Toxic Effect of Acute Cadmium and Lead Exposure in Rat Blood, Liver, and Kidney


 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Chemicals
2.2. Animals
2.3. Study Design and Experimental Procedure
2.4. Tissue Preparations
2.5. Toxic Metals and Bioelements Analysis
2.6. Hematology Analysis
2.7. Biochemical Assays
2.8. Redox Status Analysis
2.9. Histopathological Analysis
2.10. Statistical Analysis
3. Results
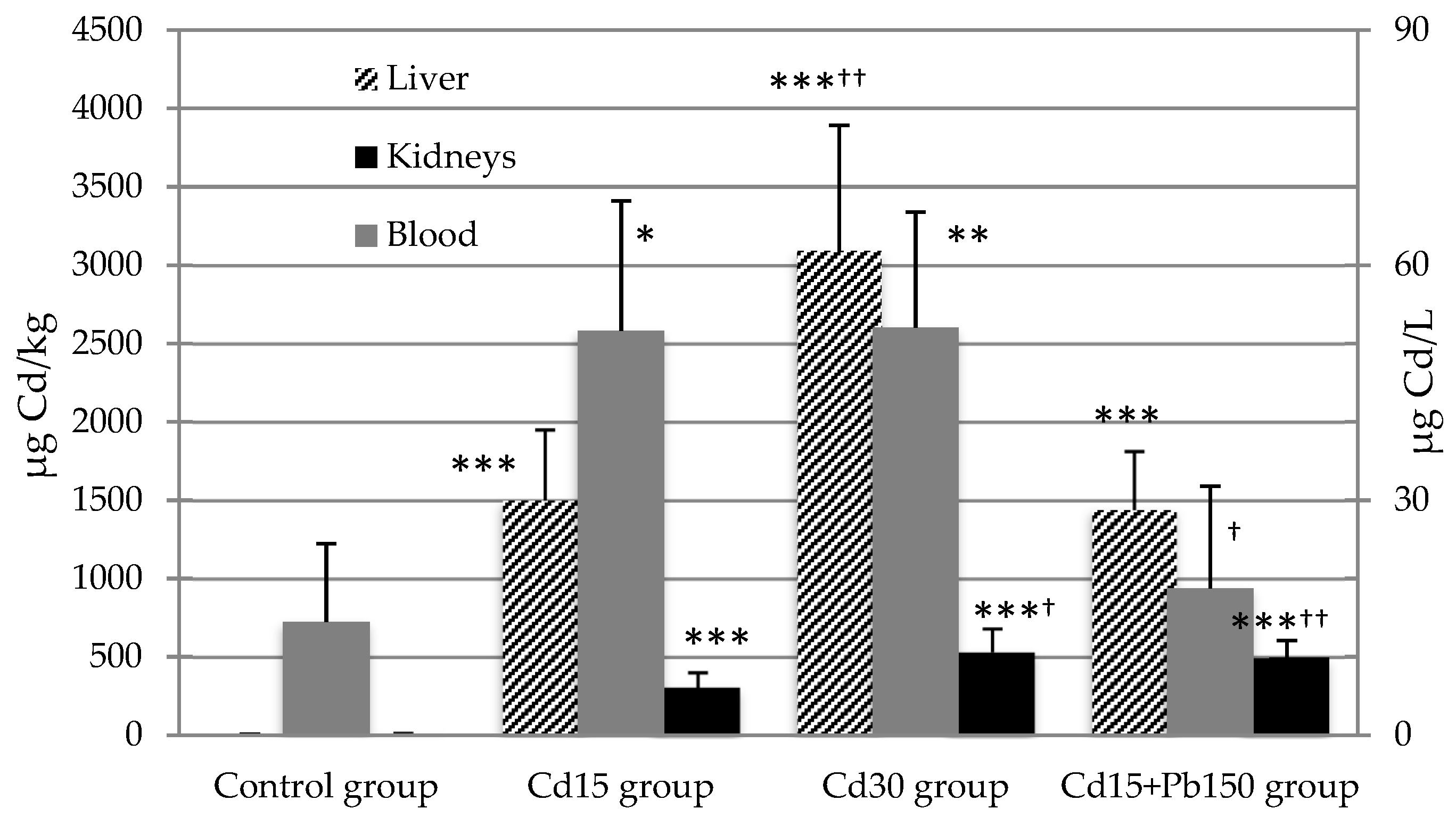
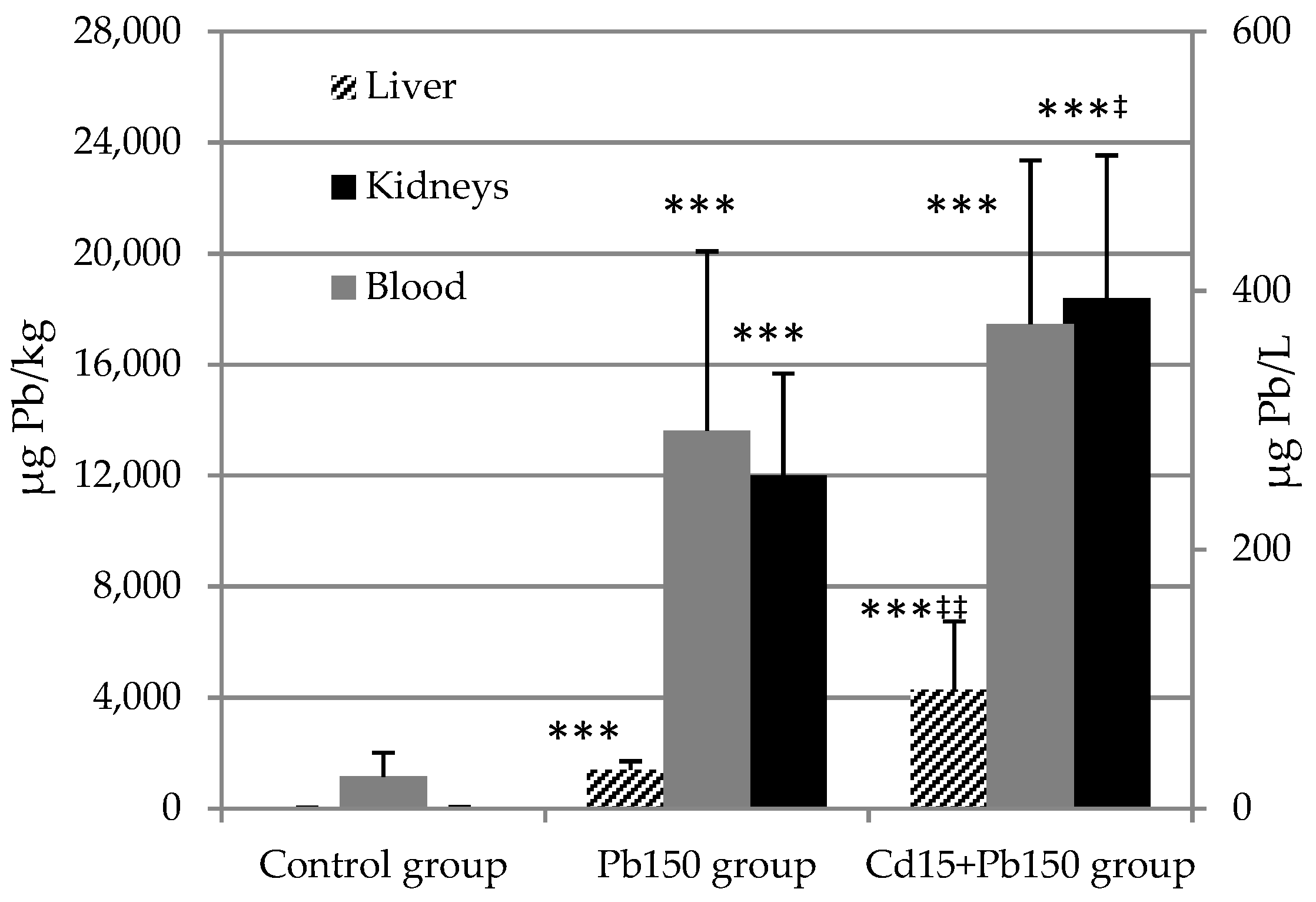
3.1. Cadmium and Lead Concentration in Tissues
3.2. Hematology
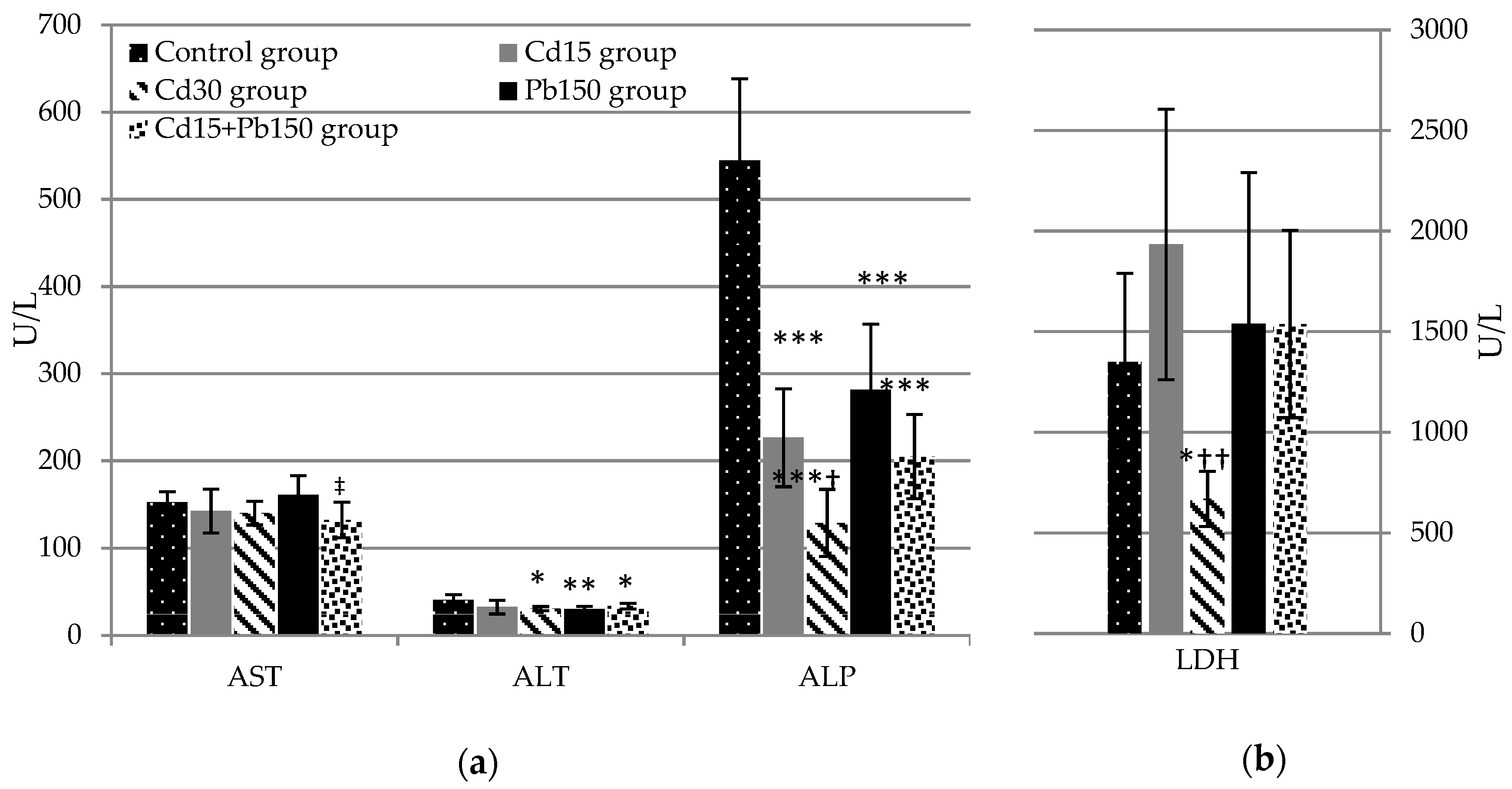
3.3. Biochemical Assays
