Are Parent-Held Child Health Records a Valuable Health Intervention? A Systematic Review and Meta-Analysis




Abstract
:1. Introduction
2. Method
2.1. Review Protocol
2.2. Search Strategy
2.3. Eligibility Criteria and Selection
2.4. Data Extraction and Quality Assessment
2.5. Data Analysis
3. Results
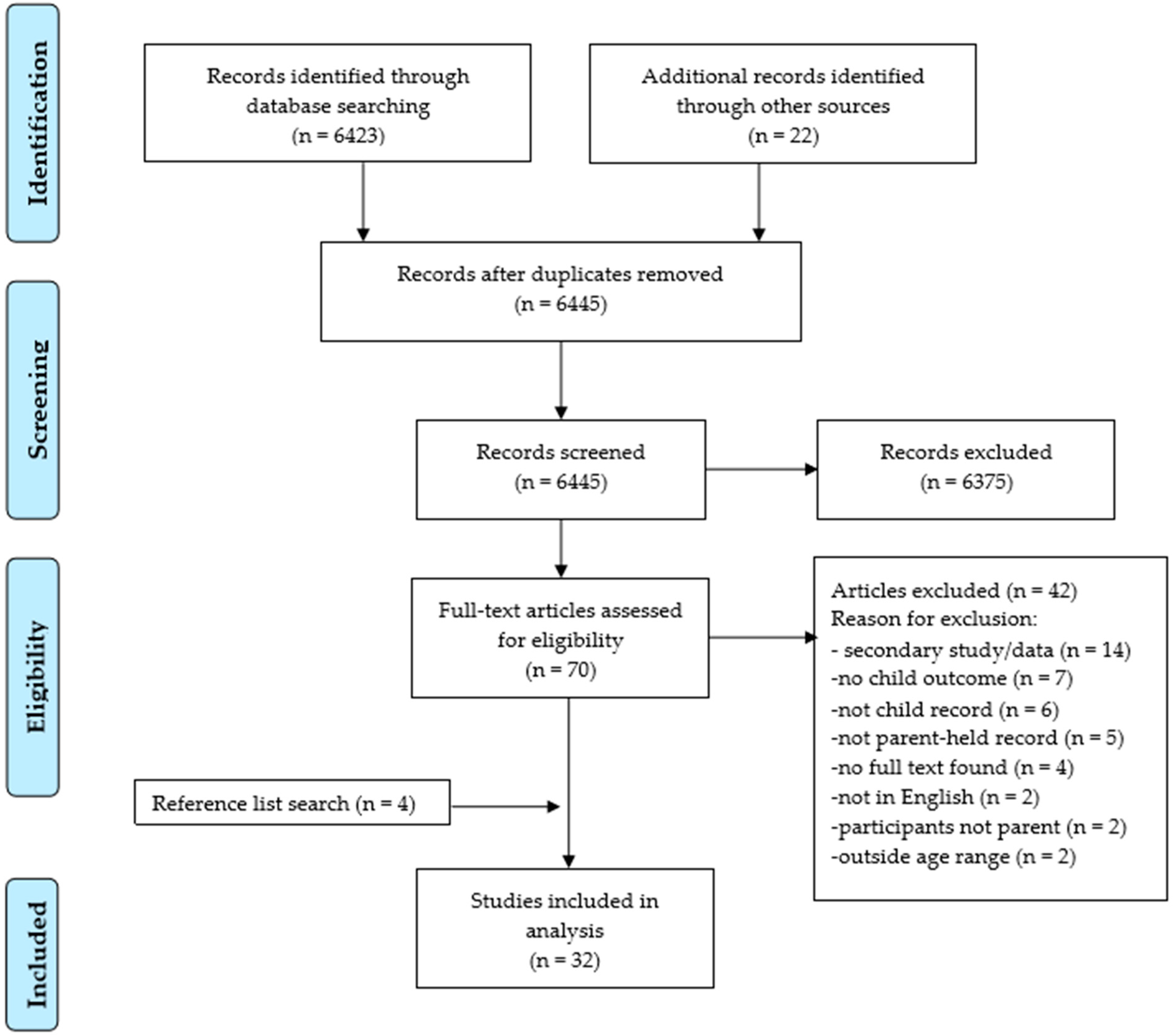
3.1. Search Result
3.2. Characteristics of Included Studies
3.3. Participants/Population
3.4. Intervention (PHCHR) Description
3.5. Findings
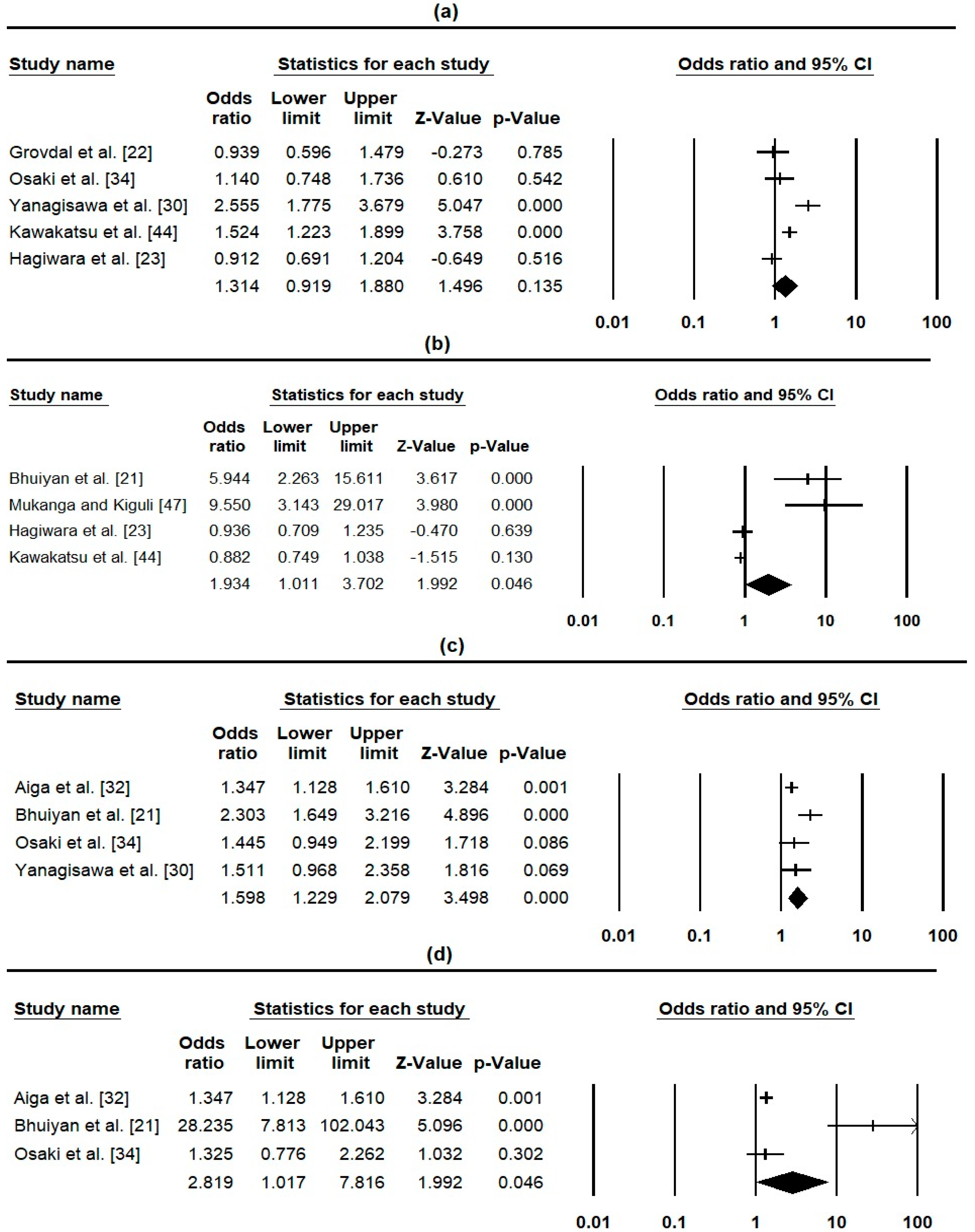
3.5.1. PHCHR Impact on Health-Related Outcomes
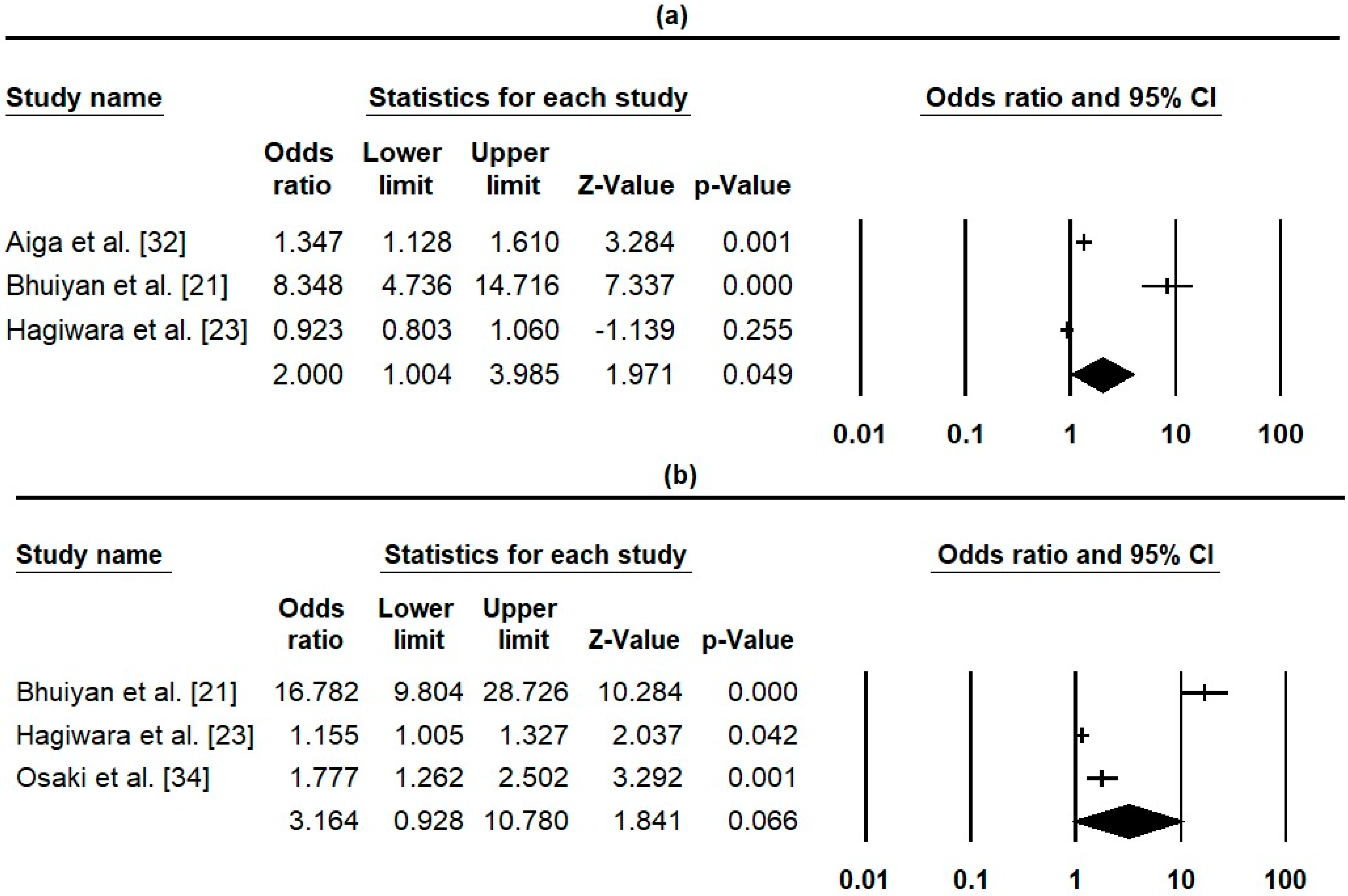
3.5.2. PHCHR impact on Parents/Mother’s Health Knowledge
3.5.3. Parent Views and Use of PHCHR
Parent View of Professionals toward Use of the PHCHR
3.5.4. Record Input in PHCHR Measured by Direct Observation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgment
Conflicts of Interest
References
- Volkmer, R.E.; Gouldstone, M.A.; Ninnes, C.P. Parental Perception of the Use and Usefulness of a Parent-held Child Health Record. J. Paediatr. Child Health 1993, 29, 150–153. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, J.; Sakagami, Y.; Perez, R.C. The Mother and Child Health Handbook in Japan as a Health Promotion Tool: An Overview of Its History, Contents, Use, Benefits, and Global Influence. Glob. Pediatr. Health 2016, 3. [Google Scholar] [CrossRef] [PubMed]
