Ambient Temperature and Associations with Daily Visits to a Psychiatric Emergency Unit in Sweden


Abstract
:1. Introduction
2. Materials and Methods
2.1. Exposure Data
2.2. Outcome Data
2.3. Statistical Methods
3. Results
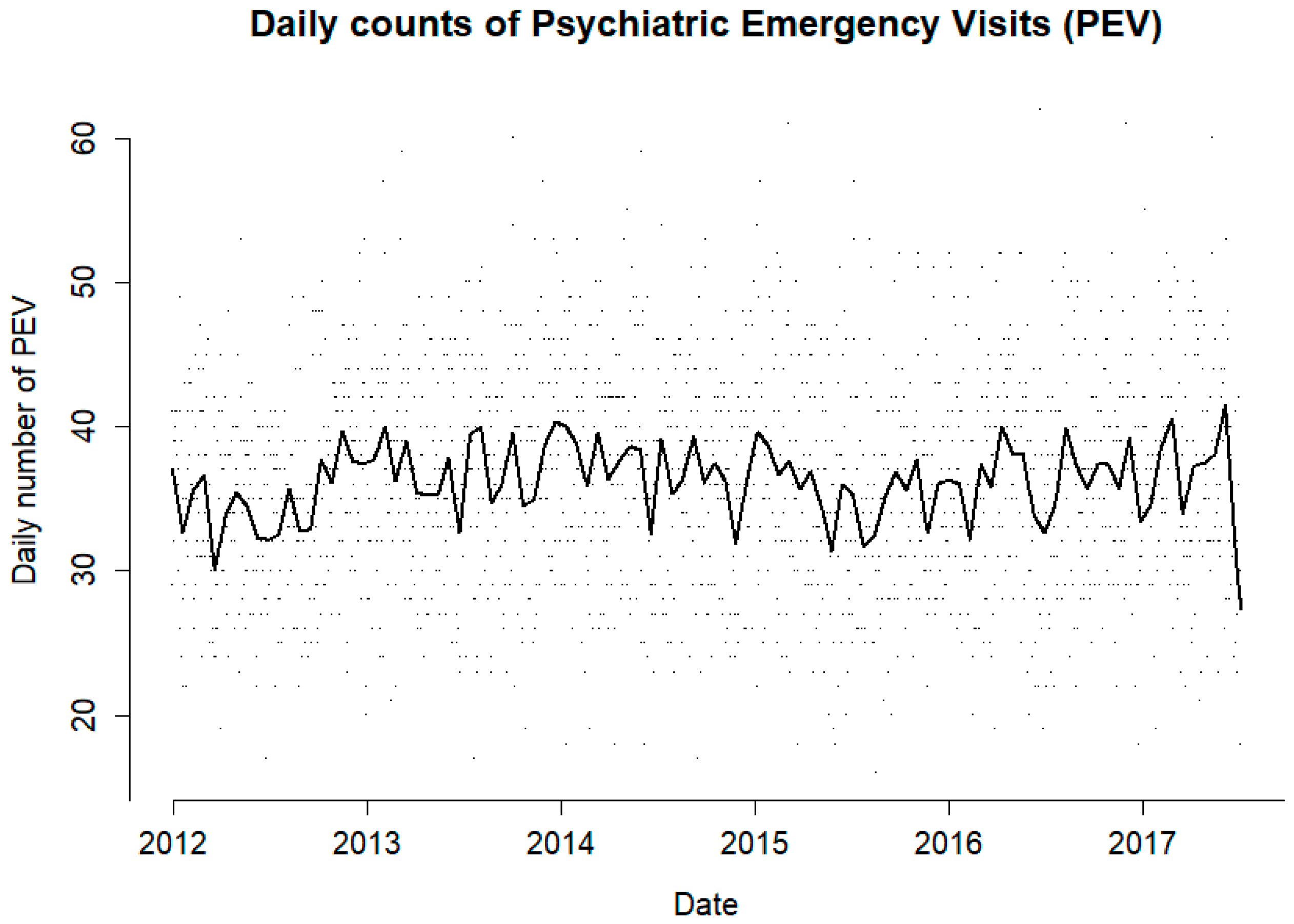
3.1. Descriptive
3.2. Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Rau, R.; Bohk-Ewald, C.; Muszyńska, M.M.; Vaupel, J.W. Seasonality of Causes of Death. In Visualizing Mortality Dynamics in the Lexis Diagram; Rau, R., Bohk-Ewald, C., Muszyńska, M.M., Vaupel, J.W., Eds.; The Springer Series on Demographic Methods and Population Analysis; Springer International Publishing: Cham, Switzerland, 2018; pp. 99–122. ISBN 978-3-319-64820-0. [Google Scholar]
- Galvão, P.; Silva, H.; Silva, C. Temporal distribution of suicide mortality: A systematic review. J Affect Disord. 2017, 228, 132–142. [Google Scholar] [CrossRef] [PubMed]
- Shiloh, R.; Shapira, A.; Potchter, O.; Hermesh, H.; Popper, M.; Weizman, A. Effects of climate on admission rates of schizophrenia patients to psychiatric hospitals. Eur. Psychiatry 2005, 20, 61–64. [Google Scholar] [CrossRef] [PubMed]
- McWilliams, S.; Kinsella, A.; O’Callaghan, E. The effects of daily weather variables on psychosis admissions to psychiatric hospitals. Int. J. Biometeorol. 2013, 57, 497–508. [Google Scholar] [CrossRef] [PubMed]
- Peng, Z.; Wang, Q.; Kan, H.; Chen, R.; Wang, W. Effects of ambient temperature on daily hospital admissions for mental disorders in Shanghai, China: A time-series analysis. Sci. Total Environ. 2017, 590–591, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Carney, P.A.; Fitzgerald, C.T.; Monaghan, C.E. Influence of climate on the prevalence of mania. Br. J. Psychiatry 1988, 152, 820–823. [Google Scholar] [CrossRef] [PubMed]
- Medici, C.R.; Vestergaard, C.H.; Hadzi-Pavlovic, D.; Munk-Jørgensen, P.; Parker, G. Seasonal variations in hospital admissions for mania: Examining for associations with weather variables over time. J. Affect. Disord. 2016, 205, 81–86. [Google Scholar] [CrossRef] [PubMed]
- Aguglia, A.; Moncalvo, M.; Solia, F.; Maina, G. Involuntary admissions in Italy: The impact of seasonality. Int. J. Psychiatry Clin. Pract. 2016, 20, 232–238. [Google Scholar] [CrossRef] [PubMed]