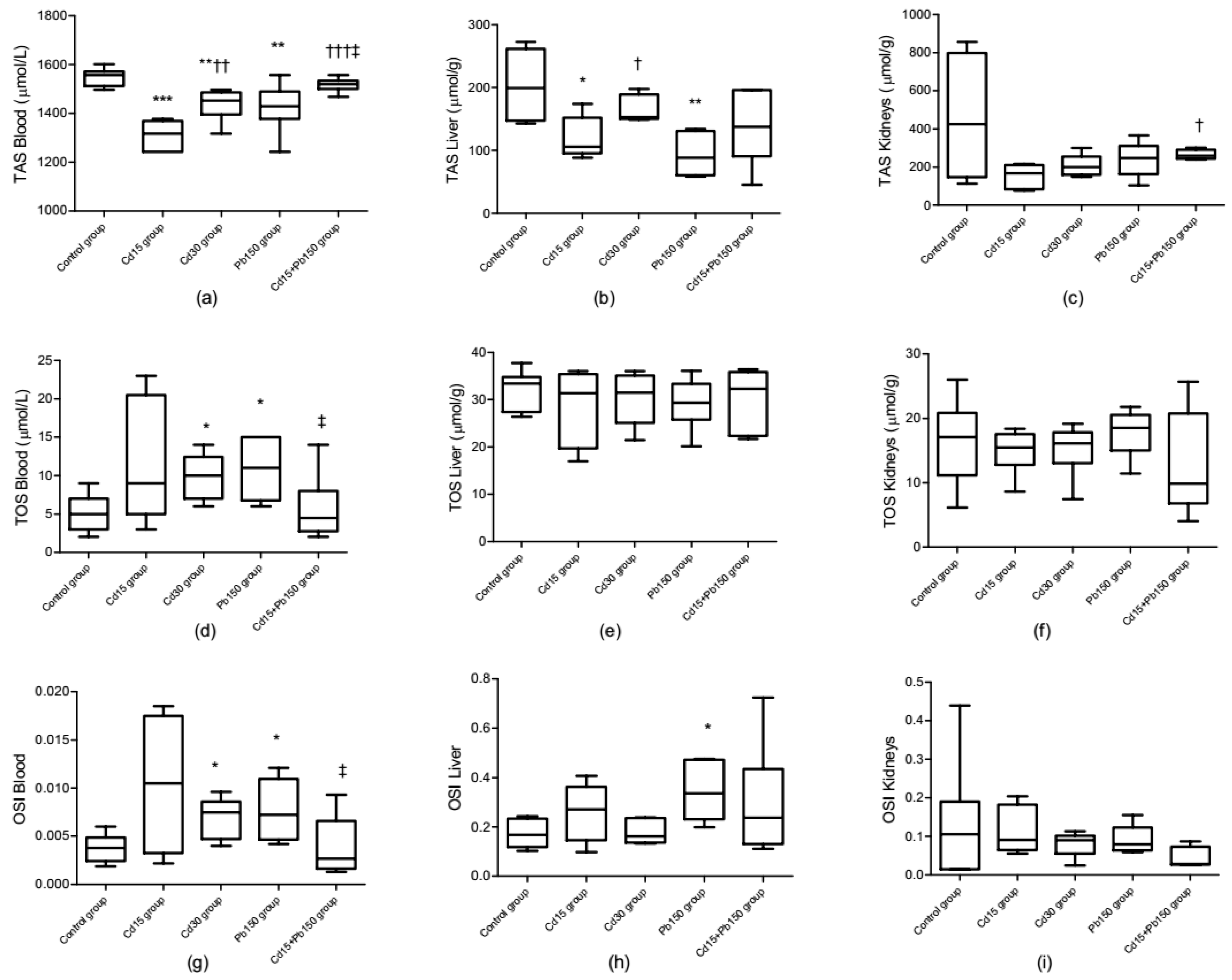
3.4. Redox Status
3.5. Bioelements Levels in Tissues
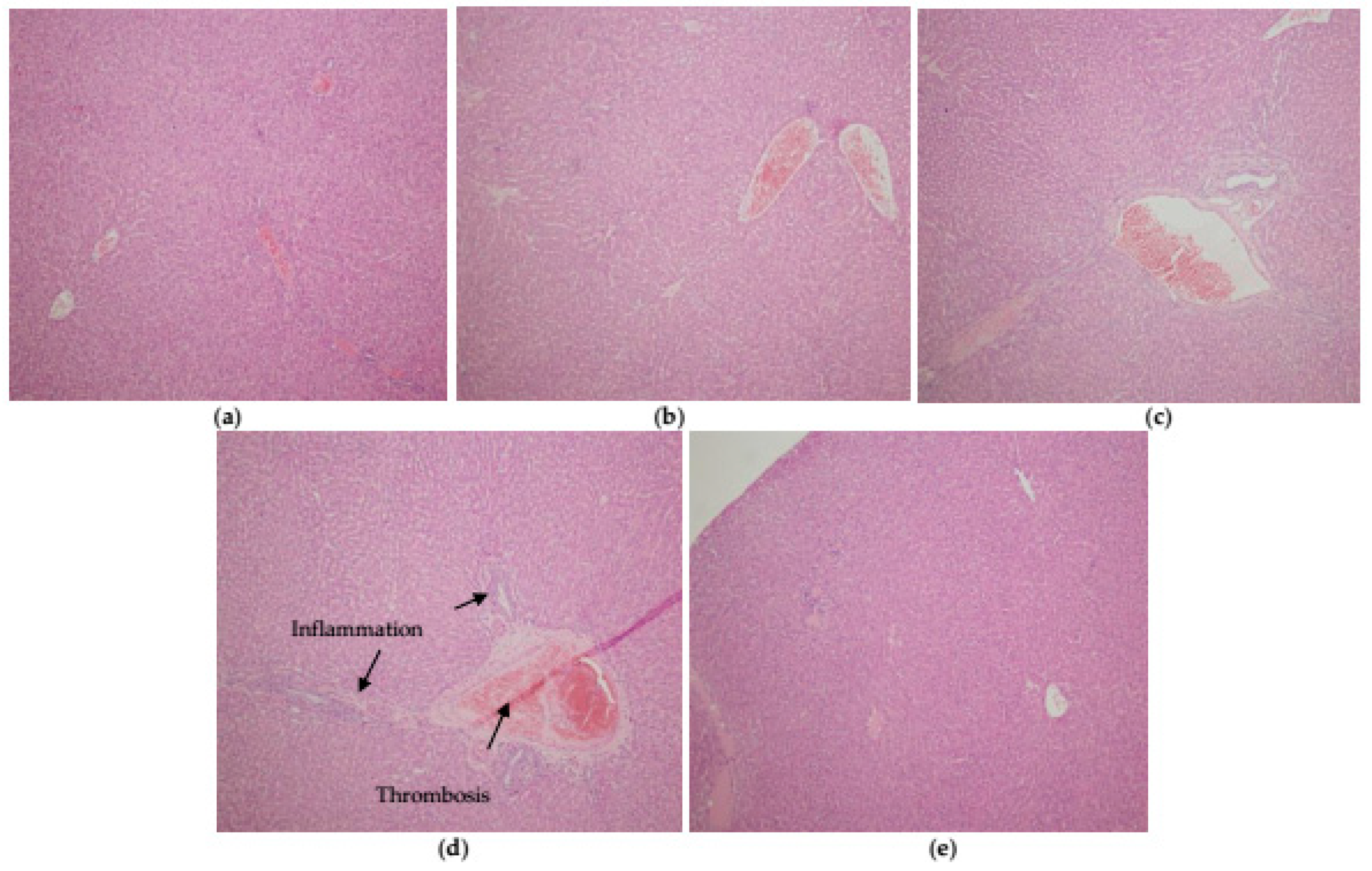
3.6. Histopathological Analysis
4. Discussion
4.1. Effects on the Hematopoietic System
4.2. Effects on Liver
4.3. Effects on Kidneys
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Järup, L.; Åkesson, A. Current status of cadmium as an environmental health problem. Toxicol. Appl. Pharmacol. 2009, 238, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Casas, S.J.; Sordo, J. Lead Chemistry, Analytical Aspects, Environmental Impact and Health Effects; Elsevier: Amsterdam, The Netherlands, 2006; ISBN 9780444529459. [Google Scholar]
- Satarug, S.; Garrett, S.H.; Sens, M.A.; Sens, D.A. Cadmium, environmental exposure, and health outcomes. Environ. Health Perspect. 2010, 118, 182–190. [Google Scholar] [CrossRef] [PubMed]
- Tchounwou, P.B.; Yedjou, C.G.; Patlolla, A.K.; Sutton, D.J. Heavy metal toxicity and the environment. EXS 2012, 101, 133–164. [Google Scholar] [PubMed]
- WHO Action Is Needed on Chemicals of Major Public Health Concern. Public Health Environmental. 2010, pp. 1–4. Available online: https://www.who.int/ipcs/assessment/public_health/chemicals_phc/en/ (accessed on 26 September 2018).