- Mudany, M.A.; Sirengo, M.; Rutherford, G.W.; Mwangi, M.; Nganga, L.W.; Gichangi, A. Enhancing Maternal and Child Health Using a Combined Mother & Child Health Booklet in Kenya. J. Trop. Pediatr. 2015, 61, 442–447. [Google Scholar] [CrossRef] [PubMed]
- Kusumayati, A.; Nakamura, Y. Increased Utilization of Maternal Health Services by Mothers Using the Maternal and Child Health Handbook in Indonesia. J. Int. Health 2007, 22, 143–151. [Google Scholar] [CrossRef]
- Mori, R.; Yonemoto, N.; Noma, H.; Ochirbat, T.; Barber, E.; Soyolgerel, G.; Nakamura, Y.; Lkhagvasuren, O. The Maternal and Child Health (MCH) Handbook in Mongolia:A Cluster-Randomized, Controlled Trial. PLoS ONE 2015, 10, e0119772. [Google Scholar] [CrossRef] [PubMed]
- McMaster, P.; McMaster, H.J.; Southall, D.P. Personal Child Health Record and Advice Booklet Programme in Tuzla, Bosnia Herzegovina. J. R. Soc. Med. 1996, 89, 202–204. [Google Scholar] [CrossRef] [PubMed]
- Shah, P.M.; Selwyn, B.J.; Shah, K.; Kumar, V.; Abraham, S.; Akhter, M.S.; Alahakone, K.; Bacalzo, F.T.; Fall, M.; Hammamy, M.T.; et al. Evaluation of the Home-Based Maternal Record: A WHO Collaborative Study. Bull. World Health Organ. 1993, 71, 535–548. [Google Scholar]
- McElligott, J.T.; Darden, P.M. Are Patient-Held Vaccination Records Associated With Improved Vaccination Coverage Rates? Pediatrics 2010, 125, e467–e472. [Google Scholar] [CrossRef]
- Fujimoto, S.; Nakamura, Y.; Ikeda, M.; Takeda, Y.; Higurashi, M. Utilization of Maternal and Child Health Handbook in Japan. Nihon Koshu Eisei Zasshi 2001, 48, 486–494. [Google Scholar]