- Nitschke, M.; Tucker, G.R.; Bi, P. Morbidity and mortality during heatwaves in metropolitan Adelaide. Med. J. Aust. 2007, 187, 662–665. [Google Scholar] [PubMed]
- Hansen, A.; Bi, P.; Nitschke, M.; Ryan, P.; Pisaniello, D.; Tucker, G. The effect of heat waves on mental health in a temperate Australian city. Environ. Health Perspect. 2008, 116, 1369–1375. [Google Scholar] [CrossRef]
- Trang, P.M.; Rocklöv, J.; Giang, K.B.; Kullgren, G.; Nilsson, M. Heatwaves and Hospital Admissions for Mental Disorders in Northern Vietnam. PLoS ONE 2016, 11, e0155609. [Google Scholar] [CrossRef]
- Wang, X.; Lavigne, E.; Ouellette-Kuntz, H.; Chen, B.E. Acute impacts of extreme temperature exposure on emergency room admissions related to mental and behavior disorders in Toronto, Canada. J. Affect. Disord. 2014, 155, 154–161. [Google Scholar] [CrossRef] [PubMed]
- Linares, C.; Culqui, D.; Carmona, R.; Ortiz, C.; Díaz, J. Short-term association between environmental factors and hospital admissions due to dementia in Madrid. Environ. Res. 2017, 152, 214–220. [Google Scholar] [CrossRef] [PubMed]
- Rocklöv, J.; Forsberg, B.; Ebi, K.; Bellander, T. Susceptibility to mortality related to temperature and heat and cold wave duration in the population of Stockholm County, Sweden. Glob. Health Act. 2014, 7, 22737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Intergovernmental Panel on Climate Change. IPCC Fifth Assessment Report; Intergovernmental Panel on Climate Change: Geneva, Switzerland, 2015. [Google Scholar]
- Kessler, R.C.; Heeringa, S.; Lakoma, M.D.; Petukhova, M.; Rupp, A.E.; Schoenbaum, M.; Wang, P.S.; Zaslavsky, A.M. The individual-level and societal-level effects of mental disorders on earnings in the United States: Results from the National Comorbidity Survey Replication. Am. J. Psychiatry 2008, 165, 703–711. [Google Scholar] [CrossRef]
- SMHI Normal Dygnsnederbörd Minst 0.1 mm, medelvärde 1961–1990|SMHI. Available online: http://www.smhi.se/klimatdata/meteorologi/nederbord/normal-dygnsnederbord-minst-0-1-mm-medelvarde-1961-1990-1.4164 (accessed on 4 April 2018).