- ATSDR Substance Priority List|ATSDR. Available online: https://www.atsdr.cdc.gov/spl/ (accessed on 26 September 2018).
- Matović, V.; Buha, A.; Dukić-Ćosić, D.; Bulat, Z. Insight into the oxidative stress induced by lead and/or cadmium in blood, liver and kidneys. Food Chem. Toxicol. 2015, 78, 130–140. [Google Scholar] [CrossRef] [PubMed]
- Flora, S.J.S.; Agrawal, S. Arsenic, Cadmium, and Lead; Academic Press: Cambridge, MA, USA, 2017; ISBN 9780128042397. [Google Scholar]
- Matović, V.; Buha, A.; Bulat, Z.; Dukić-Ćosić, D.; Đukić-Ćosić, D. Cadmium toxicity revisited: Focus on oxidative stress induction and interactions with zinc and magnesium. Arh. Hig. Rada Toksikol. 2011, 62, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Flora, G.; Gupta, D.; Tiwari, A. Toxicity of lead: A review with recent updates. Interdiscip. Toxicol. 2012, 5, 47–58. [Google Scholar] [CrossRef]
- Nieboer, E.; Richardson, D.H.S. The replacement of the nondescript term “heavy metals” by a biologically and chemically significant classification of metal ions. Environ. Pollut. 1980, 1, 3–26. [Google Scholar] [CrossRef]
- Djukić-Ćosić, D.; Ninković, M.; Maličević, Ž.; Plamenac-Bulat, Z.; Matović, V. Effect of supplemental magnesium on the kidney levels of cadmium, zinc, and copper of mice exposed to toxic levels of cadmium. Biol. Trace Elem. Res. 2006, 114, 281–292. [Google Scholar] [CrossRef]
- Bulat, Z.P.; Djukić-Ćosić, D.; Maličević, Ž.; Bulat, P.; Matović, V. Zinc or magnesium supplementation modulates Cd intoxication in blood, kidney, spleen, and bone of rabbits. Biol. Trace Elem. Res. 2008, 124, 110–117. [Google Scholar] [CrossRef]
- Bulat, Z.; Dukić-Ćosić, D.; Antonijević, B.; Buha, A.; Bulat, P.; Pavlović, Z.; Matović, V. Can zinc supplementation ameliorate cadmium-induced alterations in the bioelement content in rabbits? Arh. Hig. Rada Toksikol. 2017, 68, 38–45. [Google Scholar] [CrossRef] [Green Version]
- Rani, A.; Kumar, A.; Lal, A.; Pant, M. Cellular mechanisms of cadmium-induced toxicity: A review. Int. J. Environ. Health Res. 2014, 24, 378–399. [Google Scholar] [CrossRef] [PubMed]
- Waisberg, M.; Joseph, P.; Hale, B.; Beyersmann, D. Molecular and cellular mechanisms of cadmium carcinogenesis. Toxicology 2003, 192, 95–117. [Google Scholar] [CrossRef]
- Joseph, P. Mechanisms of cadmium carcinogenesis. Toxicol. Appl. Pharmacol. 2009, 238, 272–279. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, Y.F.; Eldebaky, H.A.A.; Mahmoud, K.G.M.; Nawito, M. Effects of lead exposure on DNA damage and apoptosis in reproductive and vital organs in female rabbits. Glob. Vet. 2012, 9, 401–408. [Google Scholar]
- Świergosz-Kowalewska, R. Cadmium distribution and toxicity in tissues of small rodents. Microsc. Res. Tech. 2001, 55, 208–222. [Google Scholar] [CrossRef] [PubMed]
- Timchalk, C.; Lin, Y.; Weitz, K.K.; Wu, H.; Gies, R.A.; Moore, D.A.; Yantasee, W. Disposition of lead (Pb) in saliva and blood of Sprague-Dawley rats following a single or repeated oral exposure to Pb-acetate. Toxicology 2006, 222, 86–94. [Google Scholar] [CrossRef] [PubMed]
- Abadin, H.; Ashizawa, A.; Stevens, Y.-W.; Llados, F.; Diamond, G.; Sage, G.; Citra, M.; Quinones, A.; Bosch, S.J.; Swarts, S.G. Toxicological Profile for Lead; The United States Public Health Service, Agency for Toxic Substances and Disease Registry: Atlanta, GA, USA, 2007; p. 582.
- Agency for Toxic Substances and Disease Registry (ATSDR). Toxicological Profile for Cadmium; The United States Public Health Service, Agency for Toxic Substances and Disease Registry: Atlanta, GA, USA, 2012; pp. 1–487.