- Garg, P.; Ha, M.T.; Eastwood, J.; Harvey, S.; Woolfenden, S.; Murphy, E.; Dissanayake, C.; Jalaludin, B.; Williams, K.; McKenzie, A.; et al. Explaining Culturally and Linguistically Diverse (CALD) Parents’ Access of Healthcare Services for Developmental Surveillance and Anticipatory Guidance: Qualitative Findings from the ‘Watch Me Grow’ Study. BMC Health Serv. Res. 2017, 17, 228. [Google Scholar] [CrossRef]
- Hooker, L.; Williams, J. Parent-Held Shared Care Records: Bridging the Communication Gaps. Br. J. Nurs. 1996, 5, 738–741. [Google Scholar] [CrossRef] [PubMed]
- Riverin, B.; Li, P.; Rourke, L.; Leduc, D.; Rourke, J. Rourke Baby Record 2014: Evidence-Based Tool for the Health of Infants and Children from Birth to Age 5. Can. Fam. Physician Méd. Fam. Can. 2015, 61, 949–955. [Google Scholar]
- Farida, N. Determinants of the mch handbook utilization by pregnant women at wanakerta health center of karawang regency in 2015 Dengan Ibu Hamil Di Puskes. Southeast Asian J. Midwifery 2016, 2, 33–41. [Google Scholar]
- Cohen, S.J.; Gitterman, B.A.; Baron, A.L.; Reiner, K.L.; Lynch, K.R. Improving Adherence with Preventive Pediatric Care Guidelines through the Use of a Parent-Held Child Health Record|Cochrane Library. Available online: https://www.cochranelibrary.com/central/doi/10.1002/central/CN-00598143/full (accessed on 25 November 2018).