- Oudin, A.; Åström, D.O.; Asplund, P.; Steingrimsson, S.; Szabo, Z.; Carlsen, H.K. The association between daily concentrations of air pollution and visits to a psychiatric emergency unit: A case-crossover study. Environ. Health 2018, 17, 4. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Zeger, S.L. On the equivalence of case-crossover and time series methods in environmental epidemiology. Biostatistics 2007, 8, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Gasparrini, A.; Guo, Y.; Hashizume, M.; Lavigne, E.; Zanobetti, A.; Schwartz, J.; Tobias, A.; Tong, S.; Rocklöv, J.; Forsberg, B.; et al. Mortality risk attributable to high and low ambient temperature: A multicountry observational study. Lancet 2015, 386, 369–375. [Google Scholar] [CrossRef]
- Armstrong, B.G.; Gasparrini, A.; Tobias, A. Conditional Poisson models: A flexible alternative to conditional logistic case cross-over analysis. BMC Med. Res. Methodol. 2014, 14, 122. [Google Scholar] [CrossRef]
- Gasparrini, A. Modelling Lagged Associations in Environmental Time Series Data: A Simulation Study., Modelling lagged associations in environmental time series data: A simulation study. Epidemiology 2016, 27, 835–842. [Google Scholar] [CrossRef]
- Gasparrini, A.; Armstrong, B.; Kenward, M.G. Distributed lag non-linear models. Stat. Med. 2010, 29, 2224–2234. [Google Scholar] [CrossRef]
- Page, L.A.; Hajat, S.; Kovats, R.S. Relationship between daily suicide counts and temperature in England and Wales. Br. J. Psychiatry 2007, 191, 106–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zanobetti, A.; O’Neill, M.S.; Gronlund, C.J.; Schwartz, J.D. Susceptibility to Mortality in Weather Extremes: Effect Modification by Personal and Small Area Characteristics in a Multi-City Case-Only Analysis. Epidemiology 2013, 24, 809–819. [Google Scholar] [CrossRef] [PubMed]
- Orru, H.; Åström, D.O. Increases in external cause mortality due to high and low temperatures: Evidence from northeastern Europe. Int. J. Biometeorol. 2017, 61, 963–966. [Google Scholar] [CrossRef] [PubMed]
- Semenza, J.C.; Rubin, C.H.; Falter, K.H.; Selanikio, J.D.; Flanders, W.D.; Howe, H.L.; Wilhelm, J.L. Heat-related deaths during the July 1995 heat wave in Chicago. N. Engl. J. Med. 1996, 335, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Naughton, M.P.; Henderson, A.; Mirabelli, M.C.; Kaiser, R.; Wilhelm, J.L.; Kieszak, S.M.; Rubin, C.H.; McGeehin, M.A. Heat-related mortality during a 1999 heat wave in Chicago. Am. J. Prev. Med. 2002, 22, 221–227. [Google Scholar] [CrossRef]
- Vida, S.; Durocher, M.; Ouarda, T.B.M.J.; Gosselin, P. Relationship between ambient temperature and humidity and visits to mental health emergency departments in Québec. Psychiatr. Serv. 2012, 63, 1150–1153. [Google Scholar] [CrossRef] [PubMed]
- Bouchama, A.; Dehbi, M.; Mohamed, G.; Matthies, F.; Shoukri, M.; Menne, B. Prognostic factors in heat wave related deaths: A meta-analysis. Arch. Intern. Med. 2007, 167, 2170–2176. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, R.; Rubin, C.H.; Henderson, A.K.; Wolfe, M.I.; Kieszak, S.; Parrott, C.L.; Adcock, M. Heat-Related Death and Mental Illness During the 1999 Cincinnati Heat Wave. Am. J. Forensic Med. Pathol. 2001, 22, 303. [Google Scholar] [CrossRef] [PubMed]