- Horiguchi, H.; Oguma, E.; Kayama, F. Cadmium induces anemia through interdependent progress of hemolysis, body iron accumulation, and insufficient erythropoietin production in rats. Toxicol. Sci. 2011, 122, 198–210. [Google Scholar] [CrossRef]
- Yuan, G.; Dai, S.; Yin, Z.; Lu, H.; Jia, R.; Xu, J.; Song, X.; Li, L.; Shu, Y.; Zhao, X. Toxicological assessment of combined lead and cadmium: Acute and sub-chronic toxicity study in rats. Food Chem. Toxicol. 2014, 65, 260–268. [Google Scholar] [CrossRef]
- Cobbina, S.J.; Chen, Y.; Zhou, Z.; Wu, X.; Zhao, T.; Zhang, Z.; Feng, W.; Wang, W.; Li, Q.; Wu, X.; et al. Toxicity assessment due to sub-chronic exposure to individual and mixtures of four toxic heavy metals. J. Hazard. Mater. 2015, 294, 109–120. [Google Scholar] [CrossRef]
- Yildirim, S.; Celikezen, F.C.; Oto, G.; Sengul, E.; Bulduk, M.; Tasdemir, M.; Ali Cinar, D. An investigation of protective effects of litium borate on blood and histopathological parameters in acute cadmium-induced rats. Biol. Trace Elem. Res. 2018, 182, 287–294. [Google Scholar] [CrossRef]
- Shaban El-Neweshy, M.; Said El-Sayed, Y. Influence of vitamin C supplementation on lead-induced histopathological alterations in male rats. Exp. Toxicol. Pathol. 2011, 63, 221–227. [Google Scholar] [CrossRef] [PubMed]
- El-Boshy, M.; Ashshi, A.; Gaith, M.; Qusty, N.; Bokhary, T.; AlTaweel, N.; Abdelhady, M. Studies on the protective effect of the artichoke (Cynara scolymus) leaf extract against cadmium toxicity-induced oxidative stress, hepatorenal damage, and immunosuppressive and hematological disorders in rats. Environ. Sci. Pollut. Res. 2017, 24, 12372–12383. [Google Scholar] [CrossRef] [PubMed]
- Abdou, H.M.; Hassan, M.A. Protective role of omega-3 polyunsaturated fatty acid against lead acetate-induced toxicity in liver and kidney of female rats. BioMed Res. Int. 2014, 2014, 435857. [Google Scholar] [CrossRef] [PubMed]
- Buha, A.; Matovic, V.; Antonijevic, B.; Bulat, Z.; Curcic, M.; Renieri, E.A.; Tsatsakis, A.M.; Schweitzer, A.; Wallace, D. Overview of cadmium thyroid disrupting effects and mechanisms. Int. J. Mol. Sci. 2018, 19, 1501. [Google Scholar] [CrossRef] [PubMed]
- Buha, A.; Wallace, D.; Matovic, V.; Schweitzer, A.; Oluic, B.; Micic, D.; Djordjevic, V. Cadmium exposure as a putative risk factor for the development of pancreatic cancer: Three different lines of evidence. BioMed Res. Int. 2017, 2017, 1981837. [Google Scholar] [CrossRef] [PubMed]
- Mezynska, M.; Brzóska, M.M. Environmental exposure to cadmium—A risk for health of the general population in industrialized countries and preventive strategies. Environ. Sci. Pollut. Res. 2018, 25, 3211–3232. [Google Scholar] [CrossRef] [PubMed]
- Carocci, A.; Catalano, A.; Lauria, G.; Sinicropi, M.S.; Genchi, G. Lead toxicity, antioxidant defense and environment. In Reviews of Environmental Contamination and Toxicology; Springer: Berlin, Germany, 2016; pp. 45–67. [Google Scholar]
- ATSDR. Case Studies in Environmental Medicine (CSEM) Lead Toxicity; ATSDR: Atlanta, GA, USA, 2019.
- Tang, L.; Chen, X.; Bao, Y.; Xu, W.; Lv, Y.; Wang, Z.; Wen, X. CT imaging biomarkers of bone damage induced by environmental level of cadmium exposure in male rats. Biol. Trace Elem. Res. 2016, 170, 146–151. [Google Scholar] [CrossRef] [PubMed]
- International Agency for Research on Cancer (IARC). Agents Classified by the IARC Monographs, Volumes 1–121; IARC Monographs: Lyon, France, 2018; pp. 1–25. [Google Scholar]
- Commission of the European Communities (CEC). A Europen Environment and Health Strategy. In Communication from the Commission to the Council, the Europen Parliament and the European Economics and Social Committee, Final; Commission of the European Communities: Brussels, Belgium, 2003. [Google Scholar]
- Wang, G.; Fowler, B.A. Roles of biomarkers in evaluating interactions among mixtures of lead, cadmium and arsenic. Toxicol. Appl. Pharmacol. 2008, 233, 92–99. [Google Scholar] [CrossRef]
- Pillai, A.; Gupta, S. Antioxidant enzyme activity and lipid peroxidation in liver of female rats co-exposed to lead and cadmium: Effects of vitamin E and Mn2+. Free Radic. Res. 2005, 39, 707–712. [Google Scholar] [CrossRef]
- Massó, E.L.; Corredor, L.; Antonio, M.T. Oxidative damage in liver after perinatal intoxication with lead and/or cadmium. J. Trace Elem. Med. Biol. 2007, 21, 210–216. [Google Scholar] [CrossRef]
- Matović, V.; Buha, A.; Bulat, Z.; Dukić-ćosić, D.; Miljković, M.; Ivanišević, J.; Kotur-Stevuljević, J. Route-dependent effects of cadmium/cadmium and magnesium acute treatment on parameters of oxidative stress in rat liver. Food Chem. Toxicol. 2012, 50, 552–557. [Google Scholar] [CrossRef] [PubMed]
- Buha, A.; Bulat, Z.; Dukic-Cosic, D.; Matovic, V. Effects of oral and intraperitoneal magnesium treatment against cadmium-induced oxidative stress in plasma of rats. Arh. Hig. Rada Toksikol. 2012, 63, 247–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pawa, S.; Ali, S. Liver necrosis and fulminant hepatic failure in rats: Protection by oxyanionic form of tungsten. Biochim. Biophys. Acta Mol. Basis Dis. 2004, 1688, 210–222. [Google Scholar] [CrossRef] [PubMed]