- Calvin, S.D.R. Maternal and Child Health Handbook among the Indigenous Peoples in the Philippines: The Case of Tagbanua Mothers and Children of Coron Island, Palawan; Osaka University: Osaka, Japan, 2010. [Google Scholar]
- Turner, K.E.; Fuller, S. Patient-Held Maternal and/or Child Health Records: Meeting the Information Needs of Patients and Healthcare Providers? Online J. Public Health Inform. 2011, 3, 1–48. [Google Scholar] [CrossRef]
- Baequni; Nakamura, Y. Is Maternal and Child Health Handbook Effective? Meta-Analysis of the Effects of MCH Handbook. J. Int. Health 2012, 27, 121–127. [Google Scholar]
- PRISMA. PRISMA 2009 Checklist. 2009. Available online: https://journals.plos.org/plosmedicine/article/file?type=supplementary&id=info:doi/10.1371/journal.pmed.1002203.s001 (accessed on 18 July 2018).
- Centre for Reviews & Dissemination CRD. CRD Guidance for Undertaking Reviews in Health Care, 3rd ed.; York Publishing Services Ltd.: Layerthorpe, UK, 2009. [Google Scholar]
- World Bank. Countries and Economies 2008. Available online: https://data.worldbank.org/country (accessed on 27 November 2018).
- Bhuiyan, S.U.; Nakamura, Y.; Qureshi, N.A. Study on the Development and Assessment of Maternal and Child Health (MCH) Handbook in Bangladesh. J. Public Health Dev. 2006, 4, 45–59. [Google Scholar]
- Grøvdal, L.B.; Grimsmo, A.; Nilsen, T.I.L. Parent-Held Child Health Records Do Not Improve Care: A Randomized Controlled Trial in Norway. Scand. J. Prim. Health Care 2006, 24, 186–190. [Google Scholar] [CrossRef]
- Hagiwara, A.; Ueyama, M.; Ramlawi, A.; Sawada, Y. Is the Maternal and Child Health (MCH) Handbook Effective in Improving Health-Related Behavior Evidence from Palestine. J. Public Health Policy 2013, 34, 31–45. [Google Scholar] [CrossRef]
- Miller, S.A. A Trial of Parent Held Child Health Records in the Armed Forces. BMJ Br. Med. J. 1990, 300, 1046. [Google Scholar] [CrossRef]
- O’Flaherty, S.; Jandera, E.; Llewellyn, J.; Wall, M. Personal Health Records: An Evaluation. Arch. Dis. Child. 1987, 62, 1152–1155. [Google Scholar] [CrossRef] [PubMed]
- Polnay, L.; Roberts, H. Evaluation of an Easy to Read Parent-Held Information and Record Booklet of Child Health. Child. Soc. 1989, 3, 255–260. [Google Scholar] [CrossRef]
- Price, S.; Fulop, N.; Mills, A. Sharing Information: An Evaluation of a Parent-Held Child Health Record Scheme. Crit. Public Health 1991, 2, 32–37. [Google Scholar] [CrossRef]
- Saffin, K.; Macfarlane, A. How Well Are Parent Held Records Kept and Completed? Br. J. Gen. Pract. 1991, 41, 249–251. [Google Scholar] [PubMed]
- Stacy, R.D.; Sharma, M.; William, A.T. Evaluation of the Use of a Parent-Held Child Health Record by Pregnant Women and Mothers of Young Children. Calif. J. Health Promot. 2008, 6, 138–142. [Google Scholar]
- Yanagisawa, S.; Soyano, A.; Igarashi, H.; Ura, M.; Nakamura, Y. Effect of a Maternal and Child Health Handbook on Maternal Knowledge and Behaviour: A Community-Based Controlled Trial in Rural Cambodia. Health Policy Plan. 2015, 30, 1184–1192. [Google Scholar] [CrossRef] [PubMed]
- Clendon, J.; Dignam, D. Child Health and Development Record Book: Tool for Relationship Building between Nurse and Mother. J. Adv. Nurs. 2010, 66, 968–977. [Google Scholar] [CrossRef] [PubMed]
- Aiga, H.; Nguyen, V.D.; Nguyen, C.D.; Nguyen, T.T.T.; Nguyen, L.T.P. Knowledge, Attitude and Practices: Assessing Maternal and Child Health Care Handbook Intervention in Vietnam. BMC Public Health 2016, 16, 129. [Google Scholar] [CrossRef]
- Hamilton, L.; Wyver, S. Parental Use and Views of the Child Personal Health Record. Aust. Educ. Dev. Psychol. 2012, 29, 66–77. [Google Scholar] [CrossRef]
- Osaki, K.; Hattori, T.; Toda, A.; Mulati, E.; Hermawan, L.; Pritasari, K.; Bardosono, S.; Kosen, S. Maternal and Child Health Handbook Use for Maternal and Child Care: A Cluster Randomized Controlled Study in Rural Java, Indonesia. J. Public Health 2018, 1–13. [Google Scholar] [CrossRef]
- Abud, S.M.; Gaíva, M.A.M. Records of Growth and Development Data in the Child Health Handbook. Rev. Gaúcha Enferm. 2015, 36, 97–105. [Google Scholar] [CrossRef]
- Campbell, H.; Halleran, J. An Evaluation of the Personal Child Health Record in Fife. Health Bull. 1993, 51, 399–406. [Google Scholar]
- Dagvadorj, A.; Nakayama, T.; Inoue, E.; Sumya, N.; Mori, R. Cluster Randomised Controlled Trial Showed That Maternal and Child Health Handbook Was Effective for Child Cognitive Development in Mongolia. Acta Paediatr. Int. J. Paediatr. 2017, 106, 1360–1361. [Google Scholar] [CrossRef] [PubMed]
