on the Evaluation of Developments in the Health Sector]: Berlin/Bonn, Germany, 2014. Available online: https://www.svr-gesundheit.de/fileadmin/user_upload/Gutachten/2014/SVR-Gutachten_2014_Langfassung.pdf (accessed on 31 August 2019).
- Hamel, K.; Ewers, M.; Schaeffer, D. Health care and regional disparities. Z. Gerontol. Geriatr. 2013, 46, 323–328. [Google Scholar] [CrossRef] [PubMed]
- Bertelsmann Stiftung. Demographie Konkret—Handlungsansätze für die Kommunale Praxis. Concrete Demography—Recommendations Action for Municipal Practice. Available online: https://www.wegweiser-kommune.de/documents/10184/16915/Demographie+konkret+2005.pdf/afdce20f-0169-4f3d-927e-f4af6a383788 (accessed on 31 August 2019).
- Bundestag [German parliament]. GKV-Versorgungsstärkungsgesetz [GKV supply strengthening law]. Bonn, Germany. 2015. Available online: https://www.bgbl.de/xaver/bgbl/start.xav?startbk=Bundesanzeiger_BGBl&jumpTo=bgbl115s1211.pdf#__bgbl__%2F%2F*%5B%40attr_id%3D%27bgbl115s1211.pdf%27%5D__1531733096996 (accessed on 31 August 2019).
- The Federal Joint Committee. Richtlinie des Gemeinsamen Bundesausschusses über die Bedarfsplanung sowie die Maßstäbe zur Feststellung von Überversorgung und Unterversorgung in der vertragsärztlichen Versorgung (Bedarfsplanungs-Richtlinie) [Directive of the Joint Federal Committee on Demand Planning and the Standards for Determining Overuse and Underuse in SHI-accredited Physician Care (Demand Planning Directive)]. Available online: https://www.g-ba.de/downloads/62-492-1522/BPL-RL_2017-11-17_iK-2018-01-01.pdf (accessed on 31 August 2019).
- Sundmacher, L.; Schang, L.; Schüttig, W.; Flemming, R.; Frank-Tewaag, J.; Geiger, I.; Franke, S.; Wende, D.; Weinhold, I.; Höser, C.; et al. Gutachten zur Weiterentwicklung der Bedarfsplanung i.S.d. §§ 99 ff. SGB V zur Sicherung der Vertragsärztlichen Versorgung [Expert Opinion on the Further Development of Demand Planning in Terms of §§ 99 ff. SGB V to Ensure the pROVISION of SHI-Accredited Physician Care]; Gemeinsamer Bundesausschuss [Joint Federal Committee]: München, Leipzig, Bonn, Greifswald and Köln, Germany, 2018; Available online: https://www.g-ba.de/downloads/39-261-3493/2018-09-20_Endbericht-Gutachten-Weiterentwickklung-Bedarfsplanung.pdf (accessed on 31 August 2019).
- Graf von Stillfried, D.; Czihal, T. What do functionally defined populations contribute to the explanation of regional differences in medical care? Bundesgesundheitsblatt Gesundh. Gesundh. 2014, 57, 197–206. [Google Scholar] [CrossRef]
- Schafer, I.; Hansen, H.; Pohontsch, N.; Bole, L.; Wagner, H.O.; Fuhr, M.; Luhmann, D.; Scherer, M. Regional variation of patient behaviour and reasons for consultation in the general practice of Northern Germany: Protocol for an observational study. BMJ Open 2016, 6, e010738. [Google Scholar] [CrossRef]
- Sturm, H.; Hermann, T.; Joos, S. Versorgungsplanung für den Landkreis Waldshut [Supply Planning for the Rural District Waldshut]; Institute of General Practice and Interprofessional Care; University Tübingen: Tübingen, Germany, 2017; Available online: http://www.landkreis-waldshut.de/fileadmin/landkreis-waldshut.de/media/gesundheitsamt/Abschlussbericht-Projektstudie-final.pdf (accessed on 31 August 2019).