- Brewerton, T.D.; Putnam, K.T.; Lewine, R.R.J.; Risch, S.C. Seasonality of cerebrospinal fluid monoamine metabolite concentrations and their associations with meteorological variables in humans. J. Psychiatr. Res. 2018, 99, 76–82. [Google Scholar] [CrossRef]
- Åström, D.O.; Forsberg, B.; Edvinsson, S.; Rocklöv, J. Acute Fatal Effects of Short-Lasting Extreme Temperatures in Stockholm, Sweden: Evidence Across a Century of Change. Epidemiology 2013, 24, 820–829. [Google Scholar] [CrossRef]
- Anderson, B.G.; Bell, M.L. Weather-related mortality: How heat, cold, and heat waves affect mortality in the United States. Epidemiology 2009, 20, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Erlangsen, A.; Andersen, P.K.; Toender, A.; Laursen, T.M.; Nordentoft, M.; Canudas-Romo, V. Cause-specific life-years lost in people with mental disorders: A nationwide, register-based cohort study. Lancet Psychiatry 2017, 4, 937–945. [Google Scholar] [CrossRef]
- Hajat, S.; O’Connor, M.; Kosatsky, T. Health effects of hot weather: From awareness of risk factors to effective health protection. Lancet 2010, 375, 856–863. [Google Scholar] [CrossRef]
- Buckley, J.P.; Samet, J.M.; Richardson, D.B. Commentary: Does Air Pollution Confound Studies of Temperature? Epidemiology 2014, 25, 242. [Google Scholar] [CrossRef] [PubMed]
- Carlsen, H.K.; Steingrimsson, S.; Sigurdsson, M.I.; Magnusson, A. The stability of diagnosis over time in a register-based study of psychiatric inpatients. Eur. Psychiatry 2015, 30, 1385. [Google Scholar] [CrossRef]


{kind=link}
| Percentiles | Warm Season 1 | Cold Season 2 | ||
|---|---|---|---|---|
| Lags 0–3 | Lags 0–14 | Lags 0–14 | Lags 0–21 | |
| 5th percentile | 1.01 (0.98–1.04) | 1.11 (0.94–1.31) | 1.25 (0.92–1.71) | 1.18 (0.70–1.98) |
| 95th percentile | 1.14 (1.02–1.28) | 1.22 (1.06–1.40) | 1.06 (0.93–1.21) | 1.02 (0.79–1.31) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carlsen, H.K.; Oudin, A.; Steingrimsson, S.; Oudin Åström, D. Ambient Temperature and Associations with Daily Visits to a Psychiatric Emergency Unit in Sweden. Int. J. Environ. Res. Public Health 2019, 16, 286. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16020286
Carlsen HK, Oudin A, Steingrimsson S, Oudin Åström D. Ambient Temperature and Associations with Daily Visits to a Psychiatric Emergency Unit in Sweden. International Journal of Environmental Research and Public Health. 2019; 16(2):286. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16020286
Chicago/Turabian StyleCarlsen, Hanne Krage, Anna Oudin, Steinn Steingrimsson, and Daniel Oudin Åström. 2019. "Ambient Temperature and Associations with Daily Visits to a Psychiatric Emergency Unit in Sweden" International Journal of Environmental Research and Public Health 16, no. 2: 286. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16020286