- Emond, A.; Howat, P.; Evans, J.A. Reliability of Parent-Held Child Health Records. Health Visitor 1995, 68, 322–323. [Google Scholar]
- Hampshire, A.J.; Blair, M.E.; Crown, N.S.; Avery, A.J.; Williams, E.I. Variation in How Mothers, Health Visitors and General Practitioners Use the Personal Child Health Record. Child. Care Health Dev. 2004, 30, 307–316. [Google Scholar] [CrossRef]
- Harrison, D.; Heese, H.D.V.; Harker, H.; Mann, M.D. An Assessment of the “Road-to-Health” Card Eased on Perceptions of Clinic Staff and Mothers. S. Afr. Med. J. 1998, 88, 1424–1428. [Google Scholar] [PubMed]
- Hikita, N.; Haruna, M.; Matsuzaki, M.; Shiraishi, M.; Takehara, K.; Dagvadorj, A.; Sumya, N.; Bavuusuren, B.; Baljinnyam, P.; Ota, E.; et al. Utilisation of Maternal and Child Health Handbook in Mongolia: A Cross-Sectional Study. Health Educ. J. 2018, 77, 458–469. [Google Scholar] [CrossRef]
- Jeffs, D.; Nossar, V.; Bailey, F.; Smith, W.; Chey, T. Retention and Use of Personal Health Records: A Population-Based Study. J. Paediatr. Child Health 1994, 30, 248–252. [Google Scholar] [CrossRef] [PubMed]
- Jessop, L.; Lotya, J.; Murrin, C.; Fallon, U.B.; Kelleher, C.C. Relationship between Parent Held Child Records for Immunisations, Parental Recall and Health Service. Ir. Med. J. 2011, 104, 1–4. [Google Scholar]
- Kawakatsu, Y.; Sugishita, T.; Oruenjo, K.; Wakhule, S.; Kibosia, K.; Were, E.; Honda, S. Effectiveness of and Factors Related to Possession of a Mother and Child Health Handbook: An Analysis Using Propensity Score Matching. Health Educ. Res. 2015, 30, 935–946. [Google Scholar] [CrossRef] [PubMed]
- Koh, H.C.; Ang, S.K.T.; Kwok, J.; Tang, H.N.; Wong, C.M.; Daniel, L.M.; Goh, W. The Utility of Developmental Checklists in Parent-Held Health Records in Singapore. J. Dev. Behav. Pediatr. 2016, 37, 647–656. [Google Scholar] [CrossRef]
- Lakhani, A.D.; Avery, A.; Gordon, A.; Tait, N. Evaluation of a Home Based Health Record Booklet. Arch. Dis. Child. 1984, 59, 1076–1081. [Google Scholar] [CrossRef] [PubMed]
- Mukanga, D.O.; Kiguli, S. Factors Affecting the Retention and Use of Child Health Cards in a Slum Community in Kampala, Uganda, 2005. Matern. Child Health J. 2006, 10, 545–552. [Google Scholar] [CrossRef] [PubMed]
- Palombo, C.N.T.; Duarte, L.S.; Fujimori, E.; Toriyama, Á.T.M. Use and Records of Child Health Handbook Focused on Growth and Development. Rev. Esc. Enferm. 2014, 48, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Tarwa, C.; De Villiers, F. The Use of the Road to Health Card in Monitoring Child Health. S. Afr. Fam. Pract. 2007, 49. [Google Scholar] [CrossRef]
- Troude, P.; L’Hélias, L.F.; Raison-Boulley, A.M.; Castel, C.; Bouyer, J.; De La Rochebrochard, E. Apgar Scores Reported in Personal Child Health Records: Validity for Epidemiological Studies? J. Paediatr. Child Health 2008, 44, 665–669. [Google Scholar] [CrossRef] [PubMed]
- Walton, S.; Bedford, H. Parents’ Use and Views of the National Standard Personal Child Health Record: A Survey in Two Primary Care Trusts. Child. Care Health Dev. 2007, 33, 744–748. [Google Scholar] [CrossRef]
- Wright, C.M.; Reynolds, L. How Widely Are Personal Child Health Records Used and Are They Effective Health Education Tools? A Comparison of Two Records. Child. Care Health Dev. 2006, 32, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Phillips, D.E.; Dieleman, J.L.; Lim, S.S.; Shearer, J. Determinants of effective vaccine coverage in low and middle-income countries: A systematic review and interpretive synthesis. BMC Health Serv. Res. 2017, 17, 681. [Google Scholar] [CrossRef] [PubMed]
- Kochhar, S.; Rath, B.; Seeber, L.D.; Rundblad, G.; Khamesipour, A.; Ali, M. Introducing New Vaccines in Developing Countries. Expert Rev. Vaccines 2013, 12, 1465–1478. [Google Scholar] [CrossRef] [PubMed]
- Greenwood, B. The Contribution of Vaccination to Global Health: Past, Present and Future. Philos. Trans. R. Soc. B Biol. Sci. 2014, 369, 20130433. [Google Scholar] [CrossRef]
- Zewdie, A.; Letebo, M.; Mekonnen, T. Reasons for Defaulting from Childhood Immunization Program: A Qualitative Study from Hadiya Zone, Southern Ethiopia. BMC Public Health 2016, 16, 1240. [Google Scholar] [CrossRef] [PubMed]
- Fawzi, W.W.; Chalmers, T.C.; Herrera, M.G.; Mosteller, F. Vitamin A Supplementation and Child Mortality. JAMA 1993, 269, 898. [Google Scholar] [CrossRef]
- Jones, G.; Steketee, R.W.; Black, R.E.; Bhutta, Z.A.; Morris, S.S.; Bellagio Child Survival Study Group. How Many Child Deaths Can We Prevent This Year? Lancet 2003, 362, 65–71. [Google Scholar] [CrossRef]