- Clarke, J.L.; Bourn, S.; Skoufalos, A.; Beck, E.H.; Castillo, D.J. An innovative approach to health care delivery for patients with chronic conditions. Popul. Health Manag. 2017, 20, 23–30. [Google Scholar] [CrossRef]
- Deutsch, A.; Heinemann, A.W.; Cook, K.F.; Foster, L.; Miskovic, A.; Goldsmith, A.; Cella, D. Inpatient rehabilitation quality of care from the patient’s perspective: Effect of data collection timing and patient characteristics. Arch. Phys. Med. Rehabil. 2019, 100, 1032–1041. [Google Scholar] [CrossRef] [PubMed]
- Carlisle, K.; Farmer, J.; Taylor, J.; Larkins, S.; Evans, R. Evaluating community participation: A comparison of participatory approaches in the planning and implementation of new primary health-care services in northern Australia. Int. J. Health Plan. Manag. 2018, 33, 704–722. [Google Scholar] [CrossRef] [PubMed]
- Tapp, H.; White, L.; Steuerwald, M.; Dulin, M. Use of community-based participatory research in primary care to improve healthcare outcomes and disparities in care. J. Comp Eff. Res. 2013, 2, 405–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muhajarine, N.; Labonte, R.; Winquist, B.D. The Canadian Index of Wellbeing: Key findings from the healthy populations domain. Can. J. Public Health 2012, 103, e342–e347. [Google Scholar] [CrossRef] [PubMed]
- Wetmore, S.; Boisvert, L.; Graham, E.; Hall, S.; Hartley, T.; Wright, L.; Hammond, J.A.; Ings, H.; Lent, B.; Pawelec-Brzychczy, A.; et al. Patient satisfaction with access and continuity of care in a multidisciplinary academic family medicine clinic. Can. Fam. Physician Med. Fam. Can. 2014, 60, e230–e236. [Google Scholar]
- Carroll, J.C.; Talbot, Y.; Permaul, J.; Tobin, A.; Moineddin, R.; Blaine, S.; Bloom, J.; Butt, D.; Kay, K.; Telner, D. Academic family health teams: Part 1: Patient perceptions of core primary care domains. Can. Fam. Physician Med. Fam. Can. 2016, 62, e23–e30. [Google Scholar]
- Eide, T.B.; Straand, J.; Melbye, H.; Rortveit, G.; Hetlevik, I.; Rosvold, E.O. Patient experiences and the association with organizational factors in general practice: Results from the Norwegian part of the international, multi-centre, cross-sectional QUALICOPC study. BMC Health Serv. Res. 2016, 16, 428. [Google Scholar] [CrossRef]
- Bonciani, M.; Schafer, W.; Barsanti, S.; Heinemann, S.; Groenewegen, P.P. The benefits of co-location in primary care practices: The perspectives of general practitioners and patients in 34 countries. BMC Health Serv. Res. 2018, 18, 132. [Google Scholar] [CrossRef] [PubMed]
- Tangermann, U.; Kleij, K.S.; Krauth, C.; Amelung, V.E. [Primary Healthcare Provision and Introduction of New Models of Care in Hard to Serve Regions: A Population Survey]. Gesundheitswesen 2019, 81, 498–504. [Google Scholar] [CrossRef]
- Stock, S.; Danner, M. [Does the elicitation of stakeholder attitudes and preferences add valuable information to small-area analyses? A health policy perspective]. Bundesgesundheitsblatt Gesundh. Gesundh. 2014, 57, 188–196. [Google Scholar] [CrossRef]
- Scheidt, L.R.; Joos, S.; Szecsenyi, J.; Steinhauser, J. Oversupplied? Undersupplied? The Perspective of Local Governments of the Federal State of Baden-Wurttemberg: A Contribution to the Discussion of Close-to-Home Health Care. Gesundheitswesen 2015, 77, e179–e183. [Google Scholar] [CrossRef] [PubMed]
- Steinhauser, J.; Scheidt, L.; Szecsenyi, J.; Gotz, K.; Joos, S. Perceptions of the local government about the primary care physicians shortage—A survey among mayors in the Federal State of Baden-Wuerttemberg. Gesundheitswesen 2012, 74, 612–617. [Google Scholar] [CrossRef] [PubMed]
- Kuhn, B.; Kleij, K.S.; Liersch, S.; Steinhauser, J.; Amelung, V. Which strategies might improve local primary healthcare in Germany? An explorative study from a local government point of view. BMC Fam. Pract. 2017, 18, 105. [Google Scholar] [CrossRef] [PubMed]
- Amelung, V.; Wolf, S.; Ozegowski, S.; Eble, S.; Hildebrandt, H.; Knieps, F.; Lagel, R.; Schlenker, R.U.; Sjuts, R. Declared dead? Recommendations regarding integrated care from the perspective of German statutory health insurance. Bundesgesundheitsblatt Gesundh. Gesundh. 2015, 58, 352–359. [Google Scholar] [CrossRef] [PubMed]
- Krinke, K.S.; Tangermann, U.; Amelung, V.E.; Krauth, C. Public preferences for primary care provision in Germany—A discrete choice experiment. BMC Fam. Pract. 2019, 20, 80. [Google Scholar] [CrossRef]
- Kuluski, K.; Nelson, M.L.A.; Tracy, C.S.; Alloway, C.A.; Shorrock, C.; Shearkhani, S.; Upshur, R.E.G. Experience of Care as a Critical Component of Health System Performance Measurement: Recommendations for Moving Forward. Healthc. Pap. 2017, 17, 8–20. [Google Scholar] [CrossRef]
- Collins, D. Pretesting survey instruments: An overview of cognitive methods. Qual. Life Res. 2003, 12, 229–238. [Google Scholar] [CrossRef]
- Statistical Office of Baden-Württemberg. Available online: http://www.statistik-bw.de/SRDB/ (accessed on 4 August 2018).