- Girotti, M.J.; Khan, N.; McLellan, B.A. Early measurement of systemic lipid peroxidation products in the plasma of major blunt trauma patients. J. Trauma 1991, 31, 32–35. [Google Scholar] [CrossRef] [PubMed]
- Witko-Sarsat, V.; Friedlander, M.; Capeillère-Blandin, C.; Nguyen-Khoa, T.; Nguyen, A.T.; Zingraff, J.; Jungers, P.; Descamps-Latscha, B. Advanced oxidation protein products as a novel marker of oxidative stress in uremia. Kidney Int. 1996, 49, 1304–1313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ellman, G.L. Tissue Sulfhydryl Groups. Arch. Biochem. Biophys. 1959, 82, 70–77. [Google Scholar] [CrossRef]
- Alamdari, D.H.; Paletas, K.; Pegiou, T.; Sarigianni, M.; Befani, C.; Koliakos, G. A novel assay for the evaluation of the prooxidant-antioxidant balance, before and after antioxidant vitamin administration in type II diabetes patients. Clin. Biochem. 2007, 40, 248–254. [Google Scholar] [CrossRef]
- Erel, O. A novel automated direct measurement method for total antioxidant capacity using a new generation, more stable ABTS radical cation. Clin. Biochem. 2004, 37, 277–285. [Google Scholar] [CrossRef]
- Erel, O. A new automated colorimetric method for measuring total oxidant status. Clin. Biochem. 2005, 38, 1103–11111. [Google Scholar] [CrossRef]
- Aycicek, A.; Erel, O. Total oxidant/antioxidant status in jaundiced newborns before and after phototherapy. J. Pediatr. 2007, 83, 319–322. [Google Scholar] [CrossRef]
- Misra, H.P.; Fridovich, I. The role of superoxide anion in the autoxidation of epinephrine and a simple assay for superoxide dismutase. J. Biol. Chem. 1972, 247, 3170–3175. [Google Scholar] [PubMed]
- Bradford, M.M. A rapid and sensitive method for the quantitation of microgram quantities of protein utilizing the principle of protein-dye binding. Anal. Biochem. 1976, 72, 248–254. [Google Scholar] [CrossRef]
- Weichselbaum, T.E. An accurate and rapid method for the determination of proteins in small amounts of blood serum and plasma. Am. J. Clin. Pathol. 1946, 10, 40–49. [Google Scholar] [CrossRef] [PubMed]
- Veglia, F.; Cighetti, G.; De Franceschi, M.; Zingaro, L.; Boccotti, L.; Tremoli, E.; Cavalca, V. Age- and gender-related oxidative status determined in healthy subjects by means of OXY-SCORE, a potential new comprehensive index. Biomarkers 2006, 11, 562–573. [Google Scholar] [CrossRef] [PubMed]
- Wu, B.; Liu, Z.; Xu, Y.; Li, D.; Li, M. Combined toxicity of cadmium and lead on the earthworm Eisenia fetida (Annelida, Oligochaeta). Ecotoxicol. Environ. Saf. 2012, 81, 122–126. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Cobbina, S.J.; Mao, G.; Xu, H.; Zhang, Z.; Yang, L. A review of toxicity and mechanisms of individual and mixtures of heavy metals in the environment. Environ. Sci. Pollut. Res. 2016, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Mladenović, J.; Ognjanović, B.; Dordević, N.; Matić, M.; Knežević, V.; Štajn, A.; Saičić, Z. Protective effects of oestradiol against cadmium-induced changes in blood parameters and oxidative damage in rats. Arh. Hig. Rada Toksikol. 2014, 65, 37–46. [Google Scholar] [CrossRef] [Green Version]
- Karmakar, R.; Bhattacharya, R.; Chatterjee, M. Biochemical, haematological and histopathological study in relation to time-related cadmium-induced hepatotoxicity in mice. BioMetals 2000, 13, 231–239. [Google Scholar] [CrossRef]
- El-Boshy, M.E.; Risha, E.F.; Abdelhamid, F.M.; Mubarak, M.S.; Hadda, T. Ben Protective effects of selenium against cadmium induced hematological disturbances, immunosuppressive, oxidative stress and hepatorenal damage in rats. J. Trace Elem. Med. Biol. 2015, 29, 104–110. [Google Scholar] [CrossRef]
- Lafuente, A.; González-Carracedo, A.; Romero, A.; Esquifino, A.I. Effect of cadmium on lymphocyte subsets distribution in thymus and spleen. J. Physiol. Biochem. 2003, 59, 43–48. [Google Scholar] [CrossRef]
- Omobowale, T.O.; Oyagbemi, A.A.; Akinrinde, A.S.; Saba, A.B.; Daramola, O.T.; Ogunpolu, B.S.; Olopade, J.O. Failure of recovery from lead induced hepatoxicity and disruption of erythrocyte antioxidant defence system in Wistar rats. Environ. Toxicol. Pharmacol. 2014, 37, 1202–1211. [Google Scholar] [CrossRef] [PubMed]
- Sharma, V.; Sharma, A.; Kansal, L. The effect of oral administration of Allium sativum extracts on lead nitrate induced toxicity in male mice. Food Chem. Toxicol. 2010, 48, 928–936. [Google Scholar] [CrossRef] [PubMed]
- Djokic, J.; Ninkov, M.; Mirkov, I.; Popov Aleksandrov, A.; Zolotarevski, L.; Kataranovski, D.; Kataranovski, M. Differential effects of cadmium administration on peripheral blood granulocytes in rats. Environ. Toxicol. Pharmacol. 2014, 37, 210–219. [Google Scholar] [CrossRef] [PubMed]
- Kataranovski, M.; Janković, S.; Kataranovski, D.; Stoŝić, J.; Bogojević, D. Gender differences in acute cadmium-induced systemic inflammation in rats. BioMed Environ. Sci. 2009, 22, 1–7. [Google Scholar] [CrossRef]
- Sharma, V.; Kansal, L.; Sharma, A.; Lodi, S.; Sharma, S. Ameliorating effect of coriandum sativum extracts on hematological and immunological variables in an animal model of lead intoxication. J. Pharm. Allied Health Serv. 2011, 1, 16–29. [Google Scholar]