- Blondel, B.; Dutilhb, P.; Delourb, M.; Uzanc, S. Poor Antenatal Care and Pregnancy Outcome. Eur. J. Obstet. Gynecol. Reprod. Biol. 1993, 50, 191–196. [Google Scholar] [CrossRef]
- Raatikainen, K.; Heiskanen, N.; Heinonen, S. Under-Attending Free Antenatal Care Is Associated with Adverse Pregnancy Outcomes. BMC Public Health 2007, 7, 268. [Google Scholar] [CrossRef]
- Victora, C.G.; Bahl, R.; Barros, A.J.D.; França, G.V.A.; Horton, S.; Krasevec, J.; Murch, S.; Sankar, M.J.; Walker, N.; Rollins, N.C.; et al. Breastfeeding in the 21st Century: Epidemiology, Mechanisms, and Lifelong Effect. Lancet 2016, 387, 475–490. [Google Scholar] [CrossRef]
- Wu, T.; Shi, J.; Bao, S.; Qu, Y.; Mu, D.Z. Effect of Premature Rupture of Membranes on Maternal Infections and Outcome of Preterm Infants. Zhongguo Dang Dai Er Ke Za Zhi 2017, 19, 861–865. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Study | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Abud and Gaiva [35] | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 9/10 |
| Aiga et al. [32] | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 9/10 |
| Bhuiyan et al. [21] | 1 | 0 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 7/10 |
| Campbell and Halleran [36] | 1 | 0 | 1 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 6/10 |
| Clendon and Dignam [31] | 1 | 0 | 0 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 6/10 |
| Dagvadorj et al. [37] | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 8/10 |
| Emond et al. [38] | 1 | 0 | 1 | 1 | 1 | 0 | 0 | 1 | 0 | 1 | 6/10 |
| Grovdal et al. [22] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 10/10 |
| Hagiwara et al. [23] | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8/10 |
| Hamilton and Wyver [33] | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 5/10 |
| Hampshire et al. [39] | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 9/10 |
| Harrison et al. [40] | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 5/10 |
| Hikita et al. [41] | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 9/10 |
| Jeffs et al. [42] | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 8/10 |
| * Jessop et al. [43] | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 8/10 |
| Kawakatsu et al. [44] | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 8/10 |
| Koh et al. [45] | 1 | 0 | 0 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 7/10 |
| Lakhani et al. [46] | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 7/10 |
| Miller [24] | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 0 | 4/10 |
| Mukanga and Kiguli [47] | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 8/10 |
| O’Flaherty et al. [25] | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 7/10 |
| Osaki et al. [34] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 10/10 |
| Palombo et al. [48] | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 7/10 |
| Polnay and Roberts [26] | 1 | 0 | 0 | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 6/10 |
| Price et al. [27] | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 0 | 4/10 |
| Saffin and Macfarlane [28] | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 7/10 |
| Stacy et al. [29] | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 6/10 |
| Tarwa and De Villiers [49] | 1 | 0 | 0 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 6/10 |
| * Troude et al. [50] | 1 | 1 | 0 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 8/10 |
| Walton and Bedford [51] | 1 | 0 | 0 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 6/10 |
| Wright and Reynolds [52] | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 8/10 |
| Yanagisawa et al. [30] | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 8/10 |
| Outcomes | Reference | Intervention: CPHR, MCHH | Impact of Intervention on Outcome | Effect Size/Comments | ||
|---|---|---|---|---|---|---|
| Positive | No Impact | Mixed | ||||
| Utilization of child healthcare/MCH care | [22] | CPHR | √ | Non-routine CHC visits (66% intervention and 62% control p = 0.58), Doctor visits outside CHC (46% intervention and 48% control p = 0.95), Specialist/hospital visits (74% intervention and 73% control p = 0.84) | ||
| [44] | MCHH | √ | ATT on fever 0.095 (t-test = 4.024, p < 0.05) and diarrhoea 0.119 (t-test = 3.665, p < 0.001) (Treatment vs. control) | |||