- Kassenärztliche Vereinigung Baden-Württemberg [Association of Statutory Health Insurance Physicians]. Stand der Bedarfsplanung [Regional Planning]. Available online: https://www.kvbawue.de/praxis/vertraege-recht/bekanntmachungen/bedarfsplanung/ (accessed on 16 July 2019).
- Ojeda, V.D.; Bergstresser, S.M. Gender, Race-Ethnicity, and Psychosocial Barriers to Mental Health Care: An Examination of Perceptions and Attitudes among Adults Reporting Unmet Need. J. Health Soc. Behav. 2008, 49, 317–334. [Google Scholar] [CrossRef]
- Epping, J.; Muschik, D.; Geyer, S. Social inequalities in the utilization of outpatient psychotherapy: Analyses of registry data from German statutory health insurance. Int. J. Equity Health 2017, 16, 147. [Google Scholar] [CrossRef]
- Carlson, M.J.; Shaul, J.A.; Eisen, S.V.; Cleary, P.D. The influence of patient characteristics on ratings of managed behavioral health care. J. Behav. Health Serv. Res. 2002, 29, 481–489. [Google Scholar] [CrossRef]
- Cutler, D.; Skinner, J.; Stern, A.D.; Wennberg, D. Physician Beliefs and Patient Preferences: A New Look at Regional Variation in Health Care Spending. Natl. Bur. Econ. Res. Work. Pap. Ser. 2013. [Google Scholar] [CrossRef]
- Kassenzahnärztliche Vereinigung Baden-Württemberg [Association of Statutory Health Insurance Dentists of Baden-Württemberg] Lückenlos gut Versorgen. [Care Report of the Association of Statutory Health Insurance Dentists of Baden-Württemberg] Stuttgart. 2018. Available online: http://www.kzvbw.de/site/binaries/content/assets/offener-bereich/presse/downloads/vb-2018-web.pdf (accessed on 26 September 2019).
- Cranz, H. Gesundheitsmonitor; BAH, Bundesverbandes der Arzneimittel-Hersteller [German Medicines Manufacturer’s Association]: Bonn, Germany, 2019. [Google Scholar]
- Lampert, T.; Kroll, L.E.; Kuntz, B.; Hoebel, J. Gesundheitliche Ungleichheit in Deutschland und im internationalen Vergleich: Zeitliche Entwicklungen und Trends. [Health inequalities in Germany and in an international comparison: Temporal developments and trends]. J. Health Monit. 2018, 3. [Google Scholar] [CrossRef]
- Nutzel, A.; Dahlhaus, A.; Fuchs, A.; Gensichen, J.; Konig, H.H.; Riedel-Heller, S.; Maier, W.; Schafer, I.; Schon, G.; Weyerer, S.; et al. Self-rated health in multimorbid older general practice patients: A cross-sectional study in Germany. BMC Fam. Pract. 2014, 15. [Google Scholar] [CrossRef] [PubMed]
- Kammer, B.P. Ein Jahr nach der Reform der Psychotherapie-Richtlinie [One Year after the Reform of the Psychotherapy Directive]; Federal Psychotherapist Chamber: Berlin, Germany, 2018; p. 40. [Google Scholar]
- Eardley, S.; Bishop, F.L.; Prescott, P.; Cardini, F.; Brinkhaus, B.; Santos-Rey, K.; Vas, J.; von Ammon, K.; Hegyi, G.; Dragan, S.; et al. A Systematic Literature Review of Complementary and Alternative Medicine Prevalence in EU. Complementary Med. Res. 2012, 19, 18–28. [Google Scholar] [CrossRef] [PubMed]
- Reis, K.; Köster, G.; Steger, A. Vertragsärztliche Bedarfsplanung: Flexiblere Instrumente für Sachgerechte Lösungen vor Ort [Requirements Planning of Contractual Medical Care: More Flexibel Instruments for Appropriate Solutions on site]; Press Release; Gemeinsamer Bundesausschuss: Berlin, Germany, 2019; Available online: https://www.g-ba.de/downloads/34-215-797/14_2019-05-16_Bedarfsplanung_Weiterentwicklung.pdf (accessed on 16 July 2019).