- Patra, R.C.; Rautray, A.K.; Swarup, D. Oxidative stress in lead and cadmium toxicity and its amelioration. Vet. Med. Int. 2011, 2011, 457327. [Google Scholar] [CrossRef] [PubMed]
- Olisekodiaka, M.J.; Igbeneghu, C.A.; Onuegbu, A.J.; Oduru, R.; Lawal, A.O. Lipid, lipoproteins, total antioxidant status and organ changes in rats administered high doses of cadmium chloride. Med. Princ. Pract. 2012, 21, 156–159. [Google Scholar] [CrossRef] [PubMed]
- Curcic, M.; Buha, A.; Stankovic, S.; Milovanovic, V.; Bulat, Z.; Đukić-Ćosić, D.; Antonijević, E.; Vučinić, S.; Matović, V.; Antonijevic, B. Interactions between cadmium and decabrominated diphenyl ether on blood cells count in rats—Multiple factorial regression analysis. Toxicology 2017, 376, 120–125. [Google Scholar] [CrossRef]
- Nordberg, G.F. Historical perspectives on cadmium toxicology. Toxicol. Appl. Pharmacol. 2009, 238, 192–200. [Google Scholar] [CrossRef]
- Ballatori, N. Transport of toxic metals by molecular mimicry. Environ. Health Perspect. 2002, 110, 689–694. [Google Scholar] [CrossRef]
- Djukić-Ćosić, D.; Ćurčić Jovanović, M.; Plamenac Bulat, Z.; Ninković, M.; Maličević, Ž.; Matović, V. Relation between lipid peroxidation and iron concentration in mouse liver after acute and subacute cadmium intoxication. J. Trace Elem. Med. Biol. 2008, 22, 66–72. [Google Scholar] [CrossRef]
- Burtis, A.C.; Edwrd, R.; Bruns, E.D. Tietz: Fundamentals of Clinical Chemistry; Elsevier: Amsterdam, The Netherlands, 2001; ISBN 9780721638652. [Google Scholar]
- Pande, M.; Mehta, A.; Pant, B.P.; Flora, S.J.S. Combined administration of a chelating agent and an antioxidant in the prevention and treatment of acute lead intoxication in rats. Environ. Toxicol. Pharmacol. 2001, 9, 173–184. [Google Scholar] [CrossRef]
- Sivaprasad, R.; Nagaraj, M.; Varalakshmi, P. Combined efficacies of lipoic acid and 2,3-dimercaptosuccinic acid against lead-induced lipid peroxidation in rat liver. J. Nutr. Biochem. 2004, 15, 18–23. [Google Scholar] [CrossRef]
- Zhu, H.; Jia, Y.; Cao, H.; Meng, F.; Liu, X. Biochemical and histopathological effects of subchronic oral exposure of rats to a mixture of five toxic elements. Food Chem. Toxicol. 2014, 71, 166–175. [Google Scholar] [CrossRef] [PubMed]
- Bulat, Z.; Đukić-Ćosić, D.; Antonijević, B.; Bulat, P.; Vujanović, D.; Buha, A.; Matović, V. Effect of magnesium supplementation on the distribution patterns of zinc, copper, and magnesium in rabbits exposed to prolonged cadmium intoxication. Sci. World J. 2012, 2012, 572514. [Google Scholar] [CrossRef] [PubMed]
- Matović, V.; Bulat, Z.P.; Djukić-Ćosić, D.; Soldatović, D. Antagonism between cadmium and magnesium: A possible role of magnesium in therapy of cadmium intoxication. Magnes. Res. 2010, 23, 19–26. [Google Scholar] [PubMed]
- Nordberg, G.F. Cadmium and health in the 21st Century—Historical remarks and trends for the future. BioMetals 2004, 17, 485–489. [Google Scholar] [CrossRef]
- Yalin, S.; Comelekoglu, U.; Bagis, S.; Sahin, N.O.; Ogenler, O.; Hatungil, R. Acute effect of single-dose cadmium treatment on lipid peroxidation and antioxidant enzymes in ovariectomized rats. Ecotoxicol. Environ. Saf. 2006, 65, 140–144. [Google Scholar] [CrossRef]
- Othman, A.I.; El Missiry, M.A. Role of selenium against lead toxicity in male rats. J. Biochem. Mol. Toxicol. 1998, 12, 345–349. [Google Scholar] [CrossRef]
- Borgert, C.J.; Price, B.; Wells, C.S.; Simon, G.S. Evaluating chemical interaction studies for mixture risk assessment. Hum. Ecol. Risk Assess. Int. J. 2001, 7, 259–306. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control Group | Cd15 Group | Cd30 Group | Pb150 Group | Cd15 + Pb150 Group | |
|---|---|---|---|---|---|
| WBC (109/L) 1 | 3.85 ± 0.68 | 3.56 ± 0.53 | 2.36 ± 0.32 *** †† | 4.08 ± 0.75 | 3.97 ± 0.66 |
| Lymphocyte (109/L) 2 | 2.58 1.84–2.94 | 1.84 ** 1.36–2.11 | 1.15 ** †† 1.01–1.16 | 2.54 2.18–2.77 | 2.22 1.44–2.69 |
| Neutrophils (109/L) 2 | 1.02 0.80–1.41 | 1.21 0.73–1.99 | 0.88 0.75–1.18 | 1.27 0.81–1.43 | 1.23 * 0.95–2.14 |
| RBC (1012/L) 1 | 6.91 ± 0.25 | 5.61 ± 0.98 *** | 5.05 ± 0.61 *** | 5.74 ± 0.67 ** | 5.19 ± 0.74 *** |
| HGB (g/L) 2 | 148.0 143.0–161.0 | 139.0 * 105.0–154.0 | 117.5 *** 104.0–128.0 | 126.5 * 118.0–153.0 | 117.0 *** 94.0–127.0 |
| HCT (L/L) 2 | 0.401 0.380–0.410 | 0.343 * 0.250–0.410 | 0.314 *** 0.260–0.340 | 0.336 * 0.300–0.420 | 0.303 *** 0.210–0.340 |
| MCV (fL) 2 | 58.0 56.0–61.0 | 58.0 57.0–62.0 | 60.5 56.0–69.9 | 60.0 56.0–63.0 | 58.0 56.0–59.0 |
| MCH (pg) 2 | 21.0 20.0–23.0 | 23.5 ** 22.0–25.0 | 23.0 * 22.0–26.0 | 22.5 22.0–24.0 | 22.0 21.0–26.0 |
| MCHC (g/L) 2 | 370.0 361.0–390.0 | 398.0 379.0–420.0 | 386.5 349.0–409.0 | 383.0 361.0–397.0 | 379.0 372.0–447.0 |
| PLT (109/L) 1 | 571.25 ± 43.03 | 701.00 ± 40.30 ** | 341.50 ± 92.36 *** ††† | 449.50 ± 100.60 ** | 525.00 ± 53.86 ††† |
| Control Group | Cd15 Group | Cd30 Group | Pb150 Group | Cd15 + Pb150 Group | |
|---|---|---|---|---|---|
| BUN (mmol/L) 1 | 10.72 ± 1.02 | 8.56 ± 0.82 *** | 8.76 ± 1.08 ** | 8.76 ± 1.12 ** | 9.08 ± 1.13 ** |