| [23] | MCHH | √ | More time spent by women with first delivery at MCH consultations (t-test = 2.14, p ≤ 0.05) but no overall effect (t-test = 0.64), knowing next appointment date by primary educated women (t-test = 2.31, p ≤ 0.05) but not overall (t-test = 0.66) | |||
| [34] | MCHH | √ | Delivery with skilled birth attendant OR = 1.14 | |||
| [26] | CPHR | √ | Hearing test visits: 76% experimental, 68% control. No child health clinic attendance: 1% experimental, 4% controls (both reported as not statistically significant) | |||
| [30] | MCHH | √ | Delivery with Skilled Birth Attendant (SBA), R = 12.2 (OR = 2.613, p < 0.01, AOR = 1.092), delivery in health facility, R = 4.4 (OR = 2.499, p < 0.01, AOR = 1.866, p < 0.01) | |||
| Uptake of immunization/vaccination | [21] | MCHH | √ | 8.3% case and 1.5% control (Child), 15.1% case and 6.6% control (mothers) (no p-value) | ||
| [23] | MCHH | √ | No overall effect on following child immunization schedules (t-test = 0.47), but effective among women with first delivery (t-test = 4.22, p ≤ 0.01) | |||
| [44] | MCHH | √ | Child vaccine ATT = 0.030, t-test = 1.516, (Treatment vs. control) | |||
| [46] | CPHR | √ | Diphtheria, Polio, Tetanus (DPT) 1st (90% study vs. 94% control), DTP 2nd dose (76% vs. 85%), DTP 3rd dose (22% vs. 31%), Pertussis 1st dose (64% vs. 58%), Pertussis 2nd dose (58% vs. 59%), Pertussis 3rd dose (19% vs. 19%) | |||
| [47] | CPHR | √ | Children with record compared to no record (OR = 9.55, 95% CI 3.19, 29.45, p < 0.001) | |||
| [34] | MCHH | √ | 2 doses of tetanus toxoid (TT) (OR = 1.98, p < 0.01) | |||
| [26] | CPHR | √ | 70% experimental and 65% control completed three vaccinations (reported as not statistically significant) | |||
| Utilization of antenatal care (ANC) | [32] | MCHH | √ | 67.5% pre-intervention 92.2% post intervention, p = 0.001 (≥3 ANC visits) | ||
| [21] | MCHH | √ | 55.9% case and 35.5% control, p < 0.05 | |||
| [34] | MCHH | √ | Significant with 6 ANC (OR = 1.67, p < 0.05) but not for 4 ANC (OR = 1.25) visits | |||
| [30] | MCHH | √ | R = 6.8 points—at least 1 ANC, R = 1.9—at least four ANC. Increased ANC attendance by four visits or more (AOR = 1.546, p < 0.05) but not significant with at least 1 ANC (OR = 1.476). | |||
| Practice of Breast Feeding (BF) and/or complementary feeding (CF) | [32] | MCHH | √ | 18.3% pre-intervention to 74.9% post-intervention, p < 0.001 (Exclusive BF) | ||
| [21] | MCHH | √ | 16.6% case and 0.7% control for BF (no p-value) | |||
| [34] | MCHH | √ | CF for 6–9 months (OR = 4.35, p < 0.001), continuing BF (OR = 2.31, p < 0.01), continuing feeding with added proteins/vitamin (OR = 1.54, p < 0.05), continuing feeding with fruits/extracts (OR = 2.18, p < 0.001), continuing feeding with various snacks (OR = 4.14, p < 0.001), start BF, then continue CF in 6–9 months (OR = 2.7, p < 0.001), training self-feeding (OR = 2.75, p < 0.001). No significant effect (p > 0.05) for exclusive BF (OR = 0.76), feeding soft-rice thrice a day (OR = 1.29) and some kind of side dishes (OR = 1.35). | |||
| Child growth and development | [37] | MCHH | √ | OR = 0.32 (protective effect) on the risk of cognitive delay (p = 0.007) | ||
| [34] | MCHH | √ | Less underweight children in case compared to control groups (OR = 0.33, p < 0.05), less stunted growth (OR = 0.53, p < 0.05) (adjusted for maternal BMI and birth weight of child). No significant difference in wasting growth (OR = 0.59, p > 0.05) | |||
| Uptake of Child vitamin A supplement | [21] | MCHH | √ | 17.6% case and 1.4% control (include both vitamin A and iron for mothers, no p-value) | ||
| [34] | MCHH | √ | Child vitamin A (OR = 2.0, p < 0.05) | |||
| Use of family planning | [21] | MCHH | √ | 41.5% case and 2% control (no p-value) | ||
| Parent-professional communication | [22] | CPHR | √ | Communication with nurses (82% intervention and 77% control p = 0.66), doctors (75% intervention and 75% control p = 0.78), other professionals (83% intervention and 77% control p = 0.6) | ||
| [23] | MCHH | √ | Effective only for women with at least secondary education (t-test = 2.03, p ≤ 0.05) but no overall effect (t-test = 1.38) (child health discussion) | |||
| [39] | CPHR | √ | 33.5% better communication with health visitors compared to GPs (24.6%), p = 0.008. | |||
| Mother-husband communication/husband support in MCH care | [23] | MCHH | √ | Slightly effective for women with at least secondary education (t-test = 1.83, p = 0.1) but no overall effect (t-test = 1.15) (child health discussion) | ||