- Lampert, P. Soziale Unterschiede in Deutschland: Mortalität und Lebenserwartung [Social differences in Germany: Mortality and Life Expectancy]; Robert Koch Institut: Berlin, Germany, 2019; Available online: http://www.rki.de/DE/Content/Gesundheitsmonitoring/Gesundheitsberichterstattung/GBEDownloadsK/2014_2_soziale_unterschiede.pdf%3F__blob%3DpublicationFile (accessed on 16 July 2019).
- Chokshi, D.A. Income, Poverty, and Health Inequality: The JAMA Forum. JAMA 2018, 319, 1312–1313. [Google Scholar] [CrossRef] [PubMed]
- Lampert, P.; Hoebel, J.; Kuntz, B.; Müters, S.; Kroll, E. Gesundheitliche Ungleichheit in verschiedenen Lebensphasen [Health inequalities at different stages of life]. In Gesundheitsberichterstattung des Bundes; Robert Koch Institut: Berlin, Germany, 2017. [Google Scholar] [CrossRef]
- OECD; European Observatory on Health Systems and Policies. Germany: Country Health Profile 2017; OECD iLibrary: Paris, France, 2017. [Google Scholar] [CrossRef]
- Manstead, A.S.R. The psychology of social class: How socioeconomic status impacts thought, feelings, and behaviour. Br J Soc Psychiol 2018, 57, 267–291. [Google Scholar] [CrossRef] [Green Version]
- Sachverständigenrat zur Begutachtung der Entwicklung im Gesundheitswesen [Subject Council on the Evaluation of Developments in the Health Sector]. Bedarfsgerechte Steuerung der Gesundheitsversorgung [Appropriate Control in Management of Health Care]; Sachverständigenrats zur Begutachtung der Entwicklung im Gesundheitswesen [Subject Council on the Evaluation of Developments in the Health Sector]: Berlin/Bonn, Germany, 2018; p. 210. Available online: https://www.svr-gesundheit.de/fileadmin/user_upload/Gutachten/2018/SVR-Gutachten_2018_WEBSEITE.pdf (accessed on 31 August 2019).
- Schoen, C.; Osborn, R.; Squires, D.; Doty, M.; Pierson, R.; Applebaum, S. New 2011 Survey of Patients with Complex Care Needs in Eleven Countries Finds That Care Is Often Poorly Coordinated. Health Aff. 2011, 30, 2437–2448. [Google Scholar] [CrossRef] [PubMed]
- Agency for Healthcare Research and Quality. The CAHPS Ambulatory Care Improvement Guide. Pract. Strateg. Improv. Patient Exp. 2017, 76–90. Available online: https://www.ahrq.gov/sites/default/files/wysiwyg/cahps/quality-improvement/improvement-guide/cahps-ambulatory-care-guide-full.pdf (accessed on 31 August 2019).
- Kimberlyn McGrail, S.B.; Jennifer, D. Let’s All Go to the PROM: The Case for Routine Patient-Reported Outcome Measurement in Canadian Healthcare. HealthcarePapers 2012, 11, 8–18. [Google Scholar] [CrossRef]
- Augurzky, B.; Hentschker, C.; Pilny, A.; Wübker, A. Krankenhausreport 2017 [Hospital Report 2017]; BARMER Statutory Health Insurance: Siegburg, Germany, 2017; Available online: https://www.barmer.de/blob/124290/fd51cb989f2db52180beea2846cc0076/data/dl-report.pdf (accessed on 31 August 2019).