| CRE (µmol/L) 2 | 42.45 39.5–43.4 | 44.75 35.5–53.4 | 45.45 ** 42.8–53.4 | 43.40 * 41.4–46.7 | 43.40 40.5–46.1 |
| TP (g/L) 2 | 59.0 53.4–63.3 | 60.3 45.3–74.2 | 61.8 53.4–64.9 | 59.5 55.1–66.8 | 52.4 ** ‡ 48.7–58.0 |
| ALB (g/L) 2 | 32.1 29.4–35.7 | 28.8 22.5–36.6 | 30.3 27.0–33.4 | 30.7 29.9–32.1 | 28.8 * 26.3–32.0 |
| DB (µmol/L) 2 | 0.4 0.3–0.5 | 0.45 0.2–0.5 | 0.4 0.3–0.6 | 0.7 ** 0.7–0.9 | 0.4 ‡‡ 0.4–0.6 |
| TB (µmol/L) 1 | 2.04 ± 0.16 | 2.56 ± 0.33 ** | 2.38 ± 0.38 * | 2.24 ± 0.16 | 2.18 ± 0.14 † |
| Fe (µmol/L) 1 | 61.7 ± 11.4 | 27.5 ± 8.8 *** | 21.6 ± 5.8 *** | 36.3 ± 10.5 *** | 31.4 ± 6.3 *** |
| Ca (mmol/L) 2 | 2.93 2.5–3.2 | 2.73 2.2–3.2 | 2.65 2.5–3.1 | 2.65 * 2.5–2.9 | 2.48 ** 2.2–2.7 |
| Mg (mmol/L) 2 | 1.70 1.5–1.9 | 1.55 1.1–2.2 | 1.30 * 1.3–1.8 | 1.35 *** 1.0–1.5 | 1.30 *** 1.1–1.5 |
| P (mmol/L) 2 | 3.05 3.0–3.4 | 2.87 2.6–4.4 | 2.71 * 2.4–3.3 | 3.15 2.9–3.2 | 3.05 2.1–3.4 |
| Cl (mmol/L) 2 | 105.0 102.0–109.0 | 110.5 102.0–118.0 | 108.5 * 105.0–116.0 | 113.0 *** 108.0–118.0 | 106.0 ‡‡ 100.0–109.0 |
| Control Group | Cd15 Group | Cd30 Group | Pb150 Group | Cd15 + Pb150 Group | ||
|---|---|---|---|---|---|---|
| Blood | MDA (µmol/L) | 2.23 1.99–3.68 | 1.94 1.49–2.82 | 2.66 † 2.17–3.13 | 2.10 1.62–2.46 | 2.41 † ‡ 2.16–3.21 |
| AOPP (µmol/g protein) | 1.84 1.67–2.19 | 1.40 * 1.20–1.95 | 1.97 1.26–3.68 | 2.34 1.53–6.04 | 13.53 *** ††† ‡‡‡ 9.94–16.59 | |
| SH-groups (mmol/L) | 0.12 0.08–0.21 | 0.16 0.10–0.22 | 0.13 0.10–0.13 | 0.16 0.13–0.26 | 0.18 0.13–0.27 | |
| PAB (HCU) | 136.6 105.3–181.6 | 186.2 169.0–215.9 | 189.6 144.3–203.5 | 191.0 133.6–201.4 | 128.6 87.2–150.0 | |
| Liver | MDA (µmol/mg protein) | 80.1 56.77–95.52 | 75.76 64.08–89.08 | 104.75 68.64–124.80 | 77.15 36.59–101.19 | 76.59 62.66–98.31 |
| AOPP (µmol/g protein) | 83.16 35.82–166.36 | 234.84 *** 172.37–252.13 | 201.66 *** 179.94–324.36 | 178.99 * 114.81–228.23 | 81.42 †† 38.05–194.69 | |
| SH groups (mmol/g protein) | 0.31 0.25–0.33 | 0.31 0.22–0.38 | 0.30 0.25–0.40 | 0.31 0.20–0.39 | 0.27 0.15–0.36 | |
| SOD (U/g) | 56.92 52.07–60.82 | 53.56 45.54–57.35 | 52.8 048.47–59.67 | 55.70 47.77–60.65 | 52.45 51.48–63.25 | |
| Kidneys | MDA (µmol/mg protein) | 209.42 132.68–232.39 | 171.94 143.99–253.74 | 237.65 † 194.81–397.13 | 283.88 * 197.42–328.57 | 273.15 *** †† 233.25–321.88 |
| AOPP (µmol/g protein) | 273.68 153.97–341.22 | 255.58 206.36–317.21 | 286.65 250.53–360.61 | 297.75 231.56–368.82 | 273.79 226.38–362.08 | |
| SH groups (mmol/g protein) | 0.27 0.18–0.34 | 0.25 0.17–0.39 | 0.25 0.21–0.35 | 0.24 0.22–0.30 | 0.27 0.17–0.31 | |
| SOD (U/g) | 62.31 37.84–74.04 | 57.02 46.90–63.07 | 52.56 46.88–70.01 | 61.83 50.54–73.51 | 60.65 37.58–76.60 | |
| Control Group | Cd15 Group | Cd30 Group | Pb150 Group | Cd15 + Pb150 Group | |
|---|---|---|---|---|---|
| Damage score | −0.083 ± 0.49 | 0.088 ± 0.51 | 0.526 ± 0.26 * | 0.485 ± 0.24 * | −0.254 ± 0.39 ‡ |
| Protection score | −0.038 ± 0.34 | −0.37 ± 0.56 | −0.29 ± 0.24 | −0.11 ± 0.37 | −0.22 ± 0.63 |
| OXY-score | −0.045 ± 0.58 | 0.46 ± 0.89 | 0.81 ± 0.39 * | 0.77 ± 0.30 * | −0.037 ± 0.80 ‡ |
| Blood | Liver | Kidney | ||||
|---|---|---|---|---|---|---|
| Cu (µmol/L) | Zn (µmol/L) | Cu (µmol/kg) | Zn (µmol/kg) | Cu (µmol/kg) | Zn (µmol/kg) | |
| Control group | 22.10 ± 1.81 | 87.76 ± 3.24 | 50.74 ± 2.80 | 462.77 ± 57.37 | 96.92 ± 10.39 | 374.18 ± 38.14 |
| Cd15 group | 16.09 ± 1.22 *** | 93.19 ± 8.61 | 57.60 ± 5.58 | 585.16 ± 90.11 ** | 79.27 ± 4.06 | 299.70 ± 25.88 *** |
| Cd30 group | 20.00 ± 2.34 †† | 74.20 ± 15.81 * ††† | 65.08 ± 10.48 ** | 576.49 ± 43.11 * | 88.27 ± 21.02 | 310.47 ± 12.89 *** |
| Pb150 group | 20.59 ± 2.40 | 92.23 ± 7.62 | 63.26 ± 3.65 * | 613.06 ± 24.48 *** | 110.95 ± 22.11 | 329.07 ± 22.95 ** |
| Cd15 + Pb150 group | 20.19 ± 1.53 ††† | 81.04 ± 7.34 † ‡ | 67.00 ± 13.17 ** | 609.78 ± 102.73 *** | 95.42 ± 11.37 | 336.67 ± 24.44 * † |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andjelkovic, M.; Buha Djordjevic, A.; Antonijevic, E.; Antonijevic, B.; Stanic, M.; Kotur-Stevuljevic, J.; Spasojevic-Kalimanovska, V.; Jovanovic, M.; Boricic, N.; Wallace, D.; et al. Toxic Effect of Acute Cadmium and Lead Exposure in Rat Blood, Liver, and Kidney. Int. J. Environ. Res. Public Health 2019, 16, 274. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16020274
Andjelkovic M, Buha Djordjevic A, Antonijevic E, Antonijevic B, Stanic M, Kotur-Stevuljevic J, Spasojevic-Kalimanovska V, Jovanovic M, Boricic N, Wallace D, et al. Toxic Effect of Acute Cadmium and Lead Exposure in Rat Blood, Liver, and Kidney. International Journal of Environmental Research and Public Health. 2019; 16(2):274. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16020274
Chicago/Turabian StyleAndjelkovic, Milena, Aleksandra Buha Djordjevic, Evica Antonijevic, Biljana Antonijevic, Momcilo Stanic, Jelena Kotur-Stevuljevic, Vesna Spasojevic-Kalimanovska, Milos Jovanovic, Novica Boricic, David Wallace, and et al. 2019. "Toxic Effect of Acute Cadmium and Lead Exposure in Rat Blood, Liver, and Kidney" International Journal of Environmental Research and Public Health 16, no. 2: 274. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16020274