| [34] | MCHH | √ | Significant in husbands’ support with respect to saving money for delivery (OR = 1.82, p < 0.01), keeping their baby warm (OR = 1.58, p < 0.05), and giving their child developmental stimulation (OR = 1.62, p < 0.05). Not significant with Identifying blood donor (OR = 1.24), Acknowledging the expected date of delivery (OR = 0.93), Preparing transportation to delivery settings (OR = 1.03), Preparing home setting for delivery of child (OR = 0.75), Contacting health personnel (OR = 0.89), Supporting mother to breastfeeding, Bathing the infant/child (OR = 0.85), Caring cord of newborn (OR = 0.66), Bringing child to the healthcare facility (OR = 0.67), Bringing child to community-based integrated health post (OR = 0.7) | |||
| Outcomes | Reference | Intervention Type: CPHR, MCHH | Impact of Intervention on Outcome | Effect Size/Comments | ||
|---|---|---|---|---|---|---|
| Positive | No Impact | Mixed | ||||
| Knowledge of child illness/MCH related conditions | [22] | CPHR | √ | 37% intervention and 47% control, p = 0.22 (child fever) | ||
| [34] | MCHH | √ | Mean (intervention/control) signs of: Newborn complications (1.64/1.84, p < 0.001, R = 0.29), sick child (1.93/2.28, p < 0.05, R = −0.28); preventing sick child (4.01 p < 0.001/3.68, p > 0.05, R = 0.56) | |||
| [30] | MCHH | √ | R = 6.2 points for anaemia, 9.9 for parasites, 7.5 for HIV transmission | |||
| Awareness on Breast feeding issues | [32] | MCHH | √ | 66.1% pre-intervention and 86.7% post-intervention, p < 0.001 (exclusive) | ||
| [23] | MCHH | √ | No overall effect (t-test = 1.14) but slightly significant for literate women (t-test = 1.85, p ≤ 0.1) (exclusive) | |||
| [21] | MCHH | √ | 28.7% of case and 4.6% of controls (no p-value) | |||
| [30] | MCHH | √ | R = 6.2 for early breast feeding (no p-value) | |||
| Awareness of pregnancy danger signs/ Complications | [21] | MCHH | √ | 46.9% case and 5% control groups (no p value) (rupture of the membrane) | ||
| [23] | MCHH | √ | t-test = 2.04, p ≤ 0.05 (rupture of membra ne) | |||
| [34] | MCHH | √ | Mean (intervention/control): Pregnancy complications (1.63/1.46 p < 0.001, R = 0.49), delivery complications (1.42/1.56 p < 0.001, R = 0.41), postpartum complications (1.02/1.04, p < 0.001, R = 0.31), birth preparedness and complication readiness (1.30/1.24, p < 0.05, R = 0.54) | |||
| [30] | MCHH | √ | Effective; R = 12.4—swelling, 18.1—Persistent vomiting, 6—Severe headache/blurred vision, 2.8—Convulsion, 19.7—Bleeding from vagina, 11.3 Premature Rupture of the membrane, 5.9—Prolonged labour, 6.5—Malpresentation, 0.6—Placenta accrete, 3.8—Convulsions (no p-value), but not for Severe bleeding after birth (R = −5.1) | |||
| Knowledge of child development | [22] | CPHR | √ | 86% intervention and 79% control, p = 0.4 | ||
| Knowledge of immunisation | [21] | MCHH | √ | 32.4% and 5.7% for case and controls (no p-value) | ||
| Knowledge of mother-child interaction | [22] | CPHR | √ | 52% intervention and 48% control, p = 0.84 | ||
| Knowledge of family planning | [21] | MCHH | √ | 60.8% case and 5.0% control (no p-value) | ||
| [23] | MCHH | √ | No overall effect (t-test = 1.4) but effective among literates (t-test = 3.16, p = 0.01). | |||
| Knowledge of recommended Antenatal care | [32] | MCHH | √ | 91.9% pre-intervention and 93.7% post intervention, p = 0.1559 (visits ≥ 3) | ||
| [21] | MCHH | √ | 78% case and 8.3% control groups, p < 0.05 | |||
| General health knowledge | [23] | MCHH | √ | No overall effect (t-test = 1.2) but effective with first delivery (t-test = 2.59, p = 0.01) (making oral rehydration salt) | ||
| [44] | MCHH | √ | ATT = 0.051 (t-test = 2.201, p < 0.05) (Treatment vs. control) (vaccination, danger signs, pregnancy risk factors and HIV/malaria prevention) | |||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chutiyami, M.; Wyver, S.; Amin, J. Are Parent-Held Child Health Records a Valuable Health Intervention? A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2019, 16, 220. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16020220
Chutiyami M, Wyver S, Amin J. Are Parent-Held Child Health Records a Valuable Health Intervention? A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2019; 16(2):220. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16020220
Chicago/Turabian StyleChutiyami, Muhammad, Shirley Wyver, and Janaki Amin. 2019. "Are Parent-Held Child Health Records a Valuable Health Intervention? A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 16, no. 2: 220. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16020220