- Batalden, M.; Batalden, P.; Margolis, P.; Seid, M.; Armstrong, G.; Opipari-Arrigan, L.; Hartung, H. Coproduction of healthcare service. BMJ Qual. Saf. 2015, 25, 509–517. [Google Scholar] [CrossRef] [Green Version]
- Rapport, F.; Hibbert, P.; Baysari, M.; Long, J.C.; Seah, R.; Zheng, W.Y.; Jones, C.; Preece, K.; Braithwaite, J. What do patients really want? An in-depth examination of patient experience in four Australian hospitals. BMC Health Serv. Res. 2019, 19, 38. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Region A (Community A, 3653 inhabitants) | Region B1 (Communities < 7000 inhabitants) | Region B2 (Communities ≥ 7000 inhabitants) | |
|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | |
| Area of communities (km2) 1 | 61.7 ± 0 | 38.6 ± 22.4 | 43.1 ± 22.6 |
| Population count 1 | 3653 ± 0 | 4330 ± 1741 | 14022 ± 6275 |
| Population density 1 | 59.2 ± 0 | 145.3 ± 93.9 | 373.5 ± 165.6 |
| GP density (per 1000 inhabitants) 2 | 0.82 ± 0 | 0.57 ± 0.41 | 0.63 ± 0.23 |
| GP supply rate 2,3 (%) | 114.8 | 89.2 | 100.3 |
| Specialist density (per 1000 inhabitants) 2 | 0.27 ± 0 | 0.25 ± 0.43 | 1.12 ± 0.99 |
| Number of undersupplied specialist groups 4,* | 1 out of 13 | 6 out of 13 | |
| Psychotherapist density (per 1000 inhabitants) 2 | 0.22 | 0.19 | |
| Psychotherapist supply rate (%) 2,3 | 129.24 | 115.8 | |
| Dentist density (per 1000 inhabitants) 5 | 0.55 | 0.904 | |
| Community A (located in Region A, 3653 inhabitants) | Region B1 (Communities with < 7000 inhabitants) | Region B2 (Communities with ≥ 7000 inhabitants) | p | ||||
|---|---|---|---|---|---|---|---|
| Sociodemographic characteristics | |||||||
| Sex | |||||||
| Female | 921 | 418 (45.4) | 95 | 39 (41.1) | 114 | 47 (41.2) | 0.538 b |
| Age | 921 | 95 | 114 | 0.035 a,* | |||
| 18–39 years | 206 (22.4) | 28 (29.5) | 34 (29.8) | ||||
| 40–65 years | 462 (50.2) | 50 (53.6) | 53 (46.5) | ||||
| ≥66 years | 253 (27.5) | 17 (17.9) | 27 (23.7) | ||||
| Monthly income | 812 | 86 | 94 | 0.101 a | |||
| <1500€ | 199 (25) | 12 (14.0) | 19 (20.2) | ||||
| 1500–<3000€ | 337 (41.5) | 39 (45.3) | 39 (41.5) | ||||
| ≥3000€ | 276 (34.0) | 35 (40.7) | 36 (38.3) | ||||
| School education/training 2 | 851 | 92 | 114 | 0.525 a | |||
| Secondary school (6–9 years) | 304 (35.7) | 37 (40.2) | 38 (35.2) | ||||
| Vocational training | 272 (32) | 30 (32.6) | 33 (30.6) | ||||
| Master craftsman or university degree | 275 (32.3) | 25 (27.2) | 37 (34.3) | ||||
| Currently employed | 879 | 562 (63.9) | 93 | 65 (69.9) | 108 | 64 (59.3) | 0.293 b |
| Health-related characteristics | |||||||
| Time resources to take care of one’s health 1, mean ± SD) | 895 | 2.65 ± 0.87 | 94 | 2.56 ± 0.68 | 114 | 2.46 ± 0.86 | 0.230 a |
| Financial resources to take care of one’s health 1 (mean ± SD) | 890 | 1.72 ± 0.72 | 92 | 1.55 ± 0.70 | 112 | 1.55 ± 0.61 | 0.013 a,* |
| Support by friends, neighbors and family, if needed, is etc. 1 (mean ± SD) | 851 | 1.479 ± 0.68 | 91 | 1.45 ± 0.62 | 108 | 1.45 ± 0.72 | 0.799 a |
| Self-assessed physical health 1 | 902 | 1.478 ± 0.61 | 94 | 1.44 ± 0.63 | 112 | 1.40 ± 0.61 | 0.261 a |
| Self-assessed mental health 1 (mean ± SD) | 887 | 1.345 ± 0.59 | 94 | 1.26 ± 0.55 | 112 | 1.3 ± 0.57 | 0.248 a |
| Presence of any chronic disease 2 | 892 | 368 (41.3) | 94 | 33 (35.1) | 112 | 40 (35.7) | 0.306 b |
| Characteristics 1 | Adjusted OR (95% CI) | ||
|---|---|---|---|
| Very Good/Good vs. Very Poor/Poor # | Satisfactory vs. Very Poor/Poor # | Very Good/Good vs. Satisfactory # | |
| Attribution to region/community | |||
| Region B2 (≥7000 inh) | 0.01 (0–0.03) ** | 0.21 (0.09–0.49) ** | 0.06 (0.03–0.12) ** |
| Region B1 (<7000 inh) | 0.01 (0–0.03) ** | 0.18 (0.08–0.42) ** | 0.07 (0.03–0.14) ** |
| Community A (3653 inh) | Reference | ||
| Age | |||
| 18–39 years | 0.51 (0.19–1.34) | 1.52 (0.58–3.95) | 0.38 (0.18–0.78) ** |
| 40–65 years | 0.73 (0.3–1.77) | 1.52 (0.58–3.95) | 0.48 (0.25–0.92) * |
| ≥66 years | Reference | ||
| Monthly income (€) | |||
| 0–<1500 | 3.45 (1.25–9.49) * | 3.68 (1.3–10.39) * | 0.93 (0.49–1.78) |
| 1500–<3000 | 1.79 (0.87–3.65) | 1.87 (0.88–3.96) | 0.95 (0.56–1.61) |
| ≥3000 | Reference | ||
| Evaluation of own financial resources for preventive healthcare | |||
| Very good/good | 2.3 (0.77–6.89) | 0.77 (0.25–2.36) | 2.96 (1.47–5.94) |
| Satisfactory | 1.09 (0.4–3.02) | 0.81 (0.29–2.24) | 1.35 (0.74–2.48) |
| Very poor/poor | Reference | ||
| Evaluation of support from friends and family | |||
| Very good/good | 2.36 (0.81–6.85) | 1.58 (0.53–4.68) | 1.49 (0.71–3.09) |
| Satisfactory | 0.82 (0.28–2.38) | 1.04 (0.35–3.06) | 0.79 (0.37–1.65) |
| Very poor/poor | Reference | ||
| Characteristics 1 | Adjusted OR (95% CI) | ||
|---|---|---|---|
| Very Good/Good vs. Very Poor/Poor # | Satisfactory vs. Very Poor/Poor # | Very Good/Good vs. Satisfactory # | |
| Attribution to Region/community | |||
| Region B2 (≥7000 inh) | 1.98 (0.68–5.74) | 1.07 (0.46–2.47) | 1.85 (0.55–6.18) |
| Region B1 (<7000 inh) | 2.54 (1.06–6.09) * | 3.28 (1.87–5.75) ** | 0.77 (0.32–1.85) |
| Community A (3653 inh) | Reference | ||
| Age | |||
| 18–39 years | 0.64 (0.29–1.37) | 0.98 (0.56–1.71) | 0.65 (0.28–1.5) |
| 40–65 years | 0.52 (0.27–1.02) | 0.93 (0.58–1.51) | 0.56 (0.27–1.17) |
| ≥66 years | Reference | ||
| Monthly Income (€) | |||
| 0–<1500 | 8.22 (2.65–25.48) ** | 1.34 (0.77–2.32) | 6.11 (1.87–19.88) ** |
| 1500–<3000 | 5.41 (1.83–15.94) ** | 1.08 (0.68–1.69) | 5.00 (1.63–15.36) ** |
| ≥3000 | Reference | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sturm, H.; Colombo, M.; Hebeiss, T.; Joos, S.; Koch, R. Patient Input in Regional Healthcare Planning—A Meaningful Contribution. Int. J. Environ. Res. Public Health 2019, 16, 3754. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16193754
Sturm H, Colombo M, Hebeiss T, Joos S, Koch R. Patient Input in Regional Healthcare Planning—A Meaningful Contribution. International Journal of Environmental Research and Public Health. 2019; 16(19):3754. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16193754
Chicago/Turabian StyleSturm, Heidrun, Miriam Colombo, Teresa Hebeiss, Stefanie Joos, and Roland Koch. 2019. "Patient Input in Regional Healthcare Planning—A Meaningful Contribution" International Journal of Environmental Research and Public Health 16, no. 19: 3754. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